Psych · General adult psychiatry — secondary / organic psychosis
Psychotic disorder due to another medical condition
Also known as Organic psychosis · Secondary psychosis · Medical-cause psychosis · Psychosis due to general medical condition · Psychotic disorder due to GMC · Symptomatic psychosis
Exam-exhaustive fellowship reference on psychotic disorder due to another medical condition — DSM-5-TR/ICD-11 framing, endocrine/neuro/autoimmune/metabolic/infective cause map, red-flag work-up tiers, when to image/LP/EEG, cautious symptomatic antipsychotics, and NMDAR/AE red-flag link without duplicating the full autoimmune monograph. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychotic disorder due to another medical condition is the DSM-5-TR name for what examiners still call organic or secondary psychosis: hallucinations and/or delusions that are the direct physiological consequence of a non-psychiatric medical disease. It is high-weight because missing treatable drivers (encephalitis, endocrine crisis, Wilson disease, neurosyphilis, space-occupying lesion, B12 deficiency) produces preventable disability and death, while over-labelling every atypical FEP as "organic forever" wastes pathways. This leaf owns the cause map, work-up ladder, imaging/LP thresholds, and symptomatic management. Deep anti-NMDAR immunotherapy and antibody monographs live in the related autoimmune encephalitis and organic psychosis topic — here you only need recognition, red flags, and correct hand-off.[1][8][11]
Definition and classification
DSM-5-TR requires: (A) prominent hallucinations or delusions; (B) evidence from history, examination or investigations that the disturbance is the direct physiological consequence of another medical condition; (C) not better explained by another mental disorder; (D) does not occur exclusively during the course of a delirium; (E) clinically significant distress or impairment. Specifiers: with delusions or with hallucinations. The medical condition is identified and coded; the psychiatric syndrome is not freestanding schizophrenia.[1][2]
ICD-11 uses secondary mental or behavioural syndromes associated with disorders classified elsewhere, with psychotic symptoms specified when present. Multi-board answers should name which manual you are applying and avoid inventing hybrid codes.[1]
