Psych · General adult psychiatry — perinatal
Perinatal mood and anxiety disorders
Also known as PMAD · Postnatal depression · Postpartum depression · Antenatal depression · Postpartum psychosis · Perinatal OCD · Puerperal psychosis · Peripartum depression
Exam-exhaustive fellowship reference on perinatal mood and anxiety disorders — antenatal and postnatal depression, postpartum psychosis, perinatal anxiety and OCD, bonding, suicide and infanticide risk assessment principles, safe prescribing in pregnancy and lactation, ECT, mother-baby units, and safeguarding. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
12 MCQs with explanations
Target exams
Red flags
Perinatal mental health is high-yield across FRANZCP MEQs, MRCPsych CASC stations, and ABPN items because it fuses general adult mood skills with obstetric timing, safeguarding, and reproductive psychopharmacology. A candidate must separate baby blues, perinatal depression, perinatal anxiety/OCD, and postpartum psychosis, then defend setting, infant safety, and a named drug plan with lactation and pregnancy framing.[7][8][10]
Overview and definition
The perinatal period in clinical psychiatry usually means pregnancy plus the first postnatal year, though service definitions vary. Peak acuity for postpartum psychosis is typically within the first two weeks after birth, whereas depressive and anxiety syndromes may begin antenatally or later in the first year.[5][7]
Perinatal depression includes antenatal and postnatal major depressive episodes. DSM-5-TR uses the mood episode specifier with peripartum onset when onset is during pregnancy or within four weeks after delivery; many services still use a broader postnatal window for care pathways. ICD-11 describes depressive disorders with perinatal timing language — state which system you are using in exam answers.[3]
Baby blues are common, mild, self-limiting mood lability and tearfulness peaking around days 3–5, not equivalent to major depression and not requiring psychotropic treatment when mild and resolving.[7]
Postpartum psychosis is a clinical emergency syndrome, not a single DSM-5-TR entity. It encompasses mania, mixed states, depressive psychosis, and sometimes atypical confusional presentations in the early puerperium, often on a bipolar diathesis background.[5][8]
Classification and spectrum
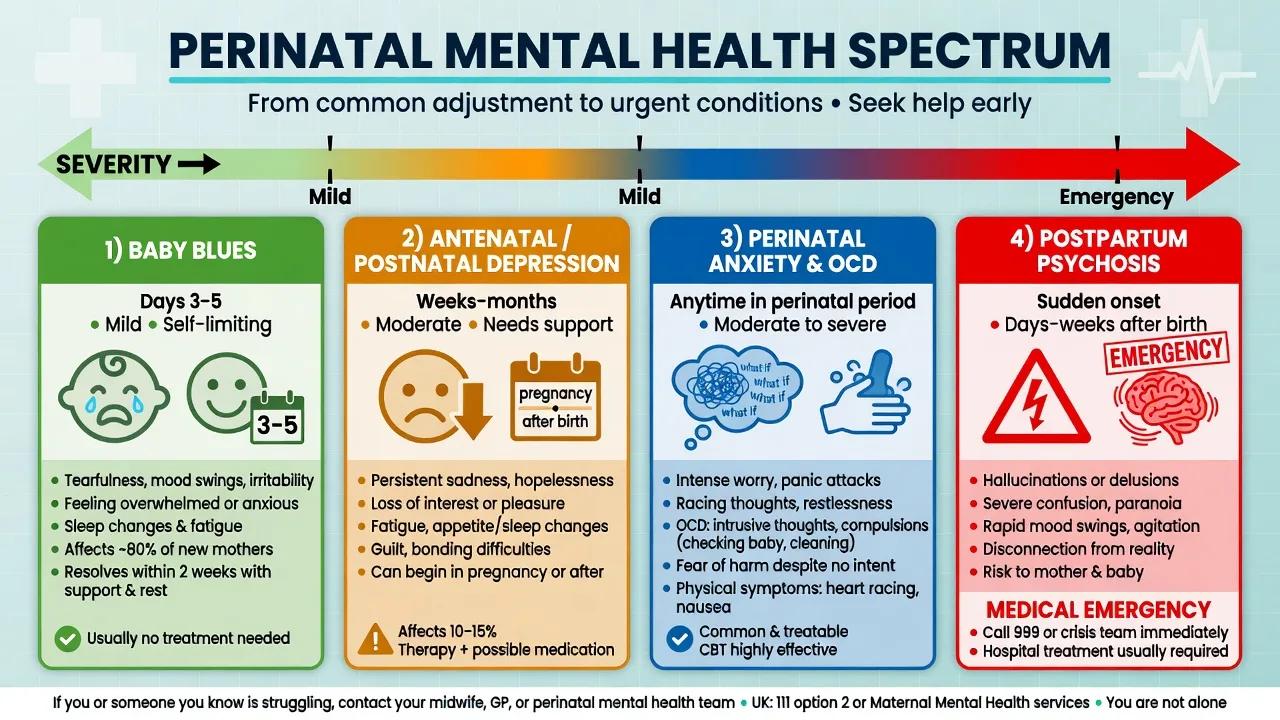
Baby blues
- Days 3–5 peak
- Tearfulness, lability, overwhelm
- Function largely preserved
- Self-limiting with support
Perinatal depression
- Weeks to months
- Anhedonia, guilt, insomnia beyond infant care
- Functional impairment
- Suicide risk must be assessed
Anxiety / OCD
- Worry, panic, avoidance
- Ego-dystonic infant-harm images common in OCD
- Checking and reassurance seeking
