Psych · General adult psychiatry — personality disorders
Paranoid personality disorder
Also known as PPD · Paranoid PD · Cluster A personality disorder · Suspicious personality
Exam-exhaustive fellowship reference on paranoid personality disorder — DSM-5-TR and ICD-11 nosology; differentials from delusional disorder and schizophrenia spectrum; trauma-linked threat-bias mechanisms; alliance-first psychotherapy; pharmacotherapy limits; risk of retaliation and litigation. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
1 MCQ with explanations
Target exams
Red flags
Paranoid personality disorder (PPD) is a medium-weight general adult and forensic-interface topic across FRANZCP, MRCPsych, ABPN and MD/DNB. Examiners test operational criteria, the PPD–delusional disorder discriminator, trauma-linked mechanisms, alliance skills, and evidence humility for treatment.[1][2][3]
Overview and definition
PPD describes a long-standing pattern of interpreting others as exploiting, harming or deceiving — typically without the fixed, incorrigible delusional intensity that defines delusional disorder, and without the broader psychotic syndrome of schizophrenia.[1][2][15]
DSM-5-TR categorical diagnosis (exam-critical). After general personality disorder criteria are met, PPD requires a pervasive distrust and suspiciousness of others such that their motives are interpreted as malevolent, beginning by early adulthood and present in a variety of contexts, as indicated by four or more of: suspects, without sufficient basis, that others are exploiting, harming, or deceiving him or her; is preoccupied with unjustified doubts about the loyalty or trustworthiness of friends or associates; is reluctant to confide in others because of unwarranted fear that the information will be used maliciously against him or her; reads hidden demeaning or threatening meanings into benign remarks or events; persistently bears grudges (is unforgiving of insults, injuries, or slights); perceives attacks on his or her character or reputation that are not apparent to others and is quick to react angrily or to counterattack; has recurrent suspicions, without justification, regarding fidelity of spouse or sexual partner. The pattern must not occur exclusively during the course of schizophrenia, a bipolar or depressive disorder with psychotic features, or another psychotic disorder, and is not attributable to the physiological effects of another medical condition.[2][3]
