Psych · General adult psychiatry — mood disorders
Psychotic depression
Also known as Major depression with psychotic features · Delusional depression · Depressive episode with psychotic symptoms · MDD with mood-congruent psychotic features · MDD with mood-incongruent psychotic features · Psychotic major depressive disorder
Exam-exhaustive fellowship reference on major depression with psychotic features — DSM-5-TR/ICD-11 framing, mood-congruent vs incongruent content, elevated suicide risk, combination antidepressant plus antipsychotic evidence (STOP-PD, STOP-PD II, Spiker, Cochrane), ECT, differentials from schizophrenia-spectrum and organic psychosis, metabolic monitoring, and maintenance after remission. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
9 MCQs with explanations
Target exams
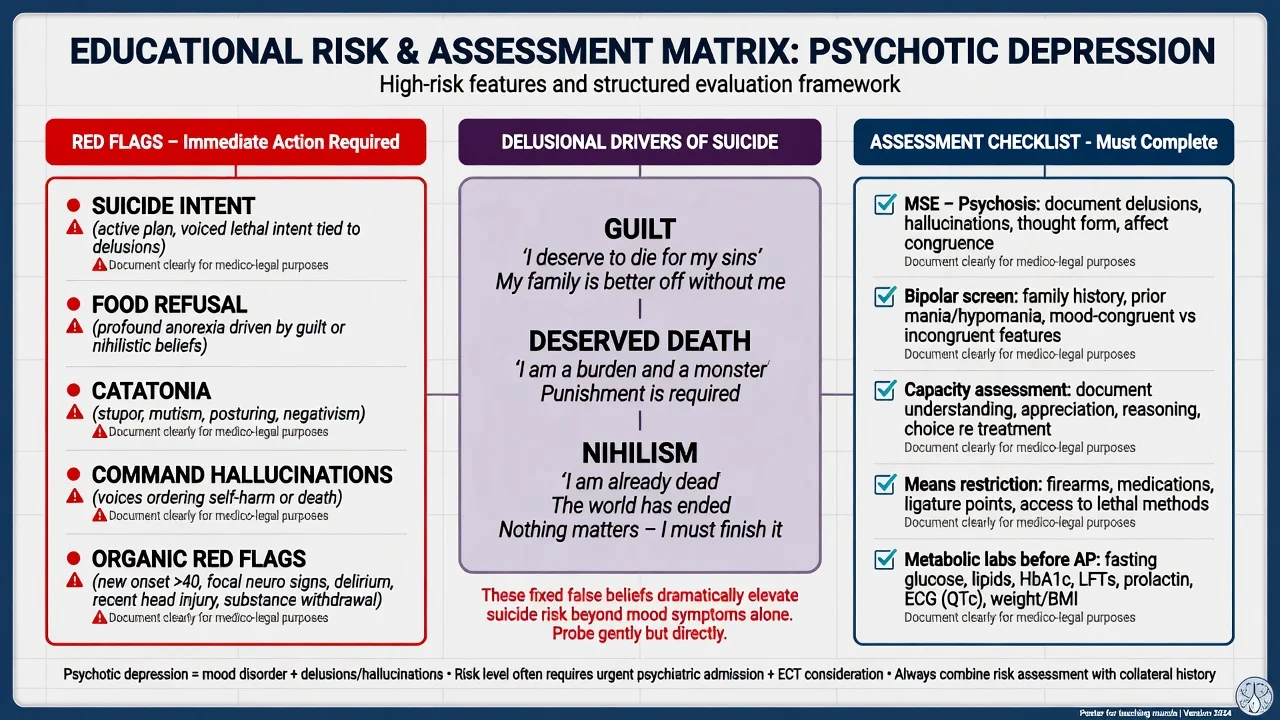
Red flags
Psychotic depression (major depression with psychotic features; historical "delusional depression") is a high-acuity fellowship phenotype. Examiners test whether you can operationalise DSM/ICD criteria, recognise elevated suicide and self-neglect risk, sequence combination pharmacotherapy versus ECT, name STOP-PD / STOP-PD II evidence, and discriminate schizophrenia-spectrum, bipolar, substance, and organic mimics without undergraduate hand-waving.[1][2][10][12]
Overview and definition
Psychotic depression is not a freestanding DSM-5-TR disorder code separate from MDD — it is a specifier applied when delusions and/or hallucinations occur in the context of a major depressive episode (or, in bipolar illness, a depressive episode with psychotic features). ICD-11 uses related language for depressive episodes/disorders with psychotic symptoms. For exams, state the parent mood diagnosis first, then the psychotic specifier, severity, and course.[12]