- Insight usually preserved
Postpartum psychosis
- Rapid onset early puerperium
- Mania, mixed, depressive psychosis
- Delusions/hallucinations, confusion
- Emergency — mother and infant safety
Bonding difficulties and mother-infant relationship problems may accompany any of the above or present with less syndromal mood pathology; they require parallel parenting support rather than medication alone.[9][10]
Epidemiology and risk factors
Headline numbers for exam use
Gavin and colleagues synthesised prevalence and incidence of perinatal depression, showing substantial burden across pregnancy and the early postpartum months.[1] Woody and colleagues later pooled prevalence near 12% with marked heterogeneity by region and methods.[16]
Munk-Olsen and colleagues demonstrated elevated first-time psychiatric contact among new mothers in the early postpartum period using Danish registers — a classic epidemiology stem for exams.[17] Wesseloo and colleagues quantified high postpartum relapse risk in women with bipolar disorder and/or prior postpartum psychosis, making preconception and postpartum planning non-negotiable.[6]
Risk factors cluster as: prior perinatal or non-perinatal mood/psychotic illness; family history of bipolar disorder; primiparity (especially for postpartum psychosis); severe sleep deprivation; obstetric complications; psychosocial adversity; intimate partner violence; substance use; and poor supports.[5][7][8] Severe mental disorders carry elevated all-cause and suicide mortality in meta-review data — apply that lens when deciding intensity of perinatal care.[11]
Pathophysiology
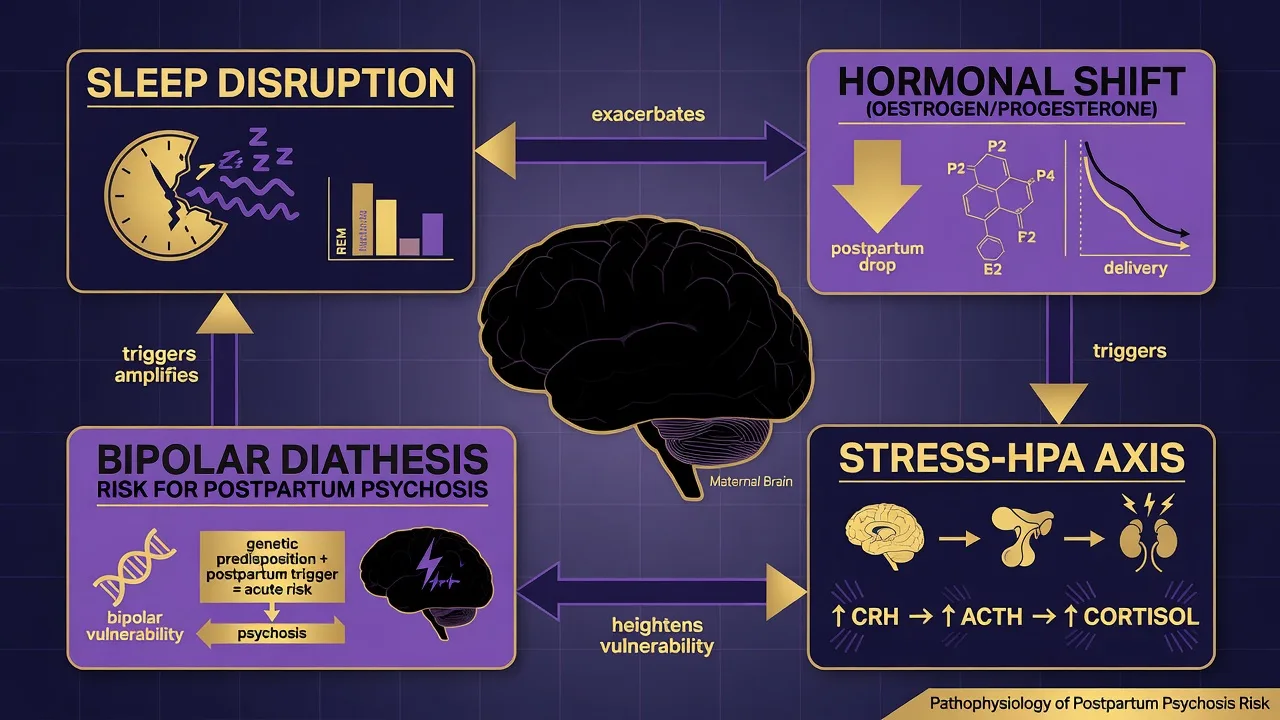
After delivery, abrupt oestrogen and progesterone withdrawal interacts with sleep loss, HPA-axis stress signalling, and genetic/bipolar diathesis — a useful viva model for why the early puerperium is a high-risk window for affective psychosis.[5][8] Psychological models matter equally: cognitive vulnerability, interpersonal role transition, perfectionism, and catastrophic appraisal of normal intrusive thoughts feed depression, anxiety and perinatal OCD.[7][23]
Untreated perinatal mental disorders can affect fetal and child outcomes through maternal behaviour, bonding quality, health-care engagement and the caregiving environment — Stein and colleagues summarise this multi-pathway impact without claiming a single causal chain for every child outcome.[9]
Clinical presentation
Antenatal depression. Persistent low mood or anhedonia, guilt, sleep and appetite change (harder to parse against pregnancy), impaired concentration, suicidal ideation, and avoidance of antenatal care. Disclosure may be inhibited by stigma and fear of child-protection involvement — ask directly and non-punitively.[7][10]