Not this diagnosis if:
- Psychosis occurs only during delirium → code delirium (with psychotic features as description).
- Timeline locked to intoxication/withdrawal or a drug's physiological effect (stimulants, high-THC cannabis, many cases of corticosteroid psychosis) → substance/medication-induced psychotic disorder.
- No adequate medical driver after work-up → primary spectrum or unspecified categories while keeping an open mind if new red flags appear.[1][2][17]
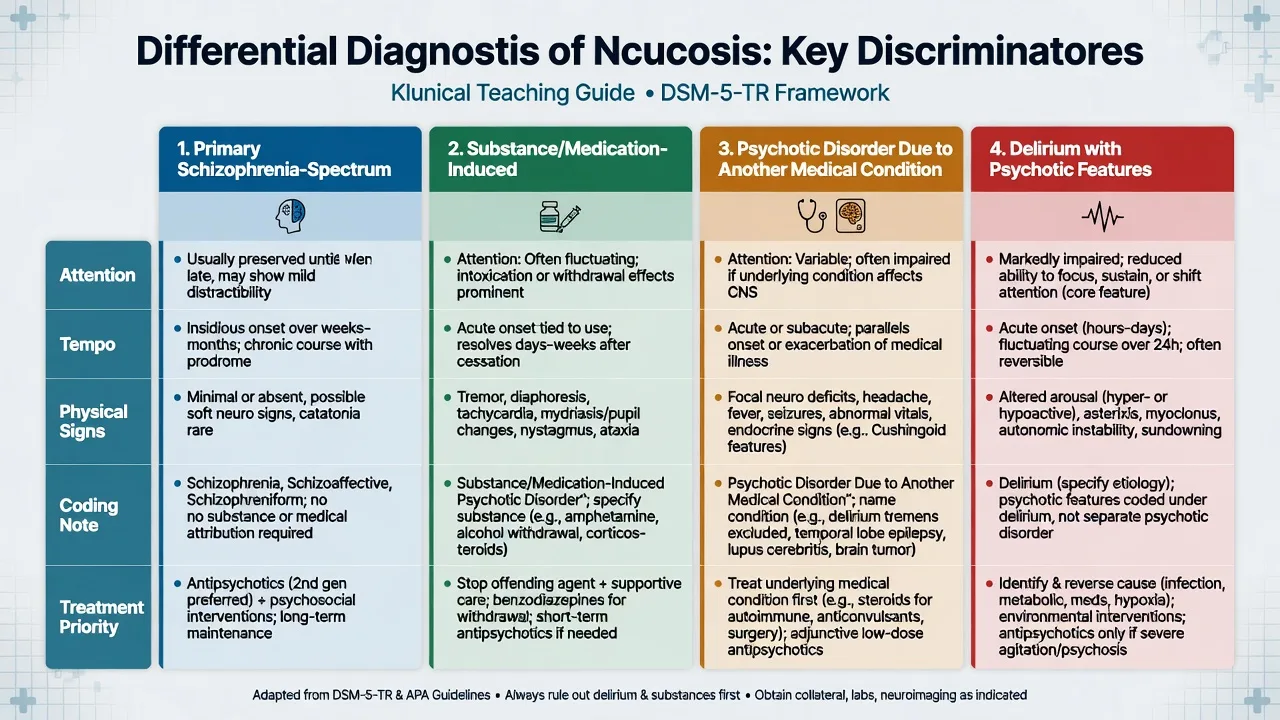
Primary spectrum / affective psychosis
- No direct medical driver after adequate work-up
- Usual age peak teens–30s more common but not exclusive
- Antipsychotic + EIS/psychosocial model
- Still do baseline physical work-up once
Substance / medication-induced
- Temporal lock to drug use, withdrawal or dose
- Steroids often here when drug is the driver
- Stop/reduce agent when safe + short symptomatic cover
- May unmask primary illness
Due to another medical condition
- Direct physiological medical cause
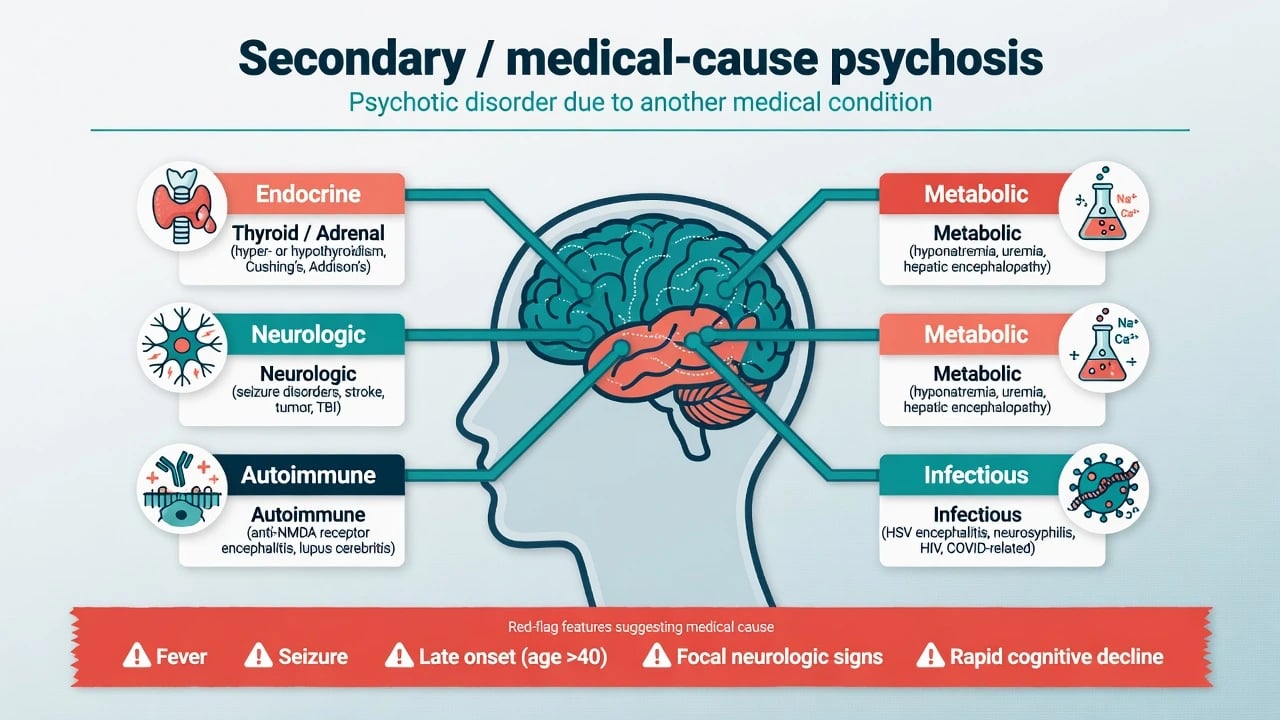
- Cause groups: endocrine, neuro, autoimmune, metabolic, infective
- Treat cause first; antipsychotics adjunctive
- Code medical + psychiatric relationship
Delirium with psychotic features
- Inattention + fluctuation are core
- Hours–days tempo; medical precipitants
- Treat cause; low-dose antipsychotics only for severe risk
- If exclusive to delirium, do not use this disorder code
Epidemiology and risk amplifiers
True medical-cause psychosis is a minority of first presentations, but the miss rate is what examiners punish. Risk amplifiers for secondary disease include late or very-late onset, explosive days–weeks tempo, fever or seizure, focal neurology, known cancer or autoimmune disease, immunosuppression, recent high-dose steroids, unexplained hyponatraemia, and presentations that "do not fit" ordinary FEP demography without substance explanation.[1][2][4]
Neuroimaging yield in unselected young FEP is modest for management-changing lesions; systematic reviews caution against reflexive CT/MRI for every uncomplicated case while supporting imaging when red flags or atypical features are present. Blackman and colleagues' meta-analysis found intracranial abnormalities are not rare on MRI in FEP cohorts, which fuels the "scan everyone" debate — regional practice still diverges (see guidelines section).[5][6][7]
