Psych · General adult psychiatry — psychotic disorders
Schizophrenia spectrum and other psychotic disorders
Also known as Schizophrenia · First-episode psychosis · Treatment-resistant schizophrenia · Schizoaffective disorder · Delusional disorder · Psychotic disorders · FEP · TRS
Exam-exhaustive fellowship reference on the schizophrenia spectrum — DSM-5-TR and ICD-11 definitions; symptom domains; epidemiology and risks; dopamine hypothesis; differentials; FEP work-up; antipsychotics with landmark trials; early intervention; LAIs; TRRIP and clozapine; psychosocial care; suicide and mortality; RANZCP/NICE/APA guidance. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Schizophrenia spectrum disorders sit at the centre of every psychiatry fellowship curriculum because they demand simultaneous mastery of phenomenology, neuroscience, pharmacology, risk, law and systems of care. A FRANZCP MEQ will ask you to assess a first presentation, choose and justify an antipsychotic with doses and monitoring, recognise treatment resistance, and plan recovery-oriented aftercare. An MRCPsych CASC will test the Mental State Examination, risk assessment, and explanation of diagnosis to a family. An ABPN item will match pathway pharmacology to side-effects and force precise TRS definitions. This topic is written so a candidate who has read nothing else can answer those questions at consultant depth.[4][5][13]
Overview and definition
Schizophrenia is a clinical syndrome of disordered reality testing, thought form, behaviour and motivation, lasting long enough and severe enough to impair function, after substance and medical mimics have been reasonably excluded. It is not diagnosed by a scan and is not "split personality." The modern exam stance is operational criteria plus formulation: criteria gate the diagnosis; formulation explains why this person became ill now and what will keep them well.[7]
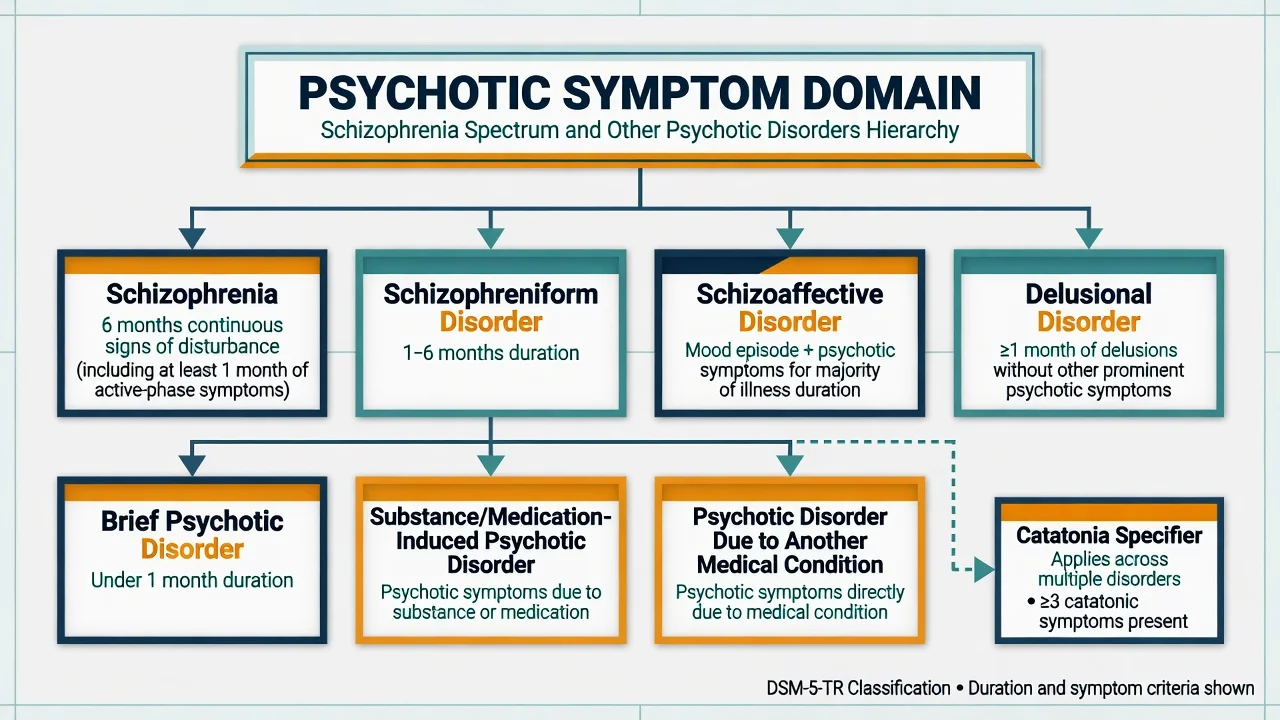
DSM-5-TR structure you must reproduce. Criterion A requires two or more of: delusions; hallucinations; disorganised speech; grossly disorganised or catatonic behaviour; negative symptoms — with at least one of the first three present. Continuous signs persist for at least 6 months, including at least 1 month of active-phase symptoms (less if successfully treated). Function is markedly below the premorbid level. Schizoaffective disorder and mood disorders with psychosis are excluded; substance and medical causes are excluded. [5]
ICD-11. Schizophrenia requires symptoms lasting at least 1 month. First-rank symptoms are no longer privileged as pathognomonic. Symptom domains are rated dimensionally. Duration differences between DSM and ICD are a classic multi-board trap — state which manual you are using. [5]
Spectrum meaning. Disorders sharing psychotic phenomenology but differing by duration, mood interface and organicity: schizophrenia, schizophreniform disorder, brief psychotic disorder, schizoaffective disorder, delusional disorder, substance/medication-induced psychotic disorder, psychotic disorder due to another medical condition, catatonia, and other/unspecified categories. [5]
Classification
Schizophrenia