Postnatal depression. Classic depressive syndrome plus themes of being a "bad mother," inability to enjoy the infant, and insomnia that continues when the infant sleeps. Passive death wishes and active suicidal plans both occur; never assume "she would never leave her baby" without a full risk assessment.[7][3]
Postpartum psychosis. Rapid onset of mania, mixed features, or depressive psychosis; insomnia; perplexity or confusion; delusions that may involve the infant; hallucinations; and severe behavioural disturbance. It is a medical-psychiatric emergency with simultaneous mother and infant safety stakes.[5][8]
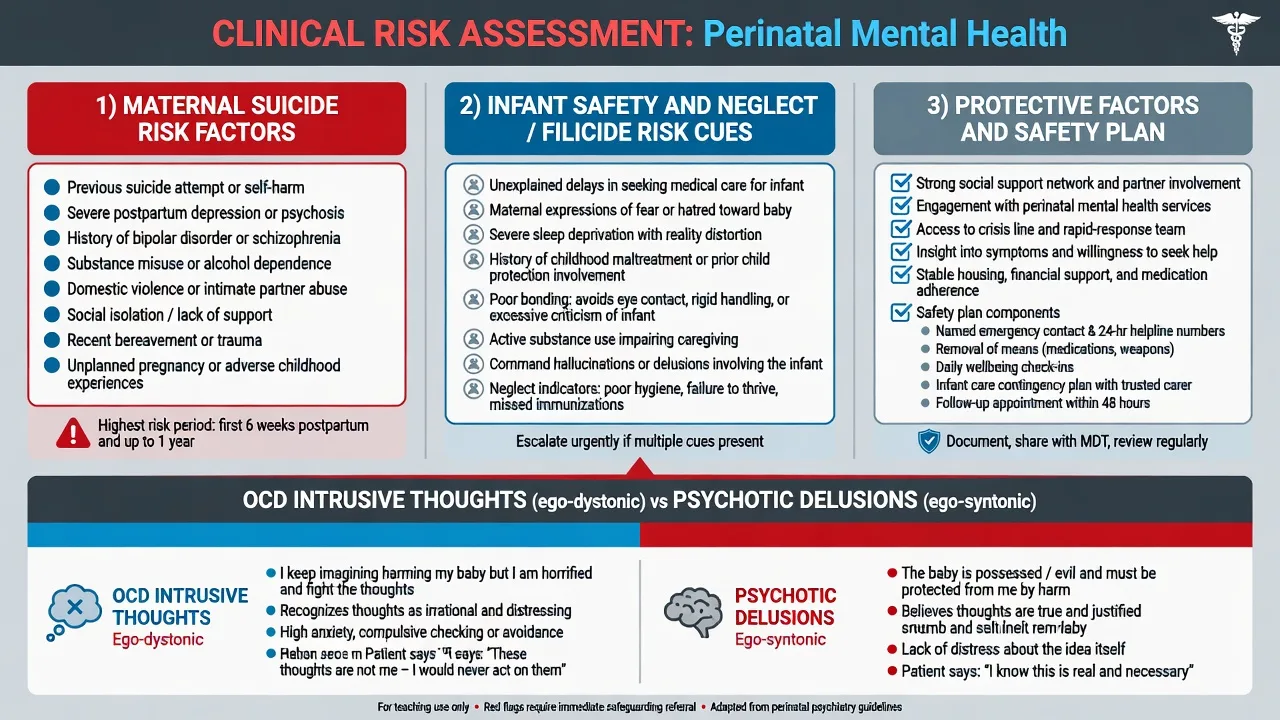
Perinatal anxiety and OCD. Panic, generalised worry, health anxiety about the infant, and ego-dystonic intrusive images of dropping, smothering or harming the baby are common in new parenthood and in clinical OCD. Patients typically recognise thoughts as unwanted and fight them; they are distressed by the thought content rather than committed to it.[22][23]
Bonding. Avoidance of the infant, emotional numbness, or harsh self-criticism about attachment may accompany depression or stand partly separately; observe interaction and enlist parenting supports.[9]
Differential diagnosis
Blues vs depression vs PPP
- Blues: days, mild, resolving
- Depression: weeks+, impairment, suicide risk
- PPP: psychosis/mania, early onset, emergency
Bipolar spectrum
- Prior mania/hypomania decisive when present
- Family history bipolar; antidepressant switching
- Postpartum mania is bipolar until proven otherwise
- Do not treat PPP as simple unipolar depression
OCD vs psychosis re infant harm
- OCD: ego-dystonic, insight, avoidance/checking
- Psychosis: ego-syntonic delusions/commands
- Both need careful risk assessment
- Misclassification either way harms care
Organic / medical
- Delirium, infection, postpartum thyroiditis
- Substance intoxication/withdrawal
- Eclampsia sequelae, rare encephalitis
- Fever, fluctuation, focal signs → investigate
Also keep birth-related PTSD, adjustment disorder, and personality-related affective instability on the board when chronology and MSE support them.[7][5]
Clinical and bedside assessment
Structure the interview: pregnancy and birth course; sleep and feeding; supports and domestic safety (intimate partner violence); prior psychiatric and perinatal episodes; bipolar screen; substances; child-protection history; and the mother's experience of the infant.[7][10]
Document a full MSE with explicit dual risk domains.[5][3]
- Maternal suicide and self-harm — ideation, intent, plan, means, hopelessness, prior attempts, protective factors.[11][3]
- Infant safety — neglect capacity, aggressive impulses, filicide/infanticide ideation, intent, means, command content, and ability to use help.[5][10]