Autoimmune encephalitis is uncommon in absolute numbers but not vanishing relative to infectious encephalitis in modern diagnostics — enough to keep AE on every organic list without making every FEP an antibody panel.[8][18]
Exam-ready framing numbers
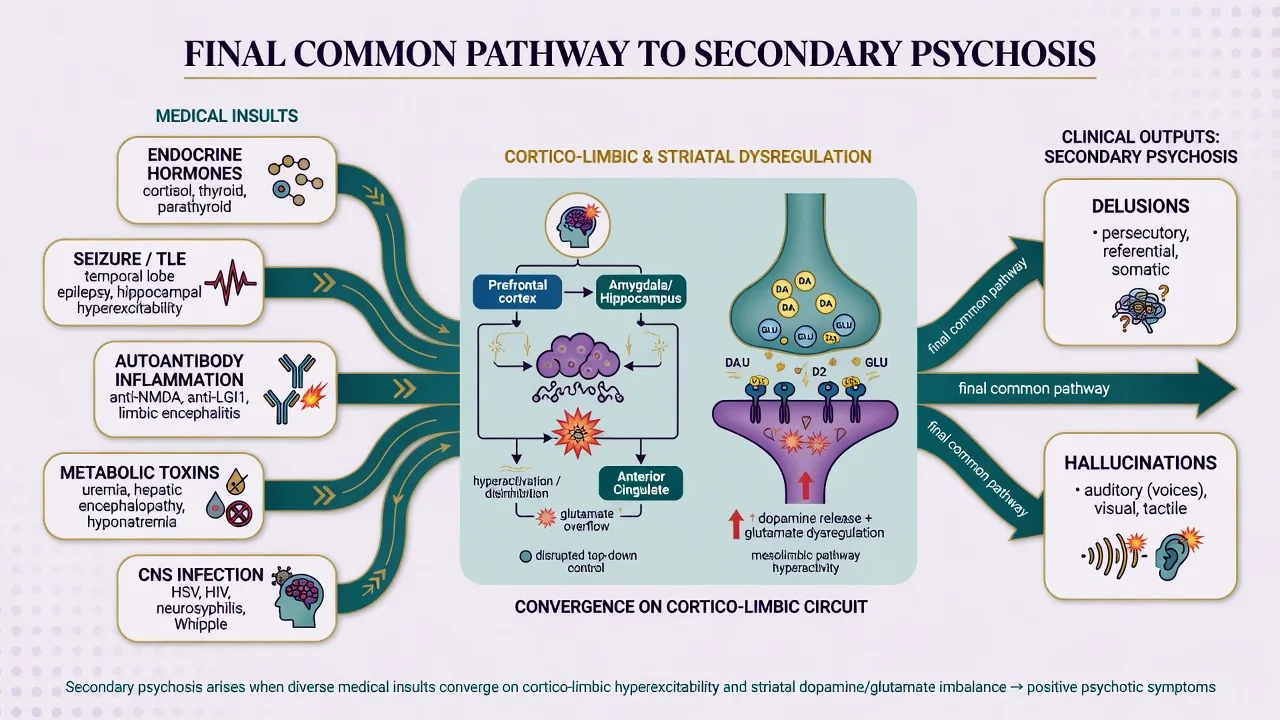
Pathophysiology (conceptual, not fluff)
Secondary psychosis is heterogeneous. Diverse insults — endocrine milieu, seizures and temporal-limbic hyperexcitability, autoantibody-mediated receptor internalisation, metabolic toxins, and CNS infection — converge on cortico-limbic and striatal circuits. Howes and Kapur's "final common pathway" language is useful as a bridge to positive symptoms and D2-targeted symptomatic treatment; it does not mean secondary psychosis is identical to primary schizophrenia biologically or prognostically.[16][1]
Anti-NMDAR encephalitis illustrates antibody-driven NMDAR hypofunction with multi-stage psychiatric then neurologic phenotypes — mechanism depth and immunotherapy belong to the AE topic; here the pathophysiologic pearl is "normal MRI does not exclude antibody disease."[12][18][10]
Metabolic and inborn-error pathways (Wilson copper toxicity, porphyria, urea-cycle disorders, some storage diseases) produce psychiatric phenotypes that can precede hard neurology — Bonnot and colleagues emphasise that IEMs remain under-recognised by psychiatrists.[3]
Clinical presentation
MSE. Document quoted delusional content and hallucination modality. Visual hallucinations raise organic suspicion (especially with clouding) but auditory hallucinations can be fully organic (including AE and epilepsy-related syndromes). Attention and orientation are the delirium discriminators.[2][4]
Tempo.
- Hours–days with fluctuation → delirium/metabolic/toxic until proven otherwise.
- Days–weeks explosive psychosis ± seizure/movement/autonomic → AE and encephalitis shortlist.[11][13]
- Weeks–months with systemic signs → endocrine, neurosyphilis, B12, slow tumour, HIV neuropsychiatric disease.[1][2]
Clues by cause group (high-yield).
| Domain | Prototypes | Bedside clues |
|---|---|---|