- Active-phase symptoms plus 6 months continuous signs (DSM-5-TR)
- Function declined or never achieved expected level
- Not better explained by mood, substance or medical illness
- Course episodic with residual deficits or continuous
Schizophreniform
- Same Criterion A phenomenology
- Episode lasts 1 to 6 months (DSM)
- Provisional if still evolving toward schizophrenia
- Better prognosis group if full recovery
Brief psychotic disorder
- Sudden onset of psychosis
- Duration at least 1 day and less than 1 month with full return to premorbid
- May follow marked stressor (specifier)
- High exam value as the time-limited differential
Schizoaffective
- Major mood episode concurrent with Criterion A
- Delusions or hallucinations for at least 2 weeks without prominent mood symptoms
- Mood symptoms present for majority of total illness duration
- Bipolar type versus depressive type
Delusional disorder. One or more delusions for a month or more without the full schizophrenia picture; functioning not markedly impaired outside the delusional impact. Subtypes: erotomanic, grandiose, jealous, persecutory, somatic, mixed, unspecified. Engagement is the therapeutic bottleneck. [5]
Substance-induced versus primary. If symptoms occur only during intoxication or withdrawal and are better explained by the substance, label substance-induced. Persistence after abstinence, or psychosis that pre-dated heavy use, points to primary illness with comorbidity. [5]
Catatonia. Three or more of stupor, catalepsy, waxy flexibility, mutism, negativism, posturing, mannerism, stereotypy, agitation, grimacing, echolalia, echopraxia. Excited and retarded poles both kill if missed. Lorazepam challenge and ECT pathways are mandatory knowledge. [5]
Epidemiology and risk factors
Headline numbers every candidate must own
Urban upbringing, migration and social defeat, childhood adversity, obstetric complications, advanced paternal age, and cannabis use in adolescence (dose and THC potency matter) increase risk. None is necessary or sufficient.[15]
Duration of untreated psychosis (DUP). Longer DUP associates with poorer symptom and functional outcomes — the rationale for early detection and early intervention orthodoxy.[15]
Mortality. Excess deaths are multi-factorial: cardiovascular disease, smoking, metabolic treatment effects, suicide, accidents, and reduced access to physical care. The FIN11 cohort associated long-term antipsychotic treatment, including clozapine, with lower mortality than no antipsychotic in real-world data — a counter to therapeutic nihilism, without denying metabolic harm that must be managed.[8][17]
Pathophysiology
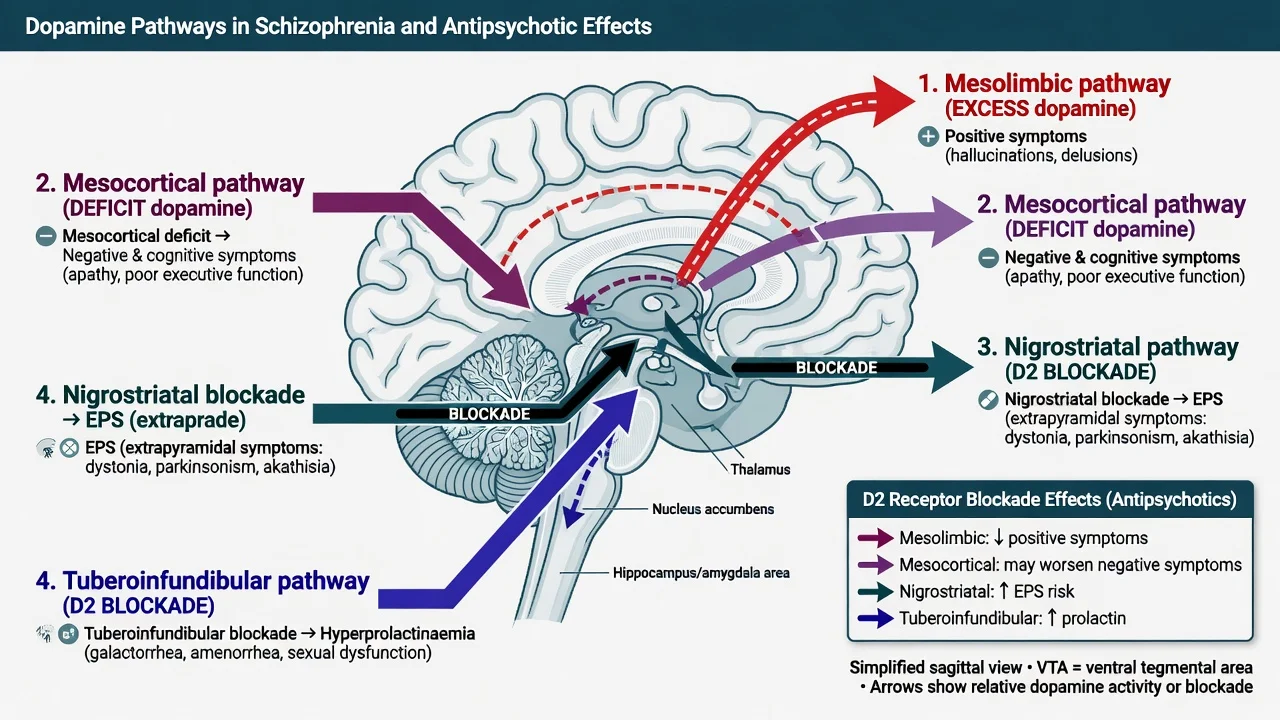
Dopamine hypothesis version III (Howes and Kapur). Multiple upstream hits converge on a final common pathway of striatal dopamine dysregulation. Excess presynaptic striatal dopamine synthesis and release links to positive symptoms and to D2-blocker efficacy. Prefrontal dopaminergic hypofunction links to negative and cognitive symptoms — pure D2 blockade often fails those domains and can worsen secondary negatives.[7]
Four pathways — clinical levers. [5]
- Mesolimbic — positive symptoms; therapeutic target of D2 blockade.
