Psych · General adult psychiatry — mood disorders
Persistent depressive disorder (dysthymia)
Also known as Dysthymia · Dysthymic disorder · Chronic depression · Double depression · PDD · Persistent depressive disorder · Chronic major depression
Exam-exhaustive fellowship reference on persistent depressive disorder (dysthymia) — DSM-5-TR consolidation of dysthymia and chronic major depression, double depression, 2-year duration rules, Klein longitudinal course, antidepressant and CBASP evidence (Keller, Levkovitz, Cuijpers), stepped care with RANZCP/NICE/APA/CANMAT deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Persistent depressive disorder (PDD) is a high-yield leaf topic because examiners test whether you recognise chronicity as a clinical problem, not a character flaw. FRANZCP MEQs want the 2-year rule, double-depression logic, a named drug with dose, and a psychotherapy plan. MRCPsych papers love dysthymia criteria, CBASP, and antidepressant meta-analytic signals. CASC stations often involve a patient who says "I've always been this way" and a GP who has never offered an adequate trial.[3][9][10]
Overview and definition
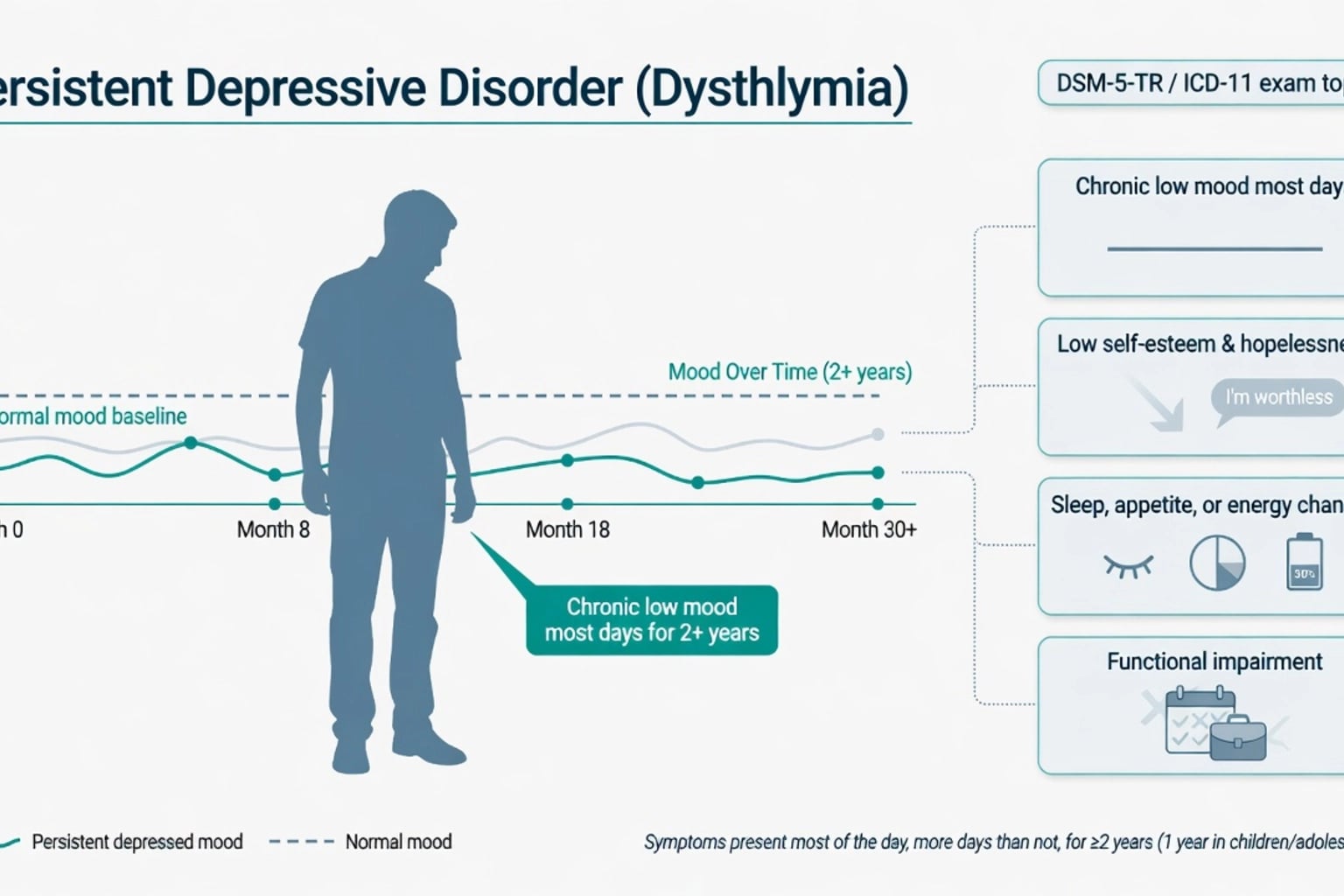
PDD in DSM-5-TR consolidates what DSM-IV split as dysthymic disorder and chronic major depressive disorder. The operational core is depressed mood for most of the day, more days than not, for at least 2 years in adults (or 1 year in children and adolescents, where mood may be irritable), plus two or more of: poor appetite or overeating; insomnia or hypersomnia; low energy or fatigue; low self-esteem; poor concentration or difficulty making decisions; feelings of hopelessness. During the 2-year (or 1-year) period, the person has never been without the symptoms for more than 2 months at a time. Symptoms cause clinically significant distress or impairment and are not better explained by persistent schizoaffective disorder, schizophrenia-spectrum psychotic disorders, or by physiological effects of a substance or another medical condition. Criteria for a major depressive disorder may be continuously present for 2 years, or major episodes may be superimposed on dysthymic symptoms (double depression framing in older literature).[9][10]
Contrast with episodic MDD. An episodic major depressive episode needs five of nine Criterion A symptoms over 2 weeks, with a clear change from baseline. PDD is a duration disorder: fewer concurrent symptoms can qualify if the mood disturbance is chronic. Many patients meet full major depressive criteria for long stretches and still sit inside the PDD construct via the persistent-MDE pathway.[9][10]
