Psych · General adult psychiatry — feeding and eating disorders
Pica and rumination disorder
Also known as Pica · Rumination disorder · Rumination syndrome · Geophagia · Pagophagia · Amylophagia · Trichophagia · PARDI · Diaphragmatic breathing for rumination
Exam-exhaustive fellowship reference on pica and rumination disorder — DSM-5-TR/ICD-11 criteria, medical complications (lead, bezoar, malnutrition), iron and zinc associations, PARDI assessment, behavioural management in ID/ASD, diaphragmatic breathing and biofeedback, baclofen for refractory rumination, pregnancy and cultural formulation. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Pica and rumination disorder are high-yield boundary and medical-risk topics at the psychiatry–gastroenterology–intellectual disability interface. FRANZCP MEQs test discrimination from bulimia nervosa and GORD, medical complications, and behavioural first-line care. MRCPsych CASCs test explanation of diaphragmatic breathing and carer safety planning. ABPN items test DSM criteria, substance-specific toxicity, and baclofen positioning. A candidate who reads only this topic should defend diagnosis, risk, and stepped care at consultant depth.[2][9][11]
Overview and definition
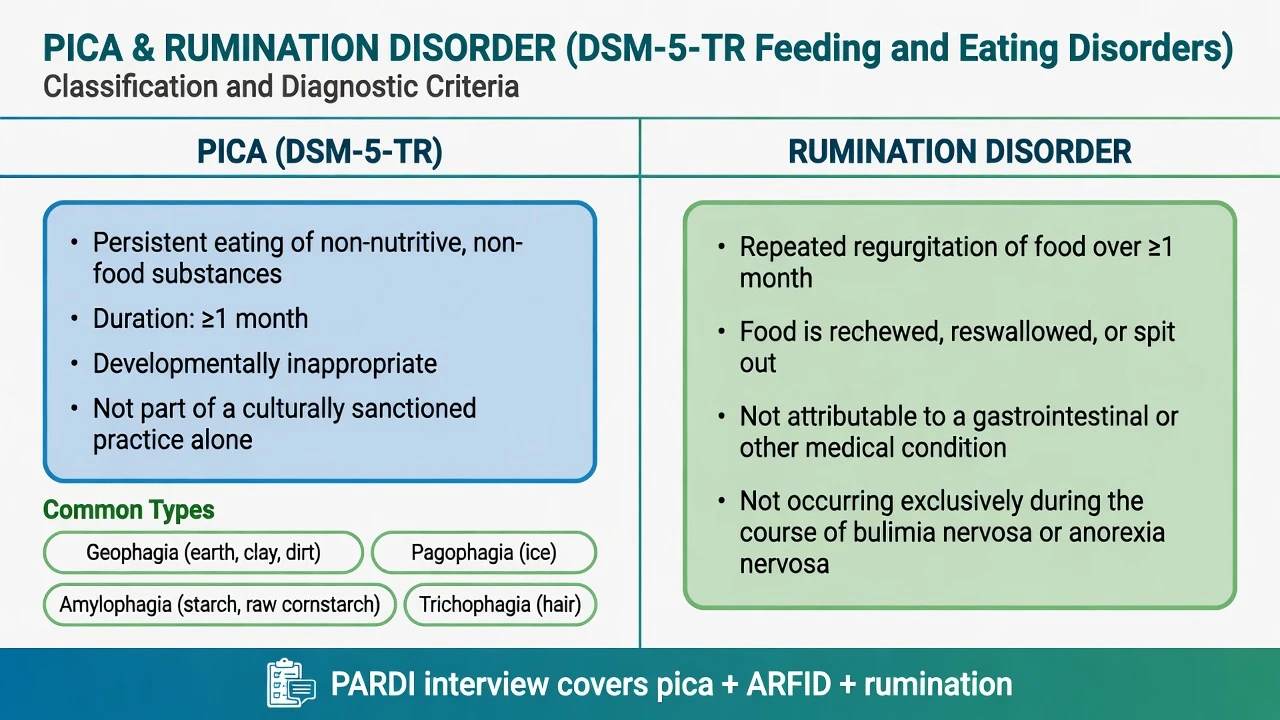
Pica (DSM-5-TR). Persistent eating of non-nutritive, non-food substances for at least 1 month. The behaviour is inappropriate to the developmental level of the individual and is not part of a culturally supported or socially normative practice. If the eating behaviour occurs in the context of another mental disorder (for example autism spectrum disorder or intellectual disability) or medical condition (including pregnancy), it is sufficiently severe to warrant additional clinical attention.[1][2]
Rumination disorder (DSM-5-TR). Repeated regurgitation of food for at least 1 month. Regurgitated food may be rechewed, reswallowed, or spit out. The behaviour is not attributable to an associated gastrointestinal or other medical condition (or exceeds what that condition would explain), and does not occur exclusively during the course of anorexia nervosa, bulimia nervosa, binge-eating disorder, or ARFID — or, if concurrent, is sufficiently severe to warrant additional clinical attention.[9][11][12]
Clinical essence for viva. Pica is defined by what is ingested (non-food) and its developmental/cultural framing. Rumination is defined by effortless postprandial regurgitation physiology, not by reverse-peristaltic vomiting with nausea and retching.[9][11]
ICD-11 and Rome IV. ICD-11 places analogous feeding and eating disorder constructs; always declare the manual used. Gastroenterology colleagues often use Rome IV rumination syndrome criteria for the same clinical phenomenon — psychiatry and GI language should be translated, not treated as mutually exclusive diagnoses of different diseases.[9][11]
