Psych · General adult psychiatry — perinatal
Postpartum psychosis
Also known as Puerperal psychosis · Postnatal psychosis · Postpartum mania · Peripartum psychosis · Childbirth-related psychosis
Exam-exhaustive fellowship reference on postpartum psychosis — onset timing, bipolar spectrum link, dual mother-infant risk, organic differential, admission and mother-baby units, Bergink-informed lithium/antipsychotic/benzodiazepine algorithms, ECT, lactation decisions, recurrence and prevention in subsequent pregnancies. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Postpartum psychosis (PPP) is a classic FRANZCP MEQ and MRCPsych CASC topic because it fuses general adult affective psychosis skills with obstetric timing, safeguarding, reproductive psychopharmacology, and service design (mother-baby units). A candidate who only remembers "rare psychosis after birth" will fail; the board expects onset window, bipolar affiliation, dual risk, a named treatment algorithm, and next-pregnancy prevention.[1][5][7]
Definition and classification
PPP is a clinical syndrome, not a single DSM-5-TR entity. It describes acute mania, mixed states, depressive psychosis, and sometimes atypical confusional presentations with onset in the early puerperium. Operational coding often uses a mood episode (or brief psychotic presentation) with peripartum onset (DSM-5-TR: onset during pregnancy or within four weeks after delivery) plus clinical service language for "puerperal psychosis," which may extend slightly beyond four weeks when the syndrome is classic.[1][5]
ICD-11 pathways may code acute and transient psychotic disorders or bipolar/affective episodes with perinatal timing notes — state which system you are using rather than inventing a unique ICD code for "postpartum psychosis."[5]
Long-term outcome literature distinguishes women whose severe illness remains largely isolated to the postpartum period from those who evolve multi-episode bipolar trajectories; Gilden and colleagues estimate that a substantial minority (often framed around two-fifths in meta-analysis) may follow an isolated-PPP pattern, but first-onset PPP still warrants bipolar-spectrum counselling and longitudinal follow-up.[12][14]

Classification spectrum and discriminators
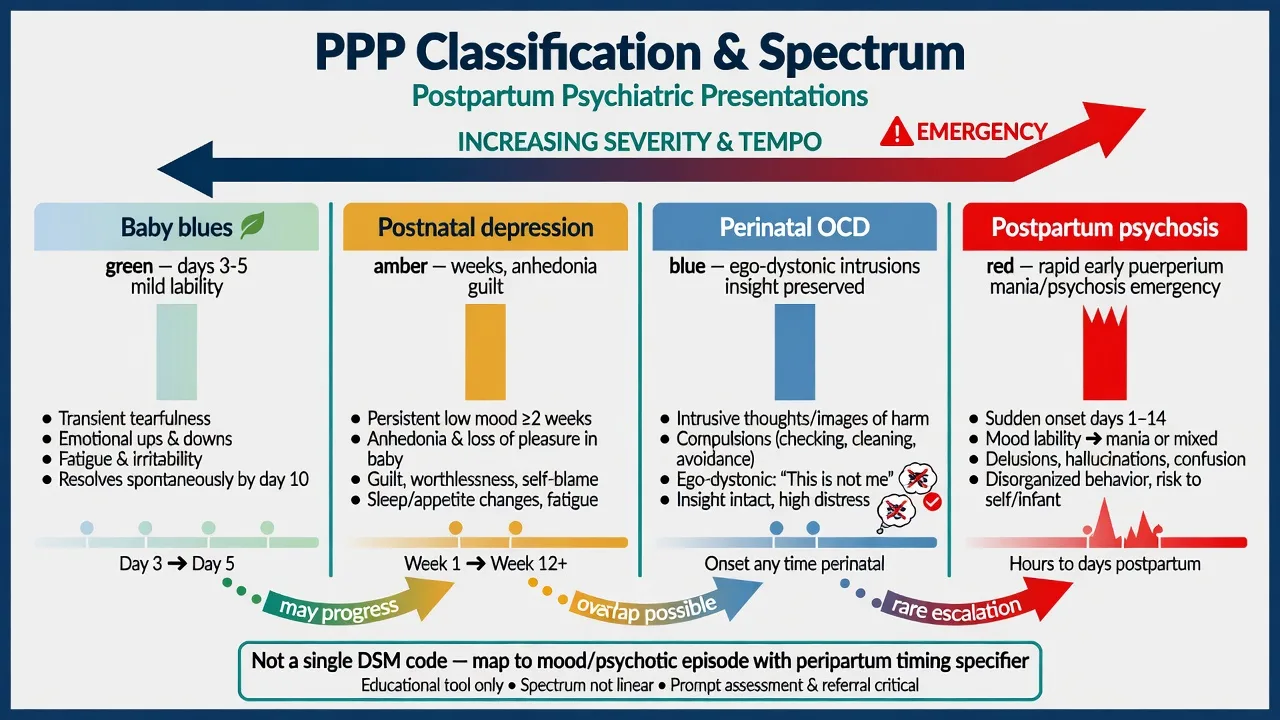
Baby blues
- Peak days 3–5
- Tearfulness, lability
- Function largely preserved
- Self-limiting
Postnatal depression
- Weeks to months
