Psych · General adult psychiatry — psychosocial rehabilitation in psychosis
Psychosocial rehabilitation in psychosis
Also known as Psychiatric rehabilitation schizophrenia · Psychosocial interventions psychosis · Supported employment IPS psychosis · Family psychoeducation schizophrenia · Cognitive remediation schizophrenia · Social skills training schizophrenia · Illness management and recovery · Recovery-oriented care psychosis
Exam-exhaustive fellowship topic on psychosocial rehabilitation for schizophrenia-spectrum and other psychotic disorders — recovery constructs, PORT-aligned packages (family psychoeducation, IPS, cognitive remediation, skills training, IMR, ACT/ICM), FEP vocational pathways, fidelity, and RANZCP/NICE/APA frames. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
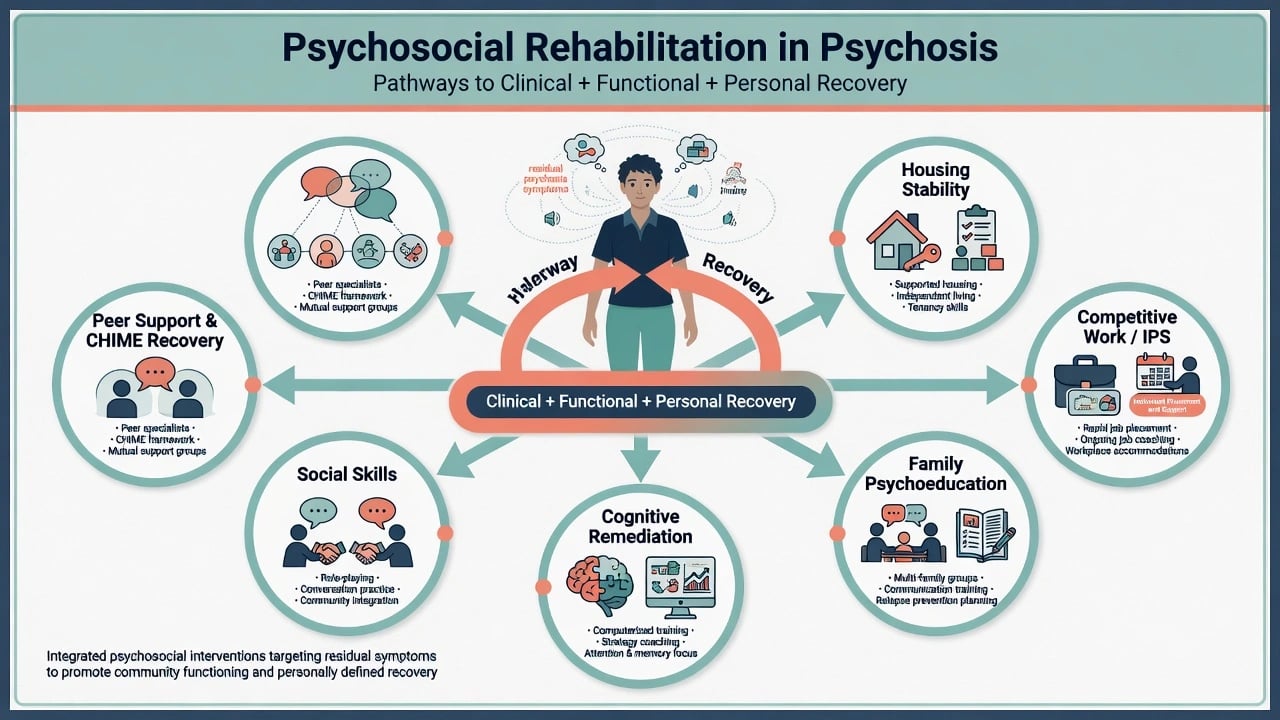
This leaf is the psychosis-specific rehabilitation map. Service-system models (ACT fidelity minutiae, Housing First service design, Clubhouse) are covered in depth in linked public-community topics; here the examiner target is what to prescribe as psychosocial care when the diagnosis is psychosis and the outcome is citizenship.[1][14]
Definition and classification
Psychosocial (psychiatric) rehabilitation in psychosis is coordinated intervention across skills, supports, environments and opportunity structures so people with schizophrenia-spectrum and related psychotic disorders can achieve valued community roles. Acute pharmacotherapy and crisis care stabilise risk and positive symptoms; rehabilitation targets the disability that remains — and the disability that was always multi-determined.[1][14]
Three recovery constructs examiners test
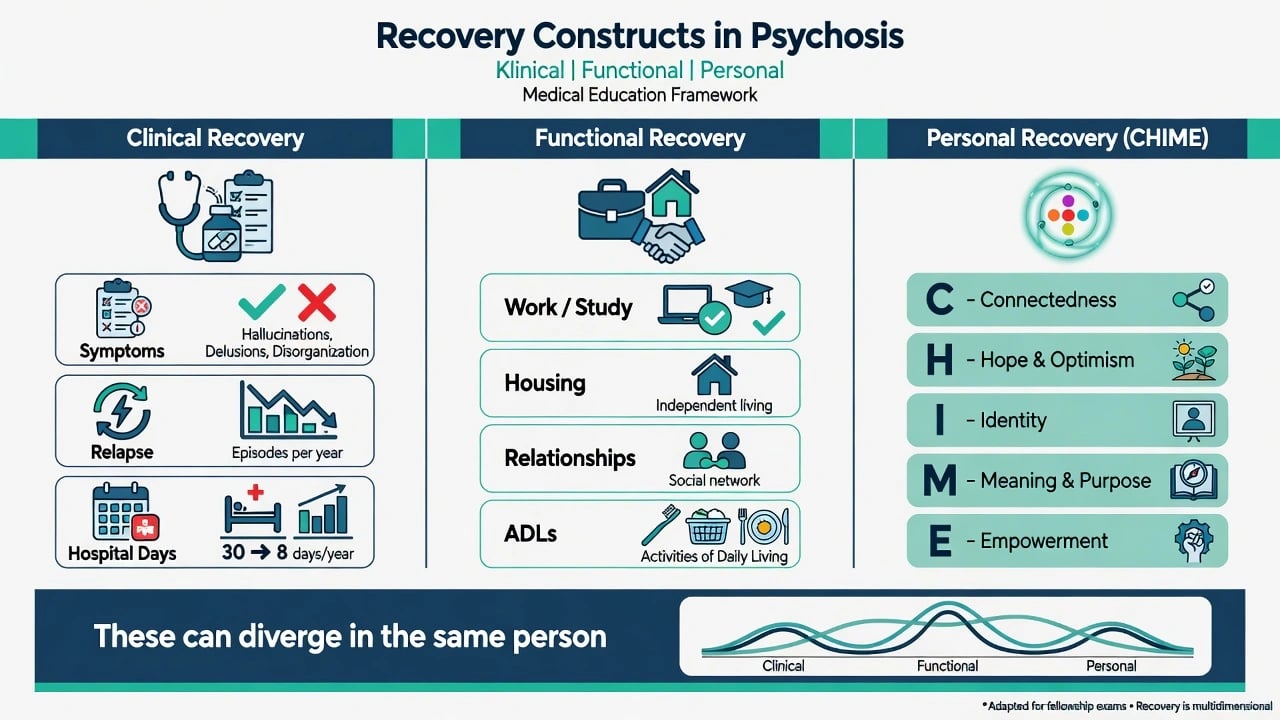
| Construct | Focus | Typical metrics | Exam trap |
|---|---|---|---|
| Clinical recovery | Symptoms, relapse, insight | CGI, PANSS-type scores, hospital days | Treating scores as the only goal |
| Functional recovery | Work, study, housing, ADLs, relationships | Employment rate, independent living | Assuming function automatically follows symptom scores |