Capacity is decision-specific. Involuntary treatment uses local Mental Health Act principles (least restrictive, statute-bound). Do not invent section numbers for the wrong jurisdiction.[3]
Screening tools
EPDS (Edinburgh Postnatal Depression Scale). Ten-item self-report developed by Cox and colleagues for postnatal depression screening; widely used antenatally and postnatally. It is a screen, not a diagnosis. Expand positive scores — especially thoughts of self-harm items — into a full clinical and risk assessment.[2]
PHQ-9. Nine DSM-aligned items; severity bands support measurement-based care. Item 9 screens suicidal thoughts but is never a complete risk assessment.[15]
Investigations
For severe, atypical or first-onset psychotic presentations: full blood count; urea and electrolytes; liver function; glucose; TSH (postpartum thyroiditis is examinable); consider B12/folate; urine drug screen; infection work-up if fever or delirium features. ECG before selected psychotropics. Neuroimaging or EEG when organic red flags fire — not routinely for classic blues or mild depression.[5][3]
Plan lithium levels, renal and thyroid monitoring if lithium is used postpartum. Use serial EPDS or PHQ-9 for response tracking.[13][15]
Management — emergency and resuscitation
Admission thresholds. Psychosis or mania; high suicide risk; inability to care for the infant safely; severe melancholic depression with poor intake; failed intensive community treatment. Prefer a mother-baby unit when available and clinically appropriate so treatment does not force unnecessary separation; use a general adult ward with infant-care arrangements when MBU beds are unavailable or risk requires a different setting.[20][5]
Acute postpartum psychosis pathway (Bergink-informed). Structured sequential care emphasising benzodiazepines for sleep and agitation, antipsychotics for psychosis/mania, lithium for many affective postpartum psychoses, and high remission rates with protocolised care; maintenance lithium reduced relapse compared with antipsychotic monotherapy in their cohort logic.[13] Exact agents, doses and levels are individualised — state local protocols and target levels (commonly therapeutic mania-range lithium levels under monitoring) rather than memorising a single universal milligram for every patient.[13][4]
Safeguarding and treatment run together: treat illness aggressively while protecting the infant through supervision plans, partner/family supports, and multi-agency involvement when thresholds are met.[10]
Management — definitive and stepped care
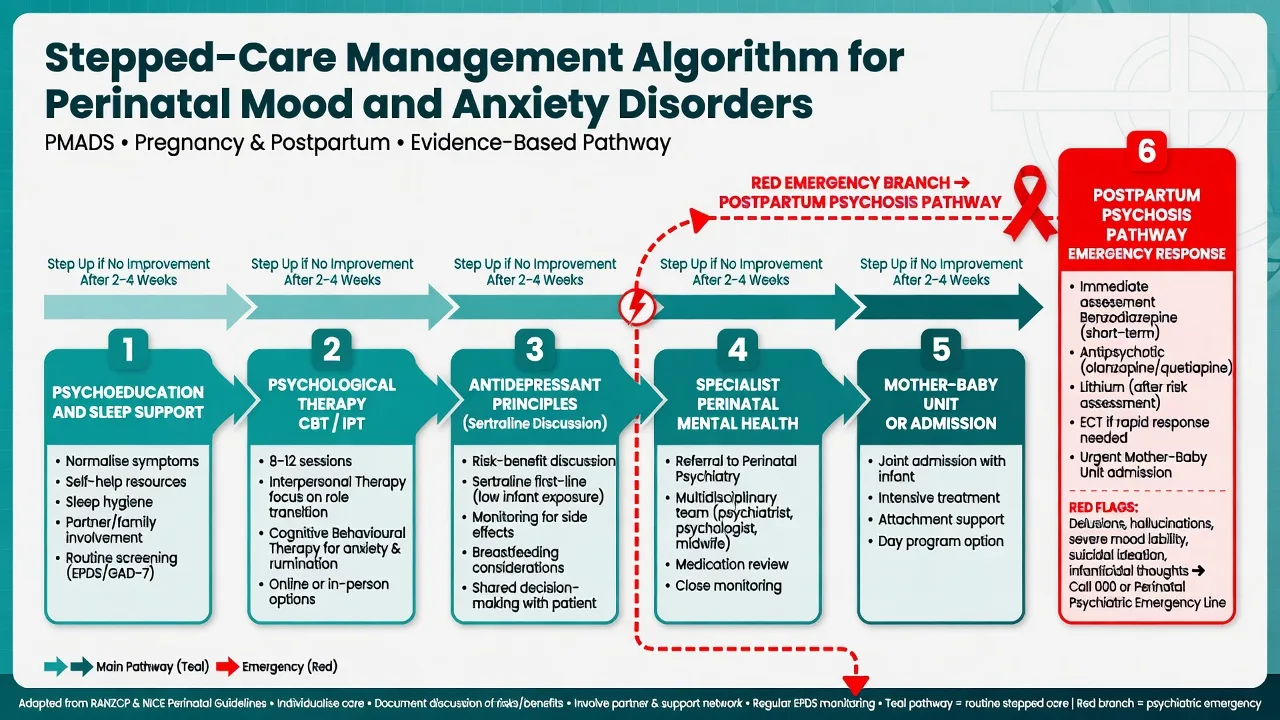
Non-psychotic perinatal depression and anxiety
