Psych · General adult psychiatry — personality disorders
Schizoid personality disorder
Also known as ScPD · Schizoid PD · Cluster A personality disorder · Detached personality
Exam-exhaustive fellowship reference on schizoid personality disorder — DSM-5-TR and ICD-11 nosology; discriminators from avoidant PD, autism spectrum disorder, and schizotypal PD; temperament and attachment mechanisms; alliance-first low-pressure psychotherapy; pharmacotherapy limits; isolation-related suicide risk. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
3 MCQs with explanations
Target exams
Red flags
Schizoid personality disorder (ScPD) is a lower-weight but high-trap Cluster A topic across FRANZCP, MRCPsych, ABPN and MD/DNB. Examiners test operational criteria, the ScPD–avoidant and ScPD–ASD discriminators, engagement skills with low-desire patients, and whether you recognise isolation-related suicide risk beneath flat affect.[1][2][8]
Overview and definition
ScPD describes a long-standing pattern of voluntary social detachment and restricted interpersonal emotional range — typically without the cognitive-perceptual oddness that defines schizotypal PD, without the malevolent appraisal core of paranoid PD, and without frank sustained psychosis.[1][2][16]
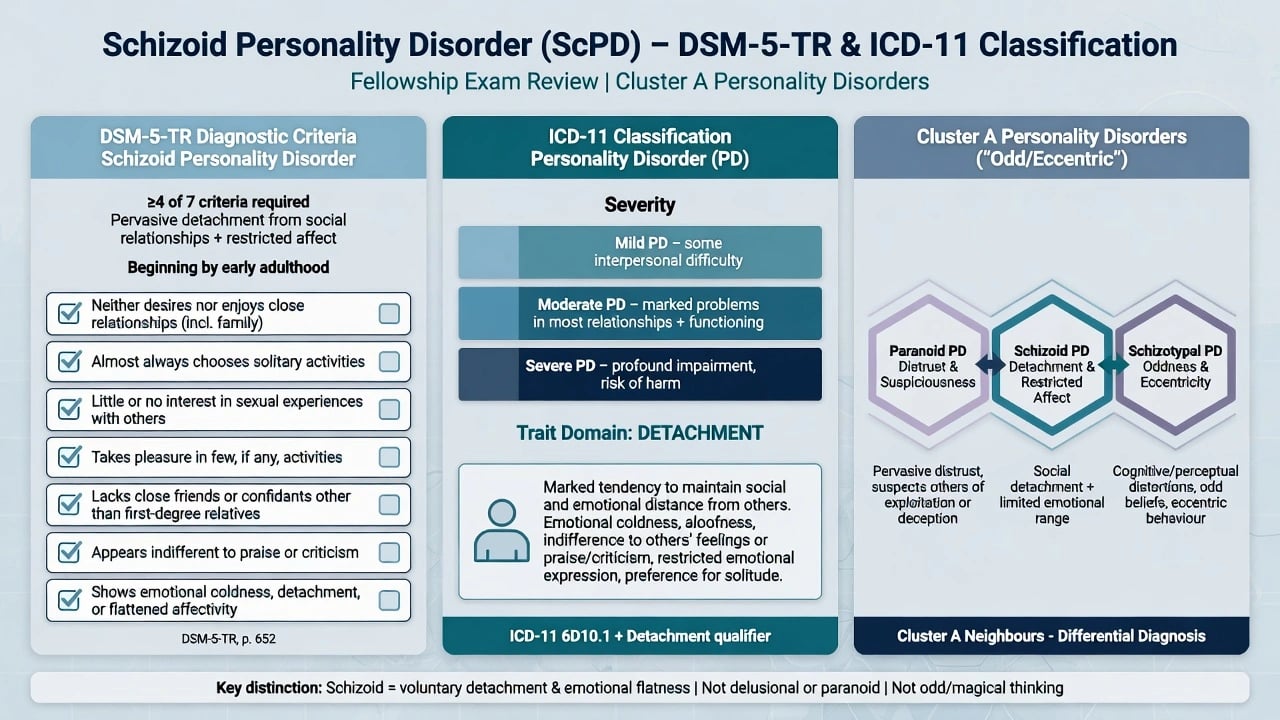
DSM-5-TR categorical diagnosis (exam-critical). After general personality disorder criteria are met, ScPD requires a pervasive pattern of detachment from social relationships and a restricted range of expression of emotions in interpersonal settings, beginning by early adulthood and present in a variety of contexts, as indicated by four or more of: neither desires nor enjoys close relationships, including being part of a family; almost always chooses solitary activities; has little, if any, interest in having sexual experiences with another person; takes pleasure in few, if any, activities; lacks close friends or confidants other than first-degree relatives; appears indifferent to the praise or criticism of others; shows emotional coldness, detachment, or flattened affectivity. The pattern must not occur exclusively during the course of schizophrenia, a bipolar or depressive disorder with psychotic features, another psychotic disorder, or autism spectrum disorder, and is not attributable to the physiological effects of another medical condition.[1][2]
ICD-11 framing. Personality disorder is graded by severity (mild, moderate, severe) with trait domain qualifiers. Features historically labelled schizoid PD map largely onto high detachment (and sometimes negative affectivity) within a severity rating. Fellowship answers should name which manual is in use and that ICD-11 is dimensional-severity first, whereas classic MCQ stems still use DSM's ≥4/7 rule.[1][2]