ICD-11 framing. Personality disorder is graded by severity (mild, moderate, severe) with trait domain qualifiers. Features historically labelled paranoid PD map largely onto high negative affectivity and dissociality/suspiciousness (and sometimes detachment) within a severity rating. Fellowship answers should name which manual is in use and that ICD-11 is dimensional-severity first, whereas classic MCQ stems still use DSM's ≥4/7 rule.[2][3]
Validity debate (viva-ready nuance). PPD is clinically common and consequential yet historically under-researched; some authors have questioned free-standing categorical validity and preferred dimensional coding of trait-paranoia, while others argue the construct remains essential for clinic and laboratory work, with closer links to trauma than to schizophrenia for many patients.[1][2][10]
Classification and nosology
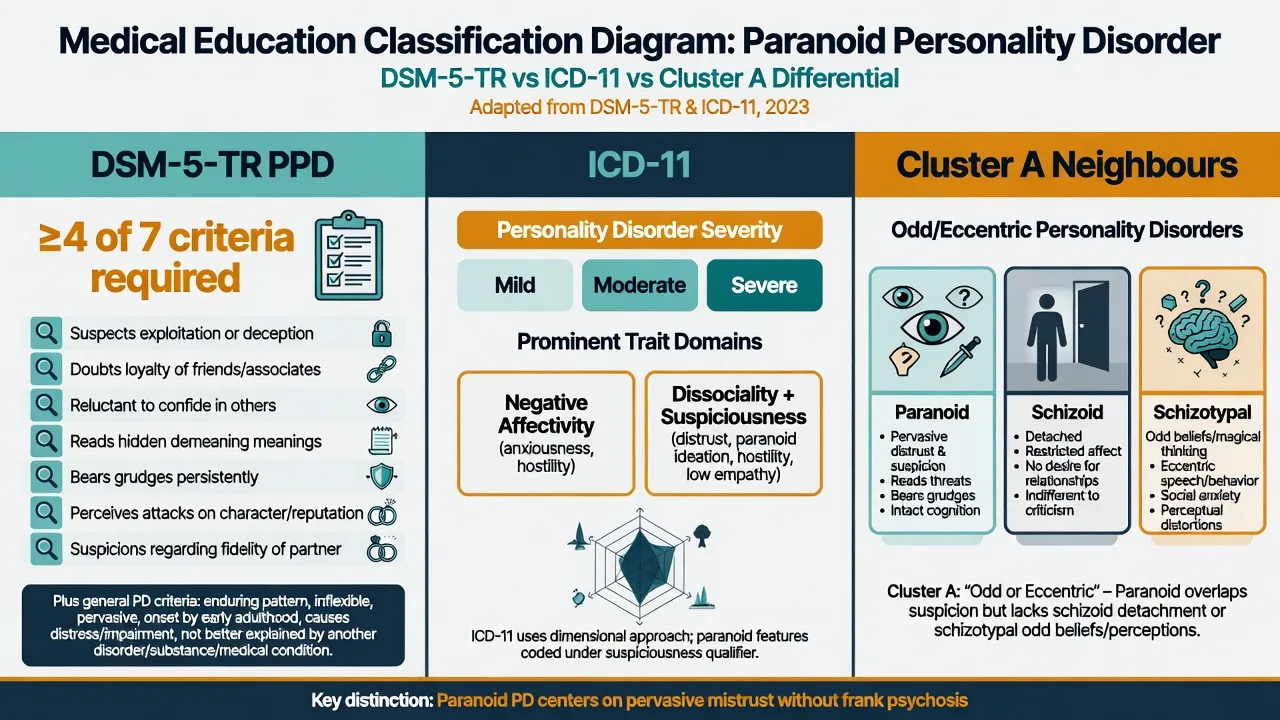
DSM-5-TR PPD
- ≥4 of 7 distrust features
- Onset by early adulthood, pervasive
- Not exclusively during psychotic disorder
- General PD criteria also required
ICD-11 PD
- Severity first: mild / moderate / severe
- Trait domains (negative affectivity, dissociality/suspiciousness)
- Dimensional language aids formulation
- Legacy categorical PPD still appears in stems
AMPD (DSM Section III)
- Criterion A: self and interpersonal impairment
- Criterion B: often antagonism/suspiciousness, negative affectivity
- Useful even if categorical diagnosis used
- Avoid trait lists without impairment
Cluster A neighbours
- Schizoid: detachment without malevolent appraisal core
- Schizotypal: cognitive-perceptual oddness
- PPD: pure pervasive distrust
- Overlap common — formulate primary pattern
Taxometric analyses of interview and self-report indicators support a dimensional latent structure for paranoid personality rather than a discrete taxon — consistent with ICD-11 trait thinking and with continuum models of non-delusional paranoia.[10]
Epidemiology and risk factors
Headline epidemiology candidates must own
Community surveys document that personality disorders are common enough to matter for service planning; PPD prevalence estimates vary by instrument and sample, with clinical and forensic enrichment relative to household surveys.[7][8][9][14] Lee's review emphasises links with childhood trauma, social stress, and violence-related outcomes, and highlights descriptive similarities and differences versus BPD samples — pushing candidates away from a pure "schizophrenia-spectrum only" story.[1] Twin data support genetic contribution to PD risk structure with environmental interaction; do not overclaim a single "PPD gene."[13]
Pathophysiology and mechanisms
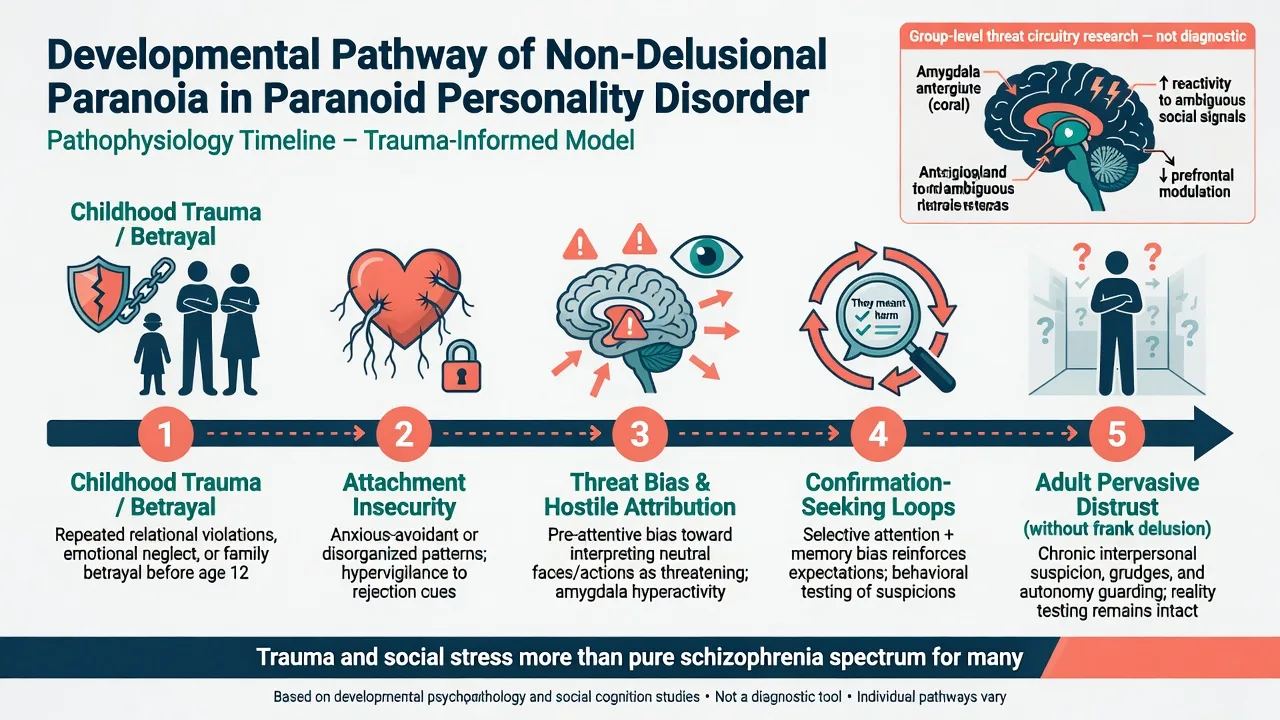
