Psych · General adult psychiatry — psychotic disorders
Schizoaffective disorder
Also known as Schizoaffective · SAD bipolar type · SAD depressive type · Schizoaffective psychosis · Affective psychosis continuum
Exam-exhaustive fellowship reference on schizoaffective disorder — DSM-5-TR and ICD-11 operational criteria; bipolar versus depressive type; longitudinal discrimination from schizophrenia and bipolar with psychosis; antipsychotic foundation with mood-stabiliser and careful antidepressant use; suicide risk including InterSePT; course and RANZCP/APA/NICE-oriented guidance. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Schizoaffective disorder (SAD) sits on the examinable fault line between schizophrenia spectrum and bipolar/major depression with psychosis. Fellowship exams punish cross-sectional labelling ("psychotic and depressed today = SAD") and reward a life-chart defence of the two duration rules. Treatment is not "schizophrenia meds plus random antidepressant": you choose an antipsychotic with trial support where available, treat the pole carefully, and own suicide risk at this interface.[1][2][8]
Overview and definition
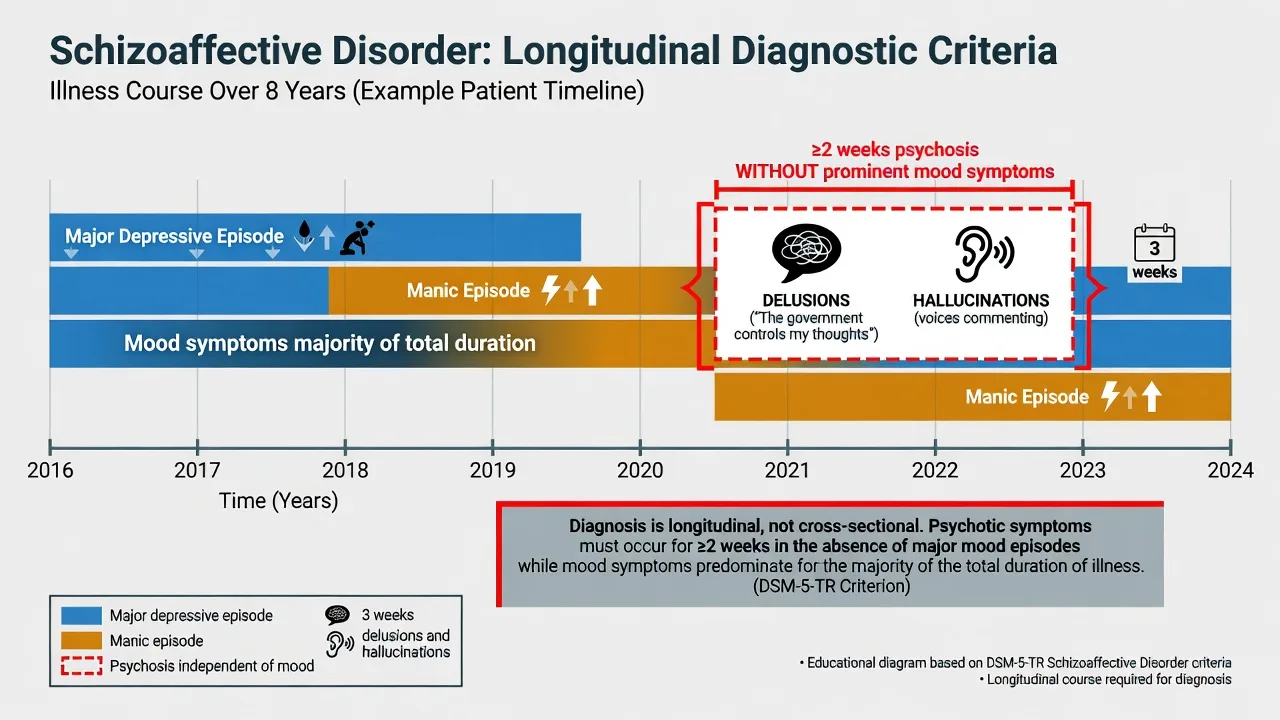
Schizoaffective disorder is an operational clinical syndrome in which a major mood episode (manic or major depressive) occurs concurrently with active-phase schizophrenia Criterion A symptoms, and the longitudinal course includes both (a) mood symptoms for most of the total duration of the active and residual illness and (b) a clear stretch of psychosis without a major mood episode.[1][20]
DSM-5-TR core logic (reproduce this at viva). Malaspina and colleagues, writing for the DSM-5 psychosis workgroup context, emphasise that SAD is defined to capture people who truly sit between pure schizophrenia and pure mood psychosis — not to name every mixed presentation. The diagnosis is inherently longitudinal. A single admission MSE is never enough.[1]
| Criterion concept | What examiners want you to say |
|---|---|
| Concurrent syndromes | Uninterrupted period with major mood episode and Criterion A symptoms (delusions, hallucinations, disorganised speech, grossly disorganised/catatonic behaviour, negative symptoms — with the usual DSM threshold structure for schizophrenia) |
| Psychosis without mood | Delusions or hallucinations for at least 2 weeks in the absence of a major mood episode during the lifetime course of the illness |
| Mood majority | Symptoms meeting criteria for a major mood episode are present for the majority of the total duration of the active and residual portions of the illness |
| Exclusion | Not attributable to substance/medication or another medical condition |
ICD-11. ICD-11 also recognises schizoaffective disorder as a psychotic disorder with concurrent mood episode features and substantial mood symptom contribution to the course. Board answers should state the manual you are using and avoid inventing identical day-count thresholds if the local exam stem specifies ICD. The shared examiner message is the same: time-course discrimination, not a single cross-section.[1][10]