- Anhedonia, guilt, suicide risk
- Usually non-psychotic
- Still assess infant care capacity
Perinatal OCD
- Ego-dystonic infant-harm images
- Insight usually preserved
- Checking/avoidance
- Not the same pathway as PPP
Postpartum psychosis
- Rapid early puerperium
- Mania/mixed/depressive psychosis
- Delusions may involve infant
- Emergency admission pathway
Epidemiology and risk
Headline numbers for exams
Incidence of classic PPP is on the order of 1–2 per 1000 births. Absolute rarity does not reduce exam weight because lethality and medicolegal stakes are high.[1][5]
Munk-Olsen and colleagues showed elevated first-time psychiatric contact among new mothers in the early postpartum period using population registers — a classic epidemiology stem linking childbirth to severe mental disorder onset.[6] Wesseloo and colleagues quantified extremely high postpartum relapse risk in women with bipolar disorder, prior PPP, or both, making prevention planning non-negotiable rather than optional.[3]
Risk factors. Bipolar diathesis (personal history of mania/hypomania or clear bipolar family history); prior PPP; primiparity; severe sleep deprivation; obstetric complications; abrupt cessation of effective mood stabilisers or antipsychotics; psychosocial isolation and intimate partner violence as amplifiers.[1][5][3] Severe mental disorders carry elevated all-cause and suicide mortality in meta-review data — apply that lens when choosing observation intensity.[11]
Pathophysiology
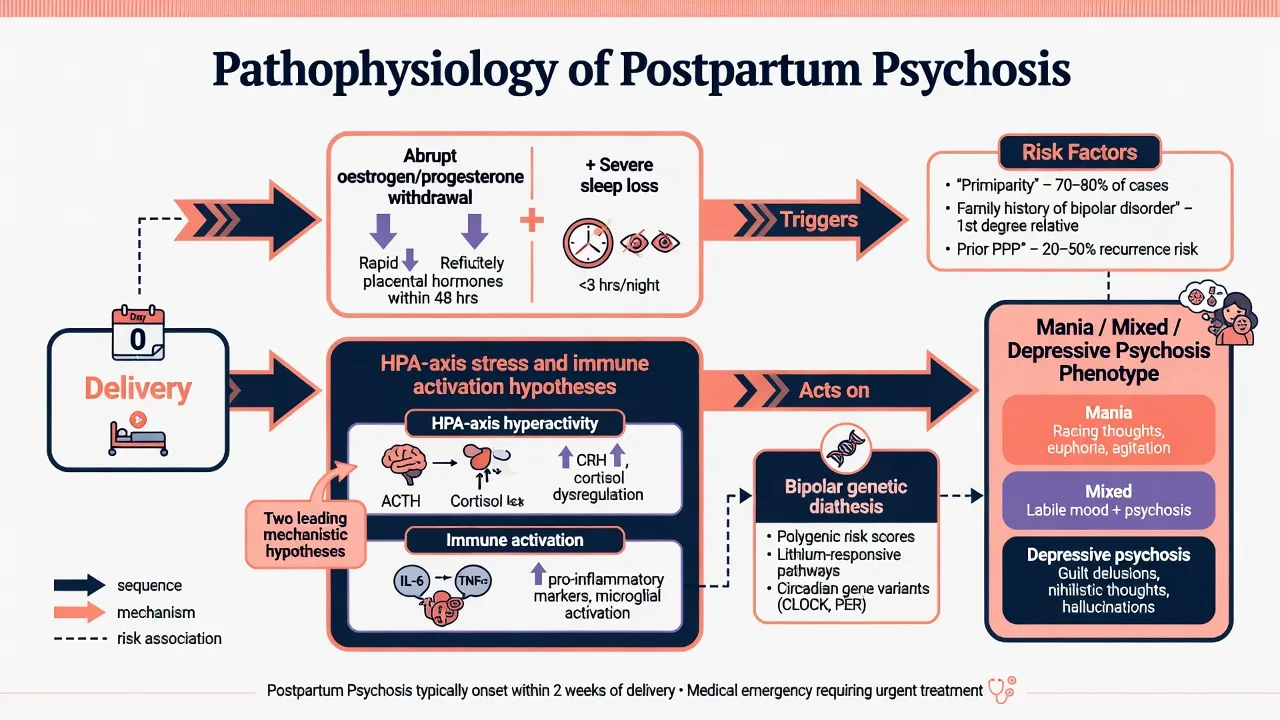
After delivery, abrupt oestrogen and progesterone withdrawal coincides with profound sleep disruption. On a bipolar genetic background this window is uniquely pro-psychotic for affective mania and psychosis compared with many other life stressors.[1][5] Immune and HPA-axis hypotheses are examinable but not diagnostic tests in routine care — do not claim a pathognomonic lab panel.[1]
Social amplifiers (isolation, birth trauma, stigma delaying help-seeking) shape presentation and delay, not the core bipolar-linked biology narrative most examiners expect.[5]
Clinical presentation
Timing. Classic onset is rapid, often within the first two weeks after birth; day 3–10 stems dominate exams. Later onset is possible but prompts a harder organic and primary schizophrenia-spectrum differential.[1][6]
