Psych · General adult psychiatry — trauma and stressor-related disorders
PTSD and acute stress disorder
Also known as Post-traumatic stress disorder · Posttraumatic stress disorder · Acute stress disorder · ASD · Complex PTSD · cPTSD · Trauma-focused CBT · Prolonged exposure · EMDR
Exam-exhaustive fellowship reference on PTSD and acute stress disorder — DSM-5-TR and ICD-11 criteria including complex PTSD, epidemiology and military/civilian risk, fear-circuit and cognitive models, differentials (depression, BPD, psychosis), PCL-5/CAPS-5, TF-CBT/PE/CPT/EMDR evidence, SSRI/SNRI doses, prazosin debate, trauma-informed care, special populations. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Trauma- and stressor-related disorders are high-yield across FRANZCP MEQs, MRCPsych CASC communication stations, and ABPN blueprints. Examiners test duration thresholds, the difference between DSM-5-TR four-cluster PTSD and ICD-11 PTSD/complex PTSD, named psychological therapies with evidence, drug doses, and the prazosin controversy. This topic is written so a candidate who has read nothing else can defend those points at consultant depth.[2][20]
Overview and definition
Post-traumatic stress disorder (PTSD) is a syndrome that follows exposure to a qualifying traumatic event and is defined by characteristic re-experiencing, avoidance, negative alterations in cognitions and mood, and marked arousal/reactivity that persist long enough to impair function. Acute stress disorder (ASD) captures a severe acute post-trauma response in a shorter time window. Not everyone exposed to trauma develops either diagnosis — conditional risk varies by trauma type, prior vulnerability and post-trauma environment.[1][2]
DSM-5-TR Criterion A (trauma). Exposure to actual or threatened death, serious injury, or sexual violence in one or more of: direct experience; witnessing in person; learning that the event occurred to a close family member or close friend (violent or accidental for death); or repeated or extreme exposure to aversive details of traumatic events (e.g. first responders). Ordinary life stressors (job loss, relationship breakup without violence) do not meet Criterion A even when distressing.[2]
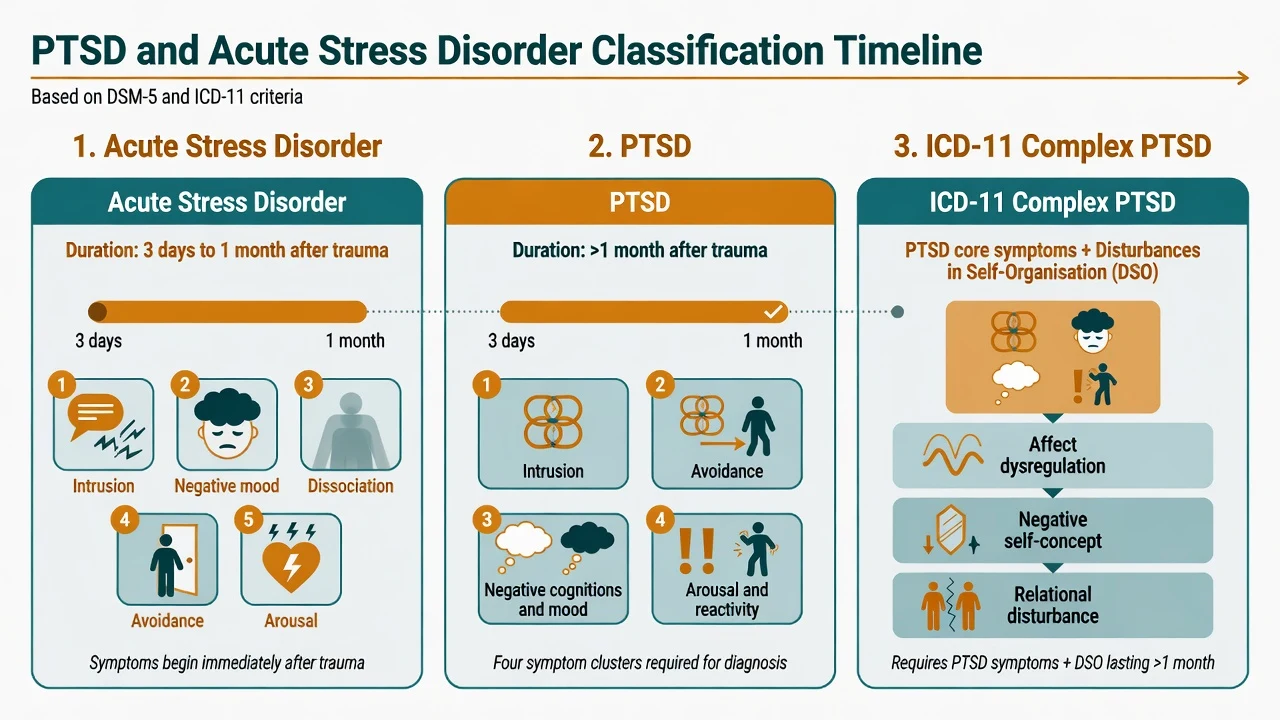
DSM-5-TR PTSD symptom architecture. Four clusters: intrusion (memories, nightmares, flashbacks, cued distress/physiological reactivity); avoidance of trauma-related memories/thoughts or external reminders; negative alterations in cognitions and mood (amnesia for important aspects, persistent negative beliefs, distorted blame, persistent negative emotional state, diminished interest, detachment, inability to experience positive emotions); marked alterations in arousal and reactivity (irritable/angry behaviour, reckless behaviour, hypervigilance, exaggerated startle, concentration problems, sleep disturbance). Duration of disturbance is more than 1 month, with clinically significant distress or impairment, not attributable to substance or another medical condition.[2]