ICD-11. Dysthymic disorder describes a persistent depressive mood lasting at least 2 years with additional depressive symptoms that are not severe enough for most of that period to meet criteria for a depressive episode; a chronic depressive episode/course qualifier covers longer major-level illness. State which manual you are using when duration language is examined.[9][10]
Classification and course specifiers
Reproduce the clinical course patterns examiners expect.[9]
| Pattern | Clinical meaning |
|---|---|
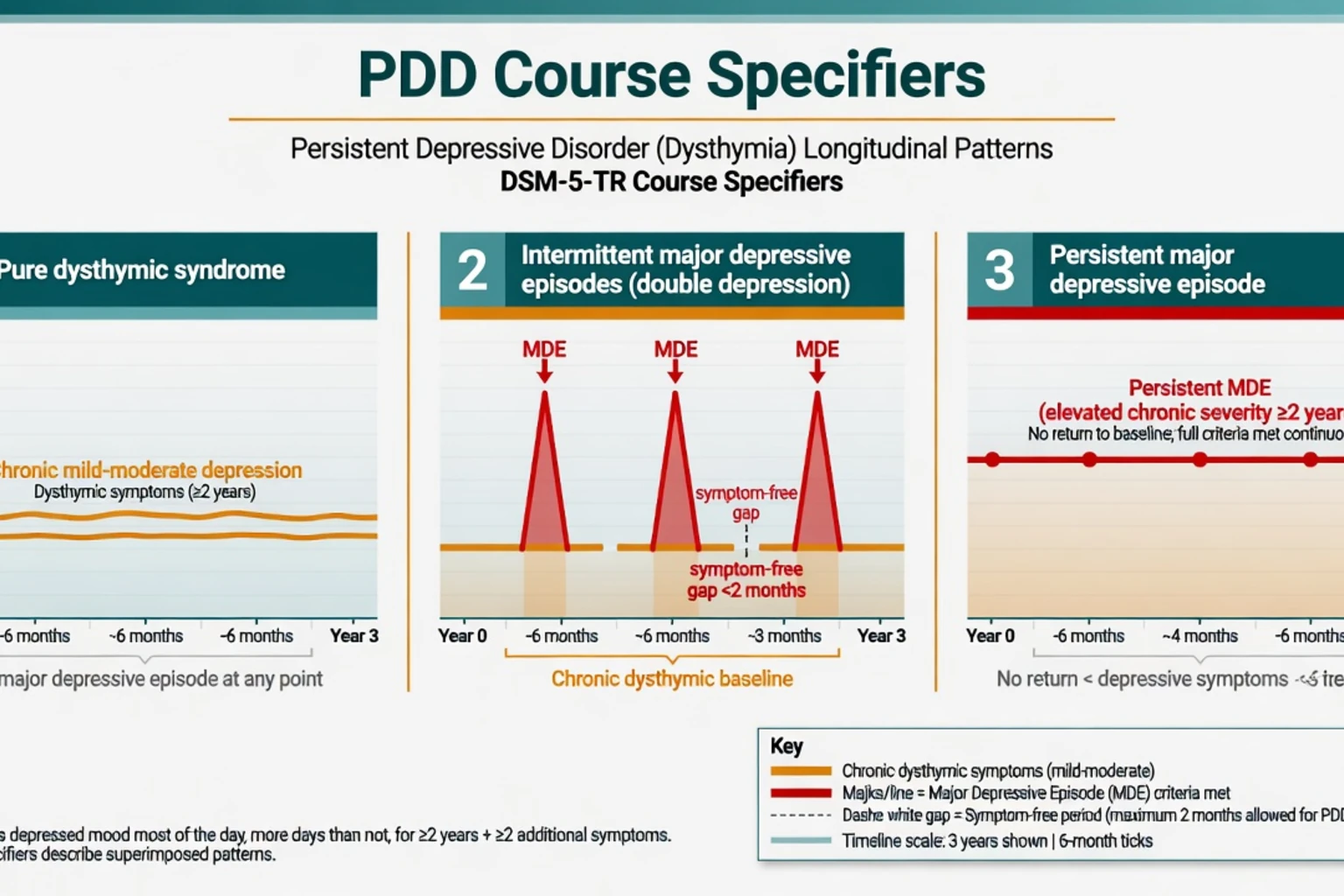
| Pure dysthymic syndrome | Full criteria for a major depressive episode have not been met in at least the preceding 2 years |
| Persistent major depressive episode | Full criteria for a major depressive episode have been met throughout the preceding 2 years |
| Intermittent major depressive episodes, with current episode | Currently in a major depressive episode, with periods of at least 8 weeks in the preceding 2 years with symptoms below major-episode threshold (classic double depression narrative) |
| Intermittent major depressive episodes, without current episode | Not currently in a major episode, but one or more major episodes occurred in the preceding 2 years |
Early onset (before age 21) versus late onset is examined because early onset associates with longer duration, higher comorbidity and personality vulnerability. Specifiers for anxious distress, atypical features, and severity still apply when clinically relevant.[3][9]
Episodic MDD
- 2-week minimum for episode
- Often clear inter-episode recovery
- Five of nine Criterion A symptoms
- May become chronic and then map to PDD
PDD / dysthymia
- ≥2 years adults (≥1 year youth)
- More days than not, most of the day
- ≥2 of 6 symptom menu + depressed mood
- Gaps ≤2 months without symptoms
Double depression
- Chronic dysthymic substrate
- Superimposed major depressive episode
- Higher impairment and suicide risk
- Treat the acute MDE at full intensity
Bipolar chronic depression
- Prior mania/hypomania decisive
- Chronic depressive polarity common in BP-II
- Stabiliser-first framing
- Do not label as uncomplicated PDD
Epidemiology and risk
Numbers candidates should own