Validity debate (viva-ready nuance). ScPD is clinically recognisable yet among the least researched personality disorders; some authors have questioned free-standing categorical validity given overlap with avoidant traits, negative schizotypy, and autistic social phenotypes, while others argue the low-desire detachment construct remains essential for clinic and differential work.[1][9][10]
Classification and nosology
DSM-5-TR ScPD
- ≥4 of 7 detachment/restricted-affect features
- Onset by early adulthood, pervasive
- Not exclusively during psychosis or ASD
- General PD criteria also required
ICD-11 PD
- Severity first: mild / moderate / severe
- Trait domain: detachment primary
- Dimensional language aids formulation
- Legacy categorical ScPD still appears in stems
AMPD (DSM Section III)
- Criterion A: self and interpersonal impairment
- Criterion B: detachment (intimacy avoidance, restricted affectivity)
- Useful even if categorical diagnosis used
- Avoid trait lists without impairment
Cluster A neighbours
- Paranoid: malevolent appraisal core
- Schizotypal: cognitive-perceptual oddness
- Schizoid: pure voluntary detachment
- Overlap possible — formulate primary pattern
Epidemiology and risk factors
Headline epidemiology candidates must own
Community surveys document personality disorders as common enough to matter for service planning; ScPD prevalence estimates vary widely by instrument and sample and are often among the lower rates, with clinical under-representation relative to household surveys because patients rarely self-refer for personality change.[1][5][6][7] Clinical reviews emphasise disability, quality-of-life impact, and male predominance in some series without consistent sex findings across all studies.[1][2] Twin data support genetic contribution to PD risk structure with environmental interaction; do not overclaim a single "ScPD gene" or equate ScPD with schizophrenia liability as strongly as schizotypal PD.[15][16]
Pathophysiology and mechanisms
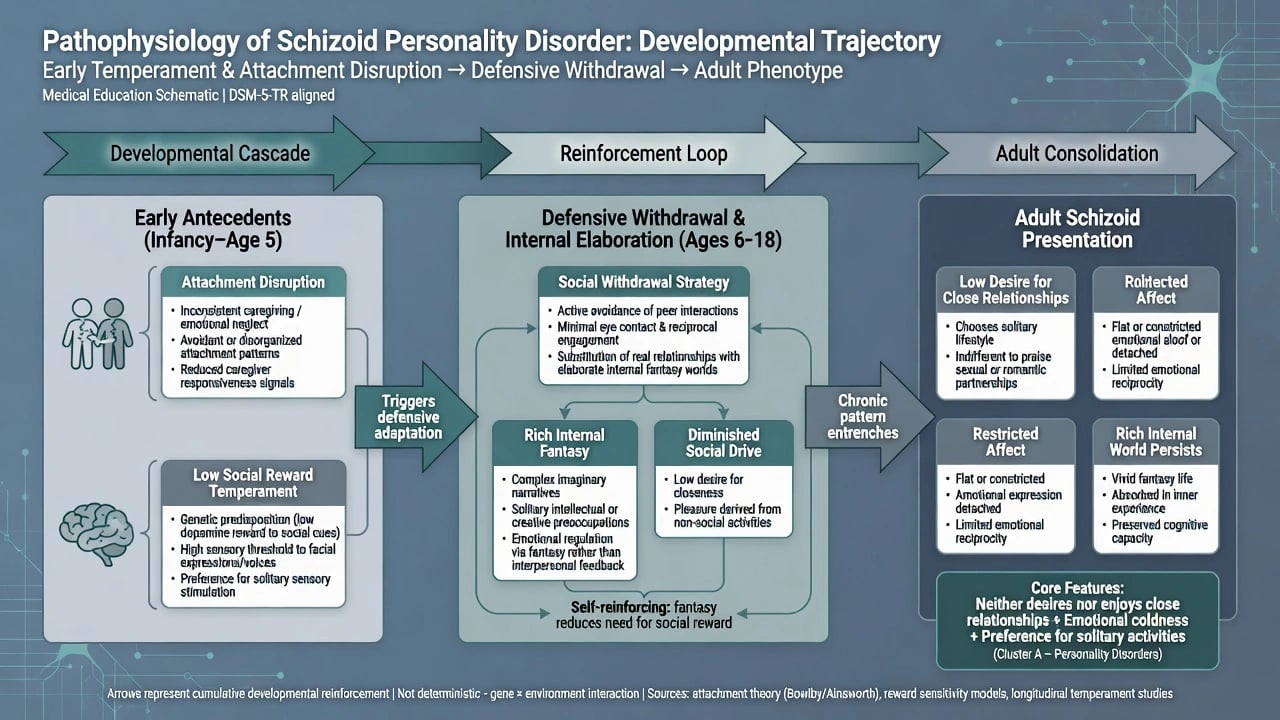
Temperament model. Clinical reviews discuss patterns of low social reward dependence, limited novelty-seeking in social domains, and high harm-avoidant tendencies that favour solitary regulation over social reinforcement. These are formulation scaffolds, not laboratory tests.[1][2]
Developmental and attachment model. Insufficient, intrusive, or inconsistent early relating may seed a defensive withdrawal strategy: real intimacy feels engulfing, and fantasy or solitary pursuits substitute for interpersonal reward. Childhood and adolescent Cluster A trait literature supports early appearance of social withdrawal patterns without equating every quiet child with lifelong ScPD.[1][8]
