Psych · General adult psychiatry — personality disorders
Personality disorder: ICD-11 dimensional model
Also known as ICD-11 personality disorder · Dimensional personality disorder · Personality disorder severity ICD-11 · Trait domain qualifiers · Borderline pattern ICD-11 · Personality difficulty
Exam-exhaustive fellowship reference on the ICD-11 dimensional model of personality disorder — severity grading (mild/moderate/severe), five trait domain qualifiers, optional borderline pattern, contrast with DSM-5-TR clusters and AMPD, clinical assessment tools, differentials, severity-guided management, and exam pearls. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
The ICD-11 dimensional model is a high-yield nosology topic across FRANZCP, MRCPsych, ABPN and MD/DNB examinations. Examiners test whether you can state the diagnostic sequence (general requirements → severity → traits → optional borderline pattern), contrast it with DSM-5-TR clusters and the Alternative Model for Personality Disorders (AMPD), recode familiar “types” into trait profiles, and link severity to risk, formulation and stepped care without stigma or therapeutic nihilism.[2][12][13]
Overview and definition
Personality disorder in ICD-11 is a pervasive disturbance in how the person experiences and thinks about the self and others, expressed in maladaptive patterns of cognition, emotional experience, emotional expression and behaviour that are relatively inflexible across contexts, have endured over time (typically several years), and are associated with substantial distress or impairment in personal, family, social, educational, occupational or other important areas of functioning. The pattern is not better explained solely by another mental disorder, substance use, medication, or a medical condition, and must be interpreted in cultural context.[1][2][3]
Unlike ICD-10 (and DSM-5-TR Section II categorical types), ICD-11 does not require you to assign one of many named type diagnoses as the primary structure. You diagnose personality disorder (or personality difficulty when subthreshold), then grade how severe the dysfunction is, then describe which trait domains colour the clinical picture. The optional borderline pattern preserves clinical continuity with a well-researched syndrome that clinicians still recognise and for which specialised psychotherapies are organised.[1][3][4]