Manic / mixed PPP. Elevated or irritable mood, decreased need for sleep that is not explained by infant care alone, pressure of speech, grandiosity, reckless behaviour, and mood-congruent or mood-incongruent psychotic content.[1]
Depressive psychotic PPP. Severe low mood, guilt or nihilism, psychomotor retardation or agitation, auditory hallucinations, and high suicide risk — still an emergency even without elation.[1][5]
Atypical / confusional. Perplexity, disorientation, or fluctuating "delirium-like" quality without fever may occur; always exclude organic delirium rather than romanticising "classic confusional puerperal psychosis."[1]
Infant-related content. Delusions of substitution, special mission, contamination, rejection ("not my baby"), or harm themes may appear. Command hallucinations involving the infant demand continuous supervision planning.[1][5]
Collateral from partner, midwife, and family is often more reliable than patient insight early in the illness.[1]
Differential diagnosis
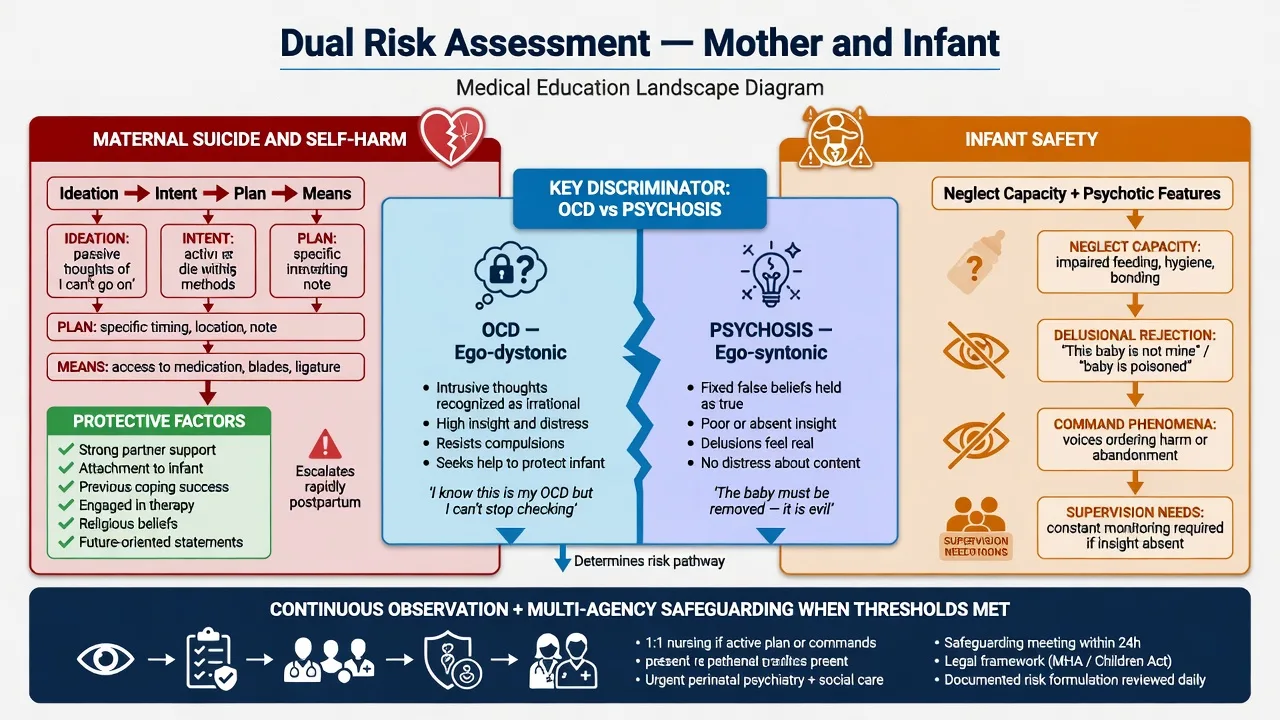
OCD vs PPP (infant harm)
- OCD: ego-dystonic, insight, horror at thought
- PPP: ego-syntonic delusion or command
- Both need careful dual risk assessment
- Mislabel either way harms care
Organic / medical
- Postpartum thyroiditis
- Infection, sepsis, delirium
- Eclampsia sequelae, substance
- Rare autoimmune encephalitis
Primary psychosis spectrum
- Schizophrenia first episode possible
- Timing + mood + family history help
- Substance-induced always on list
- Do not delay treatment while debating label
Iatrogenic / other
- Steroid or stimulant effects
- Severe sleep deprivation alone is not PPP
- Blues lack psychosis
- Personality crisis lacks true mania/psychosis
Perinatal OCD with ego-dystonic intrusive infant-harm images is a high-yield discriminator: patients typically recognise the thoughts as unwanted and fight them. That is not the same as believing the infant must be harmed or receiving commanding voices. Both still need careful risk assessment; OCD is not "safe by default," and psychosis is not "always filicidal."[15][1]
Assessment
Structure the interview: pregnancy and birth course; sleep (does she sleep when the baby sleeps?); feeding; supports; domestic safety; prior bipolar or PPP; family history of bipolar; substances; child-protection history; and the mother's beliefs about the infant.[1][5]
Document a full MSE with explicit dual risk domains.[1][11]
- Maternal suicide and self-harm — ideation, intent, plan, means, impulsivity, protective factors.[11]