| Personal recovery | Person-defined meaningful life | CHIME domains, goal attainment | Using "recovery" as a KPI for premature discharge |
CHIME (Leamy and colleagues): Connectedness, Hope, Identity, Meaning, Empowerment.[12] Slade and colleagues warn of uses and abuses of recovery — including recovery rhetoric used to deny evidence-based care or force premature discharge.[13]
Evidence-based package map (PORT scaffolding)
The 2009 schizophrenia PORT psychosocial recommendations remain high-yield exam scaffolding: family-based interventions, supported employment, skills training, CBT for residual symptoms in indicated groups, and assertive community treatment for selected high-need populations — always alongside appropriate pharmacotherapy.[1]
Epidemiology and risk factors
Unemployment, under-employment and social exclusion are common after schizophrenia-spectrum illness and are major population-health and rights outcomes, not soft afterthoughts.[2][4] Cognitive and negative symptom burden drives functional disability often more than residual positive scores alone — this is why "voices quieter" is an incomplete discharge summary.[5][6]
Revolving-door risk concentrates where engagement is fragile, dual diagnosis is untreated, community intensity is inadequate, and family high expressed emotion (EE) is unaddressed.[7][8][15] People with high hospital use and multi-need psychosis are the classic ACT/ICM target group; intensity should match need, not institutional habit.[15]
Signals examiners expect
Mechanisms of disability and recovery
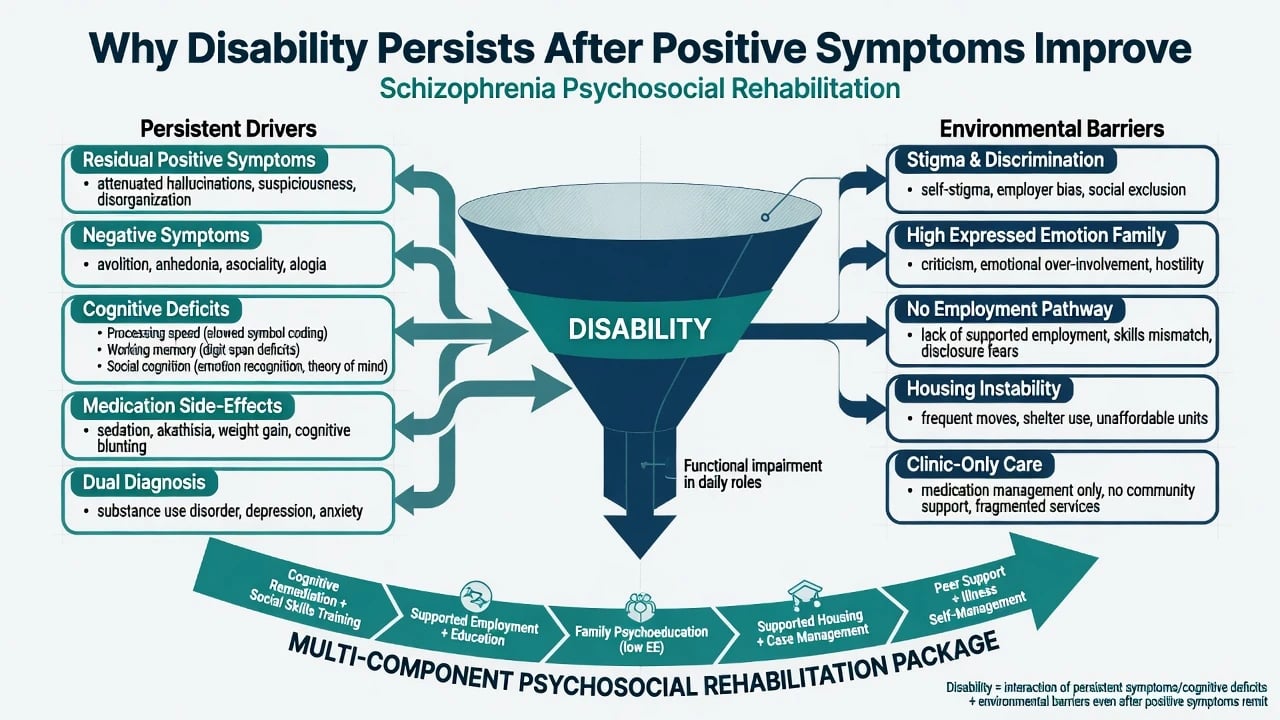
Disability after psychosis is the product of residual positives, negatives, neurocognitive deficits (processing speed, working memory, social cognition), skills gaps, medication side-effects, dual diagnosis, stigma, and opportunity structure — not symptoms alone.[1][5] Place-then-train logic (IPS) places people rapidly into competitive jobs with ongoing support rather than prolonged prevocational training that delays real roles.[2][3] Skills generalise better when taught in vivo in natural environments; clinic-only rehearsal often fails transfer.[1][15] Hope, identity and social capital mediate personal recovery under the CHIME framework.[12]