Personality difficulty sits below the threshold of personality disorder: problematic trait expressions that may cause some interpersonal friction or distress without meeting the full disorder threshold of severity and pervasiveness. It is clinically useful in primary care and for stepped care language, but it is not a substitute for diagnosing moderate or severe PD when criteria are met.[1][8][15]
Classification and nosology
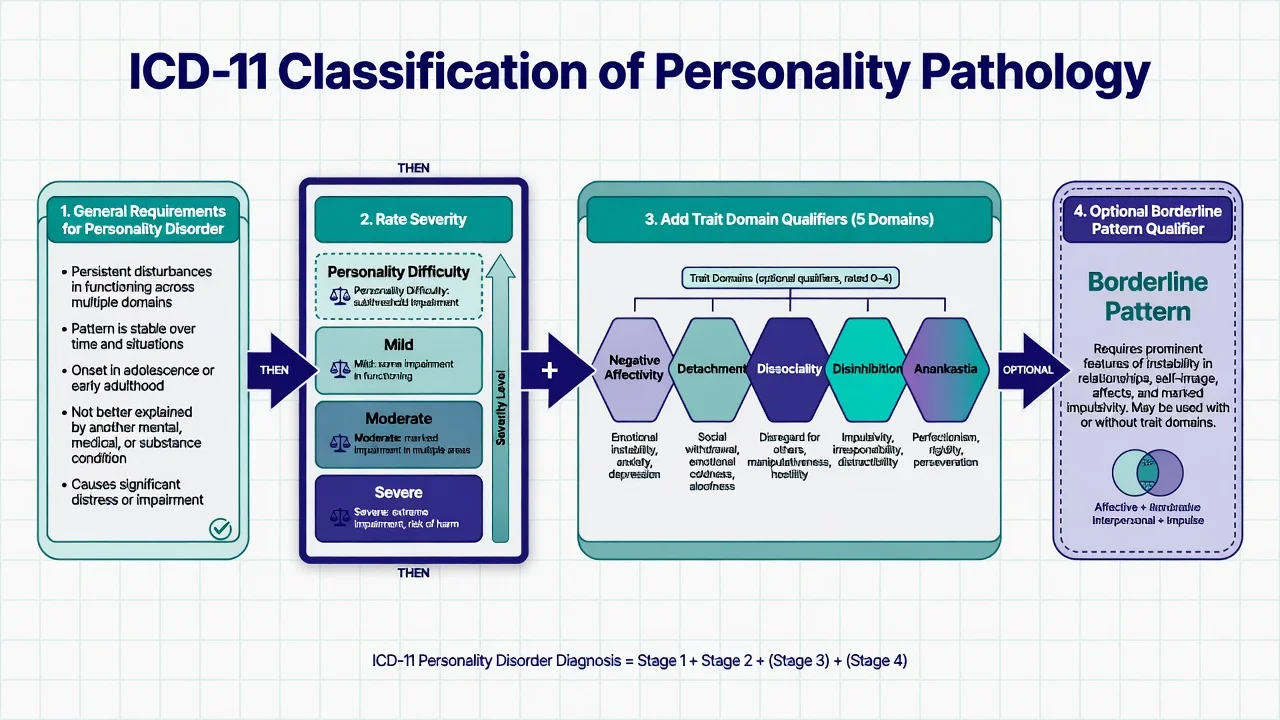
Severity (primary axis)
Severity is the principal clinical decision axis because it correlates with impairment, risk, comorbidity burden and intensity of care. Conceptual work that informed ICD-11 emphasised grading personality pathology by severity rather than multiplying overlapping categorical labels.[1][8]
| Severity | Clinical emphasis (exam-level) |
|---|---|
| Personality difficulty | Subthreshold trait problems; not full PD |
| Mild PD | Disturbance present but some important life areas relatively preserved; interpersonal problems noticeable but not globally catastrophic |
| Moderate PD | Marked problems in multiple domains of self and interpersonal functioning; substantial social/occupational impact; elevated risk behaviours more likely |
| Severe PD | Severe self and interpersonal dysfunction across most contexts; identity coherence often deeply impaired; high risk of harm to self or others; relationships severely compromised |
Severity rests on the degree and pervasiveness of disturbances in self-functioning (identity stability/coherence, self-worth, self-direction/agency) and interpersonal functioning (interest in and capacity for close relationships, understanding others’ perspectives, handling conflict), plus associated emotional, cognitive and behavioural manifestations and overall psychosocial impairment.[3][5][8]
Trait domain qualifiers (style)
After severity, specify one or more prominent trait domains that describe the stylistic expression of pathology:[1][6][9]
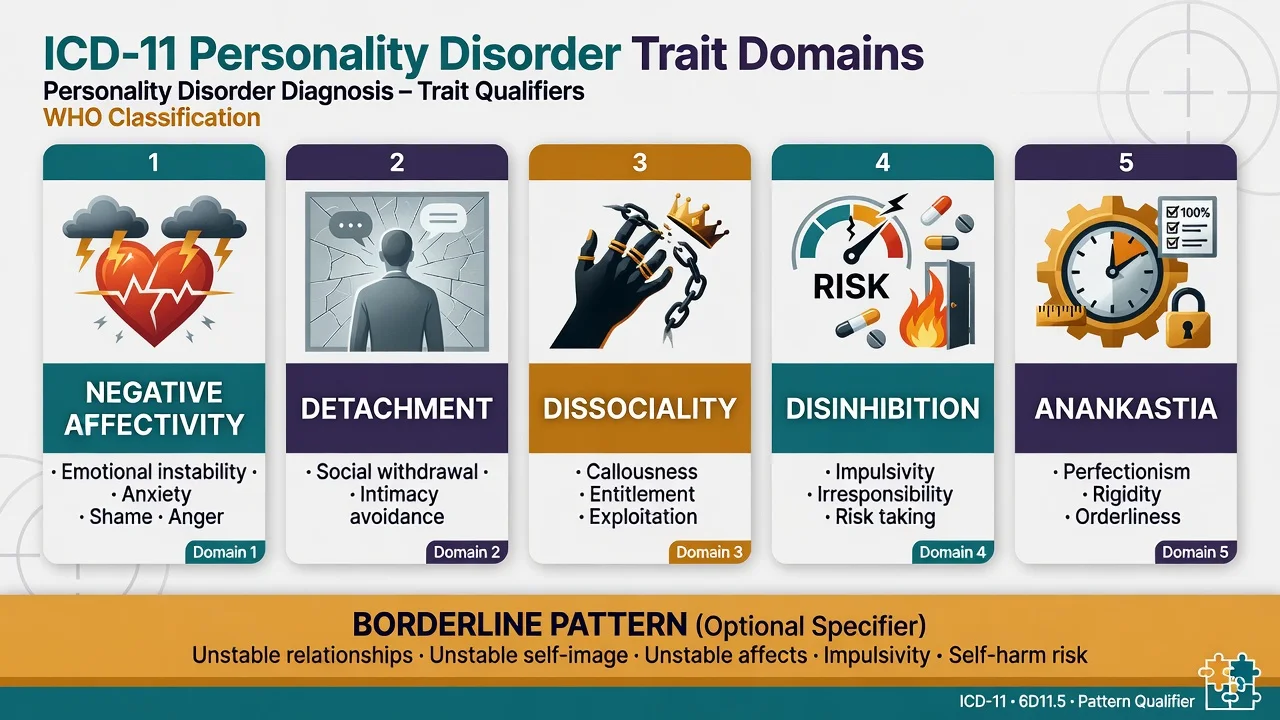
- Negative affectivity — tendency toward a broad range of negative emotions (anxiety, anger, shame, vulnerability, emotional lability) at frequency and intensity out of proportion to the situation.
- Detachment — social and interpersonal withdrawal, emotional aloofness, limited intimate connection.
- Dissociality — disregard for others’ rights and feelings, lack of empathy, entitlement, exploitation, callousness.
- Disinhibition — impulsivity, distractibility, irresponsibility, recklessness, difficulty delaying gratification.
- Anankastia — rigid perfectionism, orderliness, control, stubbornness, and preoccupation with rules or schedules (the ICD-11 home for much of the old anankastic/obsessive-compulsive personality pattern).