Operational requirements. The patient meets full major depressive episode criteria (five or more symptoms over the same two-week period with depressed mood or anhedonia as one, plus impairment), and has psychotic symptoms temporally linked to that episode. Psychotic features are typically associated with severe episodes clinically, though you still document severity and function explicitly rather than assuming the label does the work.[12][14]
Mood-congruent vs mood-incongruent. Mood-congruent content thematically matches depressive themes (guilt, deserved punishment, nihilism/Cotard-spectrum, poverty, somatic catastrophe, deserved illness). Mood-incongruent content is not thematically limited to depressive themes (e.g. thought broadcasting, passivity, bizarre persecutory systems without depressive logic). Incongruence widens the schizophrenia-spectrum differential and may colour prognosis discussions — it does not automatically reclassify the episode as schizophrenia if the mood episode is full and primary.[12]
Classification framework
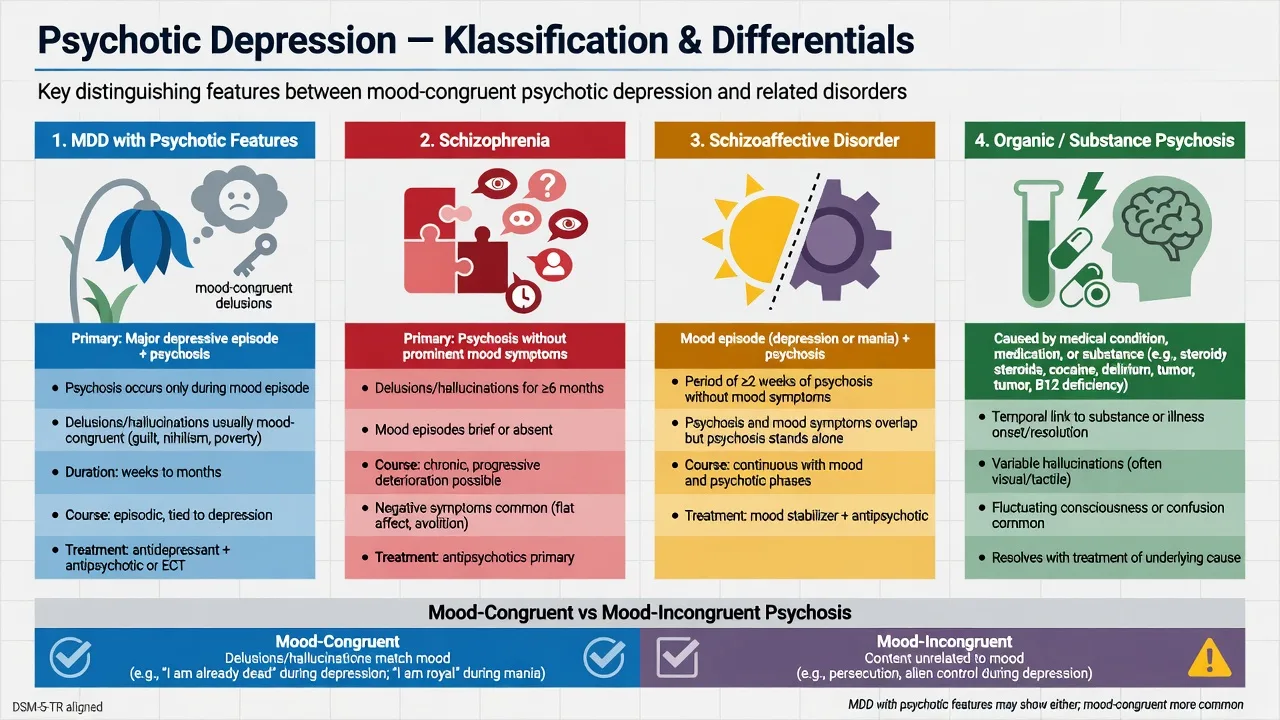
MDD + psychotic features
- Full MDE present
- Delusions and/or hallucinations during episode
- Mood-congruent or incongruent content
- Treat depression AND psychosis
Schizophrenia
- Primary psychosis trajectory
- Mood secondary or brief relative to psychosis
- Negative and cognitive syndrome often prominent
- Duration and functional criteria for schizophrenia
Schizoaffective
- Concurrent full mood + psychosis
- Periods of psychosis without prominent mood
- Longitudinal diagnosis — not a single visit guess
- Do not force after one admission
Bipolar depression + psychosis
- Prior mania/hypomania decisive when present
- Family history and postpartum mania clues
- Long-term mood stabilisation pathway
- Avoid unipolar-only maintenance framing
Historical delusional depression literature (e.g. Spiker combination trials) maps onto modern psychotic-feature language and remains examinable as classic evidence for combination treatment.[5]
Epidemiology and risk
Numbers and signals examiners expect