- Mesocortical — negative and cognitive symptoms; excessive blockade may worsen them.
- Nigrostriatal — EPS (dystonia, parkinsonism, akathisia, tardive dyskinesia).
- Tuberoinfundibular — hyperprolactinaemia (sexual dysfunction, amenorrhoea, galactorrhoea, bone risk). [5]
Glutamate / NMDA. NMDA hypofunction (ketamine/PCP model) produces positive, negative and cognitive-like effects and remains the leading complementary model. [5]
Neurodevelopmental framing. Early developmental alteration plus adolescent "second hits" (cannabis, stress, pruning). Imaging findings are group-level research signals — not individual diagnostic tests. [5]
Phenomenology deep-dive (MSE viva language)
Examiners award marks for precise phenomenological language, not slang. [5]
Delusions. Fixed false beliefs held with conviction, not amenable to reason, out of keeping with cultural/religious background. Specify content (persecutory, referential, grandiose, somatic, erotomanic, jealous, nihilistic, bizarre). Bizarre delusions are implausible within culture (e.g. thought withdrawal by satellite) — still not pathognomonic alone. [5]
Hallucinations. Perceptions without external stimulus, with full force of reality. Auditory verbal hallucinations may be second-person commands or third-person commentary/arguing voices. Ask content, frequency, controllability, and command compliance history. [5]
Passivity / made experiences. Thoughts, feelings, impulses or actions experienced as controlled by an external agency — classic Schneiderian phenomena still useful clinically even if ICD-11 de-emphasises first-rank exclusivity. [5]
Thought form. Derailment, tangentiality, circumstantiality, neologisms, word salad, thought blocking. Quote speech samples in the notes. [5]
Negative symptom interview tips. Ask about drive, pleasure from previously enjoyed activities, social contact, speech output — and observe affect. Screen depression before attributing everything to primary negatives. [5]
First-episode work-up checklist (printable mental model)
- Safety and observations (including glucose).
- Collateral history and timeline of DUP.
- Full MSE with risk formulation.
- Substance history with last use times.
- Physical examination including neurological soft signs if relevant.
- Baseline bloods and ECG as above.
- Pregnancy test when applicable.
- Imaging/autoimmune/EEG when red flags present.
- Shared decision on treatment setting (community EIS versus admission).
- Legal status documentation.
- Family contact and psychoeducation plan.
- Follow-up within days, not weeks, after starting treatment. [5]
Relapse signatures and early warning plans
Teach patients and families personalised early warning signs: sleep loss, cannabis restart, social withdrawal, suspiciousness, voice re-emergence, medication doubt. A written relapse plan names who to call, which medication to reinstate, and when to present to ED. Akathisia and depression are common relapse mimics — examine before automatic dose increases. [5]
Dual diagnosis principles
Substance use disorders co-occur frequently and worsen course. Integrated treatment beats sequential "fix substance first" models that strand patients. Motivational interviewing, contingency management for stimulants where available, opioid agonist therapy when indicated, and realistic harm reduction sit alongside antipsychotic care. Do not withhold psychosis treatment until mythical perfect abstinence. [5]
Clinical presentation