Clinical presentation (exam stems)
Classic stems examiners recycle: residual schizophrenia with quiet positives, severe unemployment and isolation; first-episode psychosis wanting study or work while family urges "full cure first"; revolving-door admissions with clinic DNA and no outreach; high-EE household after discharge with no structured family work; cognitive barrier sabotaging a supported-employment trial; dual diagnosis and housing instability mislabelled as "non-compliance"; token "rehab group" without competitive employment pathway.[1][2][10][14]
MSE/function interface: residual voices with intact goals; avolition versus skill deficit versus opportunity barrier; partial insight with recovery goals still present. Service presentation: fragmented agencies, no fixed point of responsibility, recovery KPI language without package fidelity.[1][13][14]
Differential and model contrasts
IPS (place-then-train)
- Competitive jobs
- Rapid placement
- Zero exclusion / desire to work
- Integrated vocational specialist
- Time-unlimited support
Train-and-place
- Prolonged prevocational training
- Readiness thresholds
- Delayed real jobs
- Cream-skimming risk
- Often weaker competitive outcomes
ACT / ICM
- Low shared caseload
- In-vivo outreach
- High hospital users
- Engagement focus
- Not a brand without fidelity
Standard CMHT
- Higher caseloads
- More clinic-based
- Appropriate for many
- May under-serve revolving-door
- Step up when intensity fails
Contrast personal recovery goals with clinician-only clinical recovery targets; contrast recovery-oriented care with under-treatment dressed as autonomy.[12][13] Contrast cognitive remediation integrated with rehabilitation versus isolated computer drill without role transfer.[5][6] Always separate secondary functional loss (EPS, depression, oversedation, paranoia-driven withdrawal) from primary disability needing long-horizon rehab.[14]