Stepped care includes psychoeducation, sleep protection, social and partner support, and evidence-based psychological therapies (CBT, IPT, behavioural activation) as core options; antidepressants are added when severity, prior response, patient preference or limited therapy access justify them.[7][25][3]
RANZCP mood disorder guidance frames formulation-driven care, bipolar exclusion, and shared decision-making; Australian mother-baby units provide a distinctive inpatient model for severe perinatal illness when available.[3][20]
Safe prescribing principles (pregnancy and lactation)
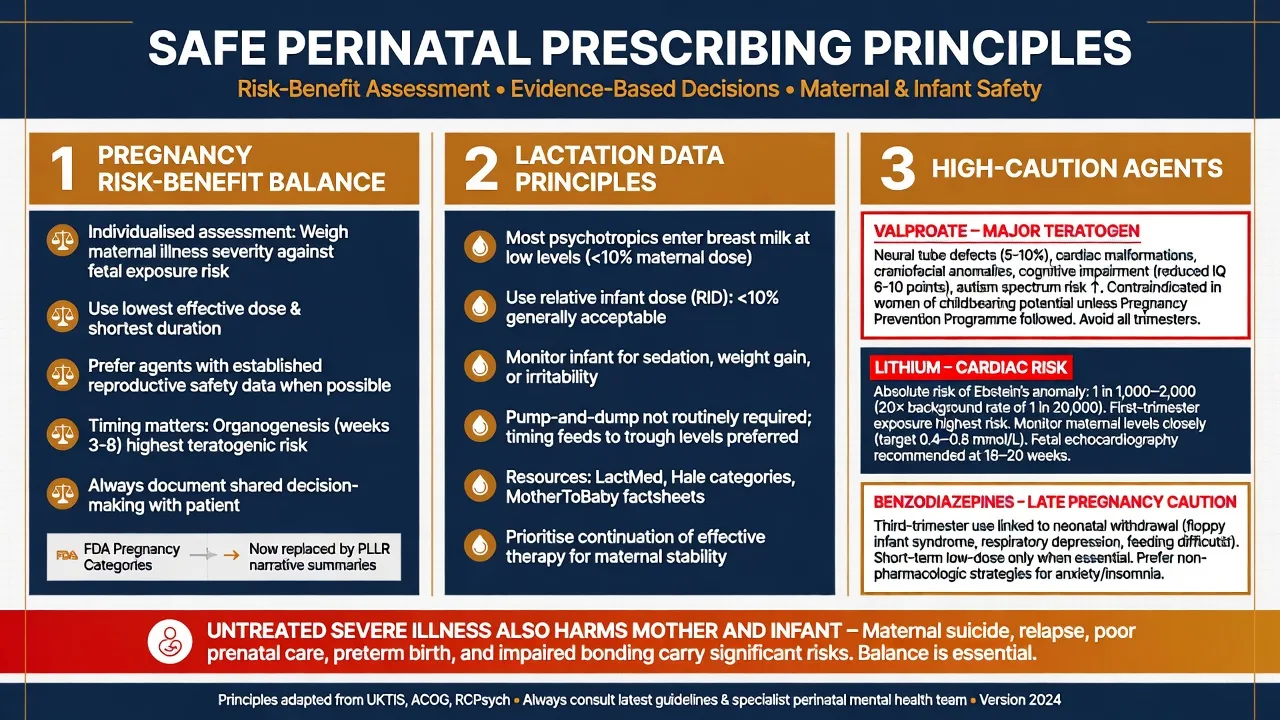
Core principle. Compare risks of medication exposure with risks of untreated or undertreated illness (relapse, suicide, poor antenatal care, impaired bonding, psychosis recurrence). Document shared decision-making.[12][3]
SSRIs in pregnancy. Large meta-analytic data show small absolute associations for some malformations in some analyses; counsel with absolute-risk framing and avoid alarmist relative-risk only talk. Individualise agent choice; many clinicians prefer agents with larger reproductive datasets (commonly sertraline in discussion) when starting de novo.[21][12]
Example first-line antidepressant discussion (postnatal, breastfeeding-preferring). Sertraline 50 mg orally daily, review early for activation and side-effects, titrate toward 100 mg if needed and tolerated, with serial EPDS/PHQ-9 and infant observation for irritability or poor feeding. Typical adult range 50–200 mg daily. This is an exam-ready example, not a universal mandate — individualise for prior response and interactions.[19][3]
Lactation. Weissman and colleagues pooled antidepressant levels in mothers, milk and infants; many SSRIs show low infant plasma levels, with agent-specific differences. Prefer drugs with more favourable milk/infant data when starting; monitor the infant clinically.[19]
Lithium. Patorno and colleagues found increased cardiac malformation risk with first-trimester lithium versus non-exposed bipolar pregnancies and versus lamotrigine, with risk rising at higher doses — counsel with absolute numbers from the paper rather than folklore. Lithium remains highly relevant for high-risk postpartum prophylaxis and treatment of affective postpartum psychosis when benefits outweigh risks under specialist care.[18][4][13]
Valproate. Major teratogen with neurodevelopmental risk — avoid in pregnancy-capable women for bipolar spectrum illness unless exceptional circumstances and rigorous pregnancy-prevention safeguards apply under local regulations. Prefer alternatives in reproductive-age planning.[3][8]
Benzodiazepines. Short-term use may help severe insomnia or agitation in acute PPP algorithms; late-pregnancy and neonatal hypotonia/withdrawal risks require caution and time-limited intent.[13]