Prodrome. Months to years of attenuated symptoms, social withdrawal, falling function, mood and sleep change, cannabis escalation. Most clinical high-risk individuals do not convert — do not over-promise prediction. [5]
Positive symptoms. Delusions; hallucinations (auditory most common clinically); formal thought disorder; passivity phenomena. Content is culturally shaped; structure is clinical. [5]
Negative symptoms. Avolition, anhedonia, alogia, affective flattening, asociality. Separate primary from secondary (depression, EPS, understimulation, substances, positive-symptom preoccupation). [5]
Cognitive deficits. Processing speed, working memory, attention, verbal learning, social cognition — often the best predictors of function. [5]
Catatonia and motor signs. Retarded catatonia risks dehydration, VTE, pressure injury and aspiration; excited catatonia risks exhaustion and collapse. [5]
Differential diagnosis
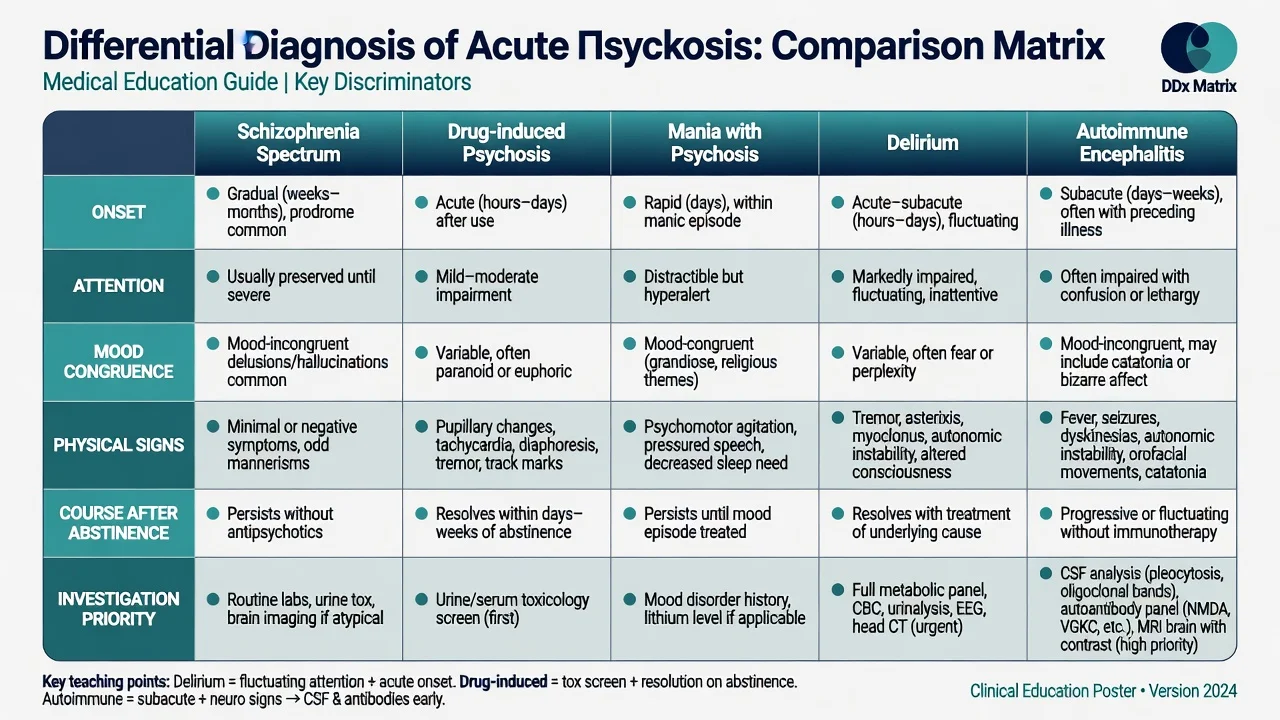
Delirium
- Inattention and fluctuation are core
- Medical illness, drugs, withdrawal
- Visual hallucinations more common than in primary psychosis
- Treat the cause; antipsychotics are cautious adjuncts
Drug-induced psychosis
- Timeline locked to intoxication or withdrawal
- Methamphetamine, high-THC cannabis, synthetics, stimulants
- May resolve with abstinence — or unmask primary illness
- Urine screen supports but never excludes
Affective psychosis
- Mood episode is primary and persistent
- Psychosis often mood-congruent in classic teaching (not absolute)
- Schizoaffective requires psychosis without mood for at least 2 weeks
- Treat mood and psychosis together
Organic / autoimmune
- Fever, seizure, dysautonomia, movement disorder, rapid decline
- NMDAR encephalitis pattern in young adults
- Late-onset first episode, focal neurology, HIV, syphilis, B12, thyroid
- Investigate before chronic labelling
Also keep OCD with poor insight, body dysmorphic disorder, PTSD with dissociative phenomena, autism with atypical beliefs, and personality (schizotypal, paranoid, borderline) on the board. [5]
Clinical and bedside assessment
Document a full Mental State Examination with examples. Record risk explicitly: suicide, self-harm, violence, vulnerability, neglect, absconding, weapons, childcare. [5]
Capacity is decision-specific and time-specific: understanding, retention, weighing, communication, plus an impairment of mind or brain. Involuntary care is last-resort, least-restrictive, statute-bound — quote local Mental Health Act principles, not invented section numbers. [5]
Risk is dynamic. Reassess after command hallucinations, relationship rupture, discharge, substance relapse, akathisia, or diagnostic disclosure. [5]
Investigations
[5]Image and special tests are mandatory when red flags fire: atypical first episode, late onset, focal neurology, seizure, profound cognitive change, immunosuppression, or suspected encephalitis. [5]
Clozapine monitoring is non-negotiable: frequent neutrophil counts early (local registry protocol), myocarditis vigilance in month one, bowel charts, plasma levels, metabolic monitoring, and smoking-status changes that alter CYP1A2 clearance. [5]
Management — resuscitation of the acute crisis
De-escalate verbally; offer oral medication; use intramuscular agents only when needed for safety; monitor airway, respiration, QTc and consciousness; never combine intramuscular olanzapine with a parenteral benzodiazepine; exclude hypoglycaemia and other organic drivers. [5]
Acute dystonia: parenteral anticholinergic per local formulary and airway readiness.
NMS: stop antipsychotic, supportive care, benzodiazepines, specialist adjuncts.