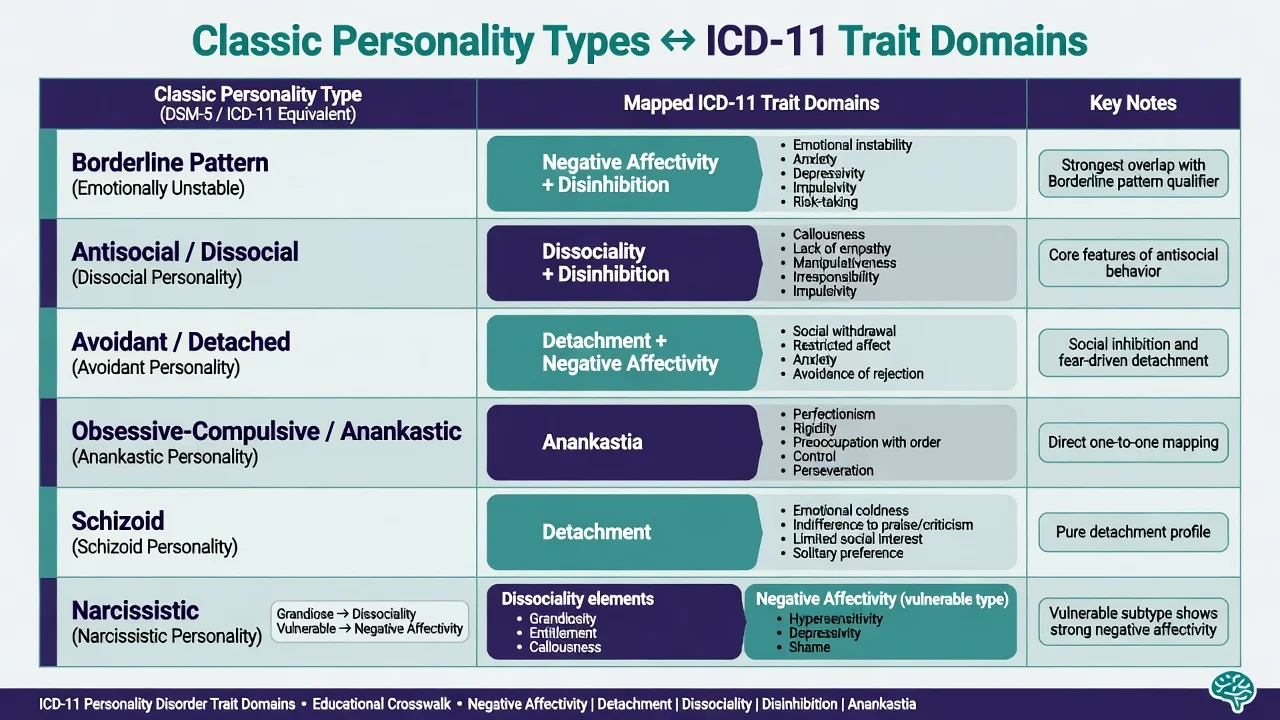
Traits can co-occur. Profiles replace the fiction that patients fit a single pure type. Research has validated the domain structure and shown meaningful crosswalks from older categorical types and DSM-5 trait systems.[6][9][11]
Borderline pattern (optional)
The borderline pattern qualifier captures pervasive instability of interpersonal relationships, self-image and affects, with impulsivity and often self-harm risk — the familiar borderline constellation. It may be used with any severity level when the pattern is prominent. It was retained for clinical utility and continuity of specialised treatment pathways, not because the model is secretly categorical again.[3][4][17]
ICD-11 versus DSM-5-TR and ICD-10
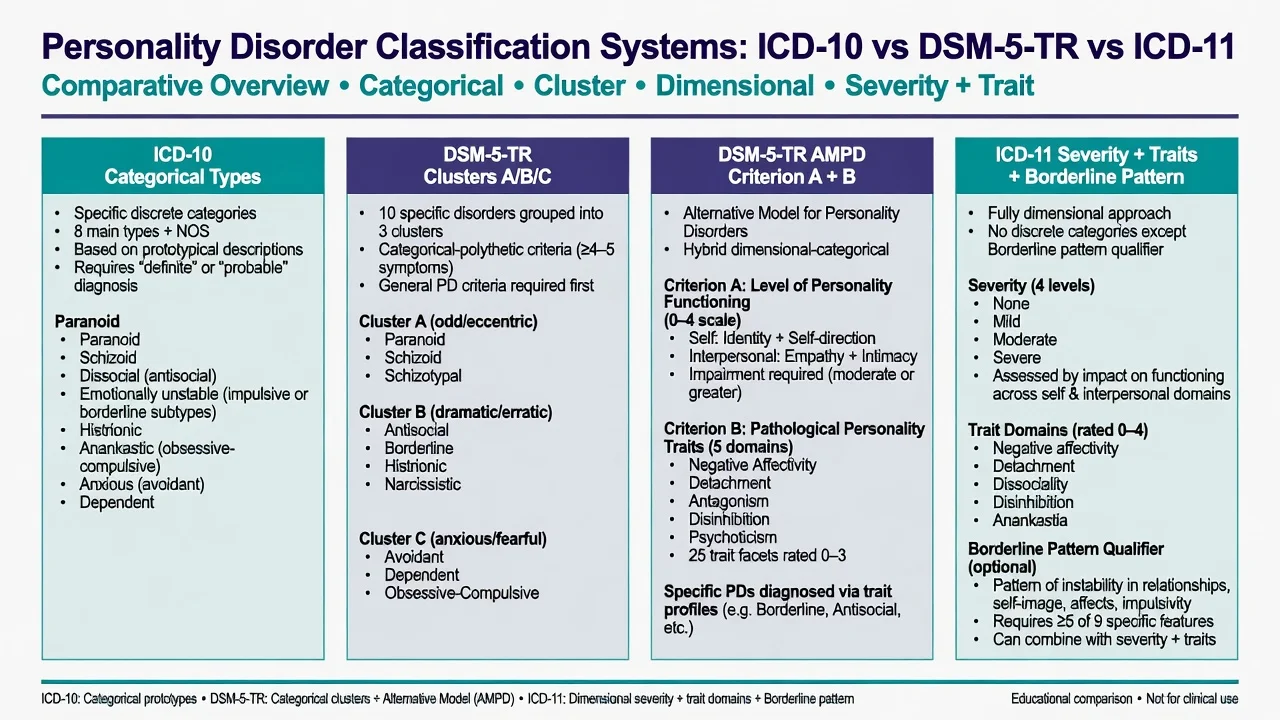
ICD-10
- Multiple categorical F60 types
- Artificial comorbidity common
- Severity implicit, not primary
- Borderline as EUPD subtype
DSM-5-TR Section II
- 10 categorical PDs + clusters A/B/C
- Still dominant in many exam stems
- High overlap and multi-PD coding
- General PD criteria + type checklist
DSM-5-TR AMPD
- Criterion A: level of personality functioning
- Criterion B: pathological traits
- Closest DSM cousin to ICD-11
- Section III — use for formulation even if diagnosis is categorical
ICD-11
- Severity first (mild/moderate/severe)
- Five trait domains + borderline pattern
- One PD diagnosis, richly specified
- Personality difficulty subthreshold option
AMPD alignment. ICD-11 severity and DSM-5-TR AMPD Criterion A both centre on self and interpersonal functioning. ICD-11 trait domains harmonise substantially with AMPD pathological traits (with naming differences — e.g. dissociality ~ antagonism; anankastia related to compulsivity/rigid perfectionism constructs).[6][16]
Epidemiology and risk factors
Community estimates of personality disorder vary with instrument, threshold and whether subthreshold difficulty is counted. Classic teaching puts community PD prevalence in a broad band (often cited around the mid-single to low-double-digit percent range depending on method), with much higher enrichment in secondary and tertiary mental health services. ICD-11-oriented general population work using severity metrics produces graded rates for mild, moderate and severe levels rather than a single binary prevalence figure.[15][1][4]
Epidemiology framing for exams