| Endocrine | Thyrotoxicosis, severe hypothyroidism, Cushing, hypercalcaemia/hyperparathyroidism, adrenal crisis | Goitre, heat/cold intolerance, weight change, striae, moon face, polyuria, tetany context, abnormal vitals |
| Neurologic | TLE-related psychosis, space-occupying lesion, stroke, TBI sequelae, neurodegenerative | Seizures, focal signs, headache, personality change, progressive cognitive loss |
| Autoimmune | Anti-NMDAR, LGI1, other AE; CNS lupus | Subacute tempo, dyskinesias/FBDS, speech reduction, autonomic storm, hyponatraemia (LGI1), catatonia |
| Metabolic / IEM | B12/folate, Wilson, porphyria, urea-cycle, hepatic/uraemic encephalopathy | Neuropathy/glossitis (B12), LFT/tremor/KF rings context (Wilson), abdominal crises + dark urine (porphyria), fluctuating encephalopathy |
| Infectious | HIV, neurosyphilis, HSV encephalitis, other CNS infections | Risk history, rash, fever, meningism, cognitive decline, endemic exposures |
NMDAR link (do not rewrite the AE monograph). Classic multi-stage course (prodrome → psychiatric → speech → dyskinesias/seizures/autonomic → hypoventilation) and mixed mood–psychosis–catatonia psychopathology are AE-owned detail. Your job on this leaf: spot red flags, order the right package, transfer for immunotherapy decisions.[12][13][10][8]
Differential diagnosis
Win on discriminators: attention, tempo, physical/neurologic signs, substance timeline, and investigation package — not alphabetical lists.[2][4]
Keep primary FEP, affective psychosis, OCD with poor insight, trauma-related phenomena, autism atypical beliefs, and personality (schizotypal/paranoid) on the board after organicity is addressed. Catatonia can be primary psychiatric or medical — treat catatonia and hunt causes in parallel.[1][14]
Bedside assessment
- Observations — temperature, HR, BP, SpO2, capillary glucose.
- History tempo chart — hour zero of change; fever, seizure, headache, head injury, cancer, autoimmune, endocrine, HIV/STI risk, travel, steroids/chemo, substances, family metabolic disease.
- Collateral — speech change, nocturnal events, movement, personality rupture, adherence.
- MSE with examples; brief cognitive/attention screen.
- Neurologic bedside — pupils, cranial nerves, tone, myoclonus/FBDS-like jerks, gait, lateralising signs.