Classification and clinical presentations

Pica substance types
- Geophagia — earth, clay, soil
- Pagophagia — ice (classic with iron deficiency)
- Amylophagia — starch/laundry starch
- Trichophagia — hair (trichobezoar risk)
- Others — paper, paint chips, chalk, faeces, glass
Rumination features
- Effortless regurgitation during/after meals
- Often within minutes of eating
- Rechew, reswallow, or spit
- Nausea/retching typically absent or minimal
- May be secretive; weight loss if food expelled
Not these diagnoses alone
- Developmental mouthing under age threshold
- Cultural geophagy without impairment criteria
- BN purging for shape/weight control
- GORD/vomiting syndromes without rumination physiology
- Depressive cognitive 'rumination' (thinking style)
Epidemiology and risk factors
Headline epidemiology (exam framing)
Population estimates vary by instrument, age, and setting. German population-based work documents pica and rumination behaviours in school-age children and in adults with associations to broader feeding/eating and general psychopathology — use these series for order-of-magnitude teaching rather than a single global percentage.[6][7] Clinical risk concentrates in intellectual disability, autism, pregnancy (especially with iron deficiency), and early childhood when supervision is limited.[1][2]
Micronutrients. Meta-analysis shows pica is significantly associated with increased risk of anaemia and lower haemoglobin/haematocrit and plasma zinc; direction of causality is not settled — deficiency may drive craving, and some substances may worsen absorption or displace diet.[3][5] In non-pregnant adults with iron deficiency or depletion, younger age associates with pica, and pagophagia is a classic clinical clue.[4]
Pathophysiology and maintaining model
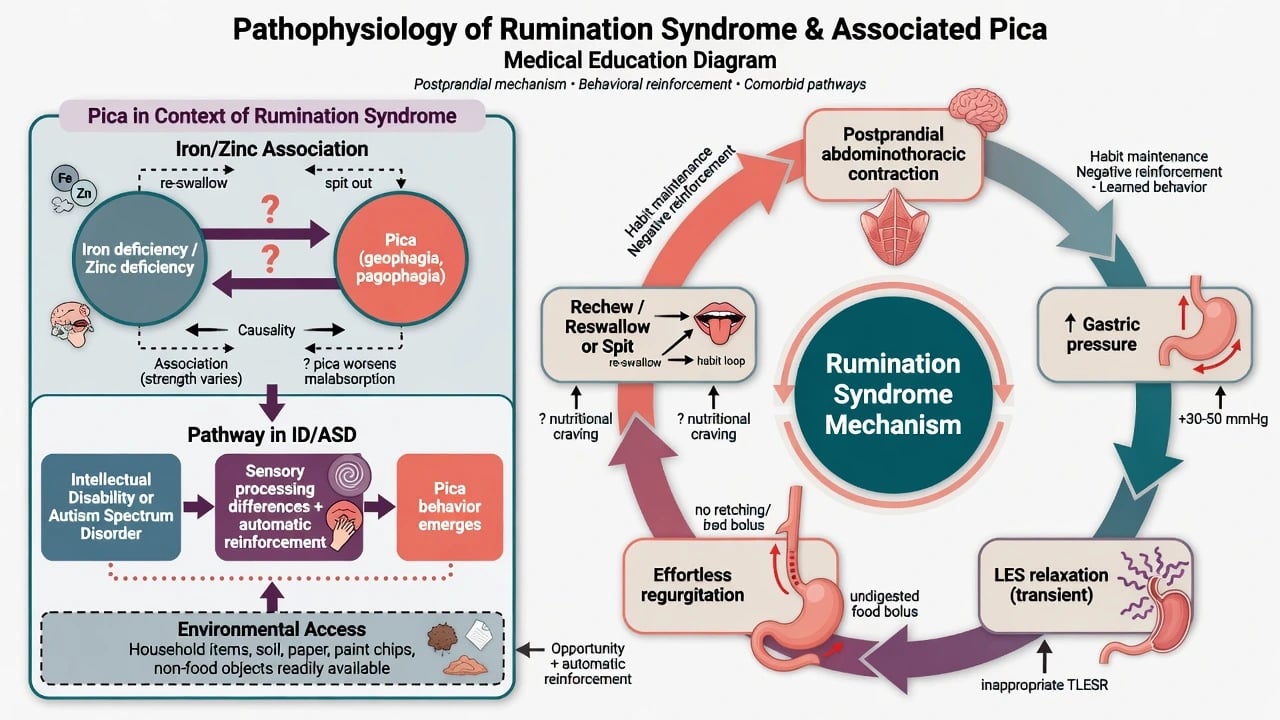
Rumination mechanism (viva-ready). After meals, learned or automatic abdominothoracic muscular contraction raises intragastric pressure. With lower oesophageal sphincter relaxation, gastric contents move effortlessly into the oesophagus and mouth. Food may be reswallowed (maintaining the habit with less social cost) or expelled (nutritional loss). This is not the reverse-peristalsis physiology of vomiting.[9][10][11] Diaphragmatic breathing competes with the abdominothoracic strain pattern and is the mechanistic basis of first-line behavioural treatment.[10]
Pica mechanisms. Multifactorial: automatic and sensory-reinforced behaviour in ID/ASD; association with iron (and zinc) deficiency; cultural geophagy in some communities; environmental access; and, historically, deprivation contexts. Lead and other toxins enter when the substance is contaminated paint, soil, or industrial material.[1][2][3]
Clinical presentation