Historical note (one viva line). Kasanin’s older “schizoaffective” concept was broader and less operational. Modern SAD is stricter and deliberately rarer than casual clinical use of the term.[1][3]
Classification
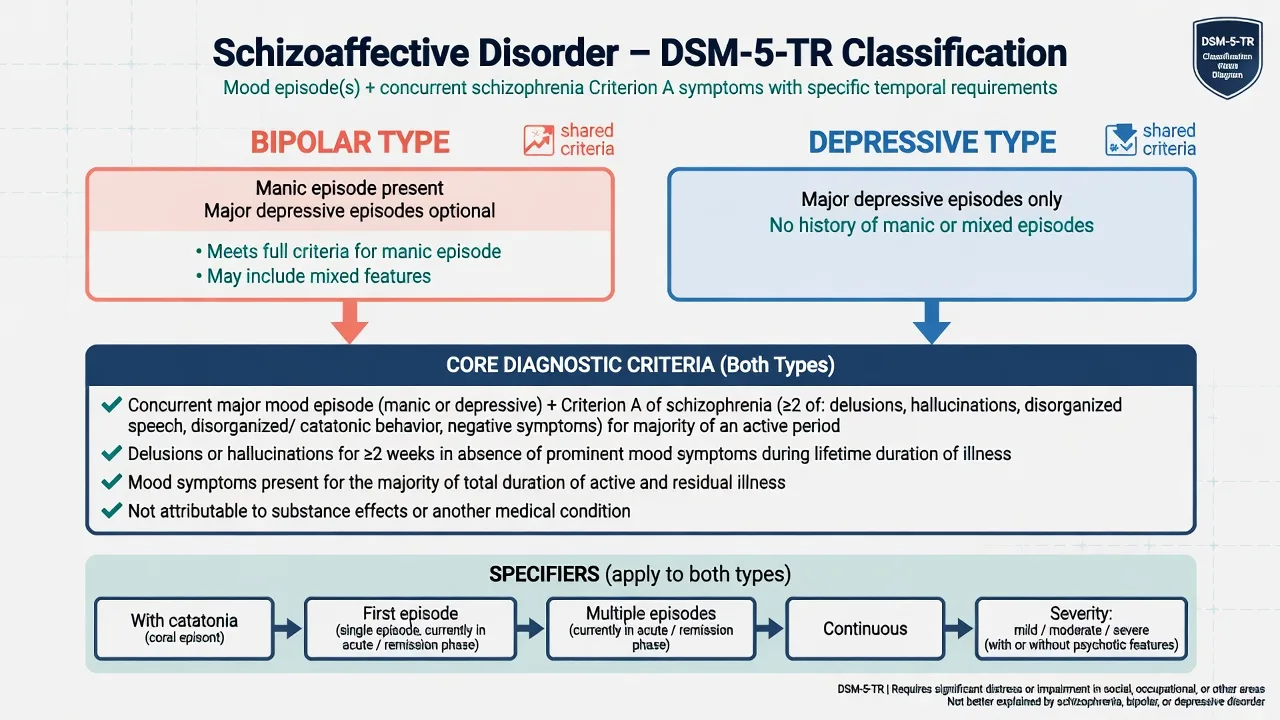
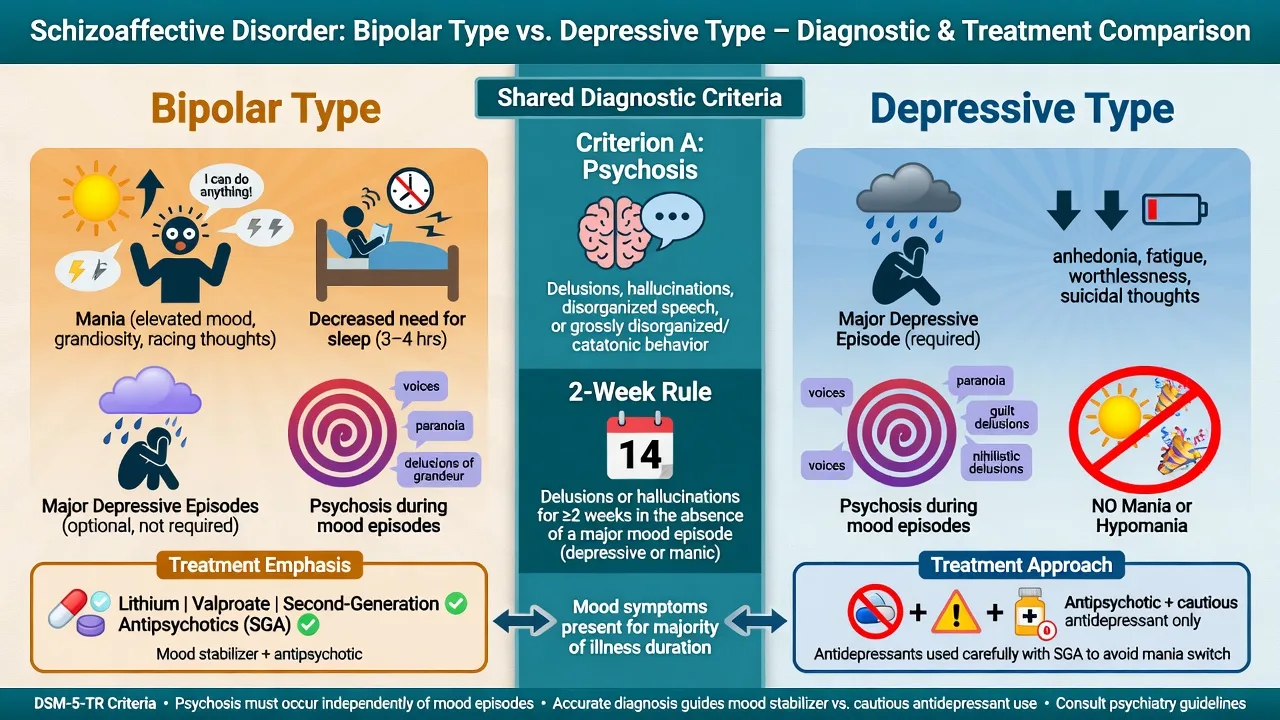
Bipolar type
- Manic episode is part of the course (major depression may also occur)
- Highest switch risk if antidepressants are used carelessly
- Mood stabiliser or antimanic SGA often needed alongside antipsychotic
- Sleep collapse and elevated energy are early relapse cues
Depressive type
- Major depressive episodes only — no lifetime mania/hypomania meeting criteria
- Psychosis may be mood-congruent or incongruent
- Antidepressant only with antipsychotic cover and polarity vigilance
- Suicide risk remains high — treat depression aggressively and safely
Shared core
- Criterion A psychosis concurrent with mood episode
- ≥2 weeks delusions/hallucinations without major mood
- Mood symptoms majority of total illness duration
- Substance/medical exclusion
Useful specifiers
- With catatonia
- First episode / multiple episodes
- Current episode severity and course descriptors
- Document residual negative symptoms when present
Bipolar type vs depressive type — one rule. If there has ever been a manic episode meeting criteria in the course of the illness, the type is bipolar. Depressive type requires major depressive episodes without a manic history. Hypomania alone does not create bipolar I mania, but any true mania reclassifies type and changes antidepressant safety calculus.[1][19]
Epidemiology and risk factors
Numbers and framing candidates must own
Population studies of psychotic disorders show that broadly defined psychotic and bipolar I conditions are not rare when carefully ascertained; strictly defined schizoaffective disorder is a smaller slice than schizophrenia in clinical series because the dual duration rules are hard to meet.[16][2] Do not quote a single universal lifetime prevalence as dogma — quote the logic and cite epidemiology that places psychotic disorders in population context.[16]
Risk factors largely overlap the schizophrenia and bipolar spectra: family history of psychosis or bipolar disorder, cannabis (especially high-THC adolescent use), obstetric and neurodevelopmental adversity, urbanicity/migration stress pathways, and sleep disruption for polarity.[15][19][10]
Mortality and suicide. Schizophrenia-spectrum cohorts show excess all-cause mortality driven by cardiovascular disease, smoking-related illness, and suicide — care principles transfer to SAD.[18] Lifetime completed suicide risk in schizophrenia has been reexamined toward roughly 5% completed (attempts higher) — use precise language, not the outdated “10–15% completed” folklore, while still treating risk as high and actionable.[17] InterSePT enrolled high-risk schizophrenia and schizoaffective patients when testing clozapine versus olanzapine for suicidal behaviour.[8]
Pathophysiology
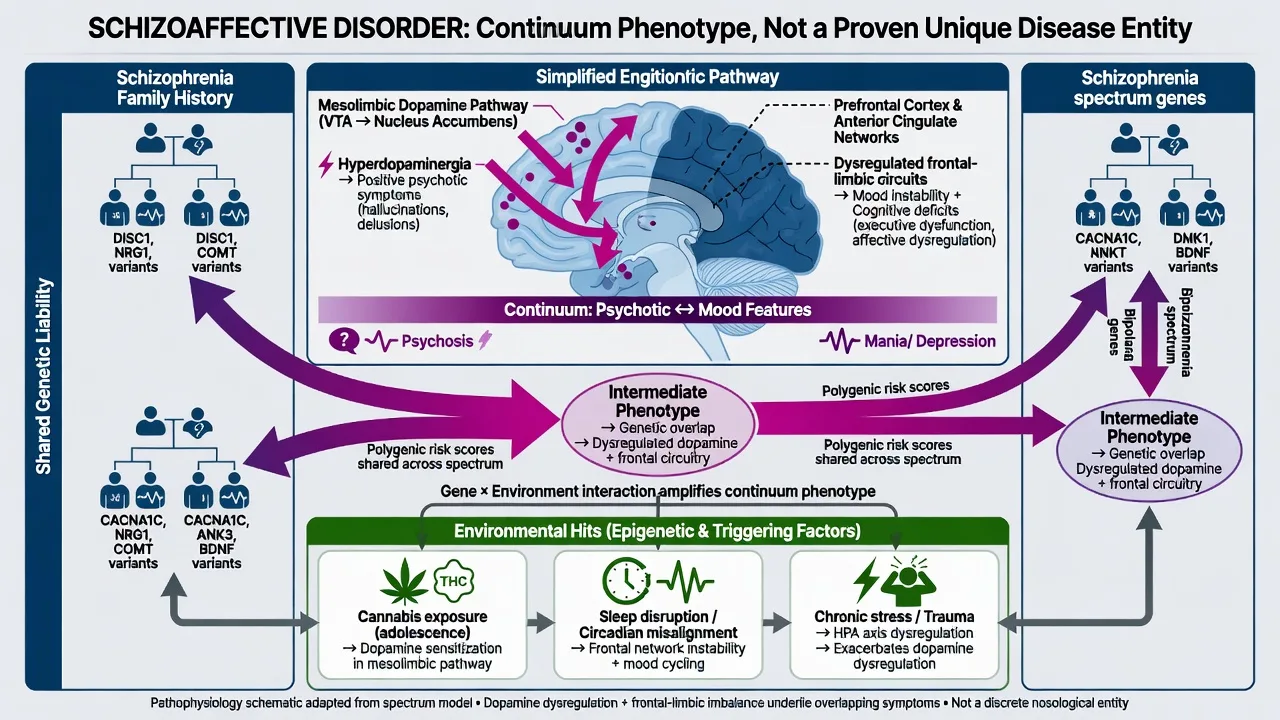
There is no examiner-proof unique “schizoaffective circuit.” The viva-safe position: SAD is a clinical bridge phenotype on the psychosis–mood continuum, with overlapping genetic liability and heterogeneous biology.[2][3]