Bedside assessment
Map functional domains: housing, work/education, ADLs, relationships, finances, community participation, physical health. Elicit person-defined goals (CHIME language) and concurrent clinical risk, capacity and substance use.[12][14]
Vocational assessment for IPS: desire to work is the primary eligibility criterion — do not cream-skim only the "job-ready". Assess preferences, disclosure choices, and side-effect trade-offs that affect workplace performance (sedation, akathisia, weight).[2][16]
Cognition: when processing speed, working memory or social cognition clearly limit roles, consider formal assessment and cognitive remediation linked to real goals, not drill for its own sake.[5][6] Assess family EE and carer burden; dual diagnosis; housing status; intensity fit for ACT/ICM versus standard community care.[7][15]
Investigations and measurement
There is no pathognomonic laboratory test for rehab need. "Investigate" the service map, programme fidelity, entitlements, and physical health screening for SMI populations. Track goal attainment, employment status, hospital days, housing stability and engagement — not only symptom scales.[1][4] Cognitive testing is indicated when results change remediation or education planning. Metabolic panel and ECG remain relevant when optimising antipsychotics toward regimens compatible with work and self-care goals.[14][16]
Acute and emergency management
Stabilise secondary drivers of pseudo-disability before declaring rehab failure: reduce EPS and unnecessary sedation, treat depression, address residual positives and substances, then re-assess goals.[14]
Definitive multi-component management
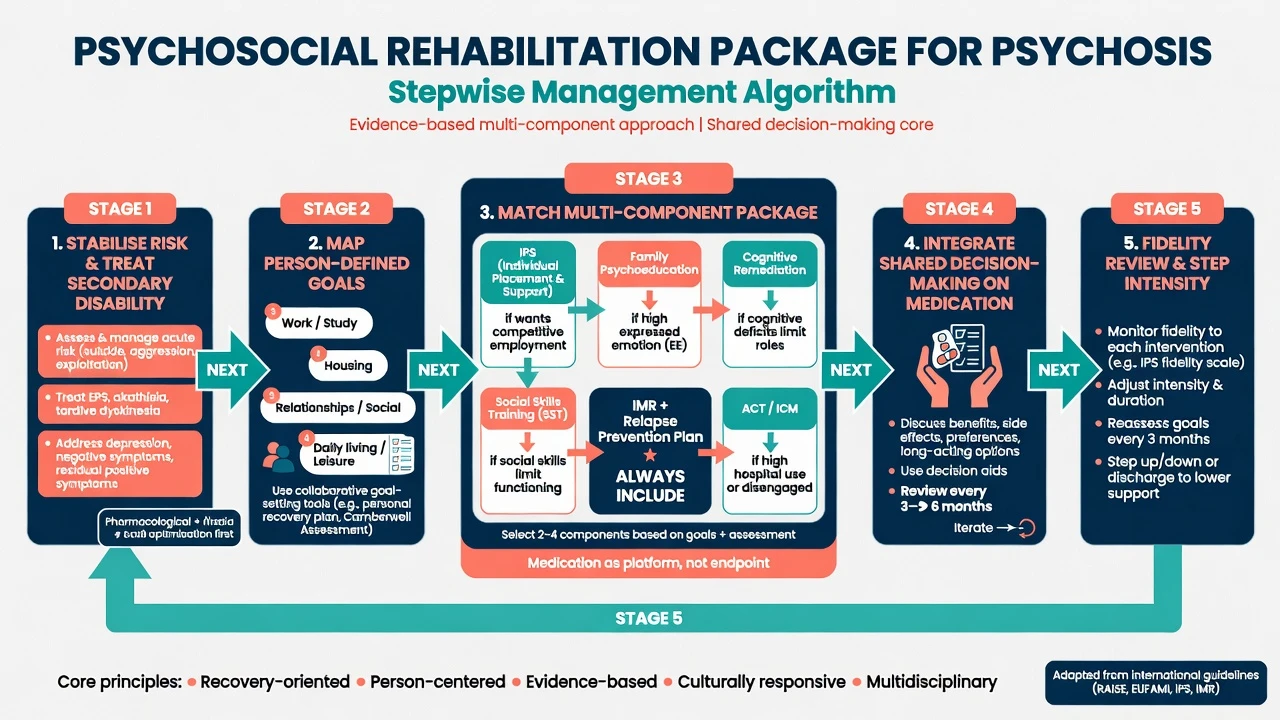
1. Optimise medical and psychiatric foundation