Cognitive-interpersonal model. Hostile attribution bias, selective attention to threat, and confirmation-seeking maintain a self-reinforcing loop: neutral remarks are coded as demeaning, confiding feels unsafe, and grudges organise memory. Reality testing remains essentially intact — the person can often acknowledge alternative explanations under safe conditions even if they do not adopt them — which helps separate PPD from frank delusion.[1][2][3]
Developmental and trauma model. Early betrayal, maltreatment, and chronic invalidation seed hypervigilant interpersonal schemas. Available clinical data support closer proximity to trauma-related psychopathology than to schizophrenia for many PPD presentations, while still recognising spectrum adjacency for some individuals who later develop frank psychosis.[1]
Psychodynamic and social learning views. Projection of unacceptable self-aspects, fragile self-esteem defended by externalising blame, and modelling of mistrust in coercive families are classic viva frameworks. Keep them as formulations, not unfalsifiable labels.[1][2]
Neurobiology (keep humble). Group-level work on threat processing and stress systems (including HPA/CRH findings discussed in reviews) is hypothesis-generating only. Imaging and biomarkers do not diagnose PPD.[1][10]
Clinical presentation
Core presentation combines pervasive distrust, loyalty doubts, reluctance to confide, reading hidden meanings, grudges, angry counterattack to perceived slights, and recurrent unjustified fidelity suspicions. On MSE, expect guarded rapport, restricted warmth, scanning for criticism, litigious narrative style, externalisation of blame, and secondary agendas (second opinions, recording sessions, requests for "proof"). Frank hallucinations, disorganisation, or fixed incorrigible delusions are not the defining features — their presence forces a psychosis-spectrum reformulation.[1][2][3]
Settings examiners use. Couple therapy and primary care see jealousy and workplace conflict; ED and crisis services see retaliatory threats after perceived betrayal; forensic settings see stalking, excessive litigation, and aggression linked to threat appraisal; CMHTs see treatment-refusing, second-opinion-shopping patients with comorbid depression or substance use.[1][3]
Differential diagnosis
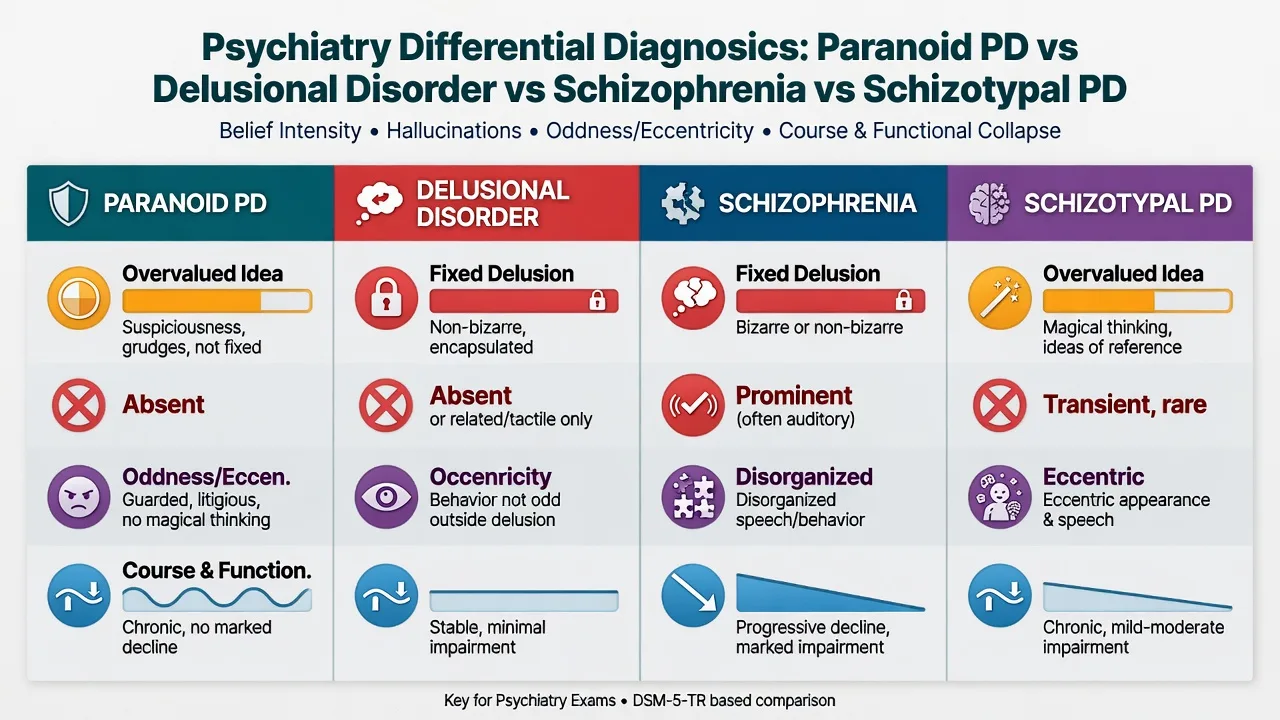
vs Delusional disorder
- DD: fixed false belief of delusional intensity
- Often encapsulated; behaviour organised around delusion
- PPD: overvalued suspiciousness, grudges, not fully delusional
- If in doubt, document intensity, fixity, insight over time
vs Schizophrenia
- Hallucinations, disorganisation, negative symptoms
- Marked functional collapse common
- PPD lacks frank psychotic syndrome as core
- Substance and organic mimics still mandatory