Acute stress disorder. Same broad trauma exposure concept; symptom burden drawn from intrusion, negative mood, dissociation, avoidance and arousal domains; duration 3 days to 1 month after trauma exposure. ASD identifies people with high acute burden and elevated risk of later PTSD, but ASD is not required before a PTSD diagnosis, and many with later PTSD never met full ASD.[4]
ICD-11. PTSD is organised around three elements: re-experiencing in the present, deliberate avoidance, and a persistent sense of current threat (hypervigilance/startle). Complex PTSD requires PTSD plus disturbances of self-organisation (DSO): affect dysregulation, negative self-concept, and disturbances in relationships — often after prolonged or repeated trauma (e.g. childhood abuse, captivity). Name which manual you are using in the exam answer.[2][20]
Classification
ASD
- 3 days to 1 month after trauma
- High acute symptom burden across domains
- Dissociation often prominent
- Predicts higher PTSD risk but is not mandatory precursor
PTSD (DSM-5-TR)
- >1 month duration
- Four clusters required in structure
- Specifiers: with dissociative symptoms; delayed expression
- Functional impairment essential
ICD-11 PTSD
- Three core elements
- Simpler diagnostic focus
- Sense of current threat central
- Used widely internationally
ICD-11 complex PTSD
- PTSD + DSO triad
- Affect, self, relationships
- Prolonged/repeated trauma history common
- Phase-based treatment discussions
Specifiers examiners probe: with dissociative symptoms (depersonalisation or derealisation); with delayed expression (full criteria not met until at least 6 months after the event, though some symptoms may appear earlier). Course may be acute, chronic or fluctuating with anniversary and reminder cues.[2]
Epidemiology and risk factors
Headline numbers every candidate must own
The National Comorbidity Survey established PTSD as a common, often chronic disorder with substantial comorbidity and functional cost in the general population.[1] Nature Reviews disease primers synthesise global epidemiology, neurobiology and treatment architecture used in modern teaching.[2] Combat-deployed service members show substantial rates of PTSD, major depression and alcohol misuse, with well-documented barriers to care (stigma, career concerns, access).[5]
Risk factors. Pre-trauma: prior trauma, prior psychiatric illness, female sex (for some trauma types in community samples), younger age at trauma, lower social support. Peri-trauma: severity, perceived life threat, peri-traumatic dissociation, interpersonal violence. Post-trauma: ongoing threat, poor social support, secondary stressors, substance use as coping. Protective factors include social connectedness, timely support, and adaptive appraisals.[1][2]
Pathophysiology
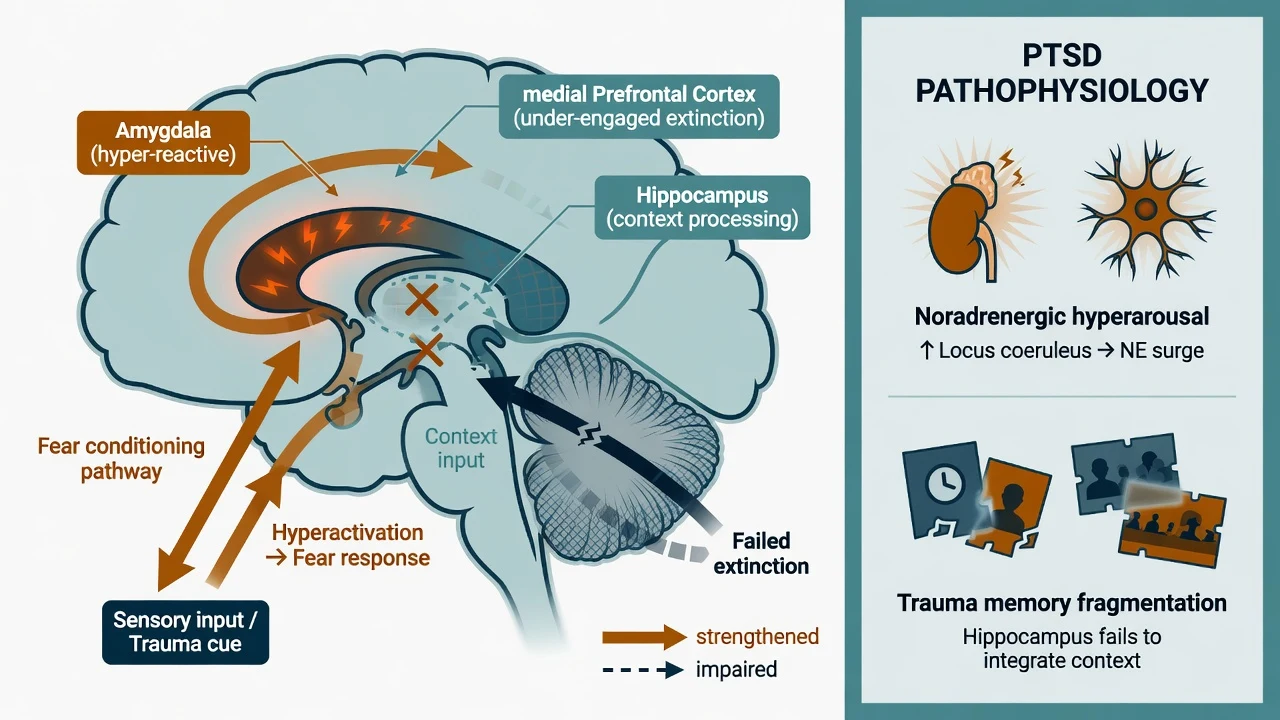
Fear conditioning and extinction. Trauma pairs cues with threat; subsequent reminders trigger conditioned fear. Successful recovery involves extinction learning and contextual discrimination. PTSD is framed as persistent fear responding with impaired extinction and overgeneralisation of threat.[2]