Antipsychotic care remains core; shared decision-making links dose, formulation (including LAI when adherence/risk justify) and side-effect profile to recovery goals such as work and parenting.[14][16] Example shared-decision language when an examiner forces a named residual-symptom plan (individualise; check local product information): for a person with residual positive symptoms impairing roles who is adherent and metabolically stable on aripiprazole 15 mg orally once daily, review akathisia, sleep and function at 1–2 weeks and consider whether dose adjustment, switch, LAI conversion or psychological strategies better serve stated goals — do not escalate polypharmacy by default "for rehab".[14][16]
2. Family psychoeducation
Structured family psychoeducation (illness education, communication training, problem-solving, reduced high EE) reduces relapse and hospitalisation compared with usual care when programmes are real, not one-off pamphlets.[7][8] PORT and RANZCP guidance treat family work as core schizophrenia care where family is involved.[1][14]
3. IPS supported employment (and education)
IPS principles examiners must name: competitive employment as the goal, rapid job search, zero exclusion based on readiness tests, integration of employment specialists with mental health care, attention to client preferences, time-unlimited support, and benefits counselling as needed.[2][3] Meta-analytic and multi-country RCT evidence shows substantially higher competitive employment rates than traditional vocational approaches; EQOLISE demonstrated effectiveness in European settings; international meta-analysis supports generalisability.[3][4] In first-episode psychosis, Killackey and colleagues showed IPS improves vocational recovery versus control.[11]
4. Cognitive remediation
Meta-analyses (Wykes; Vita) support modest-to-moderate cognitive gains; functional transfer is stronger when remediation is integrated with psychiatric rehabilitation and active coaching rather than isolated drill.[5][6] Core elements include massed practice, strategy coaching, and bridging to real-world tasks.