Cognitive-interpersonal and affect models. Low anticipated reward from closeness, restricted emotional vocabulary, and self-sufficiency schemas maintain isolation. Alexithymia correlates with schizoid traits but is not synonymous with ScPD — Coolidge and colleagues found sufficient divergence across measures to treat them as related but distinct constructs.[11]
Psychodynamic views. The classic "schizoid compromise" holds need for contact against terror of intrusion; fantasy life may be rich even when outer affect is flat. Keep as formulation language, not unfalsifiable labels.[1][2]
Neurobiology (keep humble). Limited structural work in mixed schizoid/schizotypal samples reports pyramidal pathway white-matter volume differences versus controls — hypothesis-generating only. Imaging does not diagnose ScPD.[14]
ASD continuity without collapse. Prospective and clinical studies show continuity between autistic and schizoid trait burden in some developmental pathways; still use early developmental markers, restricted/repetitive behaviours, and sensory profiles to separate ASD from ScPD rather than assuming identity.[9][10]
Clinical presentation
Core presentation combines low desire for close relationships, solitary activity preference, restricted pleasure, few confidants, indifference to praise/criticism, and emotional coldness or flattened affectivity. On MSE, expect distant but not necessarily hostile rapport, limited eye contact, sparse speech, restricted affective range, and concrete or sparse interpersonal narrative. Frank hallucinations, disorganisation, magical thinking, or fixed incorrigible delusions are not defining features — their presence forces spectrum reformulation.[1][2][16]
Settings examiners use. Primary care and occupational health see family or HR concern about "coldness"; CMHTs see depression and treatment non-engagement; crisis services see silent suicidal ideation in extreme isolation; neurodevelopmental clinics see adult ASD differential; homelessness services may enrich for severe detachment and self-neglect.[1][2][12]
Differential diagnosis
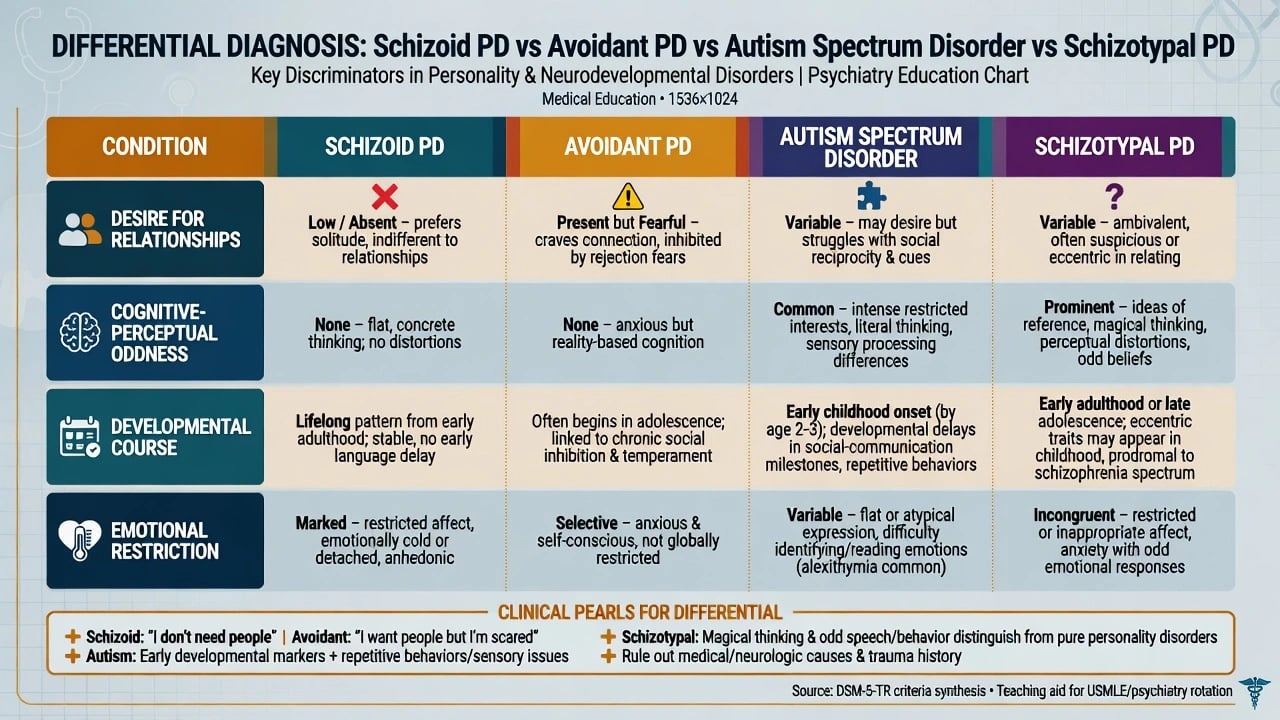
vs Avoidant PD
- AVPD: wants closeness but fears rejection/shame
- ScPD: low desire for close relationships
- Ask desire, not only avoidance behaviour
- Both may present as solitary — different core
vs Autism spectrum
- ASD: early developmental social-communication pattern
- Restricted/repetitive behaviours, sensory atypicalities
- ScPD lacks full ASD developmental signature as requirement
- Continuity of trait burden exists — formulate carefully
vs Schizotypal PD
- Odd beliefs, magical thinking, perceptual anomalies
- Eccentric speech/appearance
- ScPD may lack marked oddness