- Infant safety — neglect capacity, aggressive impulses, filicide/infanticide ideation, intent, means, command content, ability to use help, and whether unsupervised contact is safe.[1][5]
Capacity is decision-specific. Involuntary treatment uses local Mental Health Act least-restrictive principles. Do not invent section numbers for the wrong jurisdiction.[7]
Investigations
For first-onset or atypical presentations: full blood count; urea and electrolytes; liver function; glucose; TSH (postpartum thyroiditis is examinable); consider inflammatory markers and cultures if fever; urine drug screen. ECG before selected antipsychotics. Neuroimaging, EEG or lumbar puncture when organic red flags fire (fever, seizures, focal neurology, severe fluctuation, autoimmune clues) — not routinely for every classic early-puerperal manic psychosis with clear affective features.[1][13]
Before lithium: renal function, thyroid function, and a level-monitoring plan with toxicity education. Plan metabolic monitoring if second-generation antipsychotics are used.[2][7]
Emergency management and setting
Admission is the default for florid PPP. Prefer a mother-baby unit (MBU) when available and when joint admission can maintain infant safety under skilled observation; otherwise use a general adult psychiatry ward with a written infant-care and supervision plan, partner/family supports, and safeguarding liaison as required.[10][1]
Australian public MBUs share joint admission, multidisciplinary care (psychiatry, mental health nursing, midwifery/obstetric liaison, social work), and attachment-informed practice, with regional model variation — a high-yield ANZ service fact.[10]
Safeguarding and treatment run together: treat illness aggressively while protecting the infant through supervision, not through stigma-driven separation that is not risk-justified, and not through false reassurance when risk is high.[5][1]
Definitive pharmacotherapy and ECT
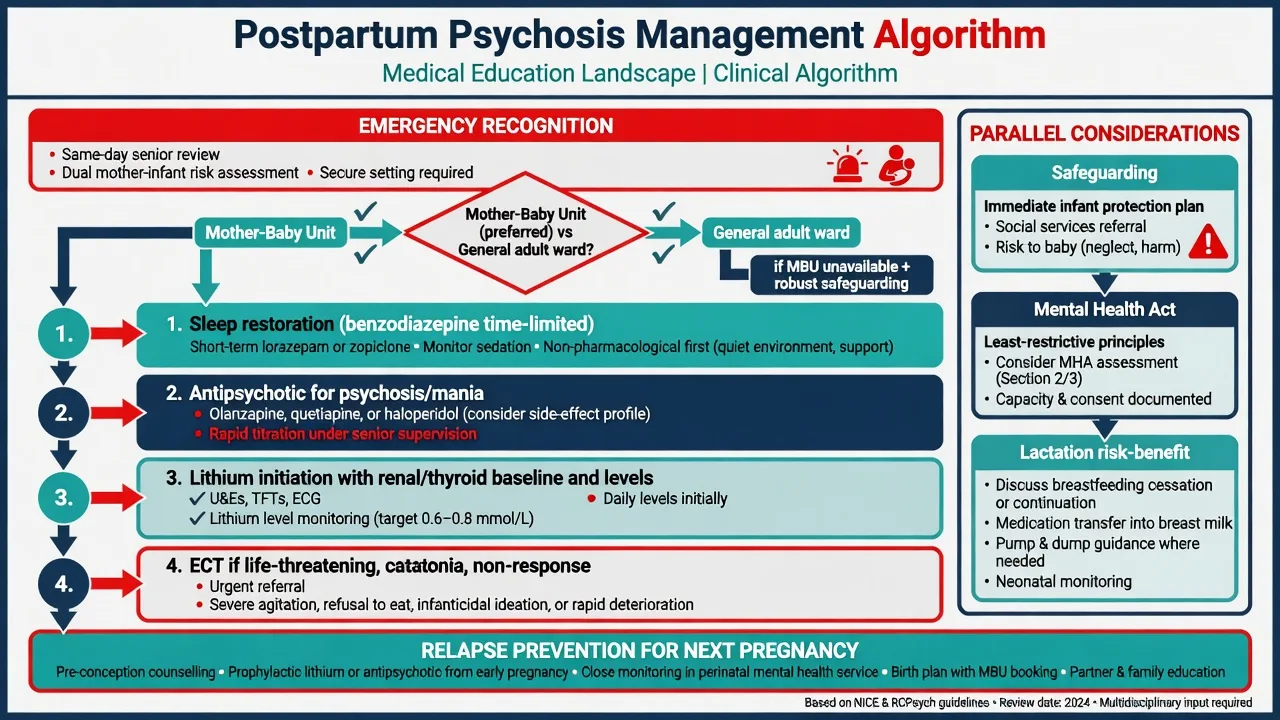
Bergink-informed sequential algorithm
Bergink and colleagues described a structured four-step pathway for first-onset postpartum psychosis/mania with very high remission rates when benzodiazepines, antipsychotics and lithium were used sequentially; nearly all patients remitted within the first three steps in their cohort, and lithium maintenance was associated with lower relapse than antipsychotic monotherapy at follow-up.[2] Later proposed algorithms (Jairaj and colleagues) retain the emergency inpatient framing and stepwise pharmacotherapy logic for contemporary practice.[13]