Circuit model (exam depth). Amygdala hyper-reactivity to threat cues; reduced top-down regulation from medial prefrontal regions; hippocampal contributions to contextual memory and discrimination. State these as group-level research models, not bedside diagnostics.[2]
Noradrenergic and HPA systems. Heightened noradrenergic tone contributes to hyperarousal, startle and nightmare physiology — the pharmacologic rationale for alpha-1 antagonism (prazosin) in nightmare-focused treatment, even though clinical trial results are mixed.[18][2]
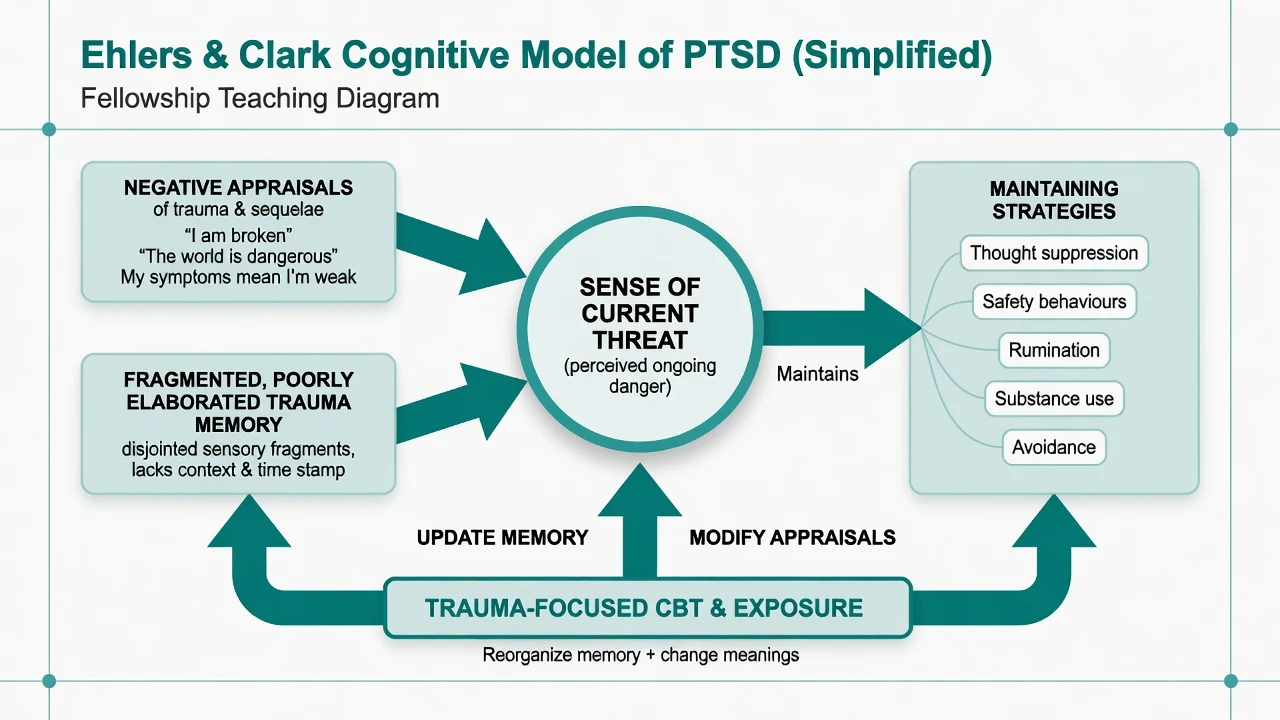
Ehlers and Clark cognitive model. Persistent PTSD occurs when the trauma and/or its sequelae are processed in a way that produces a sense of serious current threat. Two processes are critical: excessively negative appraisals of the trauma and/or its consequences; and a disturbance of autobiographical memory characterised by poor elaboration and strong perceptual priming, so that memories are easily triggered and experienced as happening now. Behavioural and cognitive strategies intended to control the threat (avoidance, thought suppression, rumination, substance use, safety behaviours) prevent cognitive change and maintain symptoms. This model directly underpins trauma-focused cognitive therapy.[3]
Clinical presentation
Core presentation: intrusive memories or nightmares; flashbacks with "here-and-now" quality; avoidance of conversations, places or media; emotional numbing or persistent shame/guilt/horror; hypervigilance and exaggerated startle; insomnia and irritability. Quote the patient ("I am still there"; "I cannot watch the news"; "I sleep with the light on").[2]
MSE focus. Affect may be restricted, tearful or irritable; thought content may include trauma-linked guilt or foreshortened future; perception may include pseudo-hallucinatory flashbacks that must be distinguished from primary psychosis; insight is often preserved regarding the trauma link; risk assessment is mandatory.[2]
Atypical and special presentations. Delayed expression; predominantly somatic complaints; cultural idioms of distress; military hypervigilance that overlaps with adaptive combat training; ASD in ED after MVA/assault with prominent dissociation. Children may show repetitive play, regression or behavioural dysregulation more than verbal flashbacks — see special populations pointer.[2][4]
Differential diagnosis
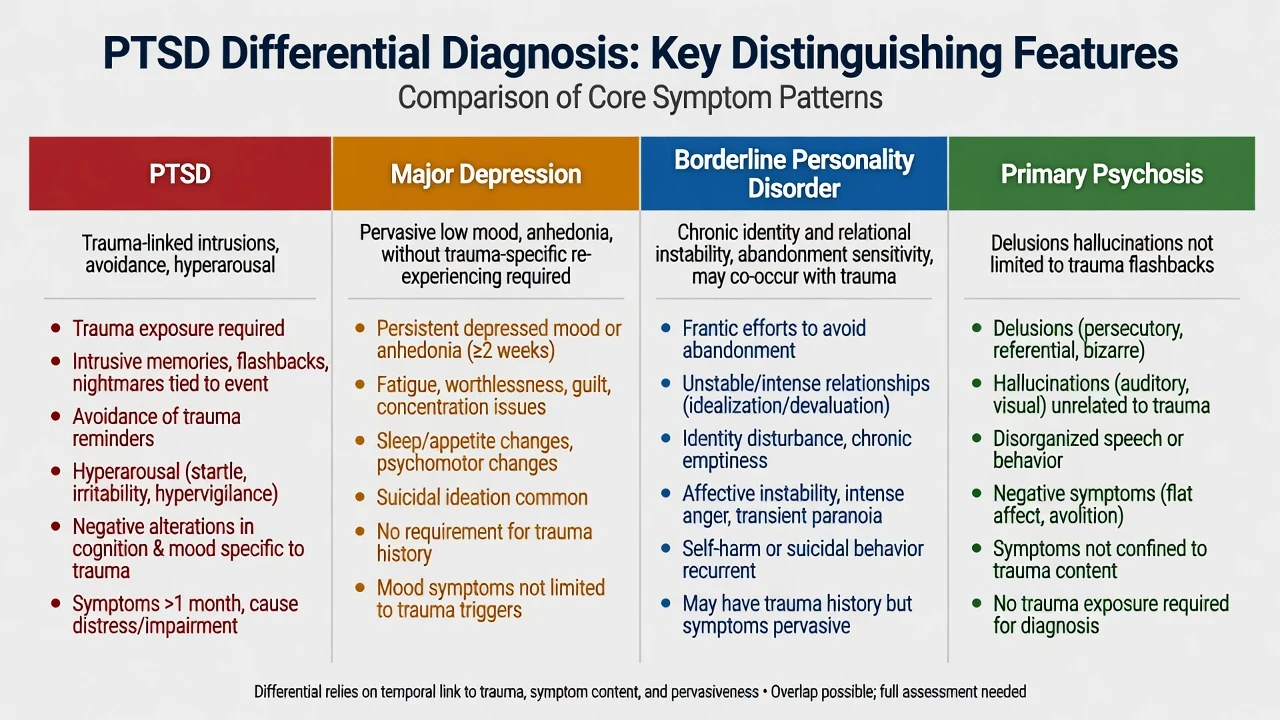
MDD
- Pervasive low mood/anhedonia may dominate
- Lacks trauma-linked intrusion/avoidance for PTSD diagnosis
- High comorbidity — treat both when both present
- Antidepressants help mood and some PTSD symptoms
BPD
- Chronic identity and relational instability
- Abandonment fears, self-harm patterns
- Trauma history common; complex PTSD overlap debated
- Need both diagnostic formulations when criteria met
Primary psychosis
- Delusions/hallucinations not limited to trauma re-experiencing
- Thought disorder, negative symptoms
- Flashbacks can be mislabelled as hallucinations