- Both Cluster A — comorbidity possible
vs Other
- Paranoid: malevolent appraisal and grudges
- Schizophrenia residual negatives: prior frank psychosis
- Depression: episodic anhedonia/withdrawal
- Late onset → organic/mood until proven otherwise
Culturally reserved communication styles, monastic or occupational solitariness without pervasive emotional restriction and impairment, and trauma-related numbing are not automatically ScPD. Cultural formulation is part of competent diagnosis.[2]
Clinical and bedside assessment
Structure the interview: developmental trajectory from school age; friendship and romantic/sexual interest history (sensitive, non-shaming); what the patient wants from relationships versus what they fear; pleasure capacity; occupational pattern; trauma; substances; prior ASD or psychosis labels; what practical problem they will own today (often sleep, work pressure, family conflict — not "personality"). Obtain collateral early; self-report may minimise social impact or distress.[1][2][8]
MSE focus. Relatedness in the room; affective range; thought content (exclude psychosis); insight into others' concern; capacity (decision-specific); suicide and self-neglect risk despite flat affect. Document how detachment appears in the room without pathologising every quiet interview.[2]
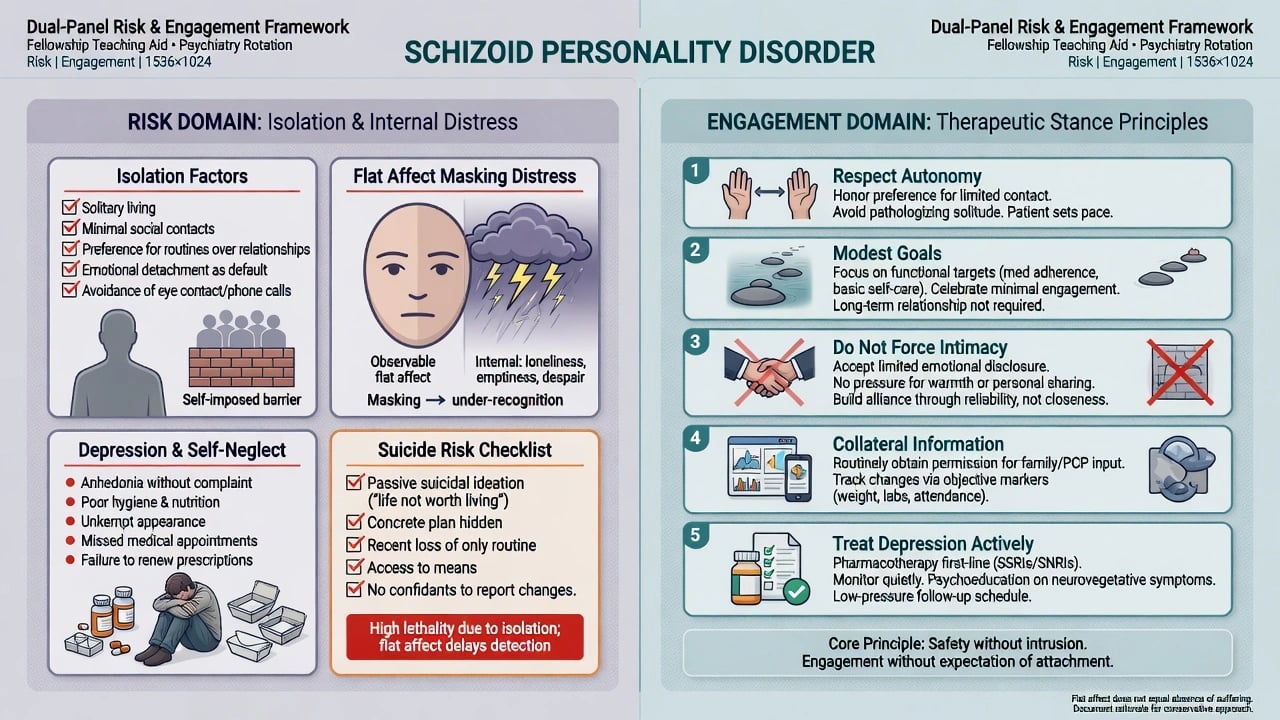
Risk domains. Suicide and self-harm risk is often underestimated when isolation, restricted affect, and low help-seeking co-occur; mini-review evidence flags schizoid traits as relevant to serious suicidal behaviour and completed suicide risk formulations.[12] Exploitation and medical neglect matter in severe isolation. Violence risk is generally less central than in paranoid presentations, but still formulate if grievances or substances are present.[1][2]
Investigations
ScPD has no laboratory gold standard. Investigate to exclude mimics and prepare for any medication: urine drug screen when relevant; FBC, U&E, LFT, TSH, glucose/lipids as baseline; pregnancy test when applicable; ECG before QT-prolonging agents; cognitive screen and neuroimaging or EEG when late-onset change, focal neurology, seizures, or significant TBI history fire. Screen systematically for depression, anxiety, ASD, substance use, other personality disorders, and frank psychosis because they change management more than the ScPD label alone.[2][4]
Management — acute crisis and resuscitation
Immediate priorities. Safety assessment for suicide, self-neglect, and medical instability; medical exclusion of organic causes of new withdrawal; least-restrictive setting. De-escalate without coercive forced socialisation. Pharmacological rapid tranquillisation is for imminent harm per local emergency protocols — not for chronic detachment.[2][4]