Psychosis arm. Howes and Kapur’s dopamine hypothesis version III remains the practical map: striatal hyperdopaminergia as a final common pathway for positive symptoms, with frontal hypodopaminergia linked to negative and cognitive domains — explaining why D2-modulating antipsychotics help positive symptoms but do not “cure” cognition.[15]
Mood arm. Polarity involves monoaminergic tone, circadian instability, and kindling-like recurrence patterns familiar from bipolar medicine. Sleep loss is both symptom and mechanism for mania risk.[19]
Nosological controversy. Systematic comparison finds SAD often intermediate between schizophrenia and mood disorders on many validators, feeding arguments that it is not a discrete natural kind — yet the operational category remains clinically useful for treatment planning when criteria are met carefully.[2][3]
Clinical presentation
Concurrent picture. Expect Criterion A phenomena (for example third-person commentary hallucinations, persecutory or grandiose delusions, thought disorder) together with a full major depressive or manic syndrome — not merely dysphoria or irritability from psychosis.[1][20]
Bipolar type MSE language. Elevated or irritable mood, decreased need for sleep, pressured speech, grandiosity or racing thoughts, plus psychosis that may be mood-congruent (grandiose special mission) or incongruent (bizarre passivity). Risk: sexual disinhibition, spending, aggression, driving, absconding.[19][1]
Depressive type MSE language. Low mood, anhedonia, guilt, psychomotor change, early waking, plus delusions of guilt/nihilism or mood-incongruent Schneiderian phenomena. Risk: suicide, self-neglect, starvation, command hallucinations.[1][17]
The critical “psychosis-only” window. Collateral must document at least 2 weeks of delusions or hallucinations when the patient was not in a major mood episode. Without this, bipolar/MDD with psychotic features remains more likely.[1]
Course texture. Residual negative symptoms, cognitive inefficiency, and incomplete functional recovery are common and may look “schizophrenia-like” between mood episodes; some patients recover more completely between poles — reassess longitudinally.[2][10]
Differential diagnosis
| Differential | Points toward this | Points toward SAD |
|---|---|---|
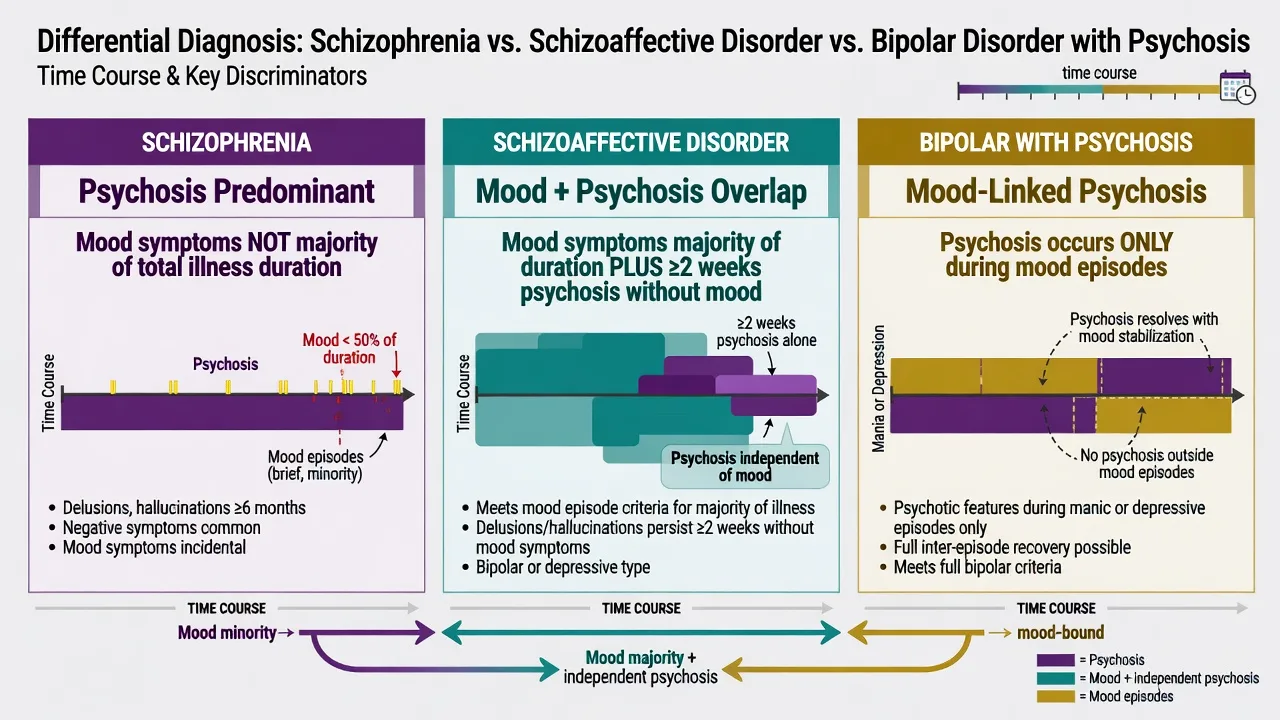
| Schizophrenia | Mood episodes brief relative to total duration; psychosis dominates residual course | Mood symptoms occupy majority of total active/residual duration and clear ≥2-week psychosis-without-mood |
| Bipolar I with psychotic features | Psychosis only during mania/depression | Psychosis continues for ≥2 weeks after mood episode ends (or between poles) |
| MDD with psychotic features | Psychosis confined to depressive episodes; no mania | Same 2-week and majority rules; bipolar type if mania ever present |
| Substance-induced | Clear intoxication/withdrawal timeline; resolves with abstinence | Persists weeks after abstinence; lifetime polarity and psychosis chart independent of drug |
| Delirium / encephalitis / medical | Fluctuating attention, fever, focal neurology, seizure, rapid cognitive plunge | Clear sensorium, typical longitudinal psychiatric course |