Klein and colleagues' 10-year prospective follow-up of dysthymic disorder and double depression demonstrated substantial persistence, high rates of major depressive episodes over time, and meaningful functional morbidity — the exam soundbite that dysthymia is not a benign "personality style". Risk correlates include family history of mood disorder, childhood adversity, anxious and avoidant personality traits, medical comorbidity, and social isolation. Early-onset illness predicts longer cumulative duration and more complex comorbidity.[3][9]
Pathophysiology
There is no single diagnostic biomarker. Viva-level framing combines biological, cognitive and interpersonal maintaining factors.[9]
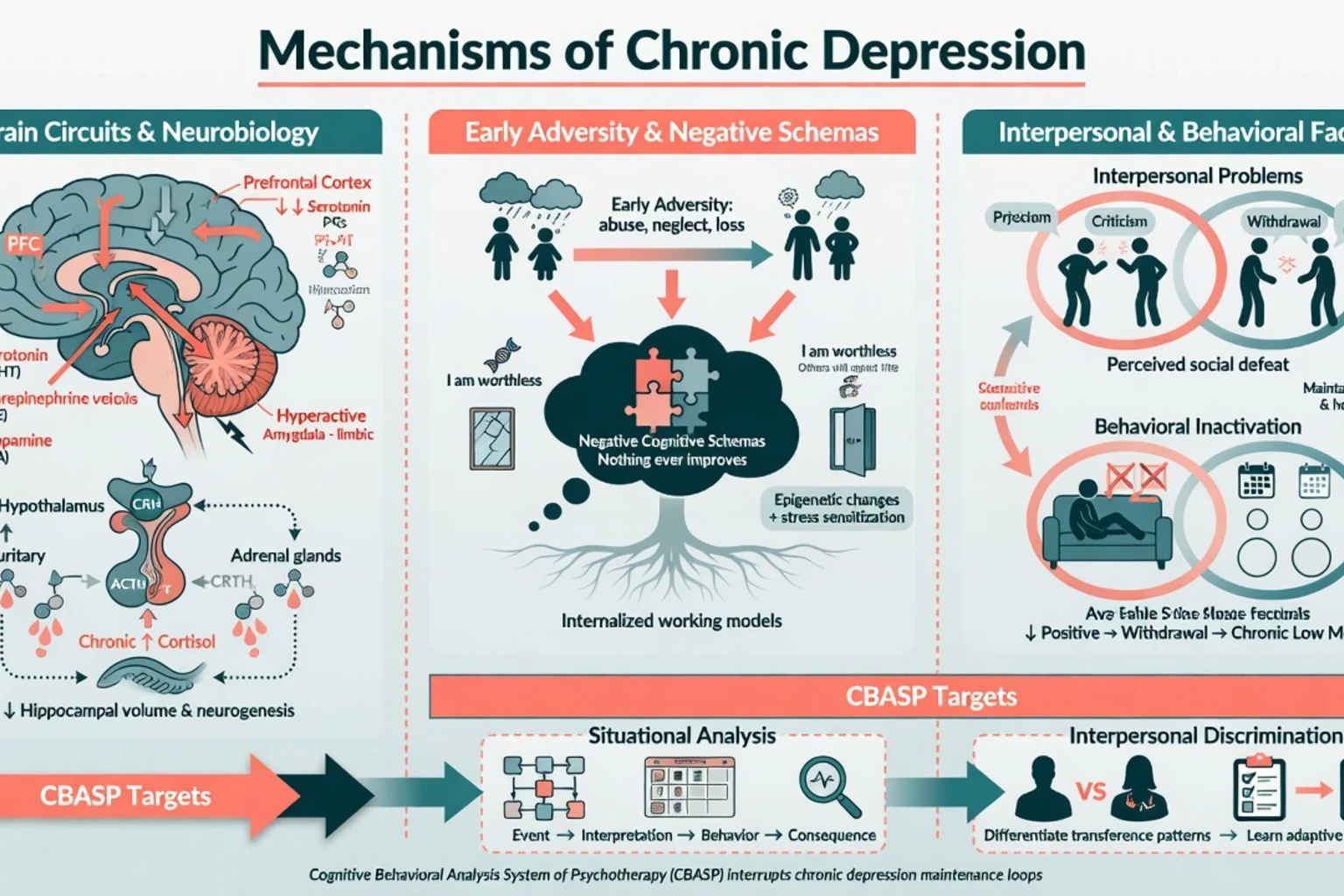
- Neurobiology. Monoamine, HPA-axis and neurotrophic hypotheses parallel episodic depression; chronic stress load and early adversity may embed more persistent dysregulation.[9]
- Cognitive-interpersonal models. Negative schemas ("I am worthless; nothing changes"), interpersonal submission/withdrawal, and behavioural inactivation maintain low mood for years. Patients often stop seeking reinforcement or help because chronicity feels identity-level.[8][9]
- CBASP model (McCullough). Chronic depression is conceptualised as a disorder of interpersonal perception and problem-solving. Situational analysis links specific interpersonal events to interpretations, behaviours and consequences; interpersonal discrimination exercises help patients notice how the therapist (and others) differ from early maltreating figures. This is why CBASP is the named psychotherapy for chronic rather than only episodic depression.[1][2][9]
Clinical presentation
Patients often present late, saying the mood has been continuous for years, sometimes "as long as I can remember." MSE language: dysthymic or depressed affect of restricted range, soft speech, slowed thinking without frank psychomotor retardation (unless a major episode is superimposed), pervasive low self-worth, hopelessness about change, and preserved reality testing. Vegetative features may be milder than melancholic major depression but still impair work and relationships. Pure dysthymic presentations can look "high-functioning" on paper yet report chronic anhedonia, decision paralysis and social withdrawal. Superimposed major episodes bring anhedonia intensification, suicidal ideation spikes, marked anergia, and clearer neurovegetative change — do not miss acuity because the baseline was already low.[3][9][10]
Differential diagnosis
Discriminators, not laundry lists.[9][10]
- Episodic MDD with full recovery — clear well periods longer than 2 months break the PDD duration narrative; if recovery is incomplete, residual symptoms may still map toward chronicity.[9]
