Psych · General adult psychiatry — reactive attachment and disinhibited social engagement
Reactive attachment and disinhibited social engagement disorders
Also known as Reactive attachment disorder · RAD · Disinhibited social engagement disorder · DSED · Indiscriminate friendliness · Disinhibited attachment disorder · Emotionally withdrawn attachment disorder · Institutional care attachment sequelae
Exam-exhaustive general-adult fellowship reference on RAD and DSED — DSM-5-TR and ICD-11 criteria, disorder versus style, BEIP and ERA evidence including child-to-adult residual trajectories, caregiving-first management, rejection of coercive attachment therapies, and adult psychiatry traps when residual early-deprivation burden is mislabelled as personality or forensic 'adult RAD'. Distinct from the CAP clinical leaf. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
This general-adult leaf is written for fellowship candidates who meet attachment disorders in adult, transition-age, adoption-consult, family, and forensic interfaces. The companion CAP leaf deepens nursery observation and looked-after-child pathways; here the examiner targets are nosology precision, RAD versus DSED versus style, caregiving-first care, APSAC red lines, and residual adult trajectories after institutional deprivation (ERA young-adult follow-up).[1][5][11]
Overview and definition
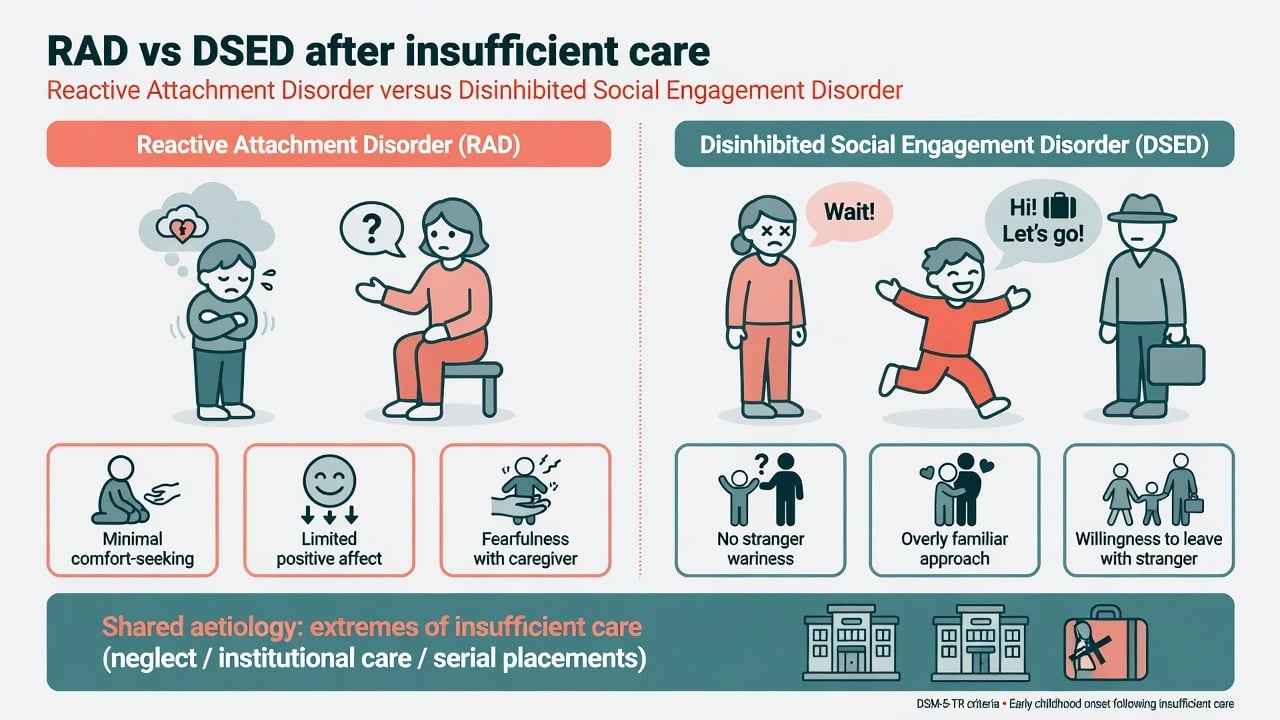
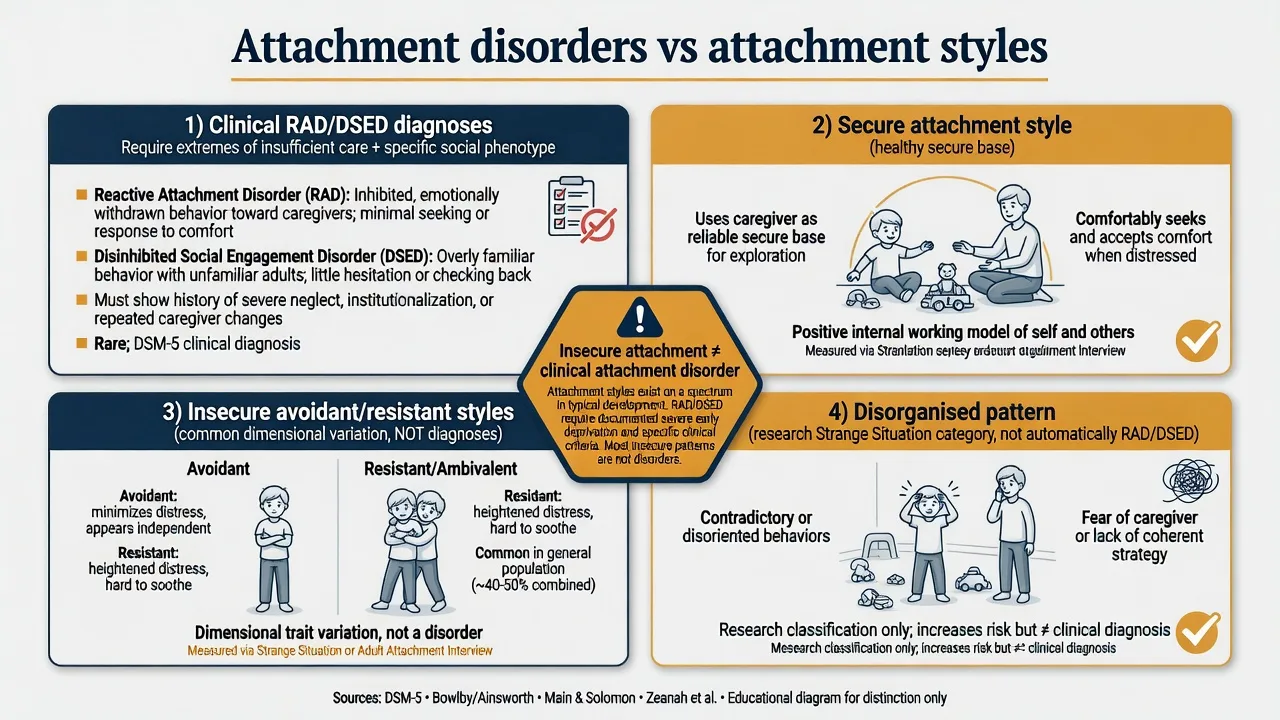
Clinical attachment disorders describe a failure to develop or use preferential, selective attachment relationships after severe social neglect or deprivation, not ordinary parenting strain or garden-variety insecurity. Modern nosology separates two phenotypes: an inhibited, emotionally withdrawn pattern (RAD) and a disinhibited social engagement pattern (DSED).[1][3]
Why general adult cares. Categorical RAD/DSED are childhood constructs with developmental thresholds, yet adult services inherit: (1) transition-age youth with residual social-boundary risk; (2) adults with documented early institutional deprivation and elevated later neurodevelopmental and mental-health burden; (3) parents and carers seeking second opinions; and (4) dangerous community misuse of "RAD" language in adult personality or forensic narratives.[11][1][2]
Formulation first. Criteria open the gate; formulation explains the caregiving ecology (institutional care, serial placements, extreme neglect), current carer capacity, developmental comorbidities, and — in adults — residual function without retrofitting a childhood diagnosis that criteria do not support.[1][8][11]
Classification: RAD versus DSED
DSM-5-TR — RAD (exam skeleton)