vs Schizotypal PD
- Odd beliefs, magical thinking, perceptual anomalies
- Eccentric speech/appearance
- PPD may lack marked oddness
- Both Cluster A — comorbidity possible
vs Other
- Schizoid: detachment without malevolent core
- BPD: transient stress paranoia + abandonment/self-harm
- Stimulant/cannabis paranoia: timeline with use
- Late onset → organic until proven otherwise
Culturally sanctioned distrust after discrimination, refugee persecution, or systemic injustice is not automatically PPD. Cultural formulation is part of competent diagnosis.[1][3]
Clinical and bedside assessment
Structure the interview: developmental and attachment history; onset of mistrust; trauma and betrayal narratives; relationship and occupational chronology; jealousy and litigation history; substance use; prior treatments and dropouts; what the patient wants help with today (often sleep, depression, work conflict — not "personality"). Obtain collateral early; self-report may minimise impairment or be distorted by threat appraisal.[1][3]
MSE focus. Rapport quality; thought content (overvalued idea vs delusion); perceptual phenomena; insight; capacity (decision-specific); risk of retaliation; testing of clinician honesty. Document how the interpersonal style appears in the room.[2][3]
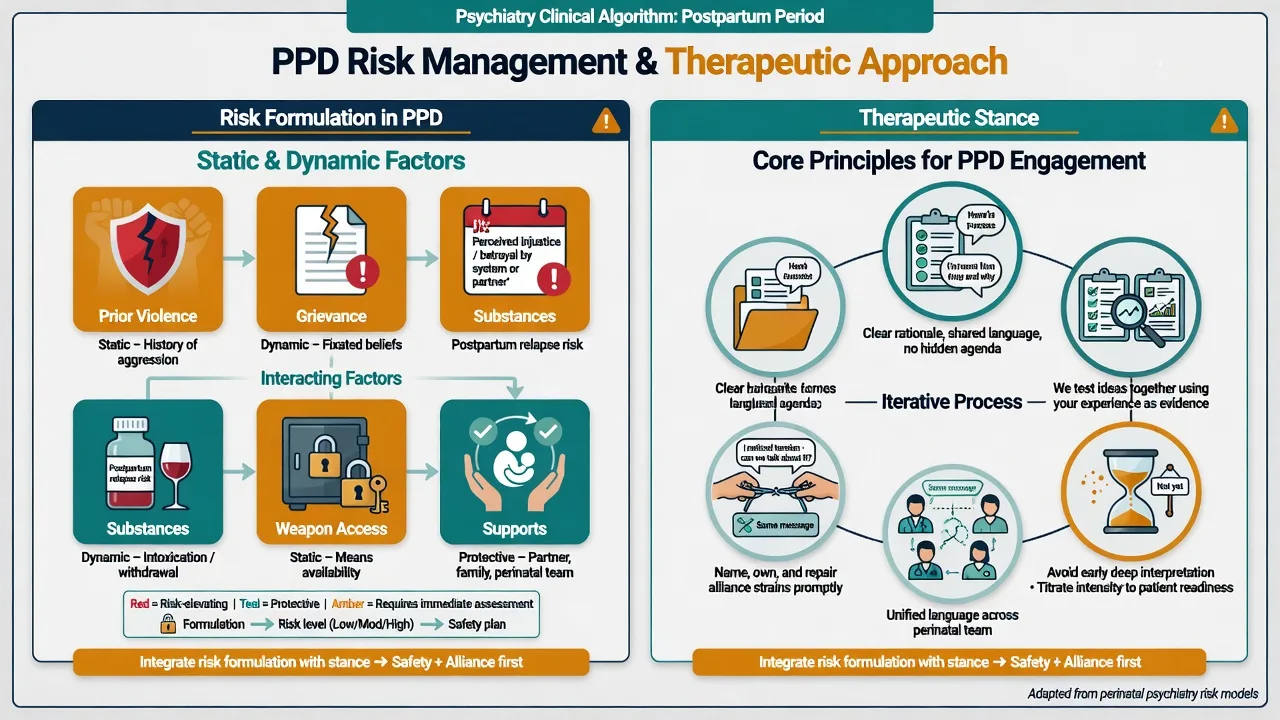
Risk domains. Suicide and self-harm rise with comorbid depression. Other-directed risk relates to threat appraisal, grievance, jealousy, substances, and means access — PPD is among stronger personality-related predictors of aggression in some clinical series, yet risk is formulated, never assumed from the label alone.[1][3]
Investigations
PPD has no laboratory gold standard. Investigate to exclude mimics and prepare for any medication: urine drug screen when relevant; FBC, U&E, LFT, TSH, glucose/lipids as baseline; pregnancy test when applicable; ECG before QT-prolonging agents; cognitive screen and neuroimaging or EEG when late-onset change, focal neurology, seizures, or significant TBI history fire. Screen systematically for depression, anxiety, PTSD, substance use, other personality disorders, and frank psychosis because they change management more than the PPD label alone.[3][6]
Management — acute crisis and resuscitation
Immediate priorities. Scene safety, weapons, medical stabilisation of intoxication, withdrawal, head injury, or delirium. De-escalate; low-stimulus environment; pharmacological rapid tranquillisation only when needed for imminent harm per local emergency protocols with monitoring — not as long-term "paranoid sedation."[3][6]