Prevention in high-risk women
Women with bipolar disorder or prior postpartum psychosis need preconception counselling, sleep plans, early warning signs, and often proactive postpartum pharmacological strategies (including lithium prophylaxis decisions as in Bergink high-risk cohorts) coordinated with obstetric care.[4][6][8]
ECT in the perinatal period
ECT remains highly effective for severe depressive disorders and is appropriate for life-threatening perinatal depression, catatonia, and selected postpartum psychosis when rapid response is required or medication is insufficient or unsafe. Consent covers anaesthetic, cognitive and obstetric considerations; coordinate with obstetric and anaesthetic teams.[14][24][5]
Perinatal OCD treatment principles
Psychoeducation that intrusive thoughts are common and usually not intent; reduce reassurance rituals; exposure and response prevention adapted to perinatal themes; treat comorbid depression; escalate if insight is lost or risk becomes psychotic/command-driven.[22][23]
Specific subtypes and scenarios
First-onset postpartum psychosis vs known bipolar relapse. Both are emergencies; known bipolar informs prophylaxis and maintenance lithium discussion; first-onset still often signals bipolar spectrum risk longitudinally.[5][8]
Breastfeeding preference with moderate depression. Optimise therapy access; if medication needed, choose agents with better lactation data and monitor infant.[19]
Tokophobia and birth trauma. Anxiety/PTSD pathways may dominate — trauma-informed care and obstetric collaboration, not automatic antidepressant first.[7]
Adolescent mothers and cultural safety. Developmental capacity, family systems, and FRANZCP cultural safety expectations shape engagement and consent.[10]
Complications and pitfalls
Classic errors: labelling psychosis as "stress"; stopping all psychotropics at positive pregnancy test without a plan; confusing OCD intrusions with imminent filicide intent (and the reverse); missing intimate partner violence; polypharmacy without formulation; and using valproate casually in pregnancy-capable patients.[5][3][22]
Prognosis and disposition
Baby blues resolve in days. Untreated major depression often lasts months and risks recurrence. Postpartum psychosis is acutely severe but shows high remission rates with structured inpatient algorithms; recurrence risk in subsequent postpartum periods is high — counsel before the next pregnancy.[13][6]
Disposition ladder. Primary care and midwifery; perinatal mental health teams; crisis services; mother-baby unit; general adult inpatient; child-protection and multi-agency plans when required.[20][10]
Special populations