In a general-population survey, Ohayon and Schatzberg reported that 18.5% of subjects meeting major depressive episode criteria had psychotic features — a reminder that this is not a rare academic curiosity, though rates are higher still in severe inpatient and late-life cohorts than in mild primary-care depression.[9]
Suicide. Systematic review and meta-analysis of psychotic (delusional) depression shows elevated completed-suicide risk relative to non-psychotic depression — examine delusional drivers (guilt, deserved death, nihilism), command content, means, and the false reassurance of psychomotor retardation.[10] Risk assessment is continuous through acute treatment and early recovery, when energy may return before delusions fully clear.
Pathophysiology and mechanisms
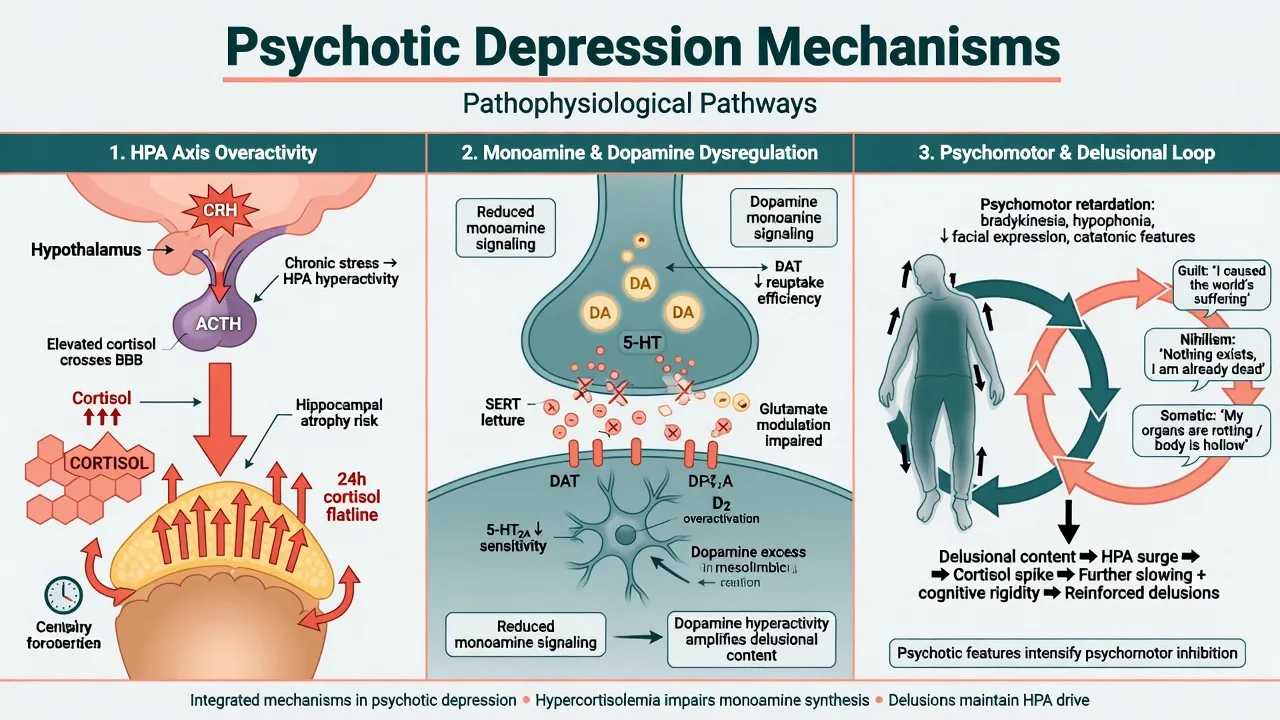
HPA-axis hyperactivity is more consistently emphasised in psychotic than non-psychotic major depression, including alterations of cortisol circadian rhythm and historical DST non-suppression literature. Schatzberg and colleagues frame HPA over-activity as central to pathogenesis and a research drug-development target (e.g. glucocorticoid receptor antagonists in trial programmes) — not a bedside diagnostic test you order to "prove" psychotic depression.[15][16]
Dopamine–monoamine interaction models help explain why antipsychotic monotherapy can blunt psychosis without remitting the depressive pole, and why combination strategies emerged clinically long before STOP-PD. Cognitive content (guilt, nihilism, somatic catastrophe) organises the delusional system once severe negative affect and cognitive rigidity lock in.[16][8]
Clinical presentation
Expect severe low mood and anhedonia with psychomotor retardation or agitation, early waking, marked guilt, and often melancholic neurovegetative change. Psychosis may be delusions alone, hallucinations alone, or both. Classic mood-congruent themes: deserved punishment, financial ruin despite evidence, fatal illness without medical basis, non-existence (Cotard-spectrum), or voices accusing guilt. Insight is often impaired; capacity for treatment decisions may be compromised.[12][9]