- PTSD can co-occur with psychotic disorders
Other
- Adjustment disorder (subthreshold)
- Prolonged grief disorder
- OCD (intrusions ego-dystonic, not trauma replay)
- TBI, substance, panic, OSA mimics of hyperarousal
Also exclude substance/medication-induced anxiety presentations and medical mimics when the history is atypical (late first onset without clear trauma, focal neurology, delirium).[2]
Clinical and bedside assessment
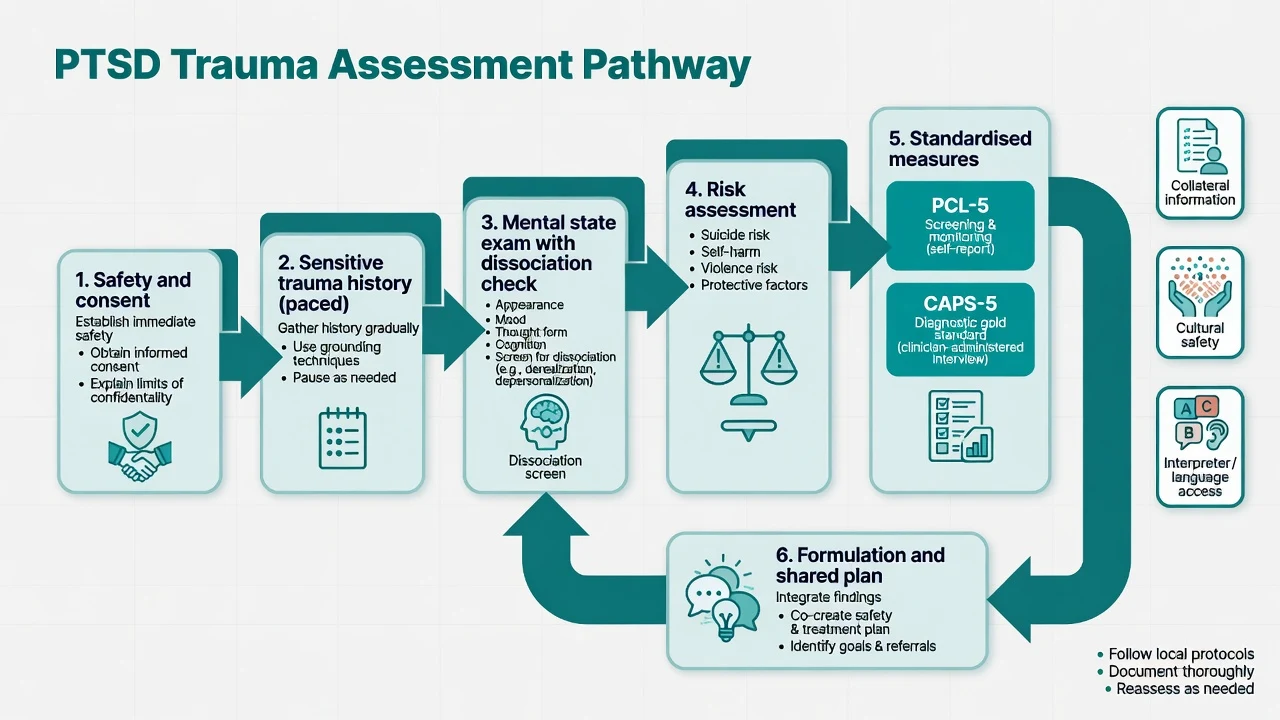
Trauma-informed interview. Prioritise safety, choice, collaboration and trustworthiness. Obtain enough detail to establish Criterion A and symptom linkage without forcing a graphic recounting in the first minutes. Offer control over pacing, breaks and gender-of-clinician preferences where feasible. Use interpreters for language needs; apply cultural formulation.[20]
History structure. Trauma chronology (what, when, ongoing threat); symptom clusters with onset/course; prior trauma; depression, anxiety, substance use; medical/TBI; forensic/military service; supports; prior treatments (therapy type and adequacy, medications, response).[2]
Risk. Suicide, self-harm, violence, vulnerability to revictimisation, child protection issues, intimate partner violence. Collaborative safety plan and means restriction. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive; do not invent section numbers for the wrong jurisdiction.[2]
PCL-5. 20-item self-report checklist corresponding to DSM-5 PTSD symptoms; used for screening, tracking severity and treatment monitoring. It does not replace clinical diagnosis or a full risk assessment.[6]
CAPS-5. Clinician-administered structured interview regarded as a gold-standard diagnostic and severity instrument for DSM-5 PTSD in research and specialist practice; training improves reliability.[7]
Investigations
There is no diagnostic blood test or MRI for PTSD. Order investigations to exclude mimics and to prepare safely for medication: TSH, FBC, U&E, LFT as indicated; ECG when cardiac risk or before agents with QTc concern; pregnancy test when relevant; urine drug screen when substance contribution is plausible; sleep study if OSA suspected; neuroimaging only with neurological red flags. Serial PCL-5 supports measurement-based care during therapy or pharmacotherapy.[6][2]
Management — acute / resuscitation
Immediate post-trauma care. Attend to medical injuries, physical safety, orientation and practical needs. Provide calm information, contact restoration and linkage to supports (psychological first aid principles). Routine single-session mandatory psychological debriefing for all survivors is not recommended as a universal prevention strategy; target those with significant symptoms and offer evidence-based early interventions when indicated.[20][4]
Acute psychiatric risks. Manage suicidality, severe agitation, panic, insomnia and substance withdrawal with appropriate medical pathways. Short-term symptomatic medication may be needed for severe insomnia or agitation, but avoid reflexive long-term benzodiazepines for PTSD core syndrome.[2]