Pica. Collateral often outperforms self-report. Map substance type (toxicity risk), frequency, secrecy, onset, developmental level, pregnancy status, residential supervision, and prior surgical or lead complications. Pagophagia (ice) is a classic bedside clue to iron deficiency; geophagia and amylophagia have cultural and pregnancy associations; trichophagia raises bezoar concern.[1][2][5]
Rumination. Effortless regurgitation during or soon after meals, often within the first half-hour, with rechewing or reswallowing. Patients may describe “food coming up” without preceding nausea. Weight loss, dental enamel injury, and social avoidance of meals occur when food is expelled. Many have been treated for years as “reflux” without response to acid suppression alone.[9][11][12]
MSE language. Shame and minimisation are common. Explicitly screen fear of fatness and body-image overvaluation so BN is not missed or overcalled. Screen suicide risk when mood disorder coexists, and screen self-injury when pica is embedded in challenging behaviour plans.[6][15]
Differential diagnosis
Bulimia nervosa
- Regurgitation/purging driven by shape/weight control
- Binge–purge cycle, body-image overvaluation
- Rumination lacks thinness drive as primary motive
- Can co-occur — dual formulate if both present
Vomiting / GORD / gastroparesis
- Vomiting: nausea, retching, pallor, forceful expulsion
- GORD: heartburn, acid, response pattern to PPI
- Rumination: effortless, meal-linked, often reswallowed
- Investigate organic red flags before pure behavioural label
Developmental / cultural
- Mouthing in infants/toddlers may be age-appropriate
- Cultural geophagy may be normative practice
- DSM requires developmental inappropriateness and non-cultural framing
- Still assess medical risk of the substance
Psychosis / safeguarding
- Command hallucinations driving ingestion
- Factitious or imposed illness rare but examinable
- Inconsistent history, multiple unexplained presentations
- Safeguarding pathway when indicated
Also discriminate ARFID (avoidant/restrictive intake without non-food ingestion as the core), medical dysphagia, and cognitive rumination (repetitive negative thinking) which shares only the English word.[8][15]
Clinical and bedside assessment
History structure. Substance inventory and access map (pica); meal timing, effortlessness, rechew/reswallow (rumination); weight trajectory; GI symptoms and prior endoscopy/PPI trials; pregnancy; ID/ASD supports; body-image and binge screen; social/occupational meal impact; prior bezoar/lead/surgery.[1][9]
Physical exam. BMI/growth; abdominal exam (mass, tenderness, obstruction signs); dentition; nutritional and neurological exam if lead risk; vitals if underweight or dehydrated.[1][12]