A consistent pattern of inhibited, emotionally withdrawn behaviour toward adult caregivers, manifested by both minimal comfort-seeking when distressed and minimal response to comfort when distressed. Persistent social and emotional disturbance includes at least two of: minimal social and emotional responsiveness to others; limited positive affect; episodes of unexplained irritability, sadness or fearfulness that are evident even during nonthreatening interactions with adult caregivers. The child has experienced a pattern of extremes of insufficient care (social neglect/deprivation; repeated changes of primary caregivers; or rearing in unusual settings that severely limit opportunities to form selective attachments) presumed responsible for the disturbance. Criteria are not met for autism spectrum disorder. Disturbance is evident before age 5 years, and the child has a developmental age of at least 9 months.[1][3]
DSM-5-TR — DSED (exam skeleton)
A pattern of behaviour in which a child actively approaches and interacts with unfamiliar adults, with at least two of: reduced or absent reticence in approaching/interacting with unfamiliar adults; overly familiar verbal or physical behaviour (not culturally sanctioned and inappropriate); diminished or absent checking back with adult caregiver after venturing away, even in unfamiliar settings; willingness to go off with an unfamiliar adult with minimal or no hesitation. Behaviours are not limited to impulsivity (as in ADHD) but include socially disinhibited behaviour. The child has experienced extremes of insufficient care as above, presumed responsible. Developmental age at least 9 months.[1][3][9]
ICD-11. Reactive attachment disorder and disinhibited social engagement disorder remain related categories with the same clinical logic: rare disorders after severe early adversity of caregiving, not synonyms for insecure style. State which manual you apply when thresholds are examined.[1]
Historical trap. Older DSM-IV language framed inhibited and disinhibited types under a single RAD heading. DSM-5/DSM-5-TR treat them as separate disorders that share aetiology but differ in presentation and course — a classic exam fail if a stem uses outdated single-disorder wording.[1][3]
RAD
- Emotionally withdrawn/inhibited
- Does not seek or accept comfort
- Limited positive affect with caregivers
- Often improves with good care
DSED
- Overly familiar with strangers
- Little checking back / wariness
- May leave with unfamiliar adults
- Often more persistent after care improves
Insecure style
- Avoidant/resistant patterns
- Common dimensional variation
- Not a clinical disorder alone
- No insufficient-care requirement
Adult residual burden
- Not a formal 'adult RAD' category
- Elevated ND/MH risk after early deprivation
- Heterogeneous adult outcomes (ERA)
- Formulate history + current syndrome
Epidemiology and risk
Numbers and patterns candidates should own
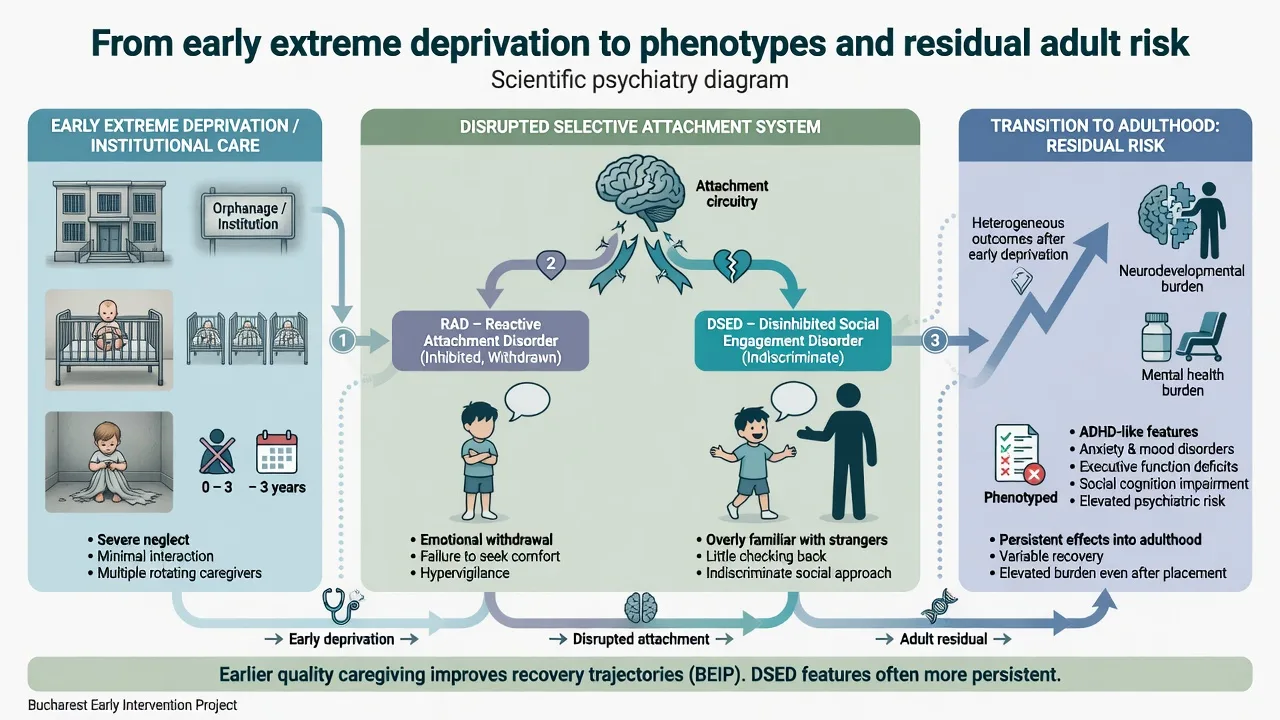
RAD and DSED are uncommon in general population samples and become clinically important after institutional rearing, chronic severe neglect, or highly unstable caregiving. The English and Romanian Adoptees (ERA) programme showed that profound early institutional privation produces heterogeneous outcomes — including attachment disorder behaviours — rather than a single uniform syndrome.[5][6]