Crisis stance. Transparent about roles and limits; avoid power struggles and early deep interpretation; do not collude with false allegations, and do not dismiss genuine safety concerns. Treat medical and psychiatric comorbidity with the same standard of care as any other patient.[1][3][4]
Management — definitive and stepwise
What the evidence actually supports
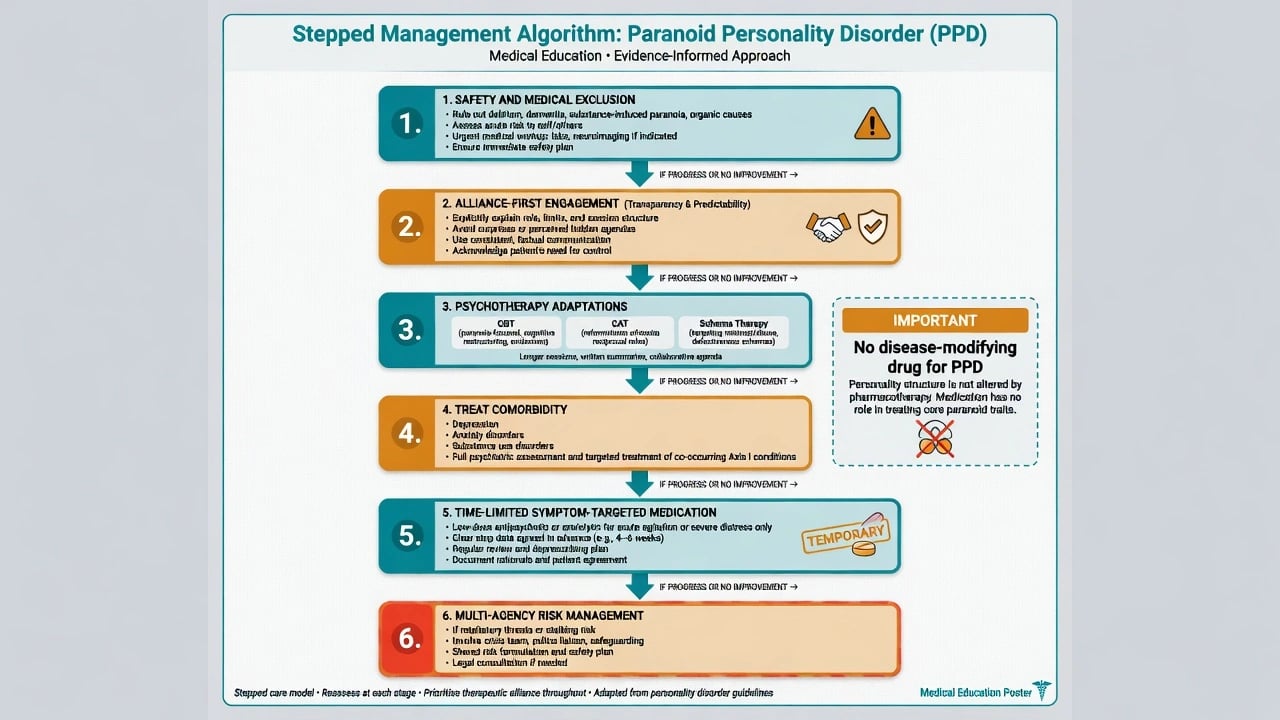
PPD-specific randomised evidence remains sparse because of recruitment and historical neglect. A 2025 systematic review and exploratory meta-analyses of psychosocial and pharmacological interventions for Cluster A disorders (including PPD) suggest treatments can be feasible and effective on clinical features and functioning, but samples are small and heterogeneity is large — cite as promising, not definitive.[4] Narrative reviews emphasise that psychotherapy is the mainstay, dropout risk is high, and no medication is approved as disease-modifying for PPD.[1][3][6]
Psychological approaches
Alliance principles (non-negotiable in exams). Predictability, transparency about confidentiality limits, collaborative agenda-setting, modest early goals, and active rupture repair. Early deep interpretation or aggressive cognitive challenge often destroys trust. Slow pacing and validating genuine elements of threat (without endorsing distortion) reduce defensive escalation.[1][3][4]
Named modalities with examinable signals. Cognitive-behavioural adaptations targeting threat bias and interpersonal mistrust are widely advocated; controlled PPD-specific trial evidence is limited. Cognitive analytic therapy has a published mixed-methods single-case experimental design in PPD showing clinical improvement signals — cite as structured case-level evidence, not a large RCT portfolio.[5] Schema therapy has multicentre RCT support in mixed personality disorder samples (including Cluster C and other PDs), providing transferable principles of limited reparenting and schema change for mistrust-related modes even when pure PPD cells are small.[11] Metacognitive interpersonal therapy has published case work in severe PPD focusing on metacognition and interpersonal cycles.[16]
Pharmacotherapy — only for targets you can name
No medication treats PPD as a whole.[3][6] Cluster A pharmacologic reviews find limited, low-quality evidence; any drug use should target named symptoms or comorbidities with review dates.[4][6]
- Major depression / anxiety: standard first-line pathways with careful engagement. Example adult plan when an examiner forces a named comorbid prescription (individualise): sertraline 50 mg orally daily, early review for activation and adherence, titrate toward 50–150 mg as tolerated with limited dispensing if overdose risk is high — this treats depression, not PPD identity.[3][6]