Structured tools. The PARDI (Pica, ARFID and Rumination Disorder Interview) is a multi-informant semi-structured interview developed for feeding disorders including pica and rumination across the lifespan (pilot validation in youth).[8] Clinical diagnosis remains primary; PARDI structures thoroughness rather than replacing medical risk assessment.
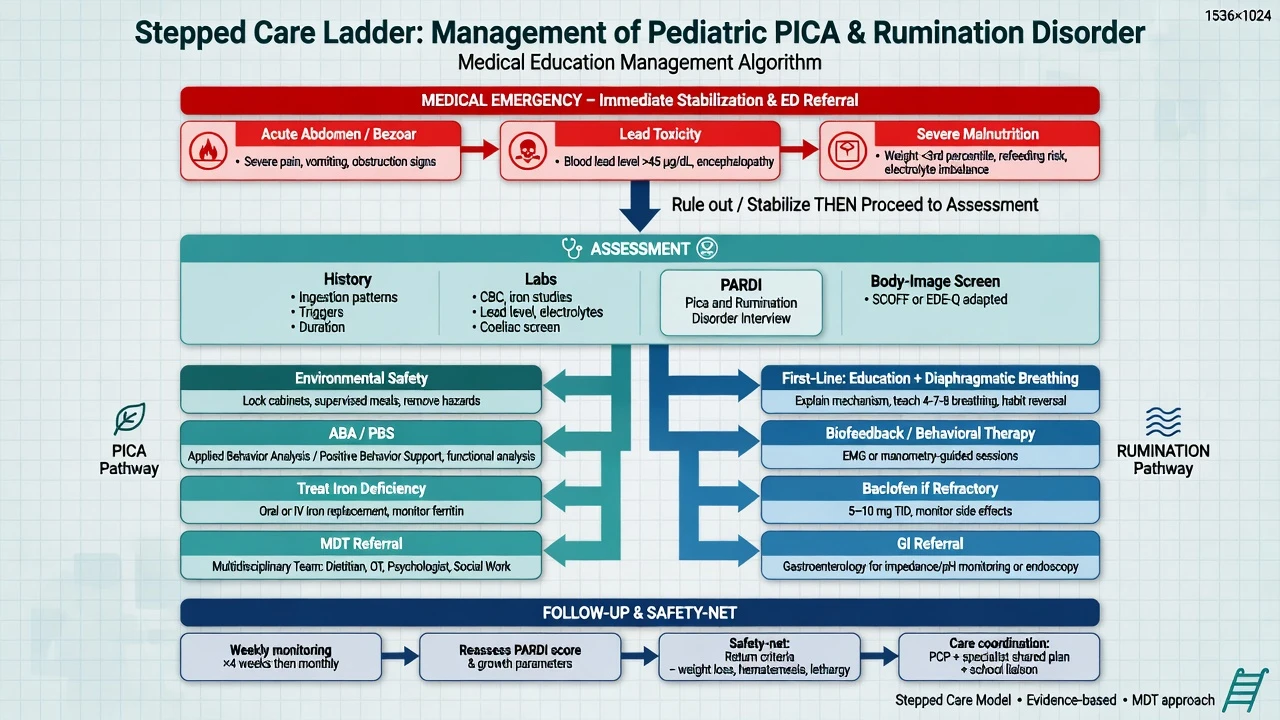
Risk domains. Acute abdomen; lead and other toxin exposure; aspiration; malnutrition; capacity and best-interests frameworks for nutrition/safety decisions in severe ID; suicide if comorbid mood disorder.[1][2][15]
Investigations
No biomarker diagnoses either disorder. Pica: FBC and iron studies routinely when pica is present; consider zinc when clinically indicated; blood lead if paint chips, soil, or industrial exposure risk; imaging and surgical review for suspected bezoar or obstruction; toxicology as substance dictates.[1][3][4] Rumination: often a clinical diagnosis; investigate organic red flags (dysphagia to solids and liquids, bleeding, nocturnal aspiration, progressive weight loss, abnormal exam). High-resolution manometry with impedance can support diagnosis when uncertain or refractory — coordinate with gastroenterology.[9][11] Baseline metabolic panel and ECG when underweight, dehydrated, or before relevant medications.
Management — acute risk and resuscitation
Severe nutritional compromise from rumination with food loss follows medical stabilisation principles shared with other feeding disorders when underweight or metabolically unstable — senior medical review, rehydration, electrolyte correction, and dietetic input.[12][15] Capacity assessment is decision-specific when compulsory medical treatment is considered under local mental health or guardianship law.[15][16]
Management — definitive and stepwise
Pica — behavioural and medical care
- Environmental safety and access control — remove or secure high-risk substances; supervise meals and transitions in ID residential settings; carer training.[1][2]
- Behavioural interventions — functional analysis; differential reinforcement of incompatible/alternative behaviour; enriched environments; applied behaviour analysis / positive behaviour support frameworks in ID/ASD. Avoid purely punitive approaches that increase secrecy without reducing access.[1][2]
- Treat micronutrient deficiency — iron repletion when iron deficiency or depletion is present (oral iron as first-line when tolerated; parenteral iron per haematology protocols when oral fails or is not absorbed; monitor response with ferritin/Hb). Iron treatment may reduce craving in deficiency-associated pica but does not replace behavioural and environmental plans in ID.[3][4][5]
- Multidisciplinary care — psychiatry, dietetics, ID team, obstetrics if pregnant, toxicology/public health if lead, surgery if bezoar.[15][16]
Rumination — behavioural first-line