- Risk — suicide, violence, vulnerability, absconding, firearms/means, dependents.
- Capacity for specific decisions (imaging, LP, treatment); legal status under local Mental Health Act principles (least restrictive; do not invent foreign section numbers).
- Medication reconciliation including OTC and complementary products.[2][4][14]
Investigations — the tiered ladder
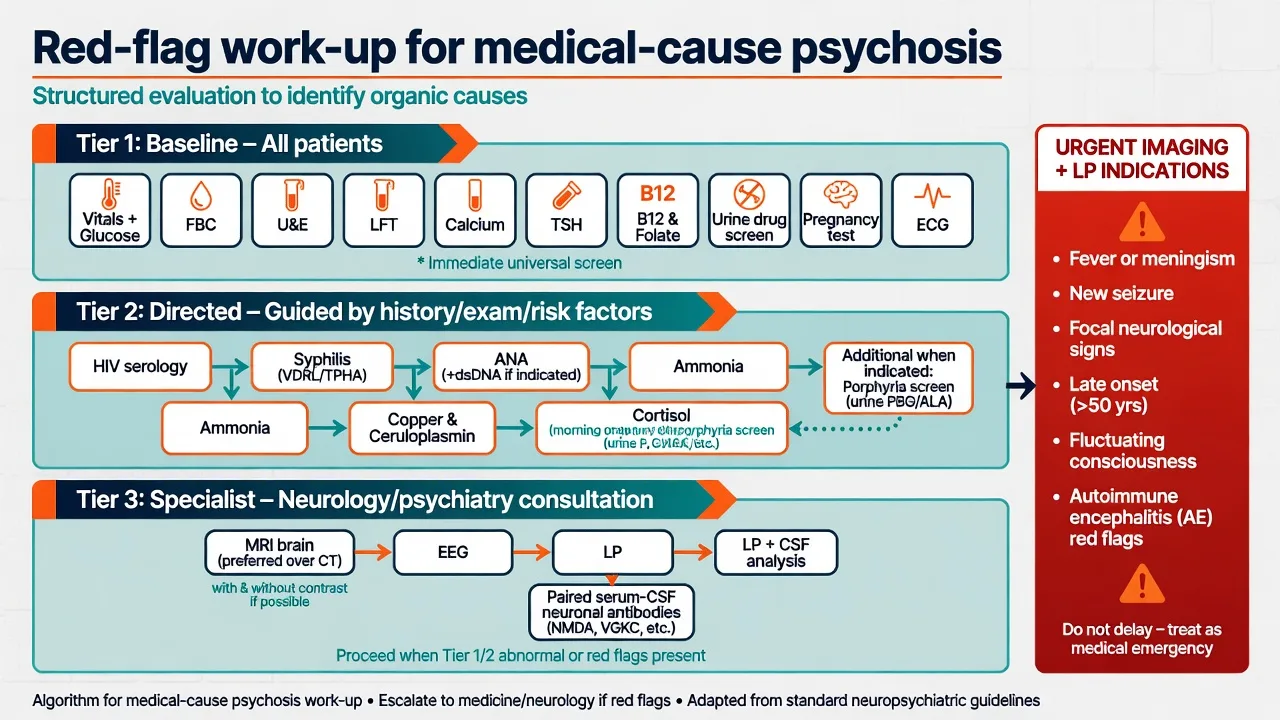
Tier 1 — nearly all new psychosis
Vitals and glucose; FBC, U&E, LFT, calcium, TSH, B12 ± folate, CRP/ESR as available; urine drug screen; pregnancy test if applicable; ECG before antipsychotics; weight/BMI and metabolic baseline when starting antipsychotics.[2][14]
Tier 2 — directed
HIV and syphilis serology (still examinable, still missed); ANA/autoimmune panel when systemic features; copper and ceruloplasmin in young atypical presentations with LFT or movement clues; ammonia if fluctuating encephalopathy; cortisol pathway if Cushing/Addison phenotype; porphyria work-up (urine porphobilinogen) for unexplained abdominal–neuro–psychiatric crises; blood gas and broader metabolic panel when indicated.[1][3][4]
Tier 3 — specialist organic package