- Severe agitation or marked cognitive-perceptual distress: time-limited low-dose second-generation antipsychotic may be considered in specialist settings after non-drug strategies, with metabolic and ECG monitoring as indicated and a stop/review date — not chronic "personality control."[4][6]
- Avoid chronic benzodiazepines for trait mistrust; they add dependence risk without modifying personality structure.[6]
Care system
Most patients are managed in outpatient psychotherapy and general adult community pathways. Step up for acute risk, frank psychosis, severe self-neglect, or uncontainable retaliation risk. Consistency of one agreed formulation across the team reduces iatrogenic rupture.[1][4]
Australian and New Zealand practice emphasises cultural safety, trauma-informed engagement, and multi-agency risk management when third-party threat is active. Mental Health Act statutes are state/territory-specific — name principles, not invented sections.[1][3]
Specific subtypes and scenarios
Litigious / workplace grievance presentations. Chronic lawsuits and workplace "campaigns" can meet PPD criteria without street violence; still assess risk and capacity, and avoid collusion with false claims.[1][3]
Jealous presentations. Recurrent unjustified fidelity suspicions are a DSM criterion; when beliefs become fixed delusions of partner infidelity, reformulate toward delusional disorder (jealous type) and treat accordingly.[3][15]
PPD + stimulant or cannabis use. Expect acute paranoia spikes; dual treatment and UDS matter more than personality rhetoric alone.[3]
PPD + major depression. Suicide risk rises; treat the depression actively while maintaining paced alliance work.[1][3]
Forensic interface. Stalking, threats, and IPV risk require static/dynamic formulation and multi-agency plans; PPD label neither excuses harm nor proves future violence.[1][3]
Complications and pitfalls
Classic pitfalls: collapsing PPD into delusional disorder or "prodromal schizophrenia" without thresholds; early confrontation destroying alliance; missing trauma, depression, substances, or late-onset organic disease; polypharmacy for chronic mistrust; pejorative labelling; under- or over-estimating violence risk; clinician countertransference (defensiveness, collusion, premature discharge).[1][2][3]
Prognosis and disposition
Course is often chronic, but engagement, safer relationships, reduced substance use, and treatment of comorbidity can improve function. Dimensional views imply graded severity rather than lifelong categorical doom. Disposition follows risk and needs: outpatient psychotherapy/CMHT when containable; escalation when acute risk or frank psychosis emerges. Reassess after relationship rupture, workplace crises, substance relapse, or new weapon access.[1][3][4]