| Personality / PTSD / OCD | Reactive short affective shifts; overvalued ideas with residual insight spectrum | Sustained syndromal mood + true delusions/hallucinations meeting criteria |
First-episode caution. Early psychosis with mood symptoms often deserves a working label (first-episode psychosis, schizophreniform, affective psychosis) until duration data mature. Premature “SAD forever” is an exam and clinical error.[10][1]
Clinical and bedside assessment
Structure assessment as life-chart + risk + capacity + organic screen + collateral.[10][11]
- Longitudinal chart: age of onset; each mania/depression; each pure-psychosis interval; hospitalisations; self-harm; treatments and adherence; substances; perinatal episodes.
- Current MSE with quoted examples of delusions, hallucinations, mood, sleep hours, insight.
- Risk: suicide (intent, plan, means, command content, mixed features, alcohol), violence, vulnerability, neglect, absconding, child protection, forensic history.
- Capacity and legal status: decision-specific capacity; least-restrictive care under local statute — name the principle, do not invent foreign section numbers.
- Collateral from family/carers is often decisive for the majority-duration and 2-week rules.
- Scales conceptually: PANSS for psychosis severity; YMRS for mania; MADRS/HAM-D for depression; CGI for global change.[10][11][19]
Investigations
Before antipsychotics and mood stabilisers, complete a safety baseline aligned with schizophrenia-spectrum physical health standards.[10][11]
- Bloods: FBC, U&E/eGFR, LFT, fasting glucose or HbA1c, lipids, TFT (essential if lithium planned), consider calcium with lithium long-term.
- ECG: QTc and cardiac risk before many antipsychotics.
- Weight/BMI, BP, waist circumference.
- Pregnancy test when relevant; discuss contraception before valproate.
- Urine drug screen supports formulation; negative screen does not exclude recent use or primary SAD.
- CT/MRI, EEG, autoimmune encephalitis panel when first presentation is atypical, late-onset, focal neurology, seizure, or rapid cognitive decline.[10][11]
Management — acute and emergency
Agitation ladder. De-escalate; offer oral antipsychotic and/or benzodiazepine per local protocol; IM options if necessary; avoid hazardous combinations (notably parenteral olanzapine with parenteral benzodiazepines in many safety frameworks).[10][11]
Pole-specific acute priorities follow the active pole while psychosis is covered.[10][19]
- Mania + psychosis: antimanic coverage (SGA and/or lithium/valproate), sleep, stimulation reduction, capacity/legal review.[19][7]
- Depression + psychosis: suicide risk, consider ECT for severe/psychotic depression with food refusal or high intent, ensure antipsychotic cover if using antidepressant later.[10][8]
- Catatonia: lorazepam challenge pathway and ECT readiness — do not force high-potency antipsychotic as first move in retarded catatonia.[10]
Medical emergencies (NMS, lithium toxicity, serotonin toxicity if serotonergic agents used) follow standard medical psychiatry algorithms — stop culprit agents, resuscitate, escalate.[10][11]