Crisis stance. Transparent roles; respect autonomy; do not force intimacy as a "cure"; still treat depression and medical need actively. Avoid both abandonment and engulfment.[1][2][3]
Management — definitive and stepwise
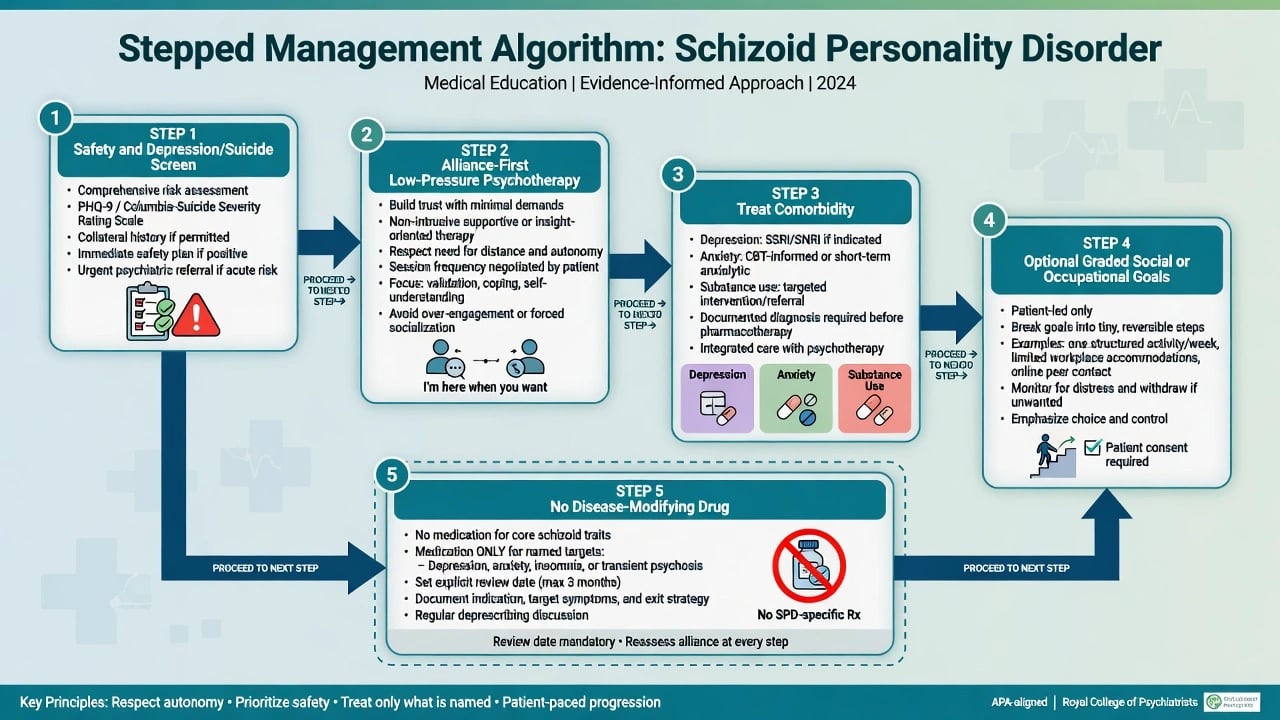
What the evidence actually supports
ScPD-specific randomised evidence is sparse because of low help-seeking and historical neglect. A 2025 systematic review and exploratory meta-analyses of psychosocial and pharmacological interventions for Cluster A disorders (including ScPD) suggest treatments can be feasible and beneficial on clinical features and functioning, but samples are small and heterogeneity is large — cite as promising, not definitive.[3] Narrative clinical reviews emphasise psychotherapy and socioeconomic stabilisation as mainstays, with pharmacotherapy ineffective for the personality pattern itself unless comorbidity is present.[1][2][4]
Psychological approaches
Alliance principles (non-negotiable in exams). Predictability, respect for interpersonal distance, collaborative modest goals, optional rather than coerced social practice, and gradual emotional vocabulary work. Early deep interpretation, forced group therapy, or aggressive intimacy demands often destroy engagement. Validate that solitude can be preferred without colluding with harmful self-neglect.[1][2][3]
Named modalities with examinable signals. Supportive and carefully adapted psychodynamic work targeting the schizoid compromise are classically taught; controlled ScPD-specific trial portfolios remain thin. Cognitive-behavioural strategies for comorbid depression, anxiety, and carefully paced behavioural activation are widely used. Schema therapy has multicentre RCT support in mixed personality disorder samples, providing transferable principles even when pure ScPD cells are small.[3][13] Cluster A treatment syntheses support psychosocial feasibility without claiming large ScPD-only RCT stacks.[3]
Pharmacotherapy — only for targets you can name
No medication treats ScPD as a whole.[2][4] Cluster A pharmacologic reviews find limited, low-quality evidence; any drug use should target named symptoms or comorbidities with review dates.[3][4]
- Major depression / anxiety: standard first-line pathways with careful engagement. Example adult plan when an examiner forces a named comorbid prescription (individualise): sertraline 50 mg orally daily, early review for activation and adherence, titrate toward 50–150 mg as tolerated with limited dispensing if overdose risk is high — this treats depression, not ScPD identity.[2][4]