Catatonic emergency: lorazepam challenge; early ECT discussion if malignant or non-responsive. [5]
Management — definitive and stepwise
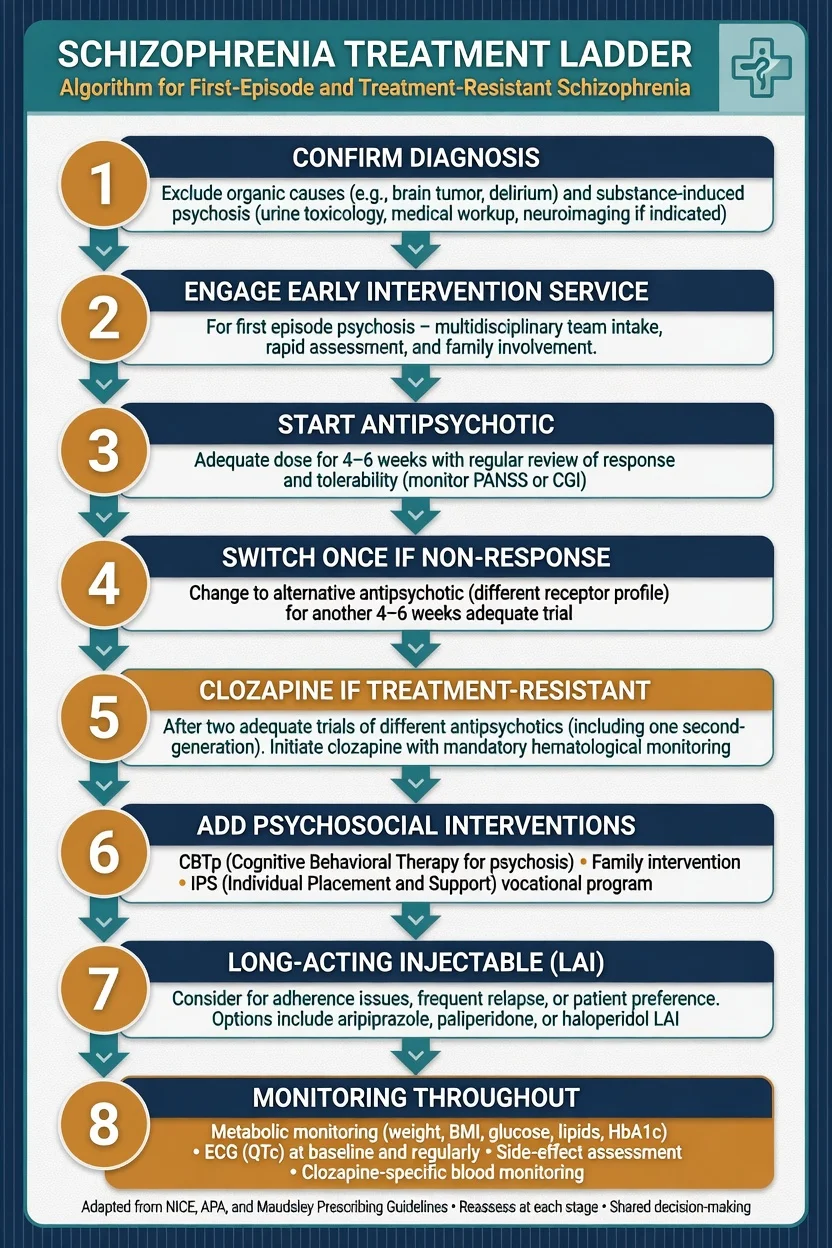
First-episode pathway
- Engage an early intervention service where available.[4][12][14]
- Start an antipsychotic after shared decision-making and baseline work-up.
- Use an adequate dose for an adequate duration (commonly 4–6 weeks with adherence confirmed) before declaring failure.
- Offer CBTp, family intervention and vocational support alongside medication.[19]
- Plan maintenance after remission; unplanned cessation drives relapse.