Risk and aetiological factors. Childhood adversity and trauma, chronic invalidation, attachment disruption, temperamental emotional intensity or impulsivity, and heritable contributions to trait extremes all feature. Trauma is common in high-severity and borderline-pattern presentations but is neither necessary nor sufficient for a PD diagnosis, and complex PTSD can co-occur without collapsing into a single label.[14][17]
Pathophysiology and mechanisms
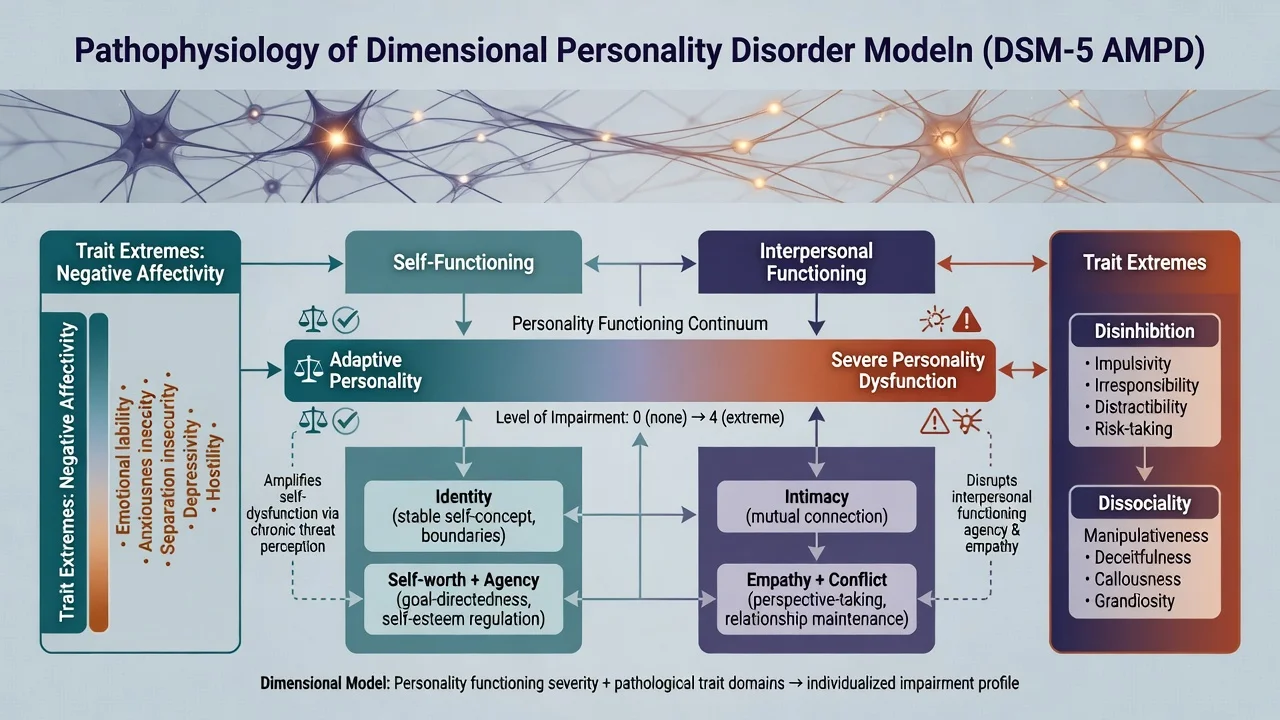
The dimensional model assumes continuity with normal personality variation: pathological traits are maladaptive extremes of temperamental dimensions related to the Big Five tradition (e.g. negative affectivity with neuroticism; detachment with low extraversion; dissociality with low agreeableness; disinhibition with low conscientiousness; anankastia with high orderliness/conscientiousness extremes).[1][7][9]
Core dysfunction. Severity is not a sum of checklist symptoms alone — it is the extent to which self (who I am, what I am worth, whether I can direct my life) and interpersonal capacities (intimacy, empathy, conflict) are reliably available under stress. This framing unifies otherwise heterogeneous “types.”[5][8][16]
Amplifying mechanisms. Attachment insecurity and mentalizing failures under interpersonal stress, biosocial emotion dysregulation (high sensitivity × invalidating environments), and maladaptive schemas convert trait vulnerability into disorder-level impairment — especially relevant when negative affectivity, disinhibition and borderline pattern co-occur.[17][12]
Neurobiology remains group-level (frontolimbic regulatory imbalance, impulsivity circuitry, stress-axis sensitivity in some severe presentations). Imaging and biomarkers do not diagnose PD in an individual patient.[17]
Clinical presentation
Presentations are best described along severity × trait profile, not only by legacy type names.[3][11]
By severity. Mild PD may present as recurrent relationship friction, workplace conflict, or chronic low-grade distress with some preserved functioning. Moderate PD typically shows multi-domain impairment, repeated crises or treatment drop-out, and substantial disability. Severe PD presents with global identity and relationship breakdown, high self-harm or aggression risk, and near-constant interpersonal chaos or profound isolation depending on trait mix.[3][8][15]
By trait emphasis.