Management — definitive and stepwise
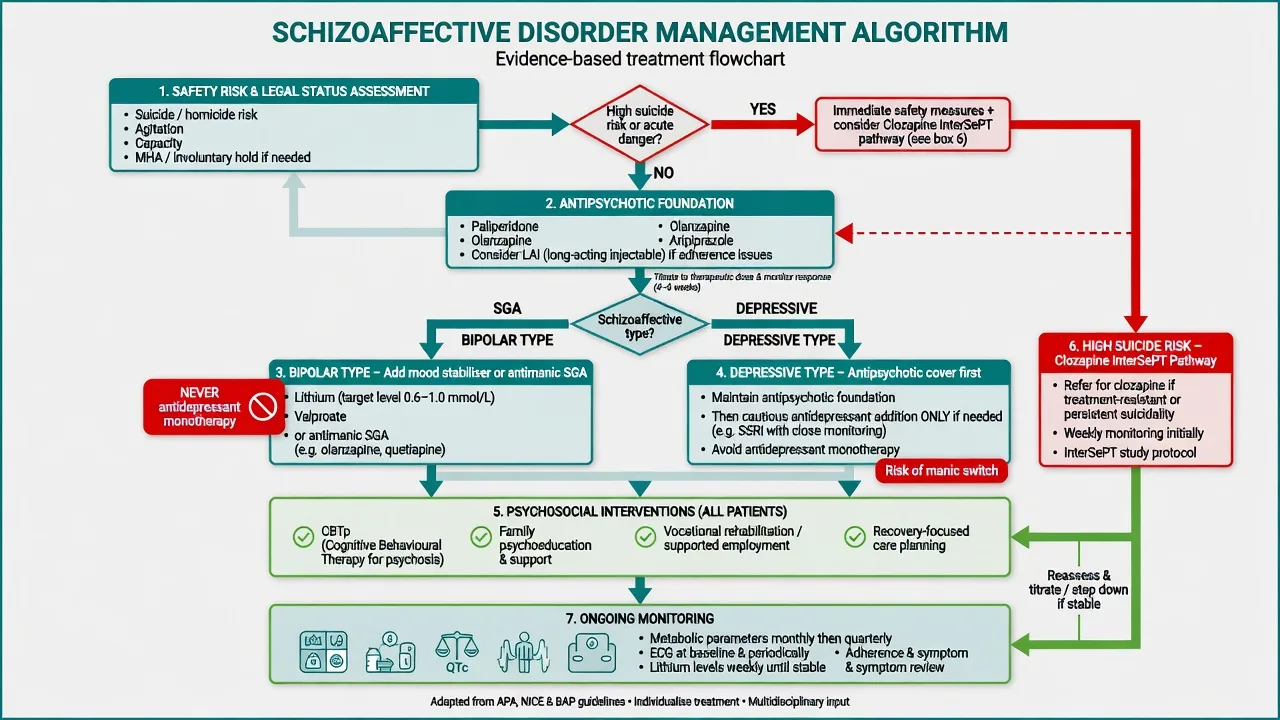
Antipsychotic foundation
Because Criterion A psychosis defines the disorder, an antipsychotic is usually the pharmacological backbone. Comparative efficacy across schizophrenia trials informs agent choice; side-effect matching and prior response matter more than brand loyalty.[12][13][10]
Schizoaffective-specific trial anchors give phenotype-level evidence beyond schizophrenia-only trials.[4][5][6]
- Paliperidone extended-release has placebo-controlled evidence in schizoaffective disorder across fixed dose-range and flexible-dose designs, including patients with or without adjunctive antidepressants/mood stabilisers. Adult trial frameworks commonly used 6–12 mg oral daily ranges (individualise; start lower in first-episode/elderly; check product information).[4][5]
- Paliperidone palmitate once-monthly reduced relapse of psychotic, depressive, and manic symptoms versus placebo in maintenance data for schizoaffective disorder — strong argument for LAI when adherence is the fracture point.[6]
- Olanzapine versus haloperidol data in schizoaffective disorder bipolar type support SGA utility on this phenotype (efficacy with differing tolerability).[7]
Illustrative adult oral starting frameworks (always localise to product info, comorbidity, and prior response) are drawn from SAD trials and schizophrenia-spectrum guidance.[4][12][10]
| Agent | Typical adult approach | Key monitoring |
|---|---|---|
| Paliperidone ER | Often 6 mg daily; trial ranges up to about 12 mg in SAD studies | Prolactin, EPS, metabolic, renal dosing adjustments |
| Olanzapine | Often 10 mg nightly; titrate toward 10–20 mg | Weight, glucose, lipids, sedation |
| Risperidone | Often 1–2 mg daily; titrate toward 2–6 mg | Prolactin, EPS |
| Aripiprazole | Often 10–15 mg daily | Akathisia |
| Quetiapine | Sedating option; titrate by indication | Metabolic, BP, sedation |
| LAI options | Paliperidone palmitate, aripiprazole LAI, others per protocol | Injection schedule + same class monitoring |
| Dose ranges are illustrative adult frameworks from SAD trials and schizophrenia-spectrum guidance — individualise and check product information.[4][5][6][12][10][11] |
Trial length for adequacy is typically in the 4–6 week therapeutic-dose window before declaring non-response, with adherence verified — pseudo-resistance is common.[14][11]
Type-specific mood treatment
Bipolar type. Add a mood-stabilising strategy alongside the antipsychotic backbone.[19][10]
- Lithium when polarity, suicide risk, and monitoring infrastructure support it — 12-hour trough targets commonly around 0.6–0.8 mmol/L for maintenance (higher acute mania targets may be used short-term, e.g. toward 0.8–1.2 mmol/L), with eGFR, TFT, calcium, and interaction counselling (NSAIDs, ACE inhibitors/ARBs, thiazides, dehydration).[9][19]
- Valproate for acute mania adjunct in appropriate patients — avoid in pregnancy and people who may become pregnant without exceptional justification and robust prevention frameworks; monitor LFT/FBC.[19][10]