Landmark trials (exam-fluent)
CATIE (Lieberman et al., NEJM 2005). Chronic US effectiveness RCT of several SGAs and perphenazine. All-cause discontinuation was high. Olanzapine had longer time to discontinuation in some comparisons but more metabolic burden. Perphenazine was not broadly inferior — a challenge to SGA marketing mythology.[1]
CUtLASS 1 (Jones et al., 2006). UK effectiveness study found no quality-of-life advantage for SGAs over FGAs as class strategies in many patients; individualise by side-effect profile.[2]
EUFEST (Kahn et al., 2008). First-episode open RCT: high discontinuation overall; tolerability differences often larger than pure efficacy differences versus high-dose-era haloperidol strategies.[3]
Leucht network meta-analysis (2013). Fifteen antipsychotics ranked for efficacy and tolerability; clozapine retains unique efficacy; others trade efficacy against side-effects.[5][11]
OPUS. Intensive early intervention improved outcomes versus standard care at 1–2 years; some advantages attenuate later — sustained quality care matters.[9][14]
RAISE-ETP / NAVIGATE. Coordinated specialty care superior to usual community care on functional and quality-of-life outcomes over two years in US FEP.[4]
Correll EIS meta-analysis (2018). Early intervention services outperform treatment as usual in early-phase psychosis.[12]
Agent selection anchors
| Domain | Prefer / consider | Caution |
|---|---|---|
| First episode, metabolic concern | Aripiprazole; careful risperidone dosing | Early olanzapine if high metabolic risk |
| Insomnia / agitation with psychosis | Olanzapine; quetiapine | Metabolic cost |
| Non-adherence / revolving relapse | LAI formulations | Know oral-to-LAI overlap rules |
| Treatment resistance | Clozapine | Monitoring infrastructure mandatory |
| High suicide risk in schizophrenia | Clozapine (InterSePT) | Not a substitute for risk management |
Illustrative adult oral ranges (confirm local formulary / product information). Risperidone often 2–6 mg/day; olanzapine 10–20 mg/day; aripiprazole 10–30 mg/day; quetiapine toward 300–800 mg/day in psychosis; amisulpride 400–800 mg/day; prefer low-dose haloperidol strategies over historical high doses. Start low in first episode. Reassess EPS, akathisia, prolactin, weight, glucose and QTc on a schedule.[10]
Long-acting injectables
LAIs reduce covert non-adherence and are associated with fewer relapses in many datasets. Offer after adherence-related relapse, in preference-sensitive FEP pathways, and when the patient chooses fewer daily decisions. Know initiation, loading/overlap, interval and missed-dose rules. [5]
Treatment-resistant schizophrenia and clozapine
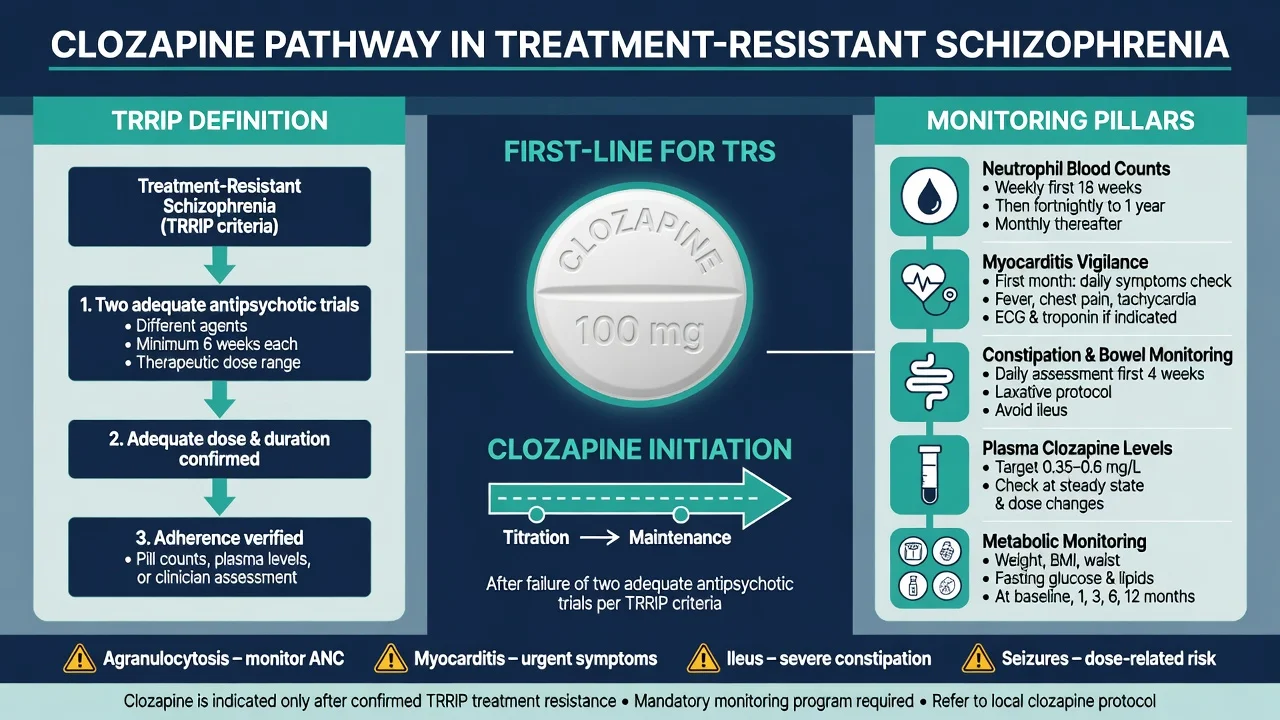
TRRIP (Howes et al., 2017). At least two failed antipsychotic trials of adequate dose and duration with adherence assessed; symptomatic threshold met; pseudo-resistance excluded.[13]
Clozapine is the only antipsychotic with robust superiority in true TRS. Kane established the principle; modern meta-analysis confirms meaningful response rates.[6][18] InterSePT showed clozapine superior to olanzapine for suicidal behaviour in schizophrenia and schizoaffective disorder.[10]
Clozapine practical non-negotiables. Slow titration; smoking induces CYP1A2 (cessation raises levels); plasma levels often discussed around 350 micrograms per litre for response assessment (local units matter); constipation can kill — prevent and ask; myocarditis window early; agranulocytosis risk highest early but never zero; seizures dose-related. Never start without a monitoring system that works on weekends. [5]
Psychosocial care
Family intervention and relapse-prevention packages, CBTp for persistent symptoms, cognitive remediation, and Individual Placement and Support for employment. Medication without psychosocial care is incomplete care.[19]
Specific scenarios
Cannabis. Adolescent high-potency use elevates risk and worsens course — cessation is a core intervention.