- High negative affectivity ± disinhibition ± borderline pattern: affective storms, abandonment crises, self-harm, unstable relationships.
- High detachment: aloofness, limited desire for intimacy, restricted affect — may be misread as depression or autism if developmental history is thin.
- High dissociality: exploitation, remorselessness, entitlement — forensic interface common.
- High anankastia: rigidity, perfectionism, control — overlap with OCD traits but personality-pervasive.
- Mixed profiles are expected; pure single-domain cases are the exception.[11][20][6]
Crisis versus quiet presentations. Emergency settings over-sample high negative affectivity/disinhibition/borderline pattern. Outpatient clinics also see chronic emptiness, work instability, serial short therapies, and high-anankastia presentations that rarely “look like BPD” but still meet severity thresholds.[17][12]
Differential diagnosis
Mood episodes
- Bipolar: days–weeks episodes; reduced sleep need with energy
- MDD: pervasive low mood/anhedonia episode structure
- PD affective shifts often hours–days, interpersonal-triggered
- Comorbidity allowed — dual diagnosis when both met
Trauma disorders
- PTSD: trauma-specific re-experiencing, avoidance, hyperarousal
- Complex PTSD: disturbances in self-organisation after prolonged trauma
- May co-occur with PD / borderline pattern
- Do not force either/or when both criteria apply
Neurodevelopmental
- ADHD: childhood-onset inattention/hyperactivity across settings
- Autism: lifelong social communication differences, restricted interests
- Rejection sensitivity can mimic interpersonal storms
- Formulate developmental timeline carefully
Organic / substance
- Late-onset personality change is a red flag
- TBI, FTD, epilepsy, endocrine disease
- Intoxication/withdrawal mimic disinhibition and aggression
- UDS, collateral, imaging/EEG when indicated
Also keep psychotic disorders, OCD (vs anankastia), and “difficult interpersonal behaviour under acute stress without longitudinal PD criteria” on the board. Personality difficulty is the correct label when impairment is real but below PD threshold — not every conflictual patient has moderate PD.[3][13][14]
Clinical and bedside assessment
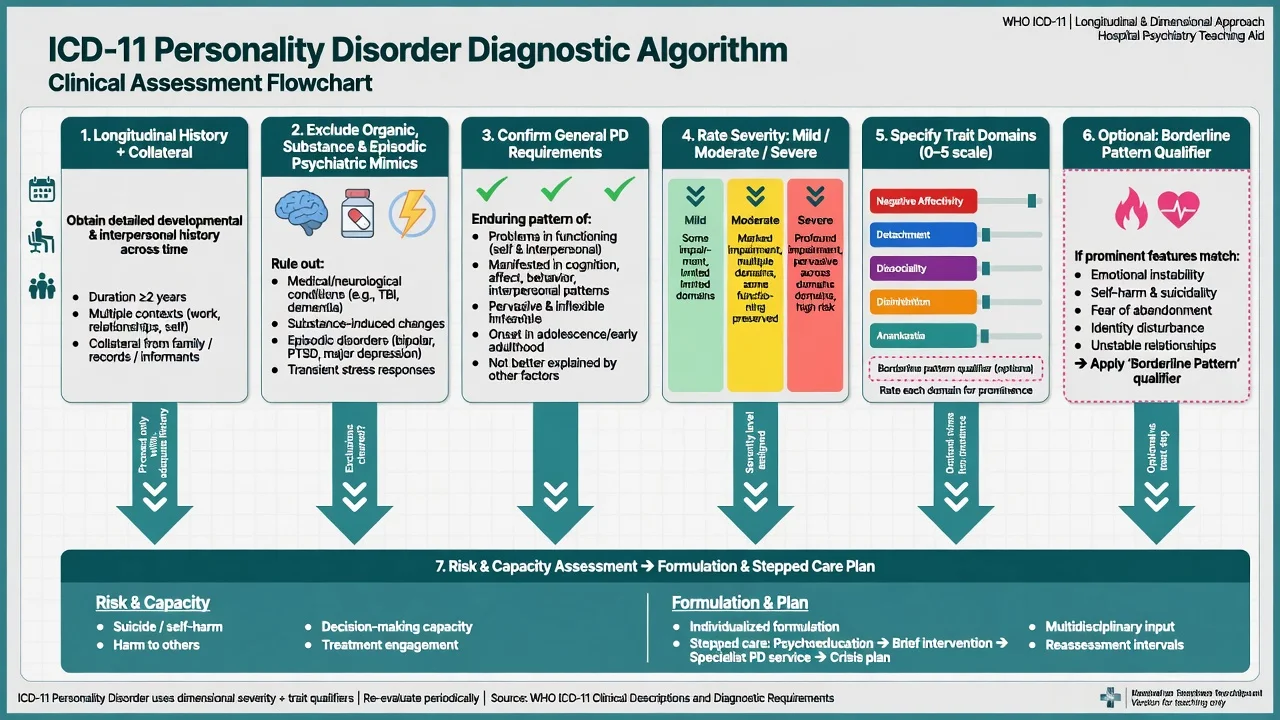
Recommended viva order.
- Longitudinal developmental and interpersonal history across contexts.
- Collateral and cultural formulation.
- Exclude or co-diagnose organic, substance, and episodic psychiatric disorders.
- Confirm general requirements for PD.
- Rate severity (mild / moderate / severe).
- Specify trait domains that are prominent.