- Antimanic SGAs (olanzapine, quetiapine, aripiprazole, risperidone, etc.) often dual-task as antipsychotic + antimanic agents.[7][12]
- Never antidepressant monotherapy. If an antidepressant is considered for bipolar-type depression, cover with mood stabiliser/antipsychotic, monitor sleep/activation, and keep duration intentional.[19][1]
Depressive type. Treat psychosis with antipsychotic; if depression persists, a cautious antidepressant added to antipsychotic may be used — re-check that true mania was never missed (misclassified bipolar type). Prefer agents and doses you can monitor; watch for switch, agitation, and suicide risk early in recovery of energy.[5][10]
Suicide-focused pharmacology
- Clozapine outperformed olanzapine for suicidal behaviour in InterSePT among high-risk schizophrenia spectrum patients including schizoaffective disorder — relevant when suicidality is prominent, independent of pure TRS framing.[8]
- Lithium has meta-analytic support for reducing suicide-related outcomes in mood disorders — consider when bipolar-type polarity and monitoring allow.[9]
- Neither replaces means restriction, leave arrangements, crisis planning, or admission when needed.[8][17]
Treatment resistance
If two adequate, adherent antipsychotic trials fail for persistent psychosis, apply TRRIP principles and offer clozapine with full monitoring (neutrophils, myocarditis vigilance early, bowel care, metabolic, levels) rather than chaotic polypharmacy.[14][10][11]
Psychosocial and recovery care
Offer family psychoeducation, CBTp access, substance interventions (especially cannabis), supported employment/education, sleep regularity, and peer support within a recovery framework — RANZCP schizophrenia-and-related-disorders guidance embeds multi-element care, not pills alone.[10][11]
Specific subtypes and scenarios
First mixed presentation. Stabilise, exclude organic causes, treat acute pole and psychosis, document timeline carefully; revise diagnosis at 6–12 months rather than branding permanent SAD from week one.[10][1]
Catatonia specifier. Treat catatonia syndrome (benzodiazepine, ECT) while managing underlying mood–psychosis illness.[10]
Substance-comorbid SAD. Dual formulation: primary spectrum illness and substance use disorder. Abstinence improves diagnostic clarity and relapse rates; do not withhold indicated antipsychotics during dangerous psychosis.[10][16]
Community multi-episode care. LAI consideration, carer education on early warning signs (sleep loss, cannabis, voices returning, elevated energy), physical health clinics, and clozapine pathway when indicated.[6][10]
Complications and pitfalls
- Antidepressant-induced mania/mixed states in bipolar type.[19]
- Metabolic syndrome, EPS, hyperprolactinaemia, QTc prolongation from antipsychotics.[12][13]
- Lithium toxicity; valproate teratogenicity.[9][19]
- Diagnostic instability used as an excuse for endless unreviewed polypharmacy.[2]
- Under-treatment of suicide risk and physical health.[17][18]
Prognosis and disposition
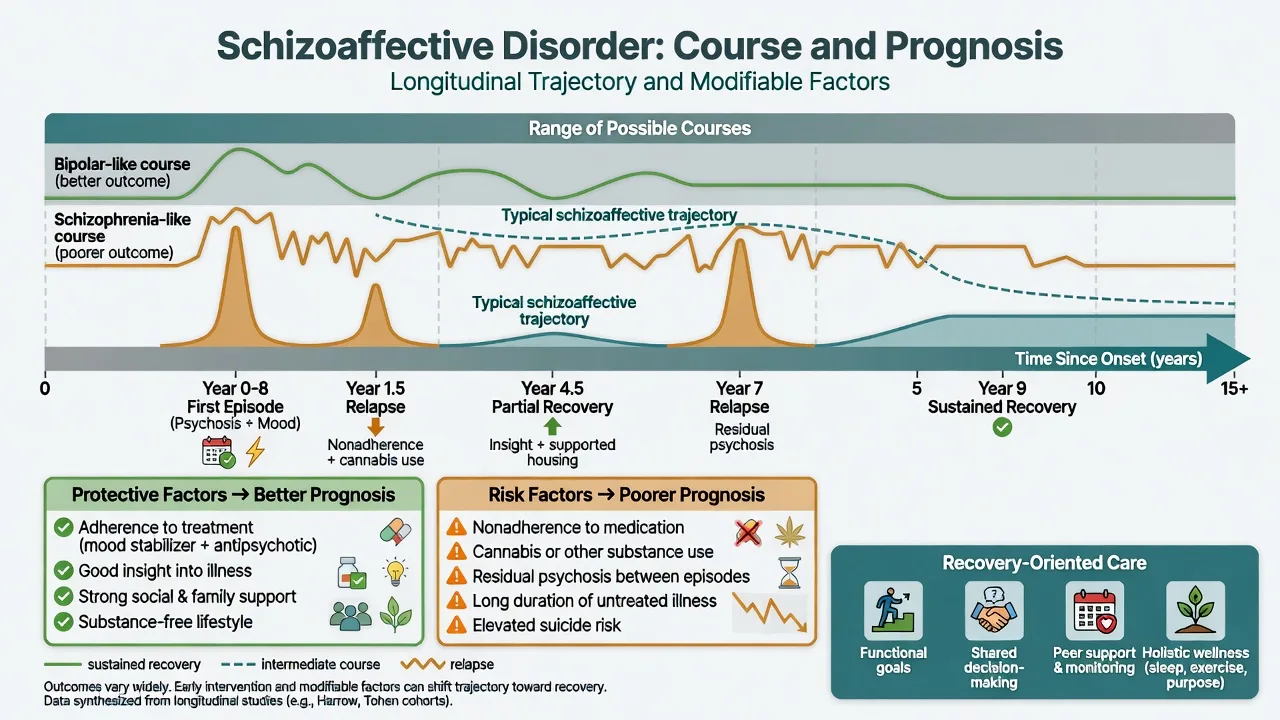
Systematic comparisons often place outcomes intermediate between schizophrenia and mood disorders at the group level, with wide individual variation — defend prognostic humility plus modifiable factors.[2]