Education and diaphragmatic breathing are first-line across ages when the patient can engage: explain the mechanism (not “your stomach is broken forever”), teach postprandial diaphragmatic breathing as a competing response to abdominothoracic strain, rehearse at meals, and practise daily.[9][10][11] Halland and colleagues demonstrate mechanistic and clinical support for diaphragmatic breathing; paediatric series (Chial) support behavioural treatment frameworks and prognosis teaching.[10][12]
Biofeedback training of abdominothoracic muscular control has randomised evidence of reducing regurgitation episodes versus placebo procedures and is an evidence-based escalation or adjunct when available.[14]
Pharmacotherapy for rumination
There is no first-line “cure tablet” that replaces breathing training. For refractory rumination syndrome, baclofen has randomised double-blind crossover evidence of reducing rumination episodes versus placebo (Pauwels et al.). In that trial, baclofen was used as 10 mg orally three times daily during active treatment periods, with monitoring for side effects (sedation, dizziness, gastrointestinal effects, withdrawal risk if stopped abruptly after longer use).[13] Position baclofen as a specialist adjunct after or alongside behavioural therapy, not as monotherapy while the mechanism remains unaddressed.[9][13] Tricyclic antidepressants have been described in combination series with breathing techniques in selected refractory cases — evidence is weaker than the baclofen RCT; specialist GI–psychiatry judgment applies.[9][11]
Stepped care intensity
Outpatient education + diaphragmatic breathing / pica behavioural plan → dietetic and GI co-management → biofeedback programmes → specialist pharmacotherapy for refractory rumination → inpatient medical care for instability or surgical complications → planned step-down with carer coaching and environmental design.[9][15][16]
Specific subtypes and scenarios
Pregnancy pica. Pagophagia and geophagia are classic; check iron studies, collaborate with obstetrics, address cultural practices respectfully while treating deficiency and medical risk.[1][5]
Severe ID with high-risk pica. PBS, environmental design, and 24-hour access control dominate; psychotropics treat comorbid conditions, not pica as a licensed primary indication.[2]
Rumination misdiagnosed as GORD. Years of PPI non-response; re-take the effortlessness and meal-timing history; teach breathing rather than escalating acid suppression alone.[9][11]
Trichophagia. Surgical trichobezoar (including Rapunzel-type extension) is a classic complication — abdominal symptoms need surgical, not only psychiatric, ownership.[1]
Rumination with eating-disorder comorbidity. If shape/weight overvaluation and binge–purge intent are present, treat BN/AN pathways in parallel rather than forcing a single label.[6][15]
Complications and pitfalls
- Missing lead poisoning or bezoar.[1][2]