The Bucharest Early Intervention Project (BEIP) randomised institutionalised young children to high-quality foster care versus care as usual and demonstrated causal benefits of earlier psychosocial enrichment for cognition and attachment-related recovery — foundational exam evidence that environment is the treatment target.[4][10][14]
Adult psychiatry pearl. Sonuga-Barke and colleagues' young-adult follow-up of the longitudinal ERA study maps child-to-adult neurodevelopmental and mental-health trajectories after early life deprivation — examiners expect you to know that residual burden can persist into adult life for some, without equating that residual burden to a freestanding adult RAD diagnosis.[11]
Middle-childhood UK adopted samples support validity of disinhibited attachment concepts beyond preschool years, with developmental origins linked to early adversity rather than current adoptive parenting failure alone.[13]
Pathophysiology and developmental mechanisms
Attachment is a species-typical biobehavioural system organising proximity-seeking under threat and use of a caregiver as a secure base. Under extremes of insufficient care, children may fail to organise selective attachment (RAD) or may show indiscriminate social approach without appropriate reticence (DSED/indiscriminate friendliness).[1][7][8]
Institutional care research shows indiscriminate behaviour is strongly associated with severe early deprivation and can be observed even when some attachment forms with a new carer — one reason DSED is separated from RAD conceptually.[7][9] Following early institutional deprivation, child–parent attachment quality is measurable but often atypical; recovery is possible yet incomplete for some social phenotypes.[8]
Mediation. Improvements in caregiving and attachment security help explain reductions in psychopathology after placement into better care — supporting interventions that target the caregiving relationship, not only child symptom suppression.[10][4]
Sensitive periods. Earlier placement into high-quality foster care is associated with better recovery trajectories across cognitive and socioemotional domains in multilevel BEIP analyses — examiners expect "timing of intervention matters" without claiming infinite plasticity or hopelessness after late placement.[4][14]
Clinical presentation
RAD (childhood). Minimal seeking of comfort when hurt, frightened or ill; little response when comfort is offered; restricted positive affect with caregivers; unexplained irritability, sadness or fearfulness even in non-threatening caregiver interactions.[1][3]
DSED (childhood). Reduced stranger wariness; overly familiar talk or touch; little checking back in unfamiliar settings; willingness to leave with an unfamiliar adult. This is not healthy sociability.[1][9][13]