Fathers and co-parents also experience perinatal mental illness and affect infant outcomes via the caregiving environment. Women with pre-existing schizophrenia, personality disorder or substance use need tailored parenting capacity and risk planning. Lactating versus formula-feeding choices alter but do not eliminate pharmacotherapy options.[9][10]
Mother-baby units
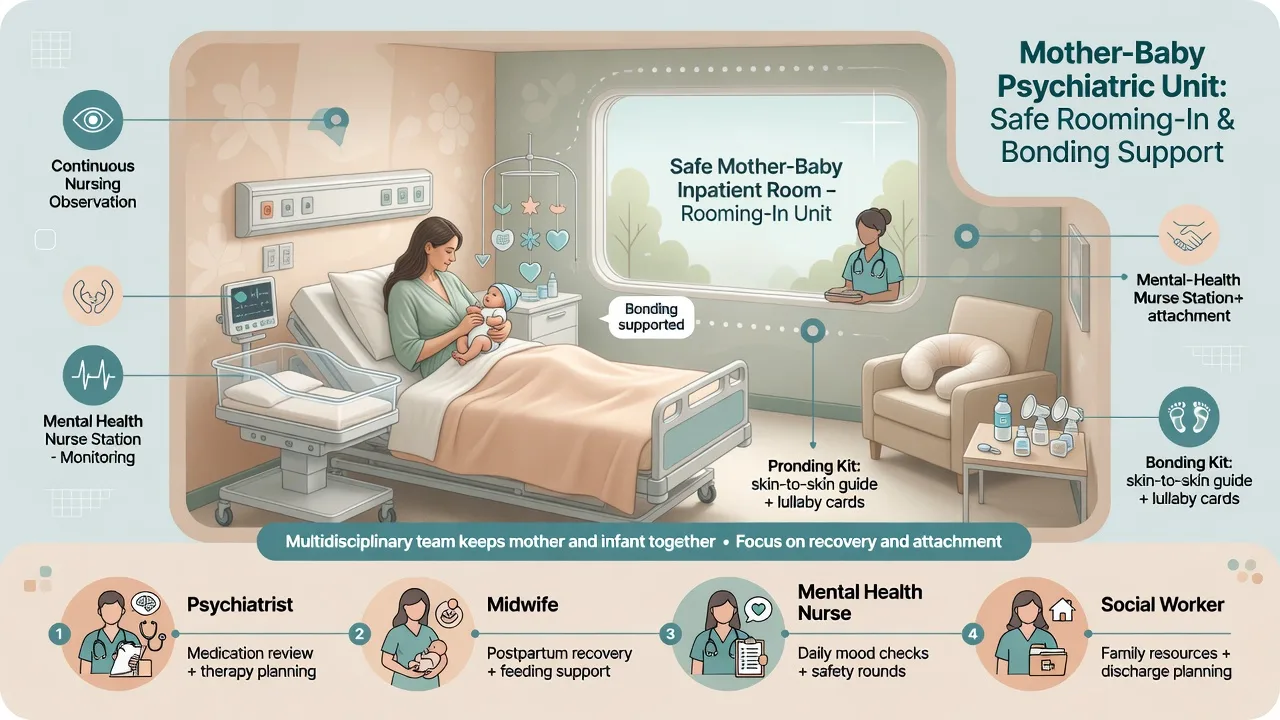
Australian public mother-baby units share core features of joint admission, multidisciplinary care (psychiatry, mental health nursing, midwifery/obstetric liaison, social work), and attachment-informed practice, with regional variation in models. They are preferred when severe illness requires admission and infant safety can be managed in a joint setting.[20]
Evidence, guidelines and regional differences
Landmark pillars for exams: Gavin and Woody prevalence syntheses; Lancet perinatal series (Howard non-psychotic disorders; Jones bipolar/psychosis; Stein child effects); Howard and Khalifeh 2020 progress review; Munk-Olsen register epidemiology; Wesseloo relapse meta-analysis; Bergink prevention, treatment algorithm and clinical review; Cox EPDS; Patorno lithium malformations; Gao SSRI malformations; Weissman lactation levels; Yonkers antidepressant pregnancy overview; UK ECT Review Group and contemporary ECT-for-PPP commentary; Galbally Australian MBU comparison; RANZCP mood guidelines.[1][16][7][8][9][10][17][6][4][13][5][2][18][21][19][12][14][24][20][3]
Exam pearls
PERINATAL emergency checklist
References
- [1]Gavin NI, Gaynes BN, Lohr KN, Meltzer-Brody S, Gartlehner G, Swinson T Perinatal depression: a systematic review of prevalence and incidence Obstet Gynecol, 2005.PMID 16260528
- [2]Cox JL, Holden JM, Sagovsky R Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale Br J Psychiatry, 1987.PMID 3651732
- [3]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [4]Bergink V, Bouvy PF, Vervoort JS, Koorengevel KM, Steegers EA, Kushner SA Prevention of postpartum psychosis and mania in women at high risk Am J Psychiatry, 2012.PMID 22407083
- [5]Bergink V, Rasgon N, Wisner KL Postpartum Psychosis: Madness, Mania, and Melancholia in Motherhood Am J Psychiatry, 2016.PMID 27609245
- [6]Wesseloo R, Kamperman AM, Munk-Olsen T, Pop VJ, Kushner SA, Bergink V Risk of Postpartum Relapse in Bipolar Disorder and Postpartum Psychosis: A Systematic Review and Meta-Analysis Am J Psychiatry, 2016.PMID 26514657
- [7]Howard LM, Molyneaux E, Dennis CL, Rochat T, Stein A, Milgrom J Non-psychotic mental disorders in the perinatal period Lancet, 2014.PMID 25455248
- [8]Jones I, Chandra PS, Dazzan P, Howard LM Bipolar disorder, affective psychosis, and schizophrenia in pregnancy and the post-partum period Lancet, 2014.PMID 25455249