Step 1 — Sleep and acute behavioural control. Time-limited benzodiazepine for severe insomnia and agitation. Example exam-ready option: lorazepam 1–2 mg orally (or IM per local rapid-tranquillisation protocol when oral route unsafe), repeated as needed within local maximums, with respiratory and fall monitoring, aiming for restorative sleep rather than chronic benzodiazepine dependence.[2][13]
Step 2 — Antipsychotic for psychosis/mania. Second-generation agents commonly discussed include olanzapine (e.g. start 5–10 mg orally at night, titrate by response and sedation toward roughly 10–20 mg/day as tolerated) or quetiapine (e.g. build toward 300–600 mg/day in divided or evening-weighted doses as indicated for mania/psychosis), with metabolic monitoring, ECG when indicated, and EPS/sedation review. Choose agent by prior response, metabolic risk, QTc profile and local formulary.[2][7][13]
Step 3 — Lithium for affective PPP. For many affective postpartum psychoses, initiate lithium carbonate after baseline renal and thyroid tests, with shared decision-making about lactation. Typical adult mania-range dosing is individualised (commonly starting around 450–900 mg/day in divided doses depending on formulation and renal function) aiming for a therapeutic serum level usually discussed in the approximate 0.6–1.0 mmol/L range for acute mania under close monitoring (local lab timing 12 hours post-dose). Educate on toxicity (tremor, GI upset, ataxia, confusion), hydration, and interacting drugs (NSAIDs, ACE inhibitors, thiazides).[2][7]
Step 4 — ECT. Consider ECT for life-threatening severity, catatonia, refusal of oral intake, medication non-response, or need for rapid definitive control. ECT has strong efficacy evidence in severe depressive disorders and is a legitimate, sometimes first-line, option in selected severe perinatal psychosis/depression after consent and obstetric-anaesthetic coordination.[8][16][1]
Lactation and infant feeding
In florid PPP, maternal and infant safety outrank feeding preference. Many antipsychotics and lithium require specialist lactation risk-benefit discussion; temporary formula feeding may be safest while levels stabilise and the mother is heavily sedated or lithium-treated. Document the plan and involve paediatric/midwifery advice rather than giving absolute "always" or "never" rules for every agent.[2][5][13]