Better signals: shorter untreated illness, good antipsychotic and mood treatment adherence, substance cessation, preserved premorbid function, strong family support, fewer residual negative symptoms.[10][2]
Worse signals: non-adherence, ongoing cannabis/stimulants, persistent positive symptoms, high suicide attempt density, medical comorbidity, isolation.[17][18]
Disposition. Admit for high suicide/violence risk, severe mania, inability to self-care, diagnostic medical uncertainty, or failed community containment. Step down with crisis plan, early-warning card, and named follow-up. Long-term care is recovery-oriented and cardiometabolically serious.[10][11]
Special populations
Youth. Prefer early intervention frameworks, family work, education retention, start-low dosing, and delayed definitive SAD labelling until criteria mature.[10]
Older adults. Intensify organic work-up for late first presentations; mind QTc, falls, renal function for lithium, and anticholinergic burden.[10][11]
Pregnancy and lactation. Avoid valproate. Lithium is a specialist risk–benefit discussion with levels and fetal medicine liaison. Prefer agents with better reproductive data when clinically suitable; do not leave severe psychosis untreated. Distinguish postpartum psychosis from chronic SAD relapse using timeline and past history.[19][10]
Cultural formulation. Delusional content is culture-shaped; form, duration, and function still decide diagnosis. Address access barriers and family explanatory models without abandoning operational criteria.[10]
Evidence, guidelines and regional differences
RANZCP clinical practice guidelines for schizophrenia and related disorders (Galletly et al.) provide the ANZ fellowship backbone for psychosis care — antipsychotic choice, physical health, early intervention principles, clozapine pathway, and psychosocial care — applied to schizoaffective presentations under related psychotic disorders.[10]
Landmark evidence pack to name in exams: Malaspina DSM-5 SAD paper; Cheniaux/Lake nosology debate; Canuso paliperidone ER RCTs; Fu paliperidone palmitate maintenance; Tohen olanzapine vs haloperidol bipolar-type SAD; InterSePT; Cipriani lithium anti-suicide meta-analysis; Leucht antipsychotic NMA; CATIE effectiveness context; TRRIP; FIN11 mortality; Perälä population prevalence framing.[1][2][4][6][7][8][9][12][13][14][18][16]
Exam pearls
MAJOR2
- Majority + 2 weeks are the two non-negotiable duration rules.[1]
- Type follows lifetime mania, not the current pole alone.[1]
- Antipsychotic backbone; mood treatment by type; no AD monotherapy in bipolar type.[4][19]
- InterSePT includes schizoaffective — clozapine is a suicide conversation, not only a TRS conversation.[8]
- Physical health monitoring is examinable content, not optional medicine.[18][10]
Self-test: diagnose from the stem
A 32-year-old has had continuous illness for 4 years. For most of that time he has had recurrent major depressive episodes and two manic admissions. Between poles, for three separate fortnights, he heard a running commentary and believed cameras were implanted while mood was objectively euthymic on collateral. Cannabis is occasional. Working diagnosis?[1]