- Add borderline pattern if clinically justified.
- Risk (suicide, self-harm, violence, vulnerability), capacity, safeguarding, and formulation linking severity + traits to a care plan.[3][4][12]
Mental State Examination. Identity coherence and self-worth themes, interpersonal stance (idealisation/devaluation, detachment, entitlement), affect range and reactivity, impulsivity cues, transient stress-related paranoia or dissociation, insight, alliance quality, and risk. Document both chronic baseline risk and today’s acute change.[17]
Tools (conceptual, not gold standards).
- PDS-ICD-11 — self-report severity aligned to ICD-11 severity construct.
- PiCD (Personality Inventory for ICD-11) — trait domain measurement.
- Brief screens (e.g. SAPAS-style approaches) for busy clinics — screening ≠ diagnosis.
- AMPD/LPFS and DSM trait inventories help when services still use DSM language but you want dimensional formulation.[5][7][16]
Clinicians in utility studies have often rated ICD-11 as more clinically useful than ICD-10 categorical typing for communication and treatment planning — a point worth stating at viva when asked “why change?”.[10]
Investigations
PD is a clinical diagnosis. There is no laboratory or imaging gold standard. Investigate to exclude mimics and to prepare for medication when used: TSH, FBC, U&E, LFT, glucose/lipids and BMI if antipsychotics considered, pregnancy test when relevant, urine drug screen when substances may explain behaviour, ECG when cardiac risk or QTc-risk drugs are planned. Neuroimaging or EEG when late-onset change, focal neurology, seizures or cognitive decline fire. Screen systematically for bipolar spectrum, PTSD, ADHD, eating disorders and substance use disorders because they change management.[17][19]
Management — acute crisis and resuscitation
Severity labels never replace dynamic risk assessment. Medical stabilisation of overdose or injury comes first. Then assess ideation, intent, plan, means, protective factors, impulsivity, substances, and the interpersonal trigger. Validate emotion without validating unsafe behaviour; co-create a time-limited safety plan; restrict means; use least-restrictive disposition; name a follow-up clinician. Legal status is jurisdiction-specific — state principles (imminent risk, incapacity, least restrictive care) without inventing section numbers for the wrong country.[17][4]
Management — definitive and stepwise
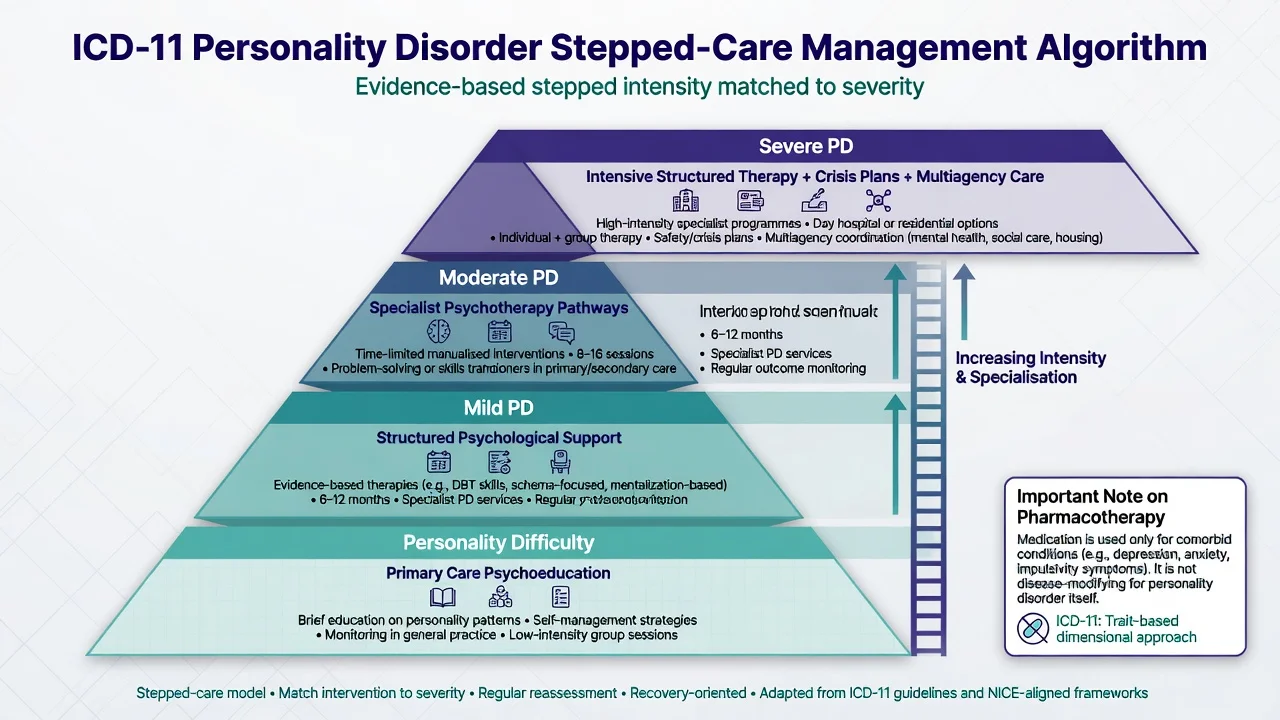
Severity guides intensity; traits guide focus
| Severity | Typical care intensity (principle) |
|---|---|
| Personality difficulty | Psychoeducation, primary care psychological support, problem-solving |
| Mild PD | Structured psychological intervention; limited specialist input |
| Moderate PD | Specialist structured psychotherapy pathway; care coordination |
| Severe PD | Intensive structured therapy access, crisis planning, multiagency support, possible brief admissions for uncontainable risk |
Traits shape the interpersonal process: mentalizing and emotion regulation work for high negative affectivity/disinhibition; behavioural boundaries and victim-safety frameworks for high dissociality; behavioural activation and social connection for high detachment; flexibility work for high anankastia.[3][12][4]
Psychotherapy first-line for moderate–severe PD / borderline pattern
The strongest randomised evidence base for specialised PD treatment remains organised around borderline presentations (high negative affectivity, disinhibition, borderline pattern). Meta-analysis supports specialised psychotherapies over control conditions for borderline pathology. Name at least one model fully in exams:[18][17]
- DBT — individual therapy, skills group, coaching where available, consultation team; hierarchy prioritises life-threatening behaviours.