Transition-age / residual. Residual DSED-type boundary problems can persist after placement improvement and may present to adult services as indiscriminate trust, exploitation vulnerability, or peer difficulties. Formulate residual features, current risk, and comorbidity — do not force childhood criteria language if developmental history is incomplete.[5][9][11][13]
Adult residual after early institutional deprivation. ERA young-adult data support lasting elevation in neurodevelopmental and mental-health problems for some exposed early in life; outcomes are heterogeneous. Adult MSE should map current syndromes (depression, anxiety, ADHD-like features, ASD differential, substance use, personality pattern) against verified early-care history rather than a single "attachment disorder" label.[6][11]
Differential diagnosis
ASD
- Pervasive social-communication differences
- RRBs and sensory features
- Present without requiring insufficient care
- May co-occur — assess both carefully
ADHD
- Multi-domain impulsivity/inattention
- Social disinhibition is not specifically stranger-boundary failure
- Often comorbid after deprivation
- Treat ADHD on its own merits
Complex PTSD / BPD (adult)
- Trauma clusters / cross-context personality pattern
- May share early adversity history
- Do not collapse into 'adult RAD'
- Use adult criteria for adult syndromes
ID / language delay
- Limited social skills from cognition/language
- Does not equal RAD without care history
- Need developmental assessment
- Adaptive support still required
Also keep depression, social anxiety, rare genetic social phenotypes, and cultural norms for stranger interaction on the board. The decisive triad for attachment disorder is insufficient-care history + specific social phenotype + multi-source observation, not behavioural difficulty in a looked-after child alone — and not adult offending with a childhood adversity history alone.[1][3][6][11]
Assessment (GA and transition interfaces)
Structure as early-care history + multi-informant phenotype + criteria map (if youth) + residual formulation (if adult) + comorbidity + risk + safeguarding.[1]
- Document extremes of insufficient care: institutional periods, neglect, number/duration of placements, age at first quality placement.
- For children/adolescents: map RAD and DSED criteria with concrete examples across home, clinic and educational settings; confirm developmental age threshold (at least 9 months) and RAD onset before age 5 when applying DSM-5-TR.
- For adults: reconstruct developmental history carefully; map residual social-boundary or socioemotional difficulties; diagnose current adult syndromes on their own criteria.
- Screen ASD, ADHD, cognition/language, PTSD/complex trauma features, mood, substance use, exploitation risk.
- Risk: absconding with strangers (youth DSED); adult sexual/financial exploitation; parental capacity if the patient is a carer; self-harm.