Methamphetamine psychosis. May be transient or persistent; reassess after abstinence; do not miss delirium and cardiac toxicity.
Pregnancy. Multidisciplinary planning; avoid abrupt cessation that triggers relapse; specialised reproductive psychiatry input.
Late-onset first episode. Intensify organic work-up. [5]
Complications and pitfalls
[5] [5]Other traps: declaring resistance after two weeks at a token dose; missing non-adherence; ignoring prolactin symptoms; polypharmacy without a clozapine trial; therapeutic nihilism; coercive care without a least-restrictive alternative. [5]
Prognosis and disposition
Better prognosis: female sex, later or acute onset, mood features, good premorbid function, short DUP. Poorer: early insidious onset, primary negative symptoms, cognitive impairment, ongoing cannabis, long DUP. Remission is symptom control; recovery is broader.[15][16]
Disposition: voluntary or involuntary admission, EIS, community team, dual diagnosis, rehabilitation, clozapine clinic, forensic pathways. Discharge without named follow-up, crisis plan and family communication fails the exam.[12]
Special populations
Adolescents need developmental and family work. Older adults need EPS/anticholinergic caution and organic vigilance. Intellectual disability risks diagnostic overshadowing. FRANZCP candidates must formulate with culture, racism, migration and spirituality without dismissing treatable psychosis.[4][17]
Evidence, guidelines and regional differences
ANZ / FRANZCP. Early intervention is standard where services exist. Physical health monitoring is a quality marker. Clozapine is underused relative to need. Mental Health Acts differ by jurisdiction — learn principles for your rostered state/territory or New Zealand setting.[12][18]
Controversies. Maintenance duration after a single episode; earlier clozapine; cannabis policy and youth risk; balancing long-term dopamine blockade with recovery goals.[8][13]
Formulation for the viva
A defensible biopsychosocial formulation for a first-episode presentation answers four questions: what is happening (syndrome and criteria), why this person (vulnerability: family history, neurodevelopmental markers, premorbid function), why now (cannabis escalation, stress, sleep loss, migration, trauma anniversary), and what maintains the problem (non-adherence, ongoing substance use, family high expressed emotion, untreated depression, akathisia, isolation). Examiners reward formulations that change management — for example, prioritising cannabis cessation and family work rather than only dose escalation.[15][19]
Antipsychotic adverse-effect map (exam matching)
| Adverse effect | Mechanism / pathway | Higher-risk agents (relative) | Management anchors |
|---|---|---|---|
| Acute dystonia | Nigrostriatal D2 blockade | High-potency FGAs, risperidone | Parenteral anticholinergic; review dose |
| Parkinsonism | Nigrostriatal D2 blockade | High-potency FGAs | Reduce dose, switch, anticholinergic carefully |
| Akathisia | Complex; often early | Aripiprazole, high-potency agents | Do not escalate antipsychotic; reduce/switch; propranolol/benzo per local practice |
| Tardive dyskinesia | Chronic D2 blockade plasticity | Cumulative FGA risk; can occur with SGAs | Prevention; VMAT2 inhibitors in specialist hands |
| Weight gain / metabolic | Histamine, 5HT2C, lifestyle | Olanzapine, clozapine | Baseline and serial metabolic monitoring; switch; metformin protocols where used |
| Hyperprolactinaemia | Tuberoinfundibular D2 blockade | Risperidone, paliperidone, FGAs | Switch to partial agonist or lower-risk agent |
| QTc prolongation | Cardiac ion channels | Some FGAs; ziprasidone; high-dose IV | Baseline ECG; electrolytes; avoid combinations |
| Sedation | H1 blockade | Quetiapine, olanzapine, clozapine | Timing, dose, fall risk |
| Agranulocytosis | Immune idiosyncratic | Clozapine | Registry blood monitoring — stop if thresholds breached |
| Myocarditis | Immune / early clozapine | Clozapine month 1 | Stop, investigate, do not rechallenge lightly |
| Constipation / ileus | Anticholinergic + other | Clozapine | Proactive laxatives; emergency abdominal pathway |
| Seizures | Dose-related threshold | Clozapine | Slow titration; levels; consider valproate specialist advice |
Pathway physiology underpins this map (mesolimbic therapeutic target; nigrostriatal EPS; tuberoinfundibular prolactin).[5][7]
Long-term care and recovery
Recovery-oriented care is not anti-medication rhetoric. It means measuring outcomes that matter: relationships, work or study, independent living, physical health, and hope — alongside positive symptom control. Supported employment (IPS) outperforms stepwise "train then place" models for many people with schizophrenia. Peer support and lived-experience workers improve engagement when integrated rather than tokenistic.[12][19]
Maintenance after remission. After a first episode, many guidelines support continuation of antipsychotic treatment for at least 1–2 years after remission, with individualised longer continuation after multiple episodes. Any deprescribing attempt needs a relapse plan, slow taper, family involvement, and rapid reinstatement criteria. Observational data linking antipsychotic continuation to lower mortality should be discussed alongside metabolic risk mitigation — not as a false choice between mind and body.[8]
Critical appraisal angles (FRANZCP CAP / MRCPsych Paper B)
When a CAP paper uses a schizophrenia trial, expect questions on: [5]
- Effectiveness versus efficacy — CATIE and CUtLASS were effectiveness designs with high discontinuation; results generalise better to real-world practice but interpret "all-cause discontinuation" carefully.