High-risk behavioural phenotypes. Food and fluid refusal driven by nihilistic or persecutory beliefs; mutism and staring evolving toward catatonia; quiet patients who "look settled" because retardation hides active planning; sudden "improvement" after deciding on a lethal plan. Collateral history is essential — families often report delusional content the patient minimises.[10][12]
Differential diagnosis
Schizophrenia-spectrum
- Primary psychosis course and functional decline
- Mood not full/primary for the whole episode
- First-rank-type content without depressive organisation
- Longitudinal diagnosis required
Schizoaffective
- Psychosis persists without prominent mood for periods
- Needs time and records — not day-1 label
- Treatment often dual mood + antipsychotic
- Different maintenance questions
Substance / medication
- Stimulants, alcohol, cannabis, steroids
- Timeline locked to exposure/withdrawal
- UDS and collateral
- Treat dual formulation
Organic / medical
- Delirium (fluctuation, attention)
- Encephalitis, endocrine, B12, stroke
- Dementia with psychosis + depression
- Investigate red flags — do not MRI everyone
Also discriminate severe OCD with overvalued ideas, BDD with near-delusional conviction, primary delusional disorder without syndromal depression, and grief with cultural explanatory models that are not delusional.[12]
Assessment
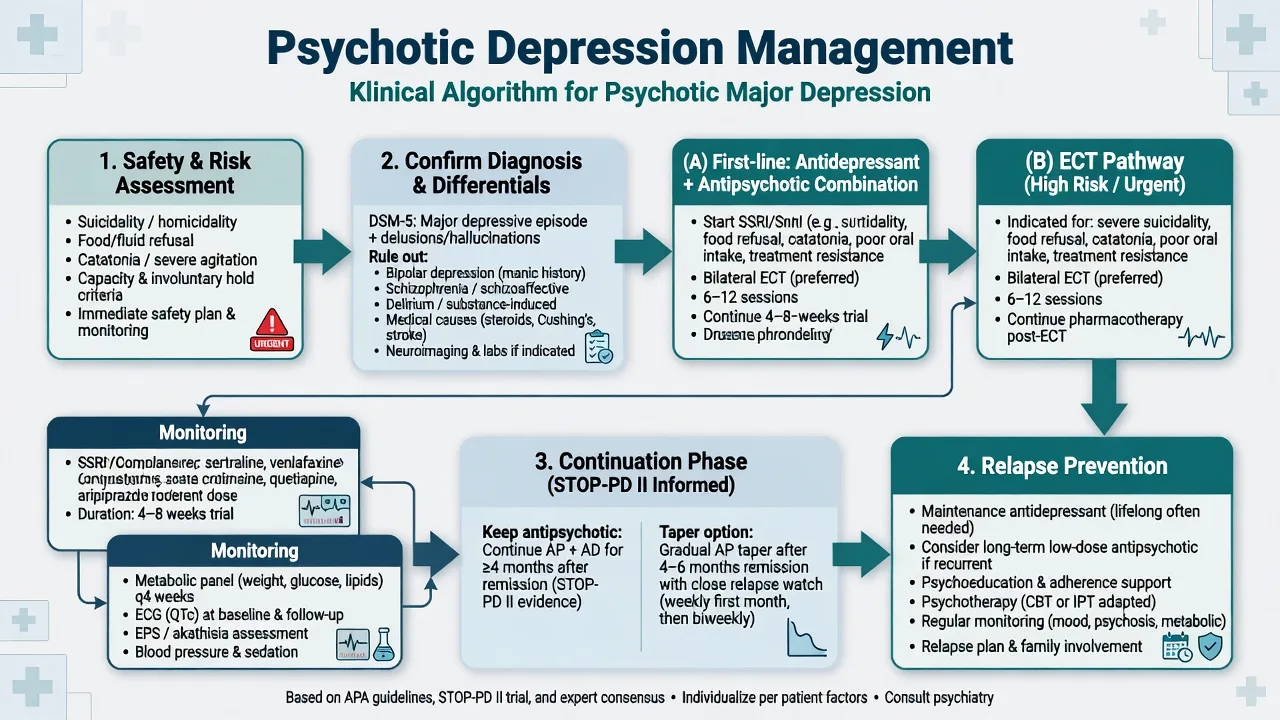
Structure the interview: (1) confirm MDE criteria and severity; (2) catalogue psychotic content (type, mood congruence, command quality, behavioural impact); (3) suicide and self-neglect risk with delusional drivers and means; (4) catatonia screen; (5) bipolar screen every time; (6) substances, medical list, perinatal status; (7) prior treatments (AD, AP, ECT response); (8) capacity and least-restrictive legal pathway under local law (do not invent section numbers); (9) collateral and prior records.[10][12][14]