- Severe agitation or marked cognitive-perceptual distress: not typical pure ScPD; if present, reassess for psychosis spectrum and only then consider time-limited low-dose second-generation antipsychotic with metabolic/ECG monitoring and a stop/review date — not chronic "personality control."[3][4][16]
- Avoid chronic antipsychotics or benzodiazepines for detachment alone; they add harm without modifying personality structure.[4]
Care system
Most patients are managed in outpatient general adult and psychotherapy pathways. Step up for acute suicide risk, frank psychosis, severe self-neglect, or uncontainable medical risk. Consistency of one agreed formulation across the team reduces iatrogenic rupture from conflicting "just make them socialise" messages.[1][2][3]
Australian and New Zealand practice emphasises cultural safety, trauma-informed engagement, and least-restrictive care. Mental Health Act statutes are state/territory-specific — name principles, not invented sections. Reserved cultural communication is not automatically ScPD.[2]
Specific subtypes and scenarios
High-functioning solitary professional. Technical excellence with minimal relationships; family distress drives referral; goals must be patient-owned (e.g. reduce family conflict, treat sleep) rather than forced sociability.[1][2]
ScPD + major depression. Highest exam trap for missed suicide risk; treat depression actively while maintaining low-pressure alliance work.[2][12]
ScPD vs adult ASD assessment. Use developmental history, restricted interests, sensory profile, and social-communication pattern; co-occurrence and trait continuity exist — dual formulation may be more honest than forced single labels.[9][10]
Severe isolation / homelessness. Self-neglect, medical non-engagement, and exploitation risk dominate; housing and physical health often precede personality rhetoric.[2]
HR-mandated counselling. Clarify limits of coerced therapy; without any shared goal, engagement is fragile — still screen risk and depression.[1][2]
Complications and pitfalls
Classic pitfalls: collapsing ScPD into ASD or residual schizophrenia without thresholds; confusing avoidant desire with schizoid low desire; therapeutic nihilism; missing silent depression and suicide risk; polypharmacy for chronic detachment; forcing intimacy or group work too early; equating alexithymia with ScPD; diagnosing from a single quiet interview without longitudinal history; pejorative labelling of introversion without impairment.[1][2][9][11][12]
Prognosis and disposition
Course is often chronic, but engagement, stable housing/work, reduced substance use, and treatment of comorbidity can improve function and quality of life. Dimensional views imply graded severity rather than lifelong categorical doom. Disposition follows risk and needs: outpatient when containable; escalation when suicide risk, frank psychosis, or severe self-neglect emerges. Reassess after relationship loss (even limited contacts), job loss, housing instability, or new depressive symptoms.[1][2][3]