- Open-label bias — EUFEST was open; knowing allocation can influence discontinuation and some ratings.
- Network meta-analysis assumptions — Leucht 2013 connects trials through common comparators; ranking is probabilistic, not a league table for every patient.
- Surrogate versus hard outcomes — PANSS change is not identical to recovery, employment, or mortality.
- Industry and sponsorship — declare and weigh.
- Missing data and LOCF — older trials often handled dropouts in ways that inflate apparent efficacy. [5]
A fellowship candidate who can critique CATIE in two minutes scores higher than one who only recites "olanzapine won."[1][2][3][5]
Legal and ethical themes (jurisdiction-labelled)
Involuntary treatment for psychosis is examined as principle, not as a memorised statute quiz across all states: [5]
- Presumption of capacity and maximising voluntary engagement.
- Decision-specific capacity assessment documented contemporaneously.
- Least restrictive alternative consistent with safety.
- Statutory criteria for detention (risk of harm to self/others and/or deterioration, plus mental illness definitions that vary by Act).
- Rights to information, advocacy, review tribunals, and second opinions.
- Family involvement balanced against privacy. [5]
State the jurisdiction you are working in. Do not invent section numbers for NSW when sitting a Victorian scenario. Risk and suicide epidemiology underpin the safety half of this calculus.[16][17]
Exam pearls
Clozapine non-negotiables
CLOZAPINE
Neutrophil monitoring on protocol — no bloods, no drug
Plasma levels guide efficacy and toxicity; watch smoking changes
Constipation and ileus kill — prevent and ask
First-month fever, tachycardia, chest pain, CRP/troponin
TRRIP: two adequate failed antipsychotics with adherence
Metabolic, seizure threshold, hypersalivation plans
Suicide advantage in high-risk schizophrenia
Only start if the service can monitor reliably
Still the only superior agent in true TRS
Red flags
References
- [1]Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia N Engl J Med, 2005.PMID 16172203
- [2]Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of the effect on Quality of Life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1) Arch Gen Psychiatry, 2006.PMID 17015810
- [3]Kahn RS, Fleischhacker WW, Boter H, et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial Lancet, 2008.PMID 18374841
- [4]Kane JM, Robinson DG, Schooler NR, et al. Comprehensive Versus Usual Community Care for First-Episode Psychosis: 2-Year Outcomes From the NIMH RAISE Early Treatment Program Am J Psychiatry, 2016.PMID 26481174
- [5]Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis Lancet, 2013.PMID 23810019
- [6]Kane JM, Honigfeld G, Singer J, et al. Clozapine in treatment-resistant schizophrenics Psychopharmacol Bull, 1988.PMID 3290950
- [7]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [8]Tiihonen J, Lönnqvist J, Wahlbeck K, et al. 11-year follow-up of mortality in patients with schizophrenia: a population-based cohort study (FIN11 study) Lancet, 2009.PMID 19595447
- [9]Bertelsen M, Jeppesen P, Petersen L, et al. Five-year follow-up of a randomized multicenter trial of intensive early intervention vs standard treatment for patients with a first episode of psychotic illness: the OPUS trial Arch Gen Psychiatry, 2008.PMID 18606949
- [10]Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) Arch Gen Psychiatry, 2003.PMID 12511175
- [11]Leucht S, Leucht C, Huhn M, et al. Sixty Years of Placebo-Controlled Antipsychotic Drug Trials in Acute Schizophrenia: Systematic Review, Bayesian Meta-Analysis, and Meta-Regression of Efficacy Predictors Am J Psychiatry, 2017.PMID 28541090
- [12]Correll CU, Galling B, Pawar A, et al. Comparison of Early Intervention Services vs Treatment as Usual for Early-Phase Psychosis: A Systematic Review, Meta-analysis, and Meta-regression JAMA Psychiatry, 2018.PMID 29800949
- [13]Howes OD, McCutcheon R, Agid O, et al. Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology Am J Psychiatry, 2017.PMID 27919182
- [14]Petersen L, Nordentoft M, Jeppesen P, et al. Improving 1-year outcome in first-episode psychosis: OPUS trial Br J Psychiatry Suppl, 2005.PMID 16055817
- [15]Marshall M, Lewis S, Lockwood A, et al. Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review Arch Gen Psychiatry, 2005.PMID 16143729
- [16]Palmer BA, Pankratz VS, Bostwick JM The lifetime risk of suicide in schizophrenia: a reexamination Arch Gen Psychiatry, 2005.PMID 15753237
- [17]Saha S, Chant D, McGrath J A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry, 2007.PMID 17909124
- [18]Siskind D, Siskind V, Kisely S Clozapine Response Rates among People with Treatment-Resistant Schizophrenia: Data from a Systematic Review and Meta-Analysis Can J Psychiatry, 2017.PMID 28655284
- [19]Bighelli I, Rodolico A, García-Mieres H, et al. Psychosocial and psychological interventions for relapse prevention in schizophrenia: a systematic review and network meta-analysis Lancet Psychiatry, 2021.PMID 34653393
- [20]Davis JM, Chen N, Glick ID A meta-analysis of the efficacy of second-generation antipsychotics Arch Gen Psychiatry, 2003.PMID 12796218