Management — definitive and stepwise
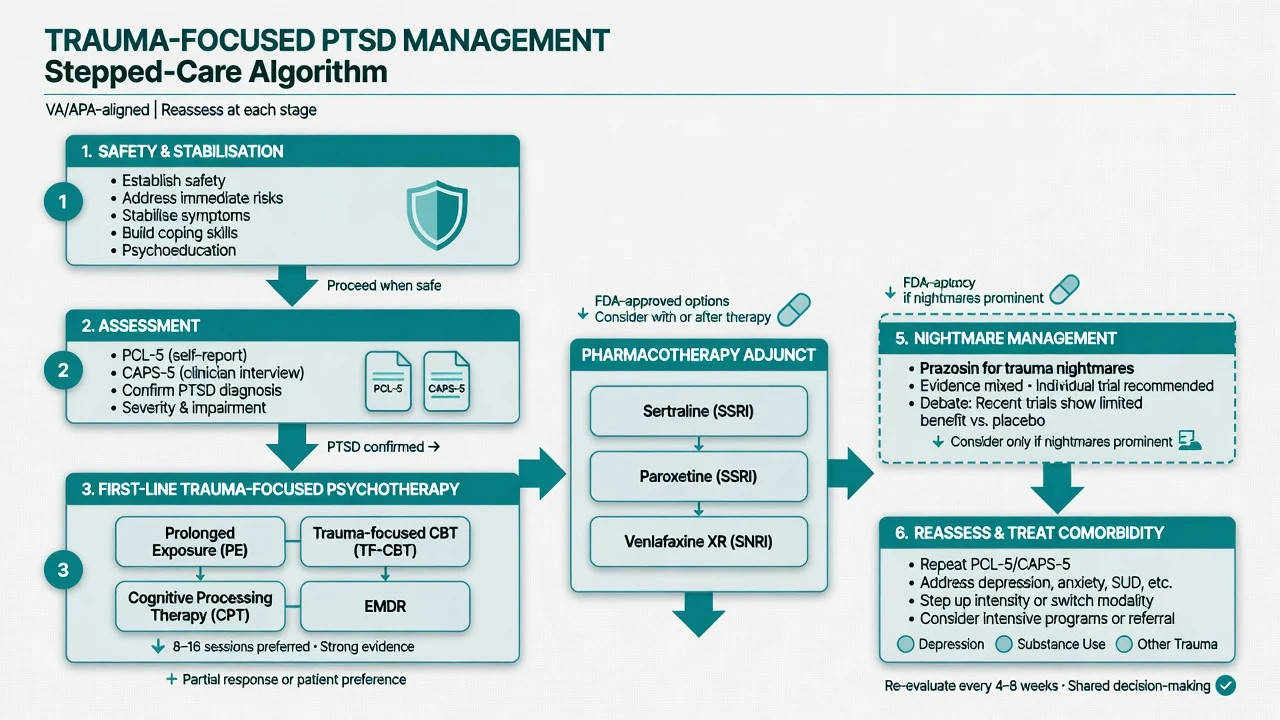
Stepped care and trauma-informed principles
Match intensity to severity, risk, preference and access. All services should embody trauma-informed care: safety, trustworthiness, choice, collaboration, empowerment and cultural humility. Psychoeducation normalises common reactions and explains treatment options without pathologising resilience.[20]
Australian and New Zealand practice draws on national ASD/PTSD guidance traditions and trauma service models; trauma-focused CBT modalities and EMDR are prioritised where skilled therapists are available, with SSRIs/SNRIs as pharmacologic options and stepped referral to specialist trauma or veteran services.[20]
Trauma-focused psychological therapies (first-line)
Meta-analyses and Cochrane reviews show that trauma-focused psychological therapies reduce PTSD symptoms versus waitlist/usual care, with the strongest and most consistent signals for trauma-focused CBT protocols and EMDR among widely studied approaches.[16][17]
| Therapy | Core mechanism (exam level) | Practical outline |
|---|---|---|
| Prolonged exposure (PE) | Extinction via imaginal and in vivo exposure; processing of trauma memory | Psychoeducation, breathing retraining optional, imaginal exposure to trauma memory, hierarchical in vivo exposure to avoided safe situations; typically ~8–15 sessions |
| Trauma-focused CBT / CT | Update appraisals and trauma memory (Ehlers–Clark) | Cognitive restructuring of threat appraisals, reclaiming life, behavioural experiments, work with triggers and meanings |
| Cognitive processing therapy (CPT) | Challenge stuck points (safety, trust, power, esteem, intimacy) | Written trauma account variants and/or cognitive-only protocols; structured worksheets |
| EMDR | Dual-attention bilateral stimulation while processing trauma memory | Standardised eight-phase protocol; less verbal exposure demand for some patients |
| Trauma-focused modalities summarised for exam use.[11][13][16][17] |
PE has robust RCT and meta-analytic support, including trials with and without added cognitive restructuring and large effectiveness programmes in women veterans and civilian samples.[11][12][15] CPT has foundational and dismantling trial support in interpersonal violence survivors and efficacy in military-related PTSD.[13][14] Choice among bona fide trauma-focused therapies is guided by availability, patient preference, comorbidity and therapist competence more than a single universal winner.[17][20]
Stabilisation vs exposure timing. Most patients with PTSD can start trauma-focused work after basic safety and engagement. Highly unstable substance dependence, acute mania/psychosis, or imminent high risk may need stabilisation first. Avoid indefinite "stabilisation only" that never reaches effective trauma processing when the patient is otherwise ready.[19][20]
Pharmacotherapy — agent, dose, monitoring