Scales. PHQ-9 can track depressive severity but under-samples psychosis — use clinician-rated instruments (HAM-D, MADRS) and structured delusion enquiry in hospital settings. PHQ-9 item 9 is not a complete risk assessment.[14]
Investigations
Before combination AD+AP: FBC, U&E, LFT, TSH; glucose, lipids, BMI/waist for metabolic risk; ECG when cardiac risk, older age, QTc-active agents, or high-dose citalopram/escitalopram contexts apply; pregnancy test when relevant; urine drug screen when substance differential is active; B12/folate if indicated. Neuroimaging, EEG, or LP only for organic red flags (late first onset with focal signs, seizure, encephalopathy, autoimmune concern) — not routine for classic recurrent psychotic depression with known prior pattern. Pre-ECT: consent, medical/anaesthetic review, labs/ECG as indicated, medication review (lithium, anticonvulsants, benzodiazepines), cognitive baseline.[1][11][12][13]
Acute / emergency management
Stabilise medical risk (hydration, electrolytes, pressure areas in immobile retardation). Manage agitation with least restrictive safe options while locking a definitive depression plan. Legal status follows jurisdiction-specific capacity and risk thresholds. Watch for NMS if antipsychotics are used, serotonin syndrome if serotonergic load is high, and severe hyponatraemia in older adults on SSRIs.[12]
Definitive management
Combination antidepressant + antipsychotic
The evidence spine for exams includes combination superiority signals from classic and modern trials.[5][1]
- Spiker et al. (1985): amitriptyline + perphenazine superior to either alone in delusional depression — classic combination signal.[5]
- Rothschild et al. (2004): olanzapine/fluoxetine combination (OFC) studied against olanzapine monotherapy and placebo in major depression with psychotic features — supports combination thinking in the atypical era (interpret regional OFC availability carefully).[6]