- Calling BN because food comes up without asking about body image and binge intent.[9][15]
- Chronic PPI escalation for rumination physiology.[9]
- Punitive pica management that increases secrecy without reducing access.[2]
- Assuming iron tablets alone extinguish ID-related automatic pica.[3][5]
- Confusing depressive cognitive rumination with rumination disorder.[11]
Prognosis and disposition
Developmental pica in children of typical intellect often remits with maturation and supervision; pica in ID may persist without ongoing environmental and behavioural supports.[1][2] Rumination syndrome often improves substantially with diaphragmatic breathing and biofeedback when correctly diagnosed; delayed diagnosis prolongs secondary nutritional and social harm.[9][12][14] Disposition: shared care with GP/paediatrics/GI as relevant; clear safety-net for abdominal emergency signs, neurological change (lead), progressive weight loss, and total food refusal.[15][16]
Special populations
Infants and young children. Apply the developmental-inappropriateness criterion carefully; safeguard when ingestion is severe or unexplained.[1][7]
Intellectual disability and autism. Highest burden of dangerous pica; dual formulation with sensory and communication supports; capacity frameworks for restrictive interventions.[2]
Pregnancy. Iron deficiency pathway; cultural geophagy nuance; fetal risk from toxins.[1][5]
Older adults. Dementia-related oral exploration may mimic pica; formulate under neurocognitive disorder care while still securing toxic substances.[2]
Cultural formulation. Distinguish normative practice from pathological pica meeting DSM severity and impairment thresholds — medical risk of the substance still matters.[1][15]
Evidence, guidelines and regional differences
Landmark pillars: Leung update review and Schnitzler neurology/psychopathology review for pica;[1][2] Miao micronutrient meta-analysis;[3] Barton iron-associated adult pica;[4] Ganesan iron–pica scoping review;[5] Hartmann child and adult prevalence series;[6][7] PARDI development;[8] Halland CGH diagnosis and treatment update;[9] diaphragmatic breathing mechanism study;[10] Absah pathophysiology review;[11] Chial paediatric classic;[12] Pauwels baclofen RCT;[13] Barba biofeedback RCT;[14] APA eating disorders practice guideline;[15] RANZCP eating disorder guidelines.[16]
Use RANZCP eating disorder multidisciplinary principles for specialist feeding-disorder care, with paediatric, adult, ID, and obstetric pathways as age and setting dictate. Medical emergencies use local surgical and toxicology services. Mental Health Act and guardianship frameworks for compulsory interventions are jurisdiction-specific; assess capacity decision-specifically. Access to formal biofeedback programmes varies — diaphragmatic breathing coaching remains deliverable in most clinics.[15][16]