When medication is chosen (preference, severe comorbidity, limited therapy access, partial response), first-line evidence supports certain SSRIs and venlafaxine XR.[8][9][10]
| Agent | Typical adult start | Common range | Notes |
|---|---|---|---|
| Sertraline | 25–50 mg orally daily | 50–200 mg daily | RCT evidence in PTSD; sexual dysfunction, GI effects; favourable cardiac/perinatal discussions often |
| Paroxetine | 20 mg orally daily | 20–50 mg daily | RCT evidence; more anticholinergic/discontinuation risk; pregnancy caution |
| Venlafaxine XR | 75 mg orally daily | 75–225 mg daily | 6-month RCT support; monitor BP; discontinuation symptoms |
| Typical adult oral ranges for exam answers; individualise and check local product information.[8][9][10] |
Sertraline demonstrated efficacy and safety versus placebo in chronic PTSD.[8] Paroxetine fixed-dose trials support benefit in chronic PTSD.[9] Venlafaxine XR showed benefit over 6 months in a large RCT.[10] Watts and colleagues' broader treatment meta-analysis supports both psychological and pharmacologic effect sizes versus control, with psychotherapy generally larger in aggregate analyses — interpret with study-design caveats.[17]
Adequate pharmacologic trial. Therapeutic dose for about 6–12 weeks for core PTSD response assessment (longer than a token 10-day trial), with adherence check, side-effect management and parallel psychotherapy whenever possible. Continue for many months after response; stop plans should be gradual.[8][10]
What not to default to. Long-term benzodiazepines are not first-line for PTSD core symptoms and may impair trauma-processing therapies and create dependence. Atypical antipsychotics are not routine first-line for uncomplicated PTSD (reserve for true comorbidity or specialist augmentation contexts). Cannabis is not an evidence-based PTSD disease-modifying treatment despite patient interest.[2][20]
Prazosin and nightmares — the debate
Prazosin (alpha-1 antagonist) is used off-label for trauma-related nightmares based on noradrenergic hyperarousal rationale and earlier positive trials. A large multi-site randomised trial in military veterans did not show benefit over placebo for overall PTSD outcomes, creating genuine equipoise.[18] Exam stance: discuss evidence mixed; consider a carefully monitored individual trial when nightmares dominate, blood pressure allows, and patient is informed; do not present prazosin as mandatory or universally effective.
Example dosing language (adult, exam-level, individualise). Night-time prazosin often started low (e.g. 1 mg orally at night) with slow titration while monitoring BP, dizziness and falls risk — exact schedules vary by protocol and population; always check local product information and comorbidities.[18]
Complex trauma and phase-based care
For PTSD related to childhood abuse and for ICD-11 complex PTSD presentations, phase-based approaches that build emotion regulation and interpersonal skills before or alongside exposure have RCT support (STAIR followed by exposure).[19] This is not a licence to delay effective trauma work indefinitely in stable patients.