- MBT — restore mentalizing under attachment arousal.
- Schema therapy / TFP — schemas/modes or identity diffusion and transference work.
- General psychiatric management / structured clinical management — structured, consistent care when specialised brands are unavailable (not “nothing”).
Pharmacotherapy — comorbidity and short targets only
No medication is established as disease-modifying treatment of personality disorder as a whole. For the best-studied severe pattern (borderline), Cochrane synthesis shows limited and uncertain benefits of pharmacological interventions for core psychopathology; NICE-aligned teaching warns against drug treatment as primary therapy for BPD itself while allowing treatment of comorbidity and short-term crisis use under review.[19][17]
Treat comorbid major depression, bipolar disorder, PTSD, ADHD, anxiety and substance use with the same standards as outside PD. Any symptom-targeted psychotropic trial needs a written target symptom, baseline safety checks (e.g. metabolic/ECG when relevant), and a review/stop date. Avoid chronic benzodiazepines for emotion regulation and unreviewed polypharmacy.[19][17]
Example when an examiner forces a named comorbid plan (individualise; check product information). For confirmed comorbid major depression without bipolarity after safety review of overdose risk: sertraline 50 mg orally daily, early review for activation/suicidality, titrate toward 50–150 mg as tolerated with limited dispensing if overdose risk is high — this treats depression, not “the personality.”[19]
ICD-11 adoption and dimensional formulation fit RANZCP-aligned teaching that prioritises formulation, risk, cultural safety and access to structured therapies. Local Mental Health Acts govern involuntary care — principles, not borrowed section numbers.[4][12]
Specific subtypes and scenarios
Borderline pattern, moderate–severe. Highest exam density: self-harm, abandonment crises, dual diagnosis with mood/trauma/substance. Psychotherapy-first; dynamic risk; avoid polypharmacy-as-care.[17][18]
High dissociality. Rights violations, lack of remorse, exploitation. Risk to others and victim safety; forensic interfaces; do not use diagnosis alone as risk score.[11][3]
High anankastia. Perfectionism and control; distinguish from OCD (ego-dystonic obsessions/compulsions vs ego-syntonic personality style). Can still cause severe occupational impairment at high severity.[11][6]
High detachment. Isolation may mask depression or autism; timeline and developmental history decide.[11][3]
Narcissistic presentations. Grandiose and vulnerable narcissism recode as severity plus trait mixtures (often dissociality elements with negative affectivity in vulnerable presentations) rather than a standalone ICD-11 type.[20][11]
Adolescents. Diagnosis is allowed when requirements are met; early structured intervention is preferred to “wait until 18.” Developmental formulation and family work matter.[17][14]
Personality difficulty in primary care. Brief psychological support and watchful waiting for escalation; do not medicalise ordinary interpersonal conflict, but do not miss evolving moderate PD with rising self-harm.[1][8][15]
Complications and pitfalls
Classic failures: stigma and diagnostic overshadowing; missing organic late-onset change; multiplying legacy PD labels as if that explains more than severity does; declaring untreatable because a branded therapy is waitlisted while omitting structured clinical management; polypharmacy without targets; using trait words pejoratively (“dissocial” as insult rather than formulation); under-rating severity in quiet high-anankastia or high-detachment patients who never present in ED.[10][13][14]
Prognosis and disposition
Severity is a better anchor for prognosis and service intensity than type name alone. Many people with high-severity borderline-pattern pathology show substantial symptomatic improvement over years in longitudinal cohorts, though functional recovery (work, relationships) often lags. Reassess severity over time as an outcome metric after therapy. Disposition ladder: primary care/structured support → specialist psychotherapy → day programs → brief crisis admission for uncontainable risk → longer inpatient only when necessary and with a discharge plan from day one.[17][8][4]
Special populations
Pregnancy and parenting. Collaborative risk–benefit decisions; minimise teratogenic polypharmacy; support attachment and safeguarding; coordinate perinatal mental health when available.[17]
Older adults. Trait intensity may attenuate, but depression, loneliness and self-harm can persist. New-onset “personality change” in late life is organic or mood disease until proven otherwise.[14]
Cultural formulation. Idioms of distress, family structures and discrimination shape presentation and help-seeking. In ANZ practice, cultural safety and Indigenous health frameworks are part of competent care.[4]
Intellectual disability and neurodiversity. Adaptive behaviour baselines differ; avoid mislabeling developmental difference as PD, and avoid missing true personality dysfunction when it coexists.[4][14]
Evidence, guidelines and controversies
Nosology development. Tyrer, Mulder and colleagues describe ICD-11 PD classification as a deliberate shift toward severity plus limited trait domains after decades of categorical failure modes (overlap, artificial comorbidity, weak boundaries).[1][8][9] Reed and colleagues summarise broader ICD-11 mental disorders innovations including dimensionalisation where justified.[2]
Clinical application and utility. Bach and First provide practical application guidance; European perspective papers and clinician utility studies support feasibility and often greater usefulness than ICD-10 typing.[3][4][10][12]