Exam pearls
PICA-RUM exam anchors
References
- [1]Leung AKC, Hon KL Pica: A Common Condition that is Commonly Missed - An Update Review Curr Pediatr Rev, 2019.PMID 30868957
- [2]Schnitzler E The Neurology and Psychopathology of Pica Curr Neurol Neurosci Rep, 2022.PMID 35674869
- [3]Miao D, Young SL, Golden CD A meta-analysis of pica and micronutrient status Am J Hum Biol, 2015.PMID 25156147
- [4]Barton JC, Barton JC, Bertoli LF Pica associated with iron deficiency or depletion: clinical and laboratory correlates in 262 non-pregnant adult outpatients BMC Blood Disord, 2010.PMID 21176208
- [5]Ganesan PR, Vasauskas AA The Association Between Pica and Iron-Deficiency Anemia: A Scoping Review Cureus, 2023.PMID 37220446
- [6]Hartmann AS, Zenger M, Glaesmer H, et al. Prevalence of pica and rumination behaviours in adults and associations with eating disorder and general psychopathology: findings from a population-based study Epidemiol Psychiatr Sci, 2022.PMID 35678377
- [7]Hartmann AS, Poulain T, Vogel M, et al. Prevalence of pica and rumination behaviors in German children aged 7-14 and their associations with feeding, eating, and general psychopathology: a population-based study Eur Child Adolesc Psychiatry, 2018.PMID 29675593
- [8]Bryant-Waugh R, Micali N, Cooke L, et al. Development of the Pica, ARFID, and Rumination Disorder Interview, a multi-informant, semi-structured interview of feeding disorders across the lifespan: A pilot study for ages 10-22 Int J Eat Disord, 2019.PMID 30312485
- [9]Halland M, Pandolfino J, Barba E Diagnosis and Treatment of Rumination Syndrome Clin Gastroenterol Hepatol, 2018.PMID 29902642
- [10]Halland M, Parthasarathy G, Bharucha AE, Katzka DA Diaphragmatic breathing for rumination syndrome: efficacy and mechanisms of action Neurogastroenterol Motil, 2016.PMID 26661735
- [11]Absah I, Rishi A, Talley NJ, Katzka D, Halland M Rumination syndrome: pathophysiology, diagnosis, and treatment Neurogastroenterol Motil, 2017.PMID 27766723
- [12]Chial HJ, Camilleri M, Williams DE, Litzinger K, Perrault J Rumination syndrome in children and adolescents: diagnosis, treatment, and prognosis Pediatrics, 2003.PMID 12509570
- [13]Pauwels A, Broers C, Van Houtte B, et al. A Randomized Double-Blind, Placebo-Controlled, Cross-Over Study Using Baclofen in the Treatment of Rumination Syndrome Am J Gastroenterol, 2018.PMID 29206813
- [14]Barba E, Accarino A, Soldevilla A, Malagelada JR, Azpiroz F Randomized, Placebo-Controlled Trial of Biofeedback for the Treatment of Rumination Am J Gastroenterol, 2016.PMID 27185077
- [15]Crone C, Fochtmann LJ, Attia E, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders Am J Psychiatry, 2023.PMID 36722117
- [16]Hay P, Chinn D, Forbes D, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders Aust N Z J Psychiatry, 2014.PMID 25351912