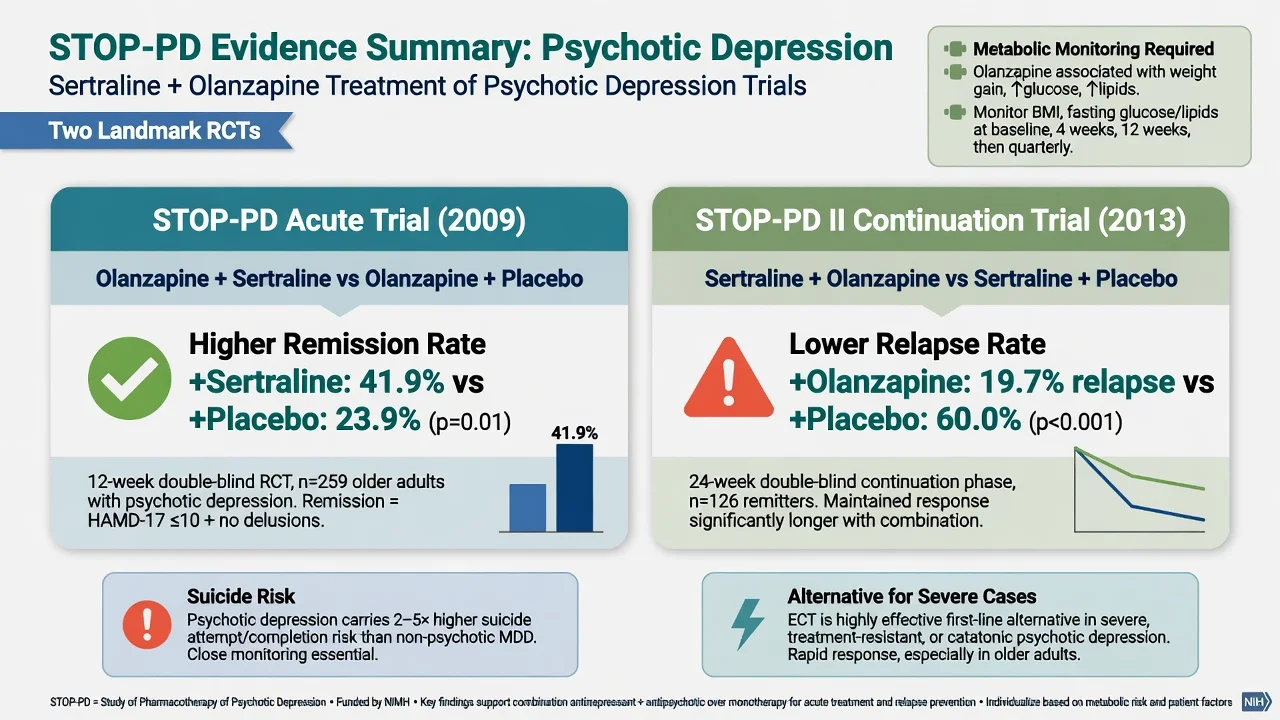
- STOP-PD (Meyers 2009): multicentre RCT — olanzapine + sertraline produced higher remission rates than olanzapine + placebo in psychotic depression. This is the modern combination trial every viva expects by name.[1]
- Wijkstra 2010: imipramine (plasma-level targeted) vs venlafaxine vs venlafaxine + quetiapine — venlafaxine–quetiapine more effective than venlafaxine alone in the published comparison.[7]
- Farahani & Correll (2012) meta-analysis: antidepressant–antipsychotic cotreatment superior to monotherapy with either class for acute psychotic depression.[8]
- Cochrane updates (Wijkstra 2015; Kruizinga 2021): evidence supports combination therapy being more effective than either treatment alone or placebo, while certainty is limited by trial numbers and heterogeneity — state uncertainty honestly.[3][4]
Exam-level dosing example (STOP-PD-aligned agents — individualise). Sertraline often start 50 mg orally daily, titrate toward 150–200 mg as tolerated with response/side-effect review; monitor for GI effects, activation, sexual dysfunction, hyponatraemia (especially older adults), and serotonergic interactions.[1][13] Olanzapine often start 5 mg orally at night (lower in frail elderly), titrate toward the range used in STOP-PD protocols (commonly up to about 15–20 mg as tolerated) with weight, glucose, lipids, sedation, and EPS/akathisia monitoring; ECG/QTc context as indicated.[1][12] Alternative pairs used in practice and trials include venlafaxine (e.g. titrate toward 225–375 mg orally daily if BP allows, as in Wijkstra high-dose arm) plus quetiapine (build carefully; Wijkstra used up to 600 mg in the combination arm — modern practice often uses lower effective ranges with metabolic vigilance).[7] Name the agent, dose, route, titration, and monitoring — vague "start an atypical" fails.