Special populations
Women. Under-recognised relative to male solitary stereotypes; present via family concern or depression.[1][2]
Adolescents. Emerging detachment needs developmental and ASD formulation; avoid premature lifelong ScPD labels without longitudinal data.[8]
Older adults. New-onset withdrawal is depression, cognitive, sensory, grief, or medical until proven otherwise — not new-onset "ScPD."[2]
Cultural formulation. Reserved styles and structural isolation are not automatically personality pathology. In ANZ practice, Indigenous cultural safety and family-inclusive care are competencies.[2]
Evidence, guidelines and controversies
Core evidence pillars include clinical reviews (Triebwasser; StatPearls/Torrico), community epidemiology (Torgersen; Lenzenweger; Grant), Cluster A treatment synthesis (Cheli), Cluster A pharmacologic review (Koch), schema therapy RCT principles (Bamelis), ASD–PD interface (Lugnegård; Cook), alexithymia distinction (Coolidge), suicidality mini-review (Attademo), developmental Cluster A literature (Esterberg), limited imaging (Via), twin PD structure (Kendler), and schizotypal spectrum context (Rosell).[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16]
Mature controversies. Whether categorical ScPD should survive dimensional ICD-11 practice; how far detachment traits belong with autism networks versus schizophrenia-spectrum research; ethics of long therapies when patient ego-syntonic preference for solitude conflicts with family goals; balancing autonomy with protection from silent suicide risk.[1][9][10][12]
Exam pearls
SCHIZOID — viva checklist
SCHIZOID
≥4/7 DSM features + general PD criteria
Cold/restricted affect — still assess suicide risk
Help-seeking low — collateral and family-driven referrals common
ICD-11 severity + detachment trait language
Zero disease-modifying drug — treat comorbidity only
Oddness absent (vs schizotypal); Organic if late onset
Intimacy desire low (vs avoidant fear)
Differentiate ASD with developmental history
60-second oral summary
ScPD is DSM ≥4/7 detachment and restricted-affect features from early adulthood, not exclusively during psychosis or ASD — related to but not the same as avoidant PD (desire low vs present-but-fearful) or schizotypal PD (oddness). Mechanisms emphasise temperament, attachment withdrawal, and low social reward more than pure schizophrenia spectrum for many. Discriminate ASD, depression, residual psychosis, and late-onset organic change. Assess silent suicide and self-neglect risk despite flat affect. Treatment: alliance-first low-pressure psychotherapy, treat comorbidity aggressively, no disease-modifying drug, modest patient-owned goals, housing and occupational stability. Hope and structure beat stigma and forced sociability.[1][2][3][9][12]