Measurement. PDS-ICD-11 operationalises severity; PiCD operationalises traits; DSM-5 trait crosswalk studies support harmonisation attempts with AMPD.[5][7][6][16]
Treatment evidence remains richest for borderline-pattern presentations: psychotherapy meta-analysis and Cochrane pharmacotherapy updates should be cited when examiners ask “does the new model change treatment?” — the answer is that severity better matches intensity of care, while evidence-based psychotherapy still leads for moderate–severe emotion-dysregulation presentations.[18][19][17]
Controversies for mature discussion. Loss of familiar type names; whether borderline pattern undermines dimensional purity; resource implications of specialised therapy access; coexistence of DSM categorical coding with ICD-11 formulation in dual-system jurisdictions; risk of under-identifying high-dissociality pathology if services only train on borderline pathways.[13][14][20]
Exam pearls
SEVERITY — ICD-11 viva order
SEVERITY
Self and interpersonal dysfunction is the core of severity
Exclude organic, substance and episodic mimics first
Verify general PD requirements (pervasive, enduring, impairing)
Estimate severity: mild / moderate / severe (or difficulty)
Record trait domains (N-D-D-D-A)
Include borderline pattern only if clinically justified
Treatment intensity follows severity; traits guide focus
Yes to hope — structured therapy, not nihilism or polypharmacy
60-second oral summary
ICD-11 diagnoses personality disorder by confirming pervasive self and interpersonal dysfunction, then grading severity (mild/moderate/severe), then specifying trait domains (negative affectivity, detachment, dissociality, disinhibition, anankastia), with optional borderline pattern. This replaces multi-type ICD-10 stacking and aligns with DSM AMPD thinking. Severity drives risk and care intensity; traits drive interpersonal style and therapy focus. Exclude organic, substance and episodic mimics. First-line care for moderate–severe presentations is structured psychotherapy; medication treats comorbidity or short targets with review dates — not the disorder as a whole. Hope and structure beat stigma and polypharmacy.[1][3][18][19]
References
- [1]Tyrer P, Mulder R, Kim YR, Crawford MJ The Development of the ICD-11 Classification of Personality Disorders: An Amalgam of Science, Pragmatism, and Politics Annu Rev Clin Psychol, 2019.PMID 30601688
- [2]Reed GM, First MB, Kogan CS, et al. Innovations and changes in the ICD-11 classification of mental, behavioural and neurodevelopmental disorders World Psychiatry, 2019.PMID 30600616
- [3]Bach B, First MB Application of the ICD-11 classification of personality disorders BMC Psychiatry, 2018.PMID 30373564
- [4]Bach B, Kramer U, Doering S, et al. The ICD-11 classification of personality disorders: a European perspective on challenges and opportunities Borderline Personal Disord Emot Dysregul, 2022.PMID 35361271
- [5]Bach B, Brown TA, Mulder RT, et al. Development and initial evaluation of the ICD-11 personality disorder severity scale: PDS-ICD-11 Personal Ment Health, 2021.PMID 34002530
- [6]Bach B, Sellbom M, Kongerslev M, et al. Deriving ICD-11 personality disorder domains from dsm-5 traits: initial attempt to harmonize two diagnostic systems Acta Psychiatr Scand, 2017.PMID 28504853
- [7]Oltmanns JR, Widiger TA A self-report measure for the ICD-11 dimensional trait model proposal: The personality inventory for ICD-11 Psychol Assess, 2018.PMID 28230410
- [8]Crawford MJ, Koldobsky N, Mulder R, Tyrer P Classifying personality disorder according to severity J Pers Disord, 2011.PMID 21699394
- [9]Mulder RT, Horwood J, Tyrer P, et al. Validating the proposed ICD-11 domains Personal Ment Health, 2016.PMID 27120419
- [10]Hansen SJ, Christensen S, Kongerslev MT, et al. Mental health professionals' perceived clinical utility of the ICD-10 vs. ICD-11 classification of personality disorders Personal Ment Health, 2019.PMID 30989832
- [11]Simon J, Lambrecht B, Bach B Cross-walking personality disorder types to ICD-11 trait domains: An overview of current findings Front Psychiatry, 2023.PMID 37091704
- [12]Swales MA Personality Disorder Diagnoses in ICD-11: Transforming Conceptualisations and Practice Clin Psychol Eur, 2022.PMID 36760321
- [13]Huprich SK Personality Disorders in the ICD-11: Opportunities and Challenges for Advancing the Diagnosis of Personality Pathology Curr Psychiatry Rep, 2020.PMID 32519211
- [14]Herpertz SC, Huprich SK, Bohus M, et al. The Challenge of Transforming the Diagnostic System of Personality Disorders J Pers Disord, 2017.PMID 28910213
- [15]Bach B, Simonsen E, Kongerslev MT, et al. ICD-11 personality disorder features in the danish general population: Cut-offs and prevalence rates for severity levels Psychiatry Res, 2023.PMID 37748238
- [16]Morey LC, McCredie MN, Bender DS, et al. Criterion A: Level of personality functioning in the alternative DSM-5 model for personality disorders Personal Disord, 2022.PMID 35787111
- [17]Bohus M, Stoffers-Winterling J, Sharp C, et al. Borderline personality disorder Lancet, 2021.PMID 34688371
- [18]Cristea IA, Gentili C, Cotet CD, et al. Efficacy of Psychotherapies for Borderline Personality Disorder: A Systematic Review and Meta-analysis JAMA Psychiatry, 2017.PMID 28249086
- [19]Stoffers-Winterling JM, Storebø OJ, Pereira Ribeiro J, et al. Pharmacological interventions for people with borderline personality disorder Cochrane Database Syst Rev, 2022.PMID 36375174
- [20]Day NJS, Green A, Denmeade G, et al. Narcissistic personality disorder in the ICD-11: Severity and trait profiles of grandiosity and vulnerability J Clin Psychol, 2024.PMID 38742471