Agents to avoid as casual defaults
Valproate is a major teratogen with neurodevelopmental risk — do not use it as the exam default mood stabiliser in reproductive-age women when lithium or antipsychotics are appropriate alternatives, and apply rigorous pregnancy-prevention frameworks if ever used under exceptional circumstances.[7][5]
Prevention in subsequent pregnancies
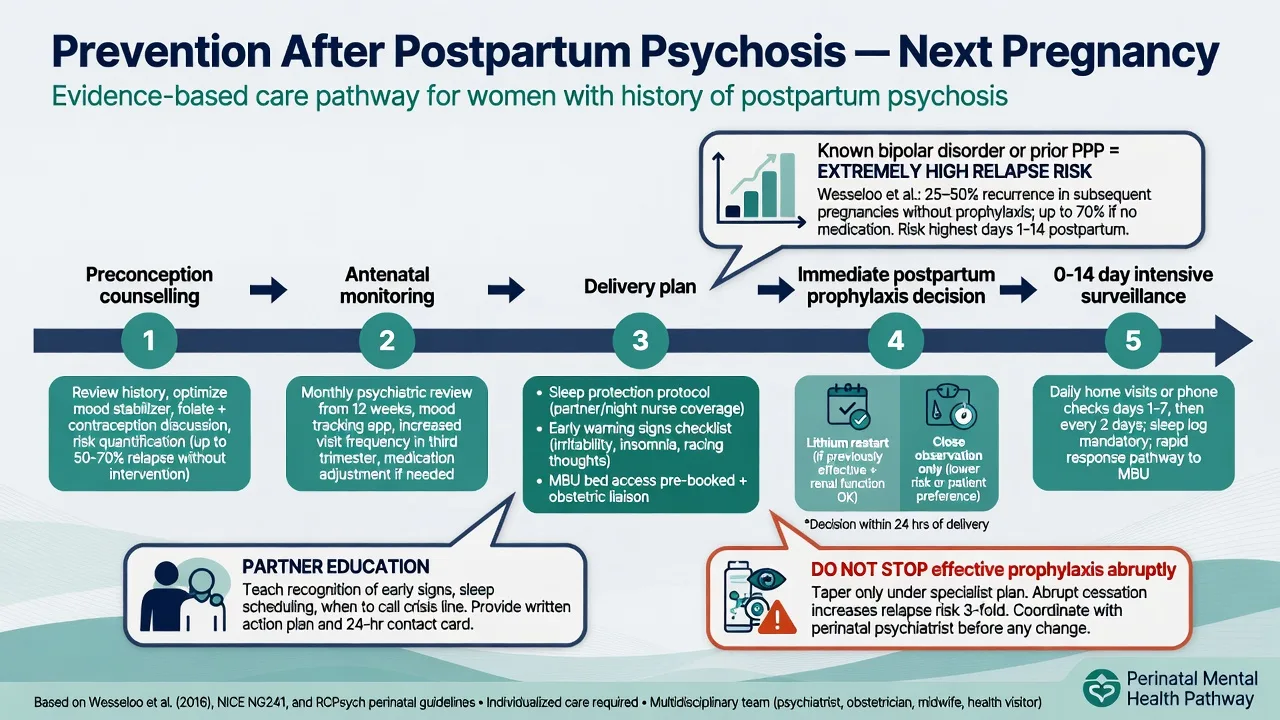
Women with prior PPP or bipolar disorder face extremely high postpartum relapse risk without a plan.[3][4]
Bergink and colleagues showed that structured prevention strategies in high-risk women (including postpartum lithium prophylaxis decisions in selected high-risk groups) can substantially reduce postpartum mania/psychosis risk compared with unmanaged trajectories.[4]
Preconception counselling elements. Recurrence risk; contraception until a plan is ready; medication choices in pregnancy (lithium cardiac malformation absolute-risk framing from Patorno and colleagues — increased risk versus non-exposed and versus lamotrigine, dose-related signals — counsel with absolute numbers, not folklore); sleep protection plan; early warning signs; planned MBU access; partner education; and obstetric-psychiatric joint care.[9][4][5][7]
Immediate postpartum plan. Decide before delivery whether to start or reinstate lithium promptly after birth (with renal/thyroid baseline already arranged), maintain antipsychotic cover if indicated, protect sleep aggressively (night supports, consider short-term benzodiazepine), and arrange intensive review in the first 14 days.[4][2][3]
Subtypes and scenarios
First-onset PPP without known bipolar diagnosis. Still treat as emergency affective psychosis; counsel that bipolar spectrum risk is substantial longitudinally even if some women remain postpartum-limited.[12][14]
Known bipolar with medication stopped in pregnancy. Classic high-risk stem — expect early puerperal mania/psychosis without prophylaxis.[3][5]
Depressive psychotic PPP. High suicide risk; lithium and/or ECT often central; do not under-treat because elation is absent.[1][8]
Catatonic features. Lorazepam challenge pathway and low threshold for ECT.[8][16]
No MBU beds. General adult admission with written infant supervision plan and safeguarding — do not delay admission waiting for a perfect bed.[10]