References
- [1]Triebwasser J, Chemerinski E, Roussos P, Siever LJ Schizoid personality disorder J Pers Disord, 2012.PMID 23281676
- [2]Torrico TJ, Madhanagopal N Schizoid Personality Disorder StatPearls, 2026.PMID 32644660
- [3]Cheli S, Wisepape CN, Witten CDY, Floridi M, et al. Psychosocial and pharmacological interventions for cluster a personality disorders: A systematic review and two exploratory meta-analyses Personal Disord, 2025.PMID 40111791
- [4]Koch J, Modesitt T, Palmer M, Ward S, et al. Review of pharmacologic treatment in cluster A personality disorders Ment Health Clin, 2016.PMID 29955451
- [5]Torgersen S, Kringlen E, Cramer V The prevalence of personality disorders in a community sample Arch Gen Psychiatry, 2001.PMID 11386989
- [6]Lenzenweger MF, Lane MC, Loranger AW, Kessler RC DSM-IV personality disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 17217923
- [7]Grant BF, Hasin DS, Stinson FS, Dawson DA, et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2004.PMID 15291684
- [8]Esterberg ML, Goulding SM, Walker EF Cluster A Personality Disorders: Schizotypal, Schizoid and Paranoid Personality Disorders in Childhood and Adolescence J Psychopathol Behav Assess, 2010.PMID 21116455
- [9]Lugnegård T, Hallerbäck MU, Gillberg C Personality disorders and autism spectrum disorders: what are the connections? Compr Psychiatry, 2012.PMID 21821235
- [10]Cook ML, Zhang Y, Constantino JN On the Continuity Between Autistic and Schizoid Personality Disorder Trait Burden: A Prospective Study in Adolescence J Nerv Ment Dis, 2020.PMID 31856140
- [11]Coolidge FL, Estey AJ, Segal DL, Marle PD Are alexithymia and schizoid personality disorder synonymous diagnoses? Compr Psychiatry, 2013.PMID 23021894
- [12]Attademo L, Bernardini F, Spatuzzi R Suicidality in Individuals with Schizoid Personality Disorder or Traits: A Clinical Mini-Review of a Probably Underestimated Issue Psychiatr Danub, 2021.PMID 34795159
- [13]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378
- [14]Via E, Orfila C, Pedreño C, Rovira A, et al. Structural alterations of the pyramidal pathway in schizoid and schizotypal cluster A personality disorders Int J Psychophysiol, 2016.PMID 27535345
- [15]Kendler KS, Aggen SH, Czajkowski N, Røysamb E, et al. The structure of genetic and environmental risk factors for DSM-IV personality disorders: a multivariate twin study Arch Gen Psychiatry, 2008.PMID 19047531
- [16]Rosell DR, Futterman SE, McMaster A, Siever LJ Schizotypal personality disorder: a current review Curr Psychiatry Rep, 2014.PMID 24828284