Specific subtypes and scenarios
ASD. Support, watchful monitoring, treat acute insomnia/risk, and offer early trauma-focused CBT for those with severe symptoms or high risk of chronicity rather than universal debriefing.[4][20]
Military and veterans. High exposure load, moral injury as a formulation concept (not a DSM diagnosis), peer stigma, and need for veteran-competent services. PE and CPT have military evidence bases.[5][12][14]
Sexual assault and IPV. Prioritise safety, forensic options without coercing reporting, gender-sensitive care, and evidence-based TF therapies; CPT has deep roots in sexual assault populations.[13]
PTSD with psychotic disorder. Carefully delivered PE or EMDR can reduce PTSD symptoms even in patients with psychotic disorders in specialised trials — coordinate with psychosis care.[17]
Complications and pitfalls
- Forcing graphic exposure in the first interview or in acute crisis.
- Missing ongoing domestic violence.
- Diagnosing "PTSD" after non-Criterion-A stressors without assessing adjustment disorder.
- Labelling flashbacks as schizophrenia without trauma formulation — and the reverse error of missing true psychosis.
- Token SSRI doses or declaring therapy "failed" after two irregular sessions.
- Benzodiazepine dependence for chronic insomnia/hyperarousal.
- Clinician secondary trauma and boundary failures — supervision matters.[2][20]
Prognosis and disposition
Many people recover after trauma without developing chronic PTSD. Among those who meet PTSD criteria, untreated course is often prolonged, but evidence-based treatment produces clinically meaningful gains for a substantial proportion.[1][16] Disposition ladder: GP and community psychology; specialist trauma services; veteran services; crisis teams; voluntary or involuntary inpatient care when risk or severe comorbidity demands. Functional outcomes (relationships, work, parenting) matter as much as PCL-5 points.[20]
Special populations
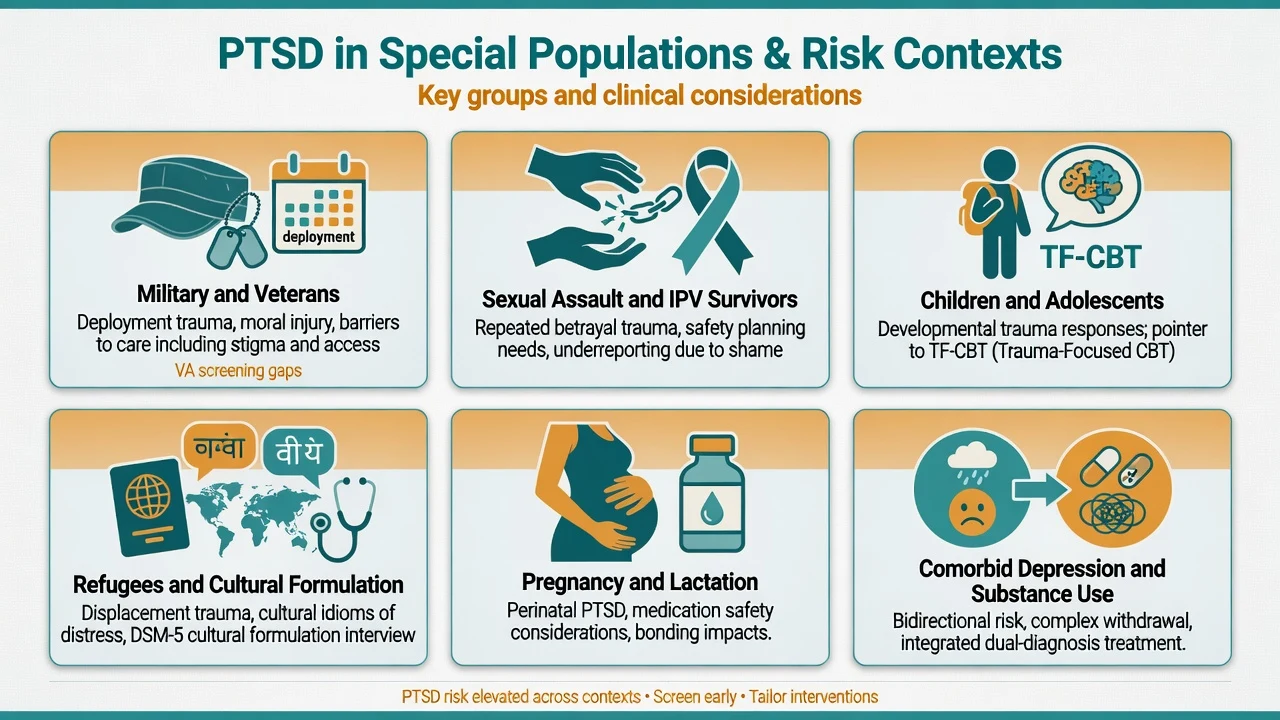
Children and adolescents. Symptom expression differs (play re-enactment, behaviour change); trauma-focused CBT adapted for youth is first-line in paediatric pathways — full CAP depth is a related specialty topic. Involve caregivers safely.[20]
Pregnancy and lactation. Prioritise psychotherapy when accessible; if an SSRI is needed, individualise risk–benefit (sertraline often discussed favourably). Untreated severe PTSD with risk is not "safer" by default.[8]
Older adults. Late-life PTSD (including delayed recognition of early-life trauma), medical comorbidity, falls and SSRI hyponatraemia risk require careful agent choice and monitoring.[2][8]
Refugees, Indigenous peoples and cultural minorities. Torture/trauma histories, interpreter needs, cultural safety, community supports; avoid pathologising cultural expressions of grief and spirit while still offering effective care.[20]
Evidence, guidelines and controversies
Landmark threads: epidemiology (Kessler NCS); disease primer (Yehuda et al.); cognitive model (Ehlers and Clark); ASD prediction (Bryant); military burden (Hoge); PCL-5 and CAPS-5 measurement; sertraline/paroxetine/venlafaxine pharmacotherapy RCTs; PE (Foa, Schnurr, Powers meta-analysis); CPT (Resick, Monson); psychotherapy systematic reviews (Bisson, Cusack); ISTSS guideline methodology; prazosin NEJM null multi-site trial; STAIR phase-based care (Cloitre).[1][2][3][11][16][18][20]
Controversies to defend both sides. Prazosin equipoise; whether complex PTSD needs separate pathways versus standard TF therapy with skills modules; how early to intervene after trauma; cannabis claims; mandatory debriefing (not supported as universal).[18][20]
Exam pearls
TRAUMA
- Duration trap: ASD 3 days–1 month; PTSD greater than 1 month.[4]
- Four vs three: DSM-5-TR four clusters; ICD-11 three elements (+ DSO for complex PTSD).[2]
- First-line: trauma-focused psychotherapy when available.[16][17]
- Drugs with doses: sertraline 50–200 mg; paroxetine 20–50 mg; venlafaxine XR 75–225 mg (adult typical ranges).[8][9][10]
- Scales: PCL-5 monitors; CAPS-5 structured diagnostic interview.[6][7]