Antipsychotic monotherapy is not an adequate plan for the depressive pole; antidepressant monotherapy is not an adequate plan once psychosis is established.[3][8]
Continuation after remission — STOP-PD II
STOP-PD II (Flint 2019): among patients with psychotic depression who remitted on sertraline plus olanzapine, continuing olanzapine with sertraline reduced relapse risk compared with sertraline plus placebo. The clinical trade-off is metabolic and other antipsychotic adverse effects versus relapse prevention — discuss duration, monitoring, and gradual taper only when stability and supports allow, with a plan for early re-emergence of psychotic symptoms.[2]
ECT
ECT has a strong short-term efficacy signal in severe depressive disorders and is often first-line or early in psychotic depression when suicide risk is high, intake is dangerous, catatonia is present, prior ECT response was excellent, pregnancy risk–benefit favours it, or combination pharmacotherapy fails or is too slow.[11][12] Work-up and consent: benefits, cognitive risks, anaesthetic/cardiac risks, electrode placement trade-offs (right unilateral vs bitemporal), medication adjustments, and continuation/maintenance discussion after late remission in highly recurrent illness. Do not frame ECT as punishment or pure last resort after years of incomplete trials.[11]
Psychotherapy and social interventions
Once acute psychosis and severe cognitive rigidity settle enough for engagement, add psychoeducation, family work, behavioural activation, and CBT-informed approaches targeting residual guilt/rumination. Therapy is adjunctive to biological treatment in the acute severe phase — not a substitute for AD+AP or ECT when risk is high.[12]
Regional guideline deltas
RANZCP mood disorder guidelines emphasise formulation-driven care, bipolar exclusion, staged pharmacological and psychological treatment, and appropriate early use of ECT for severe psychotic and melancholic presentations within Australian and New Zealand service models.[12]
Subtypes and scenarios
Mood-incongruent features. Widen differential toward schizophrenia-spectrum and schizoaffective longitudinal diagnoses; still treat the current severe depressive episode aggressively if criteria are met.[12]
Late-life psychotic depression. Higher rates of psychotic features in severe geriatric depression; somatic delusions common; medical comorbidity; ECT often highly effective; start antipsychotics low and monitor metabolic, fall, and QTc risk.[1][11][12]
Perinatal. Distinguish severe psychotic depression from postpartum psychosis (often bipolar-spectrum, abrupt, confused). Untreated severe illness harms parent and infant; ECT may be preferred; specialist perinatal liaison.[12]
Catatonic features. Lorazepam challenge and urgent ECT pathway; do not attribute mutism solely to "personality" or "oppositionality."[11][12]
Complications and pitfalls
Atypical antipsychotic adverse-effect burden (weight, glucose, lipids, sedation) is real — combination efficacy is not free. Nelson and Papakostas meta-analysis supports atypical augmentation in non-psychotic MDD non-response; in psychotic depression the antipsychotic is treating psychosis as well as mood, but metabolic monitoring still applies.[17][1]
Prognosis and disposition
Acute combination treatment and ECT both produce high response rates in appropriate patients; residual symptoms and residual delusional conviction predict relapse. STOP-PD II shows that premature antipsychotic discontinuation after combination-induced remission increases relapse risk.[1][2] Disposition ladder: intensive community with daily review → voluntary inpatient → involuntary inpatient when risk/capacity thresholds met under local law → ECT suite. STARD sequential lessons apply poorly as a sole algorithm here because STARD enrolled non-psychotic MDD outpatients — do not quote STAR*D remission steps as the primary evidence spine for psychotic depression.[18][1]
Special populations
Older adults
- Higher psychotic-feature rates in severe episodes
- Medical comorbidity and polypharmacy
- ECT often highly effective
- Lower start doses; metabolic/fall/QTc vigilance
Pregnancy
- Untreated severe psychotic depression is not zero-harm
- ECT may be preferred in high-risk illness
- Individualise every agent
- Perinatal specialist liaison
Adolescents
- Rarer phenotype — careful early-psychosis differential
- Family involvement
- Specialist CAMHS
- Limited trial data for many options
Cultural safety
- Explanatory models vs true delusion