Answer: Schizoaffective disorder, bipolar type — concurrent mood+psychosis history, mood majority, ≥2 weeks psychosis without mood, lifetime mania. Treat with antipsychotic ± mood stabiliser; avoid antidepressant monotherapy; address suicide and metabolic risk.[1][10]
References
- [1]Malaspina D, Owen MJ, Heckers S, et al. Schizoaffective Disorder in the DSM-5 Schizophr Res, 2013.PMID 23707642
- [2]Cheniaux E, Landeira-Fernandez J, Lessa Telles L, et al. Does schizoaffective disorder really exist? A systematic review of the studies that compared schizoaffective disorder with schizophrenia or mood disorders J Affect Disord, 2008.PMID 17719092
- [3]Lake CR, Hurwitz N Schizoaffective disorder merges schizophrenia and bipolar disorders as one disease--there is no schizoaffective disorder Curr Opin Psychiatry, 2007.PMID 17551352
- [4]Canuso CM, Lindenmayer JP, Kosik-Gonzalez C, et al. A randomized, double-blind, placebo-controlled study of 2 dose ranges of paliperidone extended-release in the treatment of subjects with schizoaffective disorder J Clin Psychiatry, 2010.PMID 20492853
- [5]Canuso CM, Schooler N, Carothers J, et al. Paliperidone extended-release in schizoaffective disorder: a randomized, controlled study comparing a flexible dose with placebo in patients treated with and without antidepressants and/or mood stabilizers J Clin Psychopharmacol, 2010.PMID 20814330
- [6]Fu DJ, Turkoz I, Simonson RB, et al. Paliperidone palmitate once-monthly reduces risk of relapse of psychotic, depressive, and manic symptoms and maintains functioning in a double-blind, randomized study of schizoaffective disorder J Clin Psychiatry, 2015.PMID 25562685
- [7]Tohen M, Zhang F, Keck PE, et al. Olanzapine versus haloperidol in schizoaffective disorder, bipolar type J Affect Disord, 2001.PMID 11869760
- [8]Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) Arch Gen Psychiatry, 2003.PMID 12511175
- [9]Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [10]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [11]Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Am J Psychiatry, 2020.PMID 32867516
- [12]Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis Lancet, 2013.PMID 23810019
- [13]Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia N Engl J Med, 2005.PMID 16172203
- [14]Howes OD, McCutcheon R, Agid O, et al. Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology Am J Psychiatry, 2017.PMID 27919182
- [15]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [16]Perälä J, Suvisaari J, Saarni SI, et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population Arch Gen Psychiatry, 2007.PMID 17199051
- [17]Palmer BA, Pankratz VS, Bostwick JM The lifetime risk of suicide in schizophrenia: a reexamination Arch Gen Psychiatry, 2005.PMID 15753237
- [18]Tiihonen J, Lönnqvist J, Wahlbeck K, et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study) Lancet, 2009.PMID 19595447
- [19]Grande I, Berk M, Birmaher B, et al. Bipolar disorder Lancet, 2016.PMID 26388529
- [20]Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5 Schizophr Res, 2013.PMID 23800613