- Bipolar spectrum — any prior hypo/mania or mixed features reclassifies management; chronic depression is common in bipolar II.[10]
- Personality disorder — trait affective instability or emptiness is not synonymous with syndromal PDD; both can coexist — formulate both axes and still treat the depressive syndrome.[9]
- Adjustment disorder / prolonged grief — time-locked to a stressor or bereavement with different course expectations.[10]
- Substance/medication-induced and medical mimics — alcohol, cannabis, steroids, interferon-class agents, hypothyroidism, OSA, anaemia, neurological disease.[10]
- Chronic PTSD / complex trauma dysphoria — trauma chronology and re-experiencing symptoms change the formulation and therapy choice.[9]
Assessment
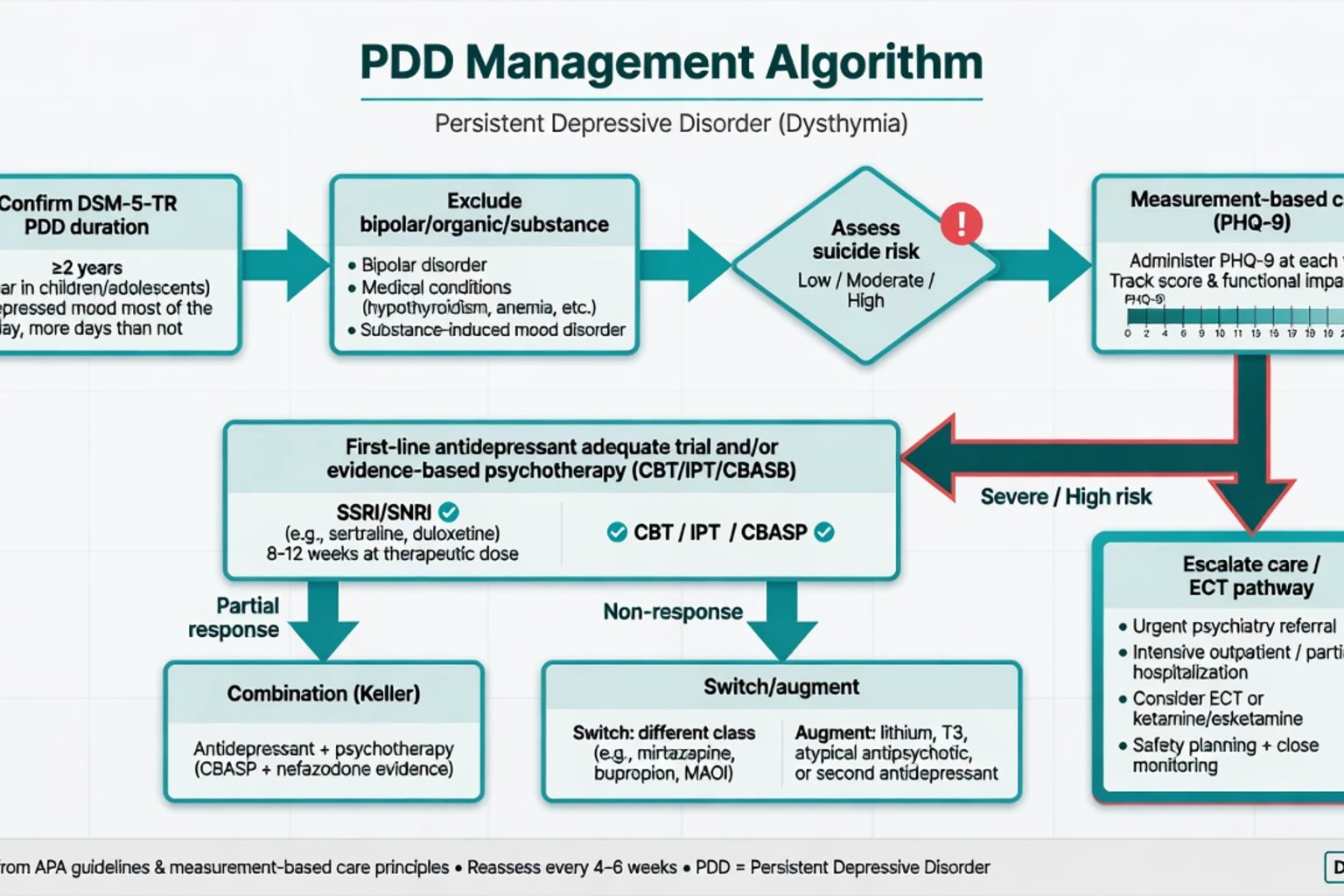
Structure a multi-year mood timeline: continuous low mood start date; any gaps greater than 2 months; dates and severity of superimposed MDEs; prior adequate trials (drug, dose, duration, adherence, adverse effects); psychotherapy exposure and modality; bipolar screen; childhood adversity; substance use; medical history; occupational and relational function; perinatal history if relevant. Complete MSE and a full suicide risk assessment every time a major episode is present or passive death wishes intensify — PHQ-9 item 9 is a screen, not a complete risk assessment.[10][13]
PHQ-9 remains useful for measurement-based care even in chronic illness; a "mild" score on a multi-year background still warrants active management if criteria and impairment are met.[13]
Investigations
Baseline before antidepressants as for MDD: TSH, FBC, U&E, LFT, glucose/lipids as indicated; pregnancy test when relevant; ECG if cardiac risk, TCA consideration, or high-dose citalopram/escitalopram context; urine drug screen when substance contribution is plausible; sleep study if OSA is likely. Neuroimaging is not routine — reserve for late first presentation with focal neurology or progressive cognitive red flags.[10][11]
Acute risk management
Psychotic, catatonic or melancholic severity, or refusal of food and fluids, follows the severe depression pathway including consideration of ECT, not a "try a light dose of SSRI and review in three months" plan.[10]
Definitive management
Psychoeducation and framing
Name the syndrome. Explain that multi-year depression is a treatable medical-psychiatric condition, not a moral failure or immutable personality. Set expectations: response may be slower than in first-episode depression; adequate trials and combination strategies matter; recovery includes function, not only a lower PHQ-9.[9][10]