When to image (MRI preferred when feasible; CT if unstable or mass-effect urgency): late/very-late first psychosis; focal neurology; trauma; progressive headache or cognitive decline; atypical tempo; AE/encephalitis red flags; unexplained first psychosis where local pathways include imaging. Evidence of routine scanning in young uncomplicated FEP is mixed — defend selective intensification, not nihilism, and know your region's policy.[5][6][7][14]
When to EEG: seizure suspicion, fluctuating consciousness, encephalopathy, AE red flags, non-convulsive status concern.[8][11]
When to LP: fever/meningism, immunodeficiency, subacute progressive psychosis with cognitive change, AE red flags, unexplained encephalitis picture — image first if raised ICP risk. Pair CSF with serum for cell-based assay neuronal antibodies when AE is on the table; commercial serum-only screens can false-reassure or false-alarm.[8][9][11]
[12] [10] [9]Acute and emergency management
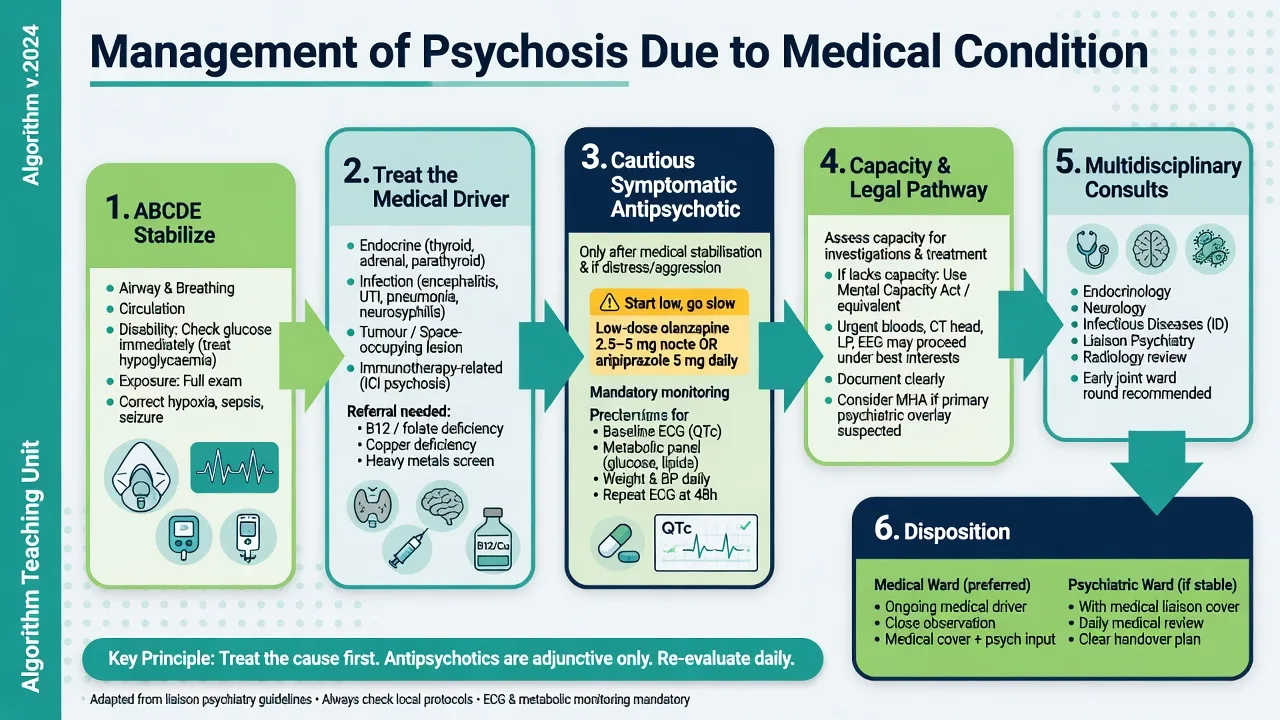
- ABCDE — correct hypoxia, hypoglycaemia, sepsis source control, seizure management.
- Do not delay medical treatment for a perfect psychiatric formulation.
- Agitation: environmental measures first; benzodiazepines when anxiety/catatonia/alcohol-withdrawal pathway fits; low-dose antipsychotics if psychosis-driven risk requires them.
- Avoid high-potency typical loading in suspected Wilson disease, Lewy body spectrum, or malignant catatonia/AE without senior input — EPS and NMS risk climb in organic brain disease.