Special populations
Women. Under-recognised relative to caricatured male litigious stereotypes; trauma and jealousy presentations are examinable.[1]
Adolescents. Emerging distrust patterns need developmental formulation; avoid premature lifelong PPD labels without longitudinal data.[2][3]
Older adults. New-onset paranoid change is organic, mood, or substance until proven otherwise — not new-onset "PPD."[3]
Cultural formulation. Structural distrust after discrimination is not automatically personality pathology. In ANZ practice, Indigenous cultural safety and family-inclusive care are competencies.[1][3]
Evidence, guidelines and controversies
Core evidence pillars include narrative clinical reviews (Lee; Triebwasser), dimensional taxometrics (Edens), community epidemiology (Torgersen; Lenzenweger; Grant; Coid), Cluster A treatment synthesis (Cheli), CAT single-case experimental design (Kellett), schema therapy RCT principles (Bamelis), Cluster A pharmacologic review (Koch), schizotypal spectrum context (Rosell), delusional disorder discriminators, twin PD structure (Kendler), and metacognitive interpersonal therapy case work (Cheli).[1][2][4][5][6][7][8][9][10][11][12][13][14][15][16]
Mature controversies. Whether categorical PPD should survive dimensional ICD-11 practice; how far non-delusional paranoia belongs with trauma networks versus schizophrenia-spectrum research; resource ethics for long therapies with limited RCT portfolios; balancing third-party protection with non-discriminatory care.[1][2][10]
Exam pearls
PARANOID — viva checklist
PARANOID
≥4/7 DSM features + general PD criteria
Alliance first — transparency, predictability, rupture repair
Reality testing largely intact (vs fixed delusion)
Assess trauma, substances, depression, organic red flags
Not delusional disorder / not schizophrenia by default
Organic exclusion for late-onset change
ICD-11 severity + suspiciousness/negative affectivity language
Drugs treat comorbidity only — no disease-modifying agent
60-second oral summary
PPD is DSM ≥4/7 distrust features from early adulthood, not exclusively during psychosis — related to but not the same as delusional disorder. Mechanisms emphasise threat bias and trauma more than pure schizophrenia spectrum for many. Discriminate schizophrenia, schizotypal, schizoid, substance, and late-onset organic change. Assess risk of retaliation and jealousy with static/dynamic factors. Treatment: alliance-first psychotherapy (CBT adaptations, CAT case evidence, schema principles, MIT case work), treat comorbidity aggressively, no disease-modifying drug, time-limited symptom targets only, multi-agency plans when third parties are at risk. Hope and structure beat stigma and nihilism.[1][3][4][5][6][15]