Pharmacotherapy
Antidepressants are superior to placebo in dysthymia in meta-analysis — do not withhold medication because severity looks "only mild but chronic."[6] Imel and colleagues found a small but significant advantage for medication relative to psychotherapy specifically in dysthymia analyses, reinforcing that pharmacology is not optional folklore in this phenotype.[7]
Named first-line example (adult outpatient). Sertraline 50 mg orally once daily, review early for activation/suicidality/GI effects, then titrate (commonly toward 100–150 mg daily, maximum per product guidance and tolerance, often up to 200 mg) with an adequate trial of 6–8+ weeks at a therapeutic dose and confirmed adherence before declaring failure. Monitoring: mood and risk, sexual side-effects, hyponatraemia risk in older adults, bleeding risk with NSAIDs/anticoagulants, discontinuation counselling. Sertraline and imipramine both showed efficacy versus placebo in classic dysthymia trials; SSRIs are usually preferred first for tolerability in contemporary practice.[4][5][6][11]
Alternative named starts aligned with broader MDD evidence and acceptability: escitalopram 10 mg orally daily (consider titration to 20 mg), or venlafaxine XR 75 mg orally daily with titration and BP monitoring, chosen by comorbidity, prior response and regional formulary.[11][15]
Maintenance. After response in chronic depression, plan longer maintenance than for a single brief episode; antidepressant continuation reduces relapse risk in depressive disorders generally (Geddes meta-analysis framing), and chronic phenotypes often need extended courses with gradual, supervised taper only after sustained stability.[14][10]
Psychotherapy — CBASP and others
Keller 2000 (NEJM) — the exam landmark. In chronic nonpsychotic major depression, 12 weeks of nefazodone, CBASP, or both were compared; combination therapy produced higher response/remission rates than either monotherapy. Nefazodone is largely historical (hepatotoxicity) — the durable teaching is combination of an antidepressant with a depression-focused structured psychotherapy for chronic depression, not the specific commercial molecule.[1]
Schatzberg 2005. Among nonresponders, switching from medication to CBASP or from CBASP to medication can still produce response — do not abandon the alternate modality after one failed track.[2]