Complications and pitfalls
Classic errors: labelling PPP as blues or "stress"; confusing OCD intrusions with psychosis (and reverse); discharging unsupported psychosis; starting valproate by default; focusing only on maternal MSE while the infant is left unsupervised; abrupt antenatal medication cessation without a relapse plan; and iatrogenic harm (lithium toxicity, severe sedation impairing infant care, metabolic effects).[1][15][7]
Prognosis and disposition
With structured inpatient algorithms, acute remission rates are high.[2] Medium-term sustained remission is common but not universal; relapse risk rises if lithium is omitted in affective cases that needed it.[2][13] Longitudinally, some women have postpartum-limited illness while others develop multi-episode bipolar disorder — counsel both possibilities and arrange follow-up.[12][14]
Disposition ladder. MBU or general inpatient → step-down perinatal mental health team → shared care with GP/obstetrics → preconception clinic before next pregnancy. Document early-warning signs and crisis contacts before discharge.[10][7]
Special populations
Adolescent mothers need developmental capacity framing and family-systems work. Pre-existing schizophrenia requires parallel parenting-capacity assessment and may follow a less purely affective algorithm. Cultural safety and stigma reduction are essential to earlier presentation. Partners are collateral historians and potential carers under stress — include them with consent.[5][10]
Evidence, guidelines and regional deltas
RANZCP mood disorder guidance supports formulation-driven care, bipolar exclusion, and shared decision-making; Australian MBUs are a distinctive inpatient model for severe perinatal illness when available.[7][10]
Landmark pillars for exams: Bergink 2016 clinical review; Bergink 2015 treatment algorithm; Bergink 2012 prevention; Wesseloo 2016 relapse meta-analysis; Munk-Olsen 2006 registers; Jones 2014 Lancet series; Gilden 2020 and Rommel 2021 long-term outcomes; Jairaj 2023 algorithm update; Patorno 2017 lithium malformations; UK ECT Review Group and contemporary ECT-for-PPP commentary; Galbally Australian MBU comparison; RANZCP mood guidelines.[1][2][4][3][6][5][12][14][13][9][8][16][10][7]
Exam pearls
POSTPARTUM PSYCHOSIS emergency pack
References
- [1]Bergink V, Rasgon N, Wisner KL Postpartum Psychosis: Madness, Mania, and Melancholia in Motherhood Am J Psychiatry, 2016.PMID 27609245