5. Social skills training and illness management
Skills training (communication, assertiveness, problem-solving, community living skills) is PORT-aligned for functional social competence deficits.[1] Illness Management and Recovery (IMR) packages psychoeducation, relapse planning, coping skills and recovery goal setting on a researched curriculum base.[9] CBT for psychosis elements address residual distress and conviction where available and indicated.[1][14]
6. Intensity: ACT / ICM when needed
Intensive case management / ACT-class models reduce hospital use and improve engagement for high-need SMI; functional gains are more variable. Critical ingredients include small shared caseloads, team approach, in-vivo outreach and high contact — brand names without fidelity are exam traps.[15]
7. First-episode multi-element packages
RAISE-ETP comprehensive care (medication, family psychoeducation, individual resilience training, supported employment/education) improved outcomes versus usual community care at two years — the exam message is multi-element early care including vocational recovery, not antipsychotic monotherapy alone.[10][11]
Subtypes and scenarios
FEP / youth. Protect education and early competitive roles; integrate supported education with IPS principles; avoid automatic abandonment of study.[10][11]
Long-term residual schizophrenia. Negative and cognitive disability dominate; package remediation + skills + IPS + family work; optimise secondary causes first.[5][14]
Treatment-resistant residual positives. Clozapine or other TRS pathways may be needed for clinical recovery while rehab continues in parallel — TRS is not a reason to cancel roles forever; PORT psychosocial packages still apply alongside optimised pharmacotherapy.[1][14]
Dual diagnosis and housing instability. Integrate substance treatment; intensity and housing platforms matter; do not make housing a reward for perfect abstinence if Housing First principles apply locally (jurisdiction-specific service design).[14][15]
Forensic interface. Graduated community leave, offence-linked goals, multi-agency fixed responsibility; recovery packages continue under legal frameworks without inventing local statutes.[13][14]
Rural and low-resource. Flexible assertive outreach; prioritise family PE and IPS-like rapid placement where full ACT staffing is impossible; fidelity spirit over brand.[2][7][15]
Cultural adaptation. Family structures, spiritual meaning and community roles shape personal recovery — adapt CHIME delivery without abandoning evidence packages.[12][14]
Complications and pitfalls
- Recovery rhetoric as under-treatment or premature discharge (Slade abuses)[13]
- Train-and-place delays and cream-skimming
- Low-fidelity "ACT" without caseload, shared team or outreach
- Cognitive remediation as computer drill without role transfer
- Ignoring secondary negatives while pushing rehab intensity
- Family contact that increases EE without structured psychoeducation
- Fragmentation with no fixed responsibility
- Sheltered-only pathways when the person wants competitive work
- Medication polypharmacy that sabotages work via sedation
Prognosis and disposition
IPS approximately doubles competitive employment odds relative to control vocational services in systematic reviews — exact ratios vary by trial but the direction is consistent and examinable.[4] Family psychoeducation reduces relapse risk when delivered properly.[7][8] Cognitive remediation improves cognition with better functional transfer when integrated.[5][6] ACT/ICM mainly cut hospital days and improve engagement.[15] FEP multi-element care beats fragmented usual care on symptoms, engagement and role outcomes in landmark programmes.[10]
Disposition is iterative: step intensity to need, review goals, do not stamp "rehab complete" after a six-week group. Long-term recovery is a trajectory, not a certificate.[12][14]
Special populations
Older adults: pace goals, address physical comorbidity and isolation, avoid ageist exclusion from IPS-like pathways. Intellectual disability and psychosis: adapted skills training and capacity supports. Pregnancy and parenting: parenting skills, safeguarding interface, shared decision-making on medication. Indigenous and culturally diverse groups: culturally safe family and community role work. Forensic restricted patients: graduated leave and offence-linked rehab goals under legal frameworks — state principles only; do not invent statutes.[14]