CBASP is the named chronic-depression psychotherapy. CBT, IPT and behavioural activation also have roles; Cuijpers meta-analyses support psychotherapy effects in chronic depression/dysthymia, often smaller than in episodic major depression, which is exactly why combination and adequate pharmacology matter.[8][12][16]
Non-response and escalation
Define non-response only after adherence, therapeutic dose and adequate duration are confirmed. Then: switch class, or augment (e.g. lithium under serum-level monitoring; atypical antipsychotic augmentation in selected cases with metabolic/EPS/QTc counselling), or intensify combination psychotherapy. Severe, psychotic or urgently life-threatening chronic depression follows TRD/ECT pathways as for MDD.[10][11]
RANZCP mood disorder guidelines embed chronic depression in formulation-driven stepped care: psychoeducation, psychological therapies, antidepressants, combination, and specialist escalation. Use local Mental Health Act principles for involuntary care when high risk and incapacitous — do not invent section numbers.[10]
Subtypes and scenarios
| Scenario | Key move |
|---|---|
| Pure dysthymia, mild–moderate impairment | Psychoeducation + SSRI adequate trial and/or CBT/IPT/CBASP; measurement-based follow-up |
| Double depression | Treat acute MDE intensity; safety plan; combination treatment early |
| Early-onset + personality traits | Formulate both axes; treat syndrome; consider CBASP interpersonal focus |
| Multiple failed token trials | Rebuild adequate trial definition; check bipolarity, adherence, alcohol |
| High suicide risk chronic depression | Care intensity up; do not normalise chronic passive death wishes |
| Late-life chronic depression | Medical work-up, hyponatraemia caution, consider ECT if severe |
Complications and pitfalls
- Labelling PDD as "personality" and withholding antidepressants or structured therapy.[6][9]
- Token doses (e.g. sertraline 25 mg for 10 days) called "failed SSRI."[4][11]
- Missing bipolarity before years of antidepressant monotherapy.[10]
- Ignoring a superimposed MDE because "baseline PHQ-9 is always 10."[3][13]
- Polypharmacy without formulation or measurement-based care.[10]
- Premature discharge from secondary care while residual chronic symptoms still drive relapse risk.[3][14]
Prognosis and disposition