- Capacity, consent and mandatory reporting — jurisdiction-specific principles only.[1][2][11]
Investigations
There is no diagnostic blood test, gene panel or scan for RAD/DSED.[1]
Investigate for sequelae of neglect and for differential diagnoses as indicated: developmental assessment, hearing/vision, growth and nutrition (youth), ASD evaluation when social-communication differentials are active, cognitive testing when delay is suspected. Baseline metabolic panel and ECG only if you plan pharmacotherapy for a named comorbidity — not to "prove attachment."[1][4]
Acute safety and safeguarding
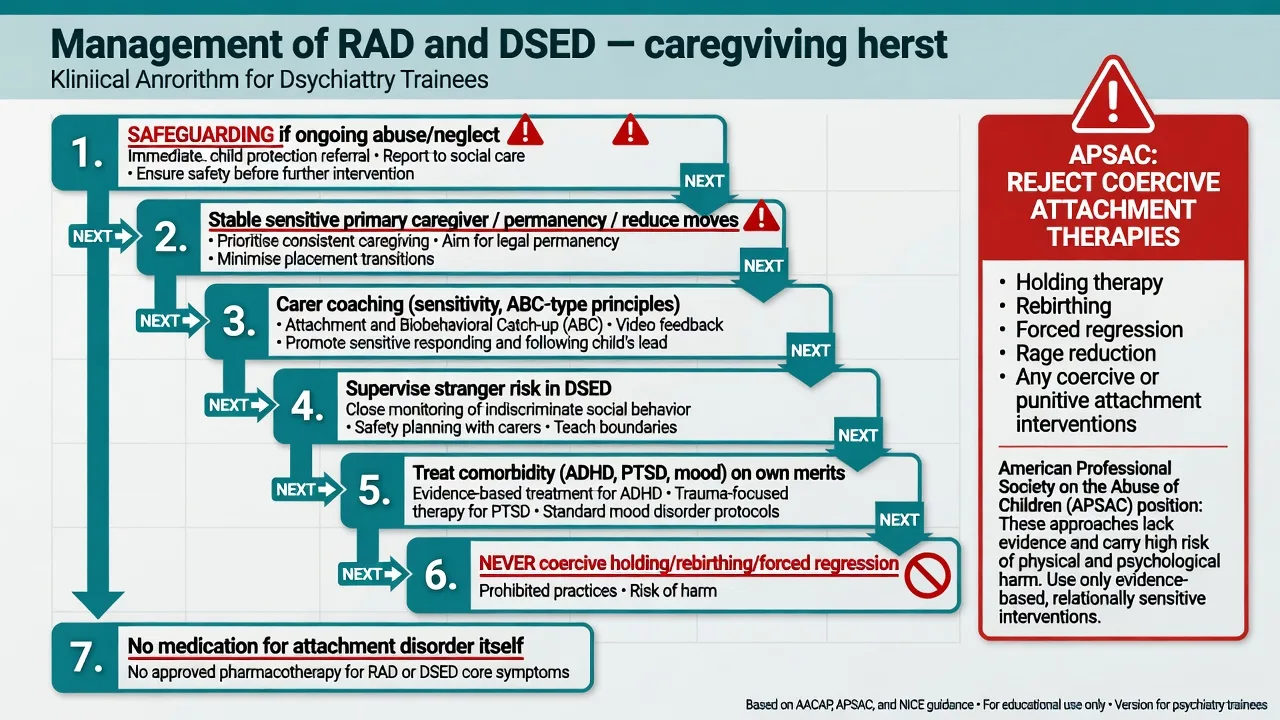
For DSED, implement practical supervision to prevent leaving with strangers. For adult residual risk, use standard adult safety planning for exploitation, self-harm, and parental capacity concerns. For RAD, prioritise consistent caregiver presence during distress rather than forced physical closeness.[1][2]
Definitive management
Caregiving environment is first-line (children and youth)
The AACAP practice parameter for RAD and DSED centres treatment on ensuring the child has an emotionally available, stable, sensitive primary caregiver (or a small number of consistent caregivers), with permanency planning that minimises further placement disruption.[1]
Psychoeducation for carers: RAD signs often improve substantially once reliable comfort is available; DSED/indiscriminate behaviour may persist longer and needs explicit boundary coaching and supervision rather than parental self-blame.[1][5][9][13]
Caregiver-focused interventions
Evidence-informed programmes that coach caregiver sensitivity, nurturing and follow-through — including Attachment and Biobehavioral Catch-up (ABC) — have randomised evidence for reducing behaviour problems among internationally adopted children and are exam-nameable models of attachment-informed parent coaching.[12][1]
Comorbidity treatment (child and adult)
Treat ADHD, anxiety, PTSD, depression, sleep disturbance, language delay and medical sequelae on their own evidence bases. Pharmacotherapy is not a treatment for attachment disorder itself; avoid antipsychotics or other agents "for attachment." If medication is used, it is for a named comorbid indication with monitoring appropriate to that agent (for example, a standard adult SSRI regimen for comorbid major depression is about the depression, not about "curing attachment").[1][2][11]
Adult residual and transition care
For transition-age youth and adults with verified early severe deprivation histories: (1) treat current syndromes (mood, anxiety, ADHD, trauma-related) with standard evidence; (2) address social-boundary and exploitation risk with practical coaching and supports; (3) use trauma-informed psychological approaches when indicated; (4) support carers/families; (5) never offer coercive attachment programmes to adults or families; (6) avoid inventing "adult RAD" as a primary diagnosis when childhood criteria and developmental timing cannot be established.[2][11][1]