- [9]Stein A, Pearson RM, Goodman SH, Rapa E, Rahman A, McCallum M, et al. Effects of perinatal mental disorders on the fetus and child Lancet, 2014.PMID 25455250
- [10]Howard LM, Khalifeh H Perinatal mental health: a review of progress and challenges World Psychiatry, 2020.PMID 32931106
- [11]Chesney E, Goodwin GM, Fazel S Risks of all-cause and suicide mortality in mental disorders: a meta-review World Psychiatry, 2014.PMID 24890068
- [12]Yonkers KA, Forray A, Smith MV Maternal Antidepressant Use and Pregnancy Outcomes JAMA, 2017.PMID 28810017
- [13]Bergink V, Burgerhout KM, Koorengevel KM, Kamperman AM, Hoogendijk WJ, Lambregtse-van den Berg MP, et al. Treatment of psychosis and mania in the postpartum period Am J Psychiatry, 2015.PMID 25640930
- [14]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [15]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [16]Woody CA, Ferrari AJ, Siskind DJ, Whiteford HA, Harris MG A systematic review and meta-regression of the prevalence and incidence of perinatal depression J Affect Disord, 2017.PMID 28531848
- [17]Munk-Olsen T, Laursen TM, Pedersen CB, Mors O, Mortensen PB New parents and mental disorders: a population-based register study JAMA, 2006.PMID 17148723
- [18]Patorno E, Huybrechts KF, Hernandez-Diaz S Lithium Use in Pregnancy and the Risk of Cardiac Malformations N Engl J Med, 2017.PMID 28854098
- [19]Weissman AM, Levy BT, Hartz AJ, Bentler S, Donohue M, Ellingrod VL, et al. Pooled analysis of antidepressant levels in lactating mothers, breast milk, and nursing infants Am J Psychiatry, 2004.PMID 15169695
- [20]Galbally M, Sved-Williams A, Kristianopulos D, Mercuri K, Brown P, Buist A Comparison of public mother-baby psychiatric units in Australia: similarities, strengths and recommendations Australas Psychiatry, 2019.PMID 30407072
- [21]Gao SY, Wu QJ, Sun C, Zhang TN, Shen ZQ, Liu CX, et al. Selective serotonin reuptake inhibitor use during early pregnancy and congenital malformations: a systematic review and meta-analysis of cohort studies of more than 9 million births BMC Med, 2018.PMID 30415641
- [22]Speisman BB, Storch EA, Abramowitz JS Postpartum obsessive-compulsive disorder J Obstet Gynecol Neonatal Nurs, 2011.PMID 22092284
- [23]Fairbrother N, Abramowitz JS New parenthood as a risk factor for the development of obsessional problems Behav Res Ther, 2007.PMID 17084810
- [24]Kellner CH Electroconvulsive Therapy (ECT) for Postpartum Psychosis: Treatment for a Medical Emergency Am J Psychiatry, 2025.PMID 41320827
- [25]Cuijpers P, Quero S, Noma H, Ciharova M, Miguel C, Karyotaki E, et al. Psychotherapies for depression: a network meta-analysis covering efficacy, acceptability and long-term outcomes of all main treatment types World Psychiatry, 2021.PMID 34002502