Naturalistic data show substantial chronicity and high cumulative major-episode rates over a decade. Better outcomes associate with treatment engagement, fewer comorbidities, and achieving true remission rather than "used to it." Disposition ladder: educated primary care with collaborative care for uncomplicated responsive illness; secondary CMHT for diagnostic complexity, high risk, treatment resistance or need for CBASP-level psychotherapy; inpatient care when risk or severity demands it. Functional recovery (work, relationships, self-care) is an outcome equal to scale scores.[3][9][10]
Special populations
Children and adolescents. Duration threshold is 1 year; mood may be irritable. Family involvement, school function, and careful monitoring if an SSRI is used (activation/suicidality) are mandatory. Early-onset PDD warrants developmental and adversity history.[9][10]
Pregnancy and lactation. Untreated chronic depression harms mother and fetus; individualise risk–benefit. Sertraline is a frequently discussed option in perinatal psychiatry contexts with obstetric collaboration; do not stop effective treatment abruptly without a plan.[10][11]
Older adults. Medical comorbidity, polypharmacy, falls, QTc and SSRI hyponatraemia dominate safety; still treat actively — chronic low mood is not normal ageing.[10]
Intellectual disability and cultural formulations. Diagnostic overshadowing is common; use collateral, adapted communication, and culturally safe formulation (FRANZCP cultural safety expectations).[10]
Evidence and guidelines (exam names)
- Keller 2000 NEJM — CBASP vs nefazodone vs combination in chronic depression; combination best.[1]
- Schatzberg 2005 — cross-over efficacy when the other modality failed.[2]
- Klein 2006 — 10-year naturalistic dysthymia/double depression course.[3]
- Thase 1996; Keller 1998 — sertraline/imipramine efficacy in dysthymia and chronic depression.[4][5]
- Levkovitz 2011 — antidepressants beat placebo in dysthymia (meta-analysis).[6]
- Imel 2008 — medication advantage signal in dysthymia vs psychotherapy comparisons.[7]
- Cuijpers 2010 / 2021 — psychotherapy meta-analytic evidence in chronic depression and broader depression therapies.[8][16]
- Schramm 2020 Lancet Psychiatry — modern PDD/dysthymia narrative review.[9]
- RANZCP 2020 mood guidelines; CANMAT 2016 psychological and pharmacological sections; Cipriani 2018 antidepressant NMA for agent selection context; Geddes 2003 maintenance framing.[10][11][12][14][15]
Exam pearls
CHRONIC care checklist
References
- [1]Keller MB, McCullough JP, Klein DN, Arnow B, et al. A comparison of nefazodone, the cognitive behavioral-analysis system of psychotherapy, and their combination for the treatment of chronic depression N Engl J Med, 2000.PMID 10816183