Evidence and regional guidelines
| Source | Exam use |
|---|---|
| PORT 2009 psychosocial (Dixon) | Package scaffolding for schizophrenia psychosocial care |
| Bond / Burns / Modini IPS | Supported employment evidence ladder |
| Wykes / Vita | Cognitive remediation effect sizes and moderators |
| McFarlane / Pharoah | Family psychoeducation and family intervention |
| Mueser IMR | Illness management curriculum evidence |
| Kane RAISE-ETP / Killackey IPS-FEP | Early psychosis multi-element and vocational RCTs |
| Dieterich ICM | Intensity for high-need SMI |
| Leamy CHIME / Slade | Personal recovery and recovery abuses |
| RANZCP schizophrenia guideline | ANZ psychosocial recommendations |
| NICE / APA schizophrenia guidance | International psychosocial themes — compare, do not invent local law |
ANZ (RANZCP): multi-element schizophrenia care explicitly includes psychosocial interventions, family work, vocational support and recovery orientation; recovery rhetoric must not replace evidence-based care.[14] UK (NICE themes): family intervention, CBT for psychosis, and vocational support are expected components for schizophrenia/psychosis pathways. US (APA practice guideline themes): psychosocial treatments including family, supported employment and skills interventions sit alongside pharmacotherapy. Always apply local mental health law for involuntary care, disability supports and employment rights without inventing form codes.[1][13][14]
Exam pearls
RECOVER-P package mnemonic
References
- [1]Dixon LB, Dickerson F, Bellack AS, et al. The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements Schizophr Bull, 2010.PMID 19955389
- [2]Bond GR, Drake RE, Becker DR An update on randomized controlled trials of evidence-based supported employment Psychiatr Rehabil J, 2008.PMID 18407876
- [3]Burns T, Catty J, Becker T, et al. The effectiveness of supported employment for people with severe mental illness: a randomised controlled trial Lancet, 2007.PMID 17905167
- [4]Modini M, Tan L, Brinchmann B, et al. Supported employment for people with severe mental illness: systematic review and meta-analysis of the international evidence Br J Psychiatry, 2016.PMID 27103678
- [5]Wykes T, Huddy V, Cellard C, et al. A meta-analysis of cognitive remediation for schizophrenia: methodology and effect sizes Am J Psychiatry, 2011.PMID 21406461
- [6]Vita A, Barlati S, Ceraso A, et al. Effectiveness, Core Elements, and Moderators of Response of Cognitive Remediation for Schizophrenia: A Systematic Review and Meta-analysis of Randomized Clinical Trials JAMA Psychiatry, 2021.PMID 33877289
- [7]McFarlane WR, Dixon L, Lukens E, et al. Family psychoeducation and schizophrenia: a review of the literature J Marital Fam Ther, 2003.PMID 12728780
- [8]Pharoah F, Mari J, Rathbone J, et al. Family intervention for schizophrenia Cochrane Database Syst Rev, 2010.PMID 21154340
- [9]Mueser KT, Corrigan PW, Hilton DW, et al. Illness management and recovery: a review of the research Psychiatr Serv, 2002.PMID 12364675
- [10]Kane JM, Robinson DG, Schooler NR, et al. Comprehensive Versus Usual Community Care for First-Episode Psychosis: 2-Year Outcomes From the NIMH RAISE Early Treatment Program Am J Psychiatry, 2016.PMID 26481174
- [11]Killackey E, Allott K, Jackson HJ, et al. Individual placement and support for vocational recovery in first-episode psychosis: randomised controlled trial Br J Psychiatry, 2019.PMID 30251616
- [12]Leamy M, Bird V, Le Boutillier C, et al. Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis Br J Psychiatry, 2011.PMID 22130746
- [13]Slade M, Amering M, Farkas M, et al. Uses and abuses of recovery: implementing recovery-oriented practices in mental health systems World Psychiatry, 2014.PMID 24497237
- [14]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [15]Dieterich M, Irving CB, Bergman H, et al. Intensive case management for severe mental illness Cochrane Database Syst Rev, 2017.PMID 28067944
- [16]Deegan PE, Drake RE Shared decision making and medication management in the recovery process Psychiatr Serv, 2006.PMID 17085613