- Document capacity and legal pathway for invasive tests.[14][4][3]
Definitive management
Primary principle: treat the medical driver. Endocrine control/replacement, antimicrobials, neurosurgical referral, B12 replacement, copper-directed therapy for Wilson disease, steroid wean when safe, and immunotherapy referral for probable AE are disease-modifying. Symptomatic antipsychotics are adjuncts, not the cure.[1][8][10][17]
Symptomatic antipsychotic examples (exam-ready)
Start low, reassess daily once the medical driver is addressed, and plan shortest effective course when psychosis is clearly secondary and remitting.[15][14]
| Scenario | Example plan | Monitoring |
|---|---|---|
| Agitated secondary psychosis, oral possible | Olanzapine 2.5–5 mg orally (nocte or divided); increase cautiously | Sedation, metabolic panel, weight; ECG if cardiac risk |
| Preference for lower metabolic burden | Aripiprazole 5–10 mg orally daily | Akathisia, ECG as indicated |
| IM needed, short-term | Olanzapine IM per local protocol or low-dose haloperidol only with QTc/EPS caution | Continuous observation; avoid in Lewy body / high NMS risk |
| Catatonia prominent | Lorazepam challenge/treatment pathway first; AE work-up if organic flags | Respiratory status; medical review |
International consensus dosing reminds examiners that first presentations and medically fragile brains often need lower chlorpromazine-equivalent doses than multi-episode primary schizophrenia.[15]
RANZCP schizophrenia CPGs embed physical health assessment, baseline investigations, and metabolic/ECG monitoring as non-negotiable when antipsychotics are used — the same standards apply when the psychosis is secondary.[14]
Subtypes and scenarios examiners love
- Endocrine psychosis — thyrotoxic psychosis; myxoedema-associated psychosis (historical "myxoedema madness"); Cushing; hypercalcaemia.
- Steroid-associated — dose and temporal relationship; often coded medication-induced; psychiatric syndromes range from mania to psychosis (Warrington).[17]
- Epilepsy-related — ictal, post-ictal, interictal psychosis; TLE classic stem.
- Space-occupying / post-stroke / TBI — personality change and psychosis spectrum.
- AE red-flag case — young woman, subacute psychosis, then seizures/dyskinesias — hand off to AE pathway for Graus/Pollak criteria and immunotherapy.[8][9][10]
- Wilson / porphyria / B12 — metabolic stems that punish premature primary labels.[3]
- HIV and neurosyphilis — still board-relevant.
- CL/ICU — post-operative, steroid pulses, complex multi-organ drivers.
Complications and pitfalls
- Premature primary schizophrenia label that freezes work-up.
- Missing delirium.
- Serum-only antibody false reassurance.
- High-dose antipsychotics in Wilson or AE precipitating severe EPS/NMS.
- Ignoring steroid timeline.
- Failing tumour search once NMDAR confirmed (AE topic detail, but name the duty).[10][3][8]
- Capacity neglect for LP/MRI.
Prognosis and disposition
Prognosis tracks reversibility and time-to-treatment of the medical driver. Many endocrine and metabolic psychoses improve with cause control; AE outcomes improve with early immunotherapy (Titulaer cohort for NMDAR); advanced structural or untreated Wilson disease may leave residual cognitive–psychiatric burden.[10][1]
Disposition: medical ward with psychiatric liaison when the driver is active; psychiatric ward only if medically stable with documented medical cover; community follow-up for residual symptoms and antipsychotic taper planning. If exhaustive work-up finds no driver, revise toward primary pathway without scorning the organic search that was done.[1][14]
Special populations
- Older adults: higher organic prior (infection, metabolic, subdural, polypharmacy, neurodegenerative psychosis) — low-and-slow psychotropics.
- Youth: AE and substance top the miss list; rare IEMs when atypical.
- Pregnancy: do not delay indicated imaging/treatment; obstetric medicine partnership.
- Intellectual disability: fight diagnostic overshadowing.
- Cultural/Indigenous care: interpreters; physical illness disparity; culture never "explains away" fever, seizure, or focal signs.[1][2][14]
Evidence and regional guidelines
| Source | Pearl for viva |
|---|---|
| Keshavan secondary psychoses | Conceptual taxonomy of secondary vs primary |
| Griswold AFP | Practical medical differential for psychosis |
| Bonnot | Metabolic/IEM secondary psychosis |
| Forbes / Sommer / Blackman | Neuroimaging yield and the scan debate |
| Pollak + Graus + Titulaer + Dalmau | AE/autoimmune psychosis recognition and outcomes (depth in AE topic) |
| RANZCP Galletly CPGs | Organic exclusion, physical health, monitoring in ANZ practice |
| Warrington | Corticosteroid psychiatric adverse effects |
| Gardner dosing | Lower-dose thinking for sensitive brains |
ANZ (RANZCP): expect documented physical examination, baseline labs and metabolic/ECG monitoring when antipsychotics start; organic differentials are explicit in schizophrenia-related guidance.[14] UK (NICE psychosis pathway spirit): physical health assessment and early intervention pathways; imaging policy is selective rather than universal in many services — defend clinical indication. US (APA-influenced practice): often lower threshold for neuroimaging in FEP in some centres; know the debate literature rather than dogma.[5][7]
Exam pearls
[1] [2] [1] [2] [12] [9]ORGANIC work-up cue
Classic stems
- 52-year-old first psychosis + weight loss + heat intolerance → thyroid + full Tier 1, not "late-onset schizophrenia" alone.