- Prazosin: mixed evidence after large veteran RCT — individualise.[18]
Self-test: 30-second viva opener
"PTSD requires a qualifying trauma, four DSM-5-TR symptom clusters for more than a month with impairment; ASD is the 3-day to 1-month severe acute form. First-line is trauma-focused psychotherapy — prolonged exposure, CPT, TF-CBT or EMDR — with sertraline, paroxetine or venlafaxine as evidence-based drug options. I assess suicide risk, ongoing safety, substances and comorbidity, use PCL-5 to track, and treat prazosin for nightmares as an individualised decision after mixed trial evidence."[2][16][18]
References
- [1]Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB Posttraumatic stress disorder in the National Comorbidity Survey Arch Gen Psychiatry, 1995.PMID 7492257
- [2]Yehuda R, Hoge CW, McFarlane AC, Vermetten E, et al. Post-traumatic stress disorder Nat Rev Dis Primers, 2015.PMID 27189040
- [3]Ehlers A, Clark DM A cognitive model of posttraumatic stress disorder Behav Res Ther, 2000.PMID 10761279
- [4]Bryant RA Acute stress disorder as a predictor of posttraumatic stress disorder: a systematic review J Clin Psychiatry, 2011.PMID 21208593
- [5]Hoge CW, Castro CA, Messer SC, McGurk D, et al. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care N Engl J Med, 2004.PMID 15229303
- [6]Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation J Trauma Stress, 2015.PMID 26606250
- [7]Weathers FW, Bovin MJ, Lee DJ, Sloan DM, Schnurr PP, et al. The Clinician-Administered PTSD Scale for DSM-5 (CAPS-5): Development and initial psychometric evaluation in military veterans Psychol Assess, 2018.PMID 28493729
- [8]Brady K, Pearlstein T, Asnis GM, Baker D, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial JAMA, 2000.PMID 10770145
- [9]Marshall RD, Beebe KL, Oldham M, Zaninelli R Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study Am J Psychiatry, 2001.PMID 11729013
- [10]Davidson J, Baldwin D, Stein DJ, Kuper E, et al. Treatment of posttraumatic stress disorder with venlafaxine extended release: a 6-month randomized controlled trial Arch Gen Psychiatry, 2006.PMID 17015818
- [11]Foa EB, Hembree EA, Cahill SP, Rauch SA, et al. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: outcome at academic and community clinics J Consult Clin Psychol, 2005.PMID 16287395
- [12]Schnurr PP, Friedman MJ, Engel CC, Foa EB, Shea MT, et al. Cognitive behavioral therapy for posttraumatic stress disorder in women: a randomized controlled trial JAMA, 2007.PMID 17327524
- [13]Resick PA, Galovski TE, Uhlmansiek MO, Scher CD, et al. A randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence J Consult Clin Psychol, 2008.PMID 18377121
- [14]Monson CM, Schnurr PP, Resick PA, Friedman MJ, et al. Cognitive processing therapy for veterans with military-related posttraumatic stress disorder J Consult Clin Psychol, 2006.PMID 17032094
- [15]Powers MB, Halpern JM, Ferenschak MP, Gillihan SJ, Foa EB A meta-analytic review of prolonged exposure for posttraumatic stress disorder Clin Psychol Rev, 2010.PMID 20546985
- [16]Bisson JI, Roberts NP, Andrew M, Cooper R, Lewis C Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults Cochrane Database Syst Rev, 2013.PMID 24338345
- [17]Cusack K, Jonas DE, Forneris CA, Wines C, et al. Psychological treatments for adults with posttraumatic stress disorder: A systematic review and meta-analysis Clin Psychol Rev, 2016.PMID 26574151
- [18]Raskind MA, Peskind ER, Chow B, Harris C, et al. Trial of Prazosin for Post-Traumatic Stress Disorder in Military Veterans N Engl J Med, 2018.PMID 29414272
- [19]Cloitre M, Koenen KC, Cohen LR, Han H Skills training in affective and interpersonal regulation followed by exposure: a phase-based treatment for PTSD related to childhood abuse J Consult Clin Psychol, 2002.PMID 12362957
- [20]Bisson JI, Berliner L, Cloitre M, Forbes D, et al. The International Society for Traumatic Stress Studies New Guidelines for the Prevention and Treatment of Posttraumatic Stress Disorder: Methodology and Development Process J Trauma Stress, 2019.PMID 31283056