Explicitly reject coercive attachment therapies
The APSAC task force report is a viva classic: coercive holding, rebirthing, and related forced-regression practices lack evidence, have caused harm, and should not be recommended. Prefer conventional, relationship-based, non-coercive interventions and standard child protection practice.[2][1]
Australian and New Zealand practice emphasises safeguarding under state/territory child-protection law, placement stability for looked-after children, carer support, and careful adult residual formulation in community mental health. Attachment disorder labels must not pathologise culturally normative collective caregiving in Indigenous families. Adult residual care sits in stepped adult services with trauma-informed, culturally safe practice — not specialised "RAD clinics" offering coercive methods.[1][2]
| Target | Prefer | Avoid |
|---|---|---|
| Core RAD/DSED (youth) | Stable sensitive caregiving + carer coaching | Medication "for attachment" |
| Placement instability | Permanency planning, reduce moves | Serial short placements without review |
| DSED social risk | Supervision, stranger-boundary coaching | Assuming "friendly child is fine" |
| Adult residual burden | Treat current syndromes + supports | Inventing freestanding "adult RAD" |
| Carer distress | Support, psychoeducation, respite | Blaming adoptive/foster carers alone |
| Community "RAD clinics" | Evidence-based non-coercive care | Holding / rebirthing / forced regression |
| Comorbid ADHD/PTSD/depression | Standard indicated treatments | Ignoring comorbidity |
| Framework for exams; individualise and follow local governance.[1][2][11][12] |
Prognosis and disposition
With stable sensitive care, inhibited RAD features often improve. Disinhibited social engagement is more likely to persist after environmental improvement, though it can attenuate with development, coaching and reduced chaos — set realistic expectations with families.[1][5][9][13]
BEIP demonstrates that moving children from institutional care into high-quality foster care improves attachment-related and cognitive recovery trajectories relative to prolonged institutional care, with stronger benefits when intervention is earlier; comprehensive multilevel analyses continue to support causal effects of the foster-care intervention on recovery from early severe deprivation.[4][10][14]
ERA young-adult follow-up shows that early severe deprivation is associated, for some, with lasting elevation in neurodevelopmental and mental-health problems into adulthood — disposition for residual adult burden is standard adult community mental health intensity matched to current syndrome and risk, not lifelong "attachment therapy."[11]
Complications and pitfalls