- 24-year-old woman subacute psychosis then seizures and orofacial movements → AE pathway now.
- 19-year-old psychosis + abnormal LFTs + tremor → copper studies; careful antipsychotic choice.
- COPD flare on high-dose prednisolone with mania/psychosis → steroid-related framing (often medication-induced coding) + medical review of dose.
- Older man progressive psychosis + Argyll Robertson context or HIV risk → syphilis/HIV serology.[1][2][3][11][17]
Related atlas leaves
- Autoimmune encephalitis and organic psychosis — full Graus/Pollak, antibody map, immunotherapy.
- First-episode psychosis — pathway care after organicity addressed.
- Delirium — exclusive fluctuating inattention syndrome.
- Epilepsy and psychiatry — ictal/post-ictal/interictal detail.
- Late-onset psychosis — old-age priors and imaging thresholds.[8][1]
References
- [1]Keshavan MS, Kaneko Y Secondary psychoses: an update World Psychiatry, 2013.PMID 23471787
- [2]Griswold KS, Del Regno PA, Berger RC Recognition and Differential Diagnosis of Psychosis in Primary Care Am Fam Physician, 2015.PMID 26131945
- [3]Bonnot O, Klünemann HH, Sedel F, et al. Secondary psychosis induced by metabolic disorders Front Neurosci, 2015.PMID 26074754
- [4]McKee J, Brahm N Medical mimics: Differential diagnostic considerations for psychiatric symptoms Ment Health Clin, 2016.PMID 29955484
- [5]Forbes M, Stefler D, Velakoulis D, et al. The clinical utility of structural neuroimaging in first-episode psychosis: A systematic review Aust N Z J Psychiatry, 2019.PMID 31113237
- [6]Sommer IE, de Kort GA, Meijering AL, et al. How frequent are radiological abnormalities in patients with psychosis? A review of 1379 MRI scans Schizophr Bull, 2013.PMID 22416264
- [7]Blackman G, Nour MM, Joyce DW, et al. Prevalence of Neuroradiological Abnormalities in First-Episode Psychosis: A Systematic Review and Meta-analysis JAMA Psychiatry, 2023.PMID 37436735
- [8]Pollak TA, Lennox BR, Müller S, et al. Autoimmune psychosis: an international consensus on an approach to the diagnosis and management of psychosis of suspected autoimmune origin Lancet Psychiatry, 2020.PMID 31669058
- [9]Graus F, Titulaer MJ, Balu R, et al. A clinical approach to diagnosis of autoimmune encephalitis Lancet Neurol, 2016.PMID 26906964
- [10]Titulaer MJ, McCracken L, Gabilondo I, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study Lancet Neurol, 2013.PMID 23290630
- [11]Herken J, Prüss H Red Flags: Clinical Signs for Identifying Autoimmune Encephalitis in Psychiatric Patients Front Psychiatry, 2017.PMID 28261116
- [12]Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies Lancet Neurol, 2008.PMID 18851928
- [13]Al-Diwani A, Handel A, Townsend L, et al. The psychopathology of NMDAR-antibody encephalitis in adults: a systematic review and phenotypic analysis of individual patient data Lancet Psychiatry, 2019.PMID 30765329
- [14]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [15]Gardner DM, Murphy AL, O'Donnell H, et al. International consensus study of antipsychotic dosing Am J Psychiatry, 2010.PMID 20360319
- [16]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [17]Warrington TP, Bostwick JM Psychiatric adverse effects of corticosteroids Mayo Clin Proc, 2006.PMID 17036562
- [18]Dalmau J, Graus F Antibody-Mediated Encephalitis N Engl J Med, 2018.PMID 29490181