References
- [1]Lee R Mistrustful and Misunderstood: A Review of Paranoid Personality Disorder Curr Behav Neurosci Rep, 2017.PMID 29399432
- [2]Triebwasser J, Chemerinski E, Roussos P, Siever LJ Paranoid personality disorder J Pers Disord, 2013.PMID 22928850
- [3]Jain L, Torrico T Paranoid Personality Disorder StatPearls, 2026.PMID 39163470
- [4]Cheli S, Wisepape CN, Witten CDY, Floridi M, et al. Psychosocial and pharmacological interventions for cluster a personality disorders: A systematic review and two exploratory meta-analyses Personal Disord, 2025.PMID 40111791
- [5]Kellett S, Hardy G Treatment of paranoid personality disorder with cognitive analytic therapy: a mixed methods single case experimental design Clin Psychol Psychother, 2014.PMID 23733739
- [6]Koch J, Modesitt T, Palmer M, Ward S, et al. Review of pharmacologic treatment in cluster A personality disorders Ment Health Clin, 2016.PMID 29955451
- [7]Torgersen S, Kringlen E, Cramer V The prevalence of personality disorders in a community sample Arch Gen Psychiatry, 2001.PMID 11386989
- [8]Lenzenweger MF, Lane MC, Loranger AW, Kessler RC DSM-IV personality disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 17217923
- [9]Grant BF, Hasin DS, Stinson FS, Dawson DA, et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2004.PMID 15291684
- [10]Edens JF, Marcus DK, Morey LC Paranoid personality has a dimensional latent structure: taxometric analyses of community and clinical samples J Abnorm Psychol, 2009.PMID 19685951
- [11]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378
- [12]Rosell DR, Futterman SE, McMaster A, Siever LJ Schizotypal personality disorder: a current review Curr Psychiatry Rep, 2014.PMID 24828284
- [13]Kendler KS, Aggen SH, Czajkowski N, Røysamb E, et al. The structure of genetic and environmental risk factors for DSM-IV personality disorders: a multivariate twin study Arch Gen Psychiatry, 2008.PMID 19047531
- [14]Coid J, Yang M, Tyrer P, Roberts A, et al. Prevalence and correlates of personality disorder in Great Britain Br J Psychiatry, 2006.PMID 16648528
- [15]Opjordsmoen S Delusional disorder as a partial psychosis Schizophr Bull, 2014.PMID 24421383
- [16]Cheli S, Cavalletti V, Popolo R, Dimaggio G A case study on a severe paranoid personality disorder client treated with metacognitive interpersonal therapy J Clin Psychol, 2021.PMID 34263957