- [2]Bergink V, Burgerhout KM, Koorengevel KM, Kamperman AM, Hoogendijk WJ, Lambregtse-van den Berg MP, et al. Treatment of psychosis and mania in the postpartum period Am J Psychiatry, 2015.PMID 25640930
- [3]Wesseloo R, Kamperman AM, Munk-Olsen T, Pop VJ, Kushner SA, Bergink V Risk of Postpartum Relapse in Bipolar Disorder and Postpartum Psychosis: A Systematic Review and Meta-Analysis Am J Psychiatry, 2016.PMID 26514657
- [4]Bergink V, Bouvy PF, Vervoort JS, Koorengevel KM, Steegers EA, Kushner SA Prevention of postpartum psychosis and mania in women at high risk Am J Psychiatry, 2012.PMID 22407083
- [5]Jones I, Chandra PS, Dazzan P, Howard LM Bipolar disorder, affective psychosis, and schizophrenia in pregnancy and the post-partum period Lancet, 2014.PMID 25455249
- [6]Munk-Olsen T, Laursen TM, Pedersen CB, Mors O, Mortensen PB New parents and mental disorders: a population-based register study JAMA, 2006.PMID 17148723
- [7]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [8]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [9]Patorno E, Huybrechts KF, Hernandez-Diaz S Lithium Use in Pregnancy and the Risk of Cardiac Malformations N Engl J Med, 2017.PMID 28854098
- [10]Galbally M, Sved-Williams A, Kristianopulos D, Mercuri K, Brown P, Buist A Comparison of public mother-baby psychiatric units in Australia: similarities, strengths and recommendations Australas Psychiatry, 2019.PMID 30407072
- [11]Chesney E, Goodwin GM, Fazel S Risks of all-cause and suicide mortality in mental disorders: a meta-review World Psychiatry, 2014.PMID 24890068
- [12]Gilden J, Kamperman AM, Munk-Olsen T, Hoogendijk WJG, Kushner SA, Bergink V Long-Term Outcomes of Postpartum Psychosis: A Systematic Review and Meta-Analysis J Clin Psychiatry, 2020.PMID 32160423
- [13]Jairaj C, Seneviratne G, Bergink V, Sommer IEC, Dazzan P Postpartum psychosis: A proposed treatment algorithm J Psychopharmacol, 2023.PMID 37515460
- [14]Rommel AS, Molenaar NM, Gilden J, Kushner SA, Westerbeek NJ, Kamperman AM, et al. Long-term outcome of postpartum psychosis: a prospective clinical cohort study in 106 women Int J Bipolar Disord, 2021.PMID 34708260
- [15]Speisman BB, Storch EA, Abramowitz JS Postpartum obsessive-compulsive disorder J Obstet Gynecol Neonatal Nurs, 2011.PMID 22092284
- [16]Kellner CH Electroconvulsive Therapy (ECT) for Postpartum Psychosis: Treatment for a Medical Emergency Am J Psychiatry, 2025.PMID 41320827