- Labelling any foster/adopted child's behaviour problems as RAD without insufficient-care phenotype criteria.[1][2]
- Missing ASD or ADHD while over-diagnosing attachment disorder.[1][3]
- Missing ongoing maltreatment while discussing "attachment issues" only.[1]
- Blaming adoptive parents who are providing good care for residual DSED.[13][5]
- Referring to coercive holding/rebirthing programmes.[2]
- Prescribing psychotropics as primary treatment for attachment pattern.[1]
- Retrofitting adult personality or criminal behaviour as "adult RAD" without developmental criteria — a general-adult exam fail.[11][2]
- Ignoring genuine residual adult mental-health burden after early deprivation while arguing only about childhood labels.[11]
Special populations
Previously institutionalised and internationally adopted children are the classic high-risk groups in ERA/BEIP teaching. Looked-after youth transitioning to adult services need explicit social-boundary, exploitation, and comorbidity plans. Adults with documented early institutional deprivation need careful residual formulation and standard adult care. Indigenous and culturally diverse families require culturally safe assessment — collective caregiving is not automatically "insufficient care." Parents of children with attachment disorders seen in adult/family clinics need psychoeducation that rejects coercive therapies and supports permanency.[4][5][6][11][13]
Evidence, guidelines and controversies
Primary written standard. AACAP Practice Parameter for RAD and DSED (Zeanah, Chesher, Boris 2016) — assessment, caregiving-first treatment, and differential diagnosis teaching point for all boards.[1]
Safety line. APSAC task force (Chaffin 2006) rejects dangerous attachment therapies — mandatory viva knowledge.[2]
Causal environment evidence. Nelson et al. Science 2007 BEIP cognitive recovery; McGoron mediation analyses; King et al. multilevel AJP 2023 recovery analyses.[4][10][14]
Phenotype validity. Gleason et al. evidence-derived criteria for inhibited and disinhibited types; Zeanah/Smyke indiscriminate behaviour in institutions; Bruce et al. internationally adopted disinhibited behaviour; Kay/Green middle-childhood UK adoptees.[3][7][9][13]
Longitudinal residual risk. O'Connor and Rutter attachment disorder behaviour after deprivation; Rutter group heterogeneity; Sonuga-Barke Lancet 2017 child-to-adult trajectories — the GA-facing evidence spine.[5][6][11]
Intervention model. Yarger et al. ABC RCT in internationally adopted children — nameable carer-coaching evidence.[12]
Controversies examiners probe: residual versus positive diagnosis of attachment problems; how long DSED features persist; whether adult residual burden should ever be labelled as attachment disorder; boundary with ASD/ADHD; community marketing of coercive therapies.[1][2][11]
Exam pearls
CARE SAFE plan
Self-test: high-yield traps
- DSM-5-TR split? RAD and DSED are separate disorders (not DSM-IV single-type framing).