- Interpreter and family decision styles
- FRANZCP cultural safety expectations
- Do not pathologise culturally normative beliefs
Population-specific monitoring changes first steps — state them explicitly at viva.[11][12]
Evidence, guidelines and controversies
Landmark pillars: STOP-PD acute combination superiority of sertraline + olanzapine over olanzapine + placebo;[1] STOP-PD II continuation olanzapine for relapse prevention;[2] Spiker 1985 classic TCA + first-generation antipsychotic combination;[5] Rothschild OFC trial;[6] Wijkstra 2010 venlafaxine–quetiapine arm;[7] Farahani–Correll and Cochrane synthesis favouring combination over monotherapy;[3][4][8] Gournellis suicide meta-analysis;[10] Ohayon & Schatzberg prevalence;[9] HPA-axis literature (Keller; Schatzberg);[15][16] UK ECT Review Group;[11] RANZCP 2020 and CANMAT pharmacotherapy framing.[12][13]
Controversies to handle calmly: optimal duration of antipsychotic after remission; metabolic harm versus relapse prevention; whether some patients can remitted on antidepressant alone (evidence overall favours combination); mood-incongruent features and long-term diagnostic revision; access equity for ECT.[2][3][8]
Exam pearls
PSYCHDEP
PSYCHDEP is a memory scaffold for the viva sequence — still apply full formulation and local legal standards.[1][2][12]
References
- [1]Meyers BS, Flint AJ, Rothschild AJ, Mulsant BH, Whyte EM, Peasley-Miklus C, et al. A double-blind randomized controlled trial of olanzapine plus sertraline vs olanzapine plus placebo for psychotic depression: the study of pharmacotherapy of psychotic depression (STOP-PD) Arch Gen Psychiatry, 2009.PMID 19652123
- [2]Flint AJ, Meyers BS, Rothschild AJ, Whyte EM, Alexopoulos GS, Rudorfer MV, et al. Effect of Continuing Olanzapine vs Placebo on Relapse Among Patients With Psychotic Depression in Remission: The STOP-PD II Randomized Clinical Trial JAMA, 2019.PMID 31429896
- [3]Kruizinga J, Liemburg E, Burger H, Cipriani A, Geddes J, Robertson L, et al. Pharmacological treatment for psychotic depression Cochrane Database Syst Rev, 2021.PMID 34875106
- [4]Wijkstra J, Lijmer J, Burger H, Cipriani A, Geddes J, Nolen WA Pharmacological treatment for psychotic depression Cochrane Database Syst Rev, 2015.PMID 26225902
- [5]Spiker DG, Weiss JC, Dealy RS, Griffin SJ, Hanin I, Neil JF, et al. The pharmacological treatment of delusional depression Am J Psychiatry, 1985.PMID 3883815
- [6]Rothschild AJ, Williamson DJ, Tohen MF, Schatzberg A, Andersen SW, Van Campen LE, et al. A double-blind, randomized study of olanzapine and olanzapine/fluoxetine combination for major depression with psychotic features J Clin Psychopharmacol, 2004.PMID 15232326
- [7]Wijkstra J, Burger H, van den Broek WW, Birkenhäger TK, Janzing JG, Boks MP, et al. Treatment of unipolar psychotic depression: a randomized, double-blind study comparing imipramine, venlafaxine, and venlafaxine plus quetiapine Acta Psychiatr Scand, 2010.PMID 19694628
- [8]Farahani A, Correll CU Are antipsychotics or antidepressants needed for psychotic depression? A systematic review and meta-analysis of trials comparing antidepressant or antipsychotic monotherapy with combination treatment J Clin Psychiatry, 2012.PMID 22579147
- [9]Ohayon MM, Schatzberg AF Prevalence of depressive episodes with psychotic features in the general population Am J Psychiatry, 2002.PMID 12411219
- [10]Gournellis R, Tournikioti K, Touloumi G, Thomadakis C, Michalopoulou PG, Christodoulou C, et al. Psychotic (delusional) depression and completed suicide: a systematic review and meta-analysis Ann Gen Psychiatry, 2018.PMID 30258483
- [11]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [12]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [13]Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [14]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [15]Keller J, Flores B, Gomez RG, Solvason HB, Kenna H, Williams GH, et al. Cortisol circadian rhythm alterations in psychotic major depression Biol Psychiatry, 2006.PMID 16458262
- [16]Schatzberg AF Anna-Monika Award Lecture, DGPPN Kongress, 2013: the role of the hypothalamic-pituitary-adrenal (HPA) axis in the pathogenesis of psychotic major depression World J Biol Psychiatry, 2015.PMID 24933348
- [17]Nelson JC, Papakostas GI Atypical antipsychotic augmentation in major depressive disorder: a meta-analysis of placebo-controlled randomized trials Am J Psychiatry, 2009.PMID 19687129
- [18]Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942