- [2]Schatzberg AF, Rush AJ, Arnow BA, Banks PL, et al. Chronic depression: medication (nefazodone) or psychotherapy (CBASP) is effective when the other is not Arch Gen Psychiatry, 2005.PMID 15867104
- [3]Klein DN, Shankman SA, Rose S Ten-year prospective follow-up study of the naturalistic course of dysthymic disorder and double depression Am J Psychiatry, 2006.PMID 16648329
- [4]Thase ME, Fava M, Halbreich U, Kocsis JH, et al. A placebo-controlled, randomized clinical trial comparing sertraline and imipramine for the treatment of dysthymia Arch Gen Psychiatry, 1996.PMID 8792754
- [5]Keller MB, Gelenberg AJ, Hirschfeld RM, Rush AJ, et al. The treatment of chronic depression, part 2: a double-blind, randomized trial of sertraline and imipramine J Clin Psychiatry, 1998.PMID 9862606
- [6]Levkovitz Y, Tedeschini E, Papakostas GI Efficacy of antidepressants for dysthymia: a meta-analysis of placebo-controlled randomized trials J Clin Psychiatry, 2011.PMID 21527126
- [7]Imel ZE, Malterer MB, McKay KM, Wampold BE A meta-analysis of psychotherapy and medication in unipolar depression and dysthymia J Affect Disord, 2008.PMID 18456340
- [8]Cuijpers P, van Straten A, Schuurmans J, van Oppen P, et al. Psychotherapy for chronic major depression and dysthymia: a meta-analysis Clin Psychol Rev, 2010.PMID 19781837
- [9]Schramm E, Klein DN, Elsaesser M, Furukawa TA, et al. Review of dysthymia and persistent depressive disorder: history, correlates, and clinical implications Lancet Psychiatry, 2020.PMID 32828168
- [10]Malhi GS, Bell E, Bassett D, Boyce P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [11]Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [12]Parikh SV, Quilty LC, Ravitz P, Rosenbluth M, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 2. Psychological Treatments Can J Psychiatry, 2016.PMID 27486150
- [13]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [14]Geddes JR, Carney SM, Davies C, Furukawa TA, et al. Relapse prevention with antidepressant drug treatment in depressive disorders: a systematic review Lancet, 2003.PMID 12606176
- [15]Cipriani A, Furukawa TA, Salanti G, Chaimani A, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis Lancet, 2018.PMID 29477251
- [16]Cuijpers P, Quero S, Noma H, Ciharova M, et al. Psychotherapies for depression: a network meta-analysis covering efficacy, acceptability and long-term outcomes of all main treatment types World Psychiatry, 2021.PMID 34002502