- Developmental age threshold? At least 9 months; RAD onset before age 5.
- First-line treatment? Stable sensitive caregiving + carer coaching — not medication for attachment.
- Which phenotype more often persists after good care? DSED / disinhibited features.
- APSAC line? Refuse coercive holding/rebirthing.
- Adult pearl? Residual deprivation burden (ERA young adult) ≠ invent adult RAD for forensic convenience.
- Always differential? ASD and ADHD.
- Landmark environment trial? BEIP foster-care randomisation after institutional care.[1][2][3][4][11]
References
- [1]Zeanah CH, Chesher T, Boris NW; AACAP Committee on Quality Issues Practice Parameter for the Assessment and Treatment of Children and Adolescents With Reactive Attachment Disorder and Disinhibited Social Engagement Disorder J Am Acad Child Adolesc Psychiatry, 2016.PMID 27806867
- [2]Chaffin M, Hanson R, Saunders BE, Nichols T, et al. Report of the APSAC task force on attachment therapy, reactive attachment disorder, and attachment problems Child Maltreat, 2006.PMID 16382093
- [3]Gleason MM, Fox NA, Drury S, Smyke A, et al. Validity of evidence-derived criteria for reactive attachment disorder: indiscriminately social/disinhibited and emotionally withdrawn/inhibited types J Am Acad Child Adolesc Psychiatry, 2011.PMID 21334562
- [4]Nelson CA 3rd, Zeanah CH, Fox NA, Marshall PJ, et al. Cognitive recovery in socially deprived young children: the Bucharest Early Intervention Project Science, 2007.PMID 18096809
- [5]O'Connor TG, Rutter M; English and Romanian Adoptees Study Team Attachment disorder behavior following early severe deprivation: extension and longitudinal follow-up J Am Acad Child Adolesc Psychiatry, 2000.PMID 10846304
- [6]Rutter ML, Kreppner JM, O'Connor TG; English and Romanian Adoptees study team Specificity and heterogeneity in children's responses to profound institutional privation Br J Psychiatry, 2001.PMID 11483469
- [7]Zeanah CH, Smyke AT, Dumitrescu A Attachment disturbances in young children. II: Indiscriminate behavior and institutional care J Am Acad Child Adolesc Psychiatry, 2002.PMID 12162634
- [8]O'Connor TG, Marvin RS, Rutter M, Olrick JT, et al. Child-parent attachment following early institutional deprivation Dev Psychopathol, 2003.PMID 12848433
- [9]Bruce J, Tarullo AR, Gunnar MR Disinhibited social behavior among internationally adopted children Dev Psychopathol, 2009.PMID 19144228
- [10]McGoron L, Gleason MM, Smyke AT, Drury SS, et al. Recovering from early deprivation: attachment mediates effects of caregiving on psychopathology J Am Acad Child Adolesc Psychiatry, 2012.PMID 22721591
- [11]Sonuga-Barke EJS, Kennedy M, Kumsta R, Knights N, et al. Child-to-adult neurodevelopmental and mental health trajectories after early life deprivation: the young adult follow-up of the longitudinal English and Romanian Adoptees study Lancet, 2017.PMID 28237264
- [12]Yarger HA, Lind T, Raby KL, Zajac L, et al. Intervening With Attachment and Biobehavioral Catch-Up to Reduce Behavior Problems Among Children Adopted Internationally: Evidence From a Randomized Controlled Trial Child Maltreat, 2022.PMID 33882710
- [13]Kay C, Green J, Sharma K Disinhibited Attachment Disorder in UK Adopted Children During Middle Childhood: Prevalence, Validity and Possible Developmental Origin J Abnorm Child Psychol, 2016.PMID 26857922
- [14]King LS, Guyon-Harris KL, Valadez EA, Radulescu A, et al. A Comprehensive Multilevel Analysis of the Bucharest Early Intervention Project: Causal Effects on Recovery From Early Severe Deprivation Am J Psychiatry, 2023.PMID 37211832