Psych · General adult psychiatry — psychotic disorders
Schizophreniform and brief psychotic disorder
Also known as Brief psychotic disorder · Schizophreniform disorder · Acute and transient psychotic disorder · ATPD · Acute polymorphic psychosis · Brief reactive psychosis · Nonaffective acute remitting psychosis · NARP
Exam-exhaustive fellowship reference on duration-defined nonaffective psychoses — DSM-5-TR brief psychotic disorder (1 day to under 1 month) and schizophreniform disorder (1 to under 6 months); ICD-11 ATPD; good prognostic features; diagnostic instability; FEP-style acute care and post-remission maintenance. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
These two diagnoses exist because time is part of the nosology. Fellowship exams fail candidates who invent lifetime schizophrenia on day three of voices, who withhold treatment because “it might be brief,” or who cannot recite the good prognostic features of schizophreniform disorder and the 1 day / 1 month / 6 month thresholds that separate BPD, schizophreniform, and schizophrenia.[8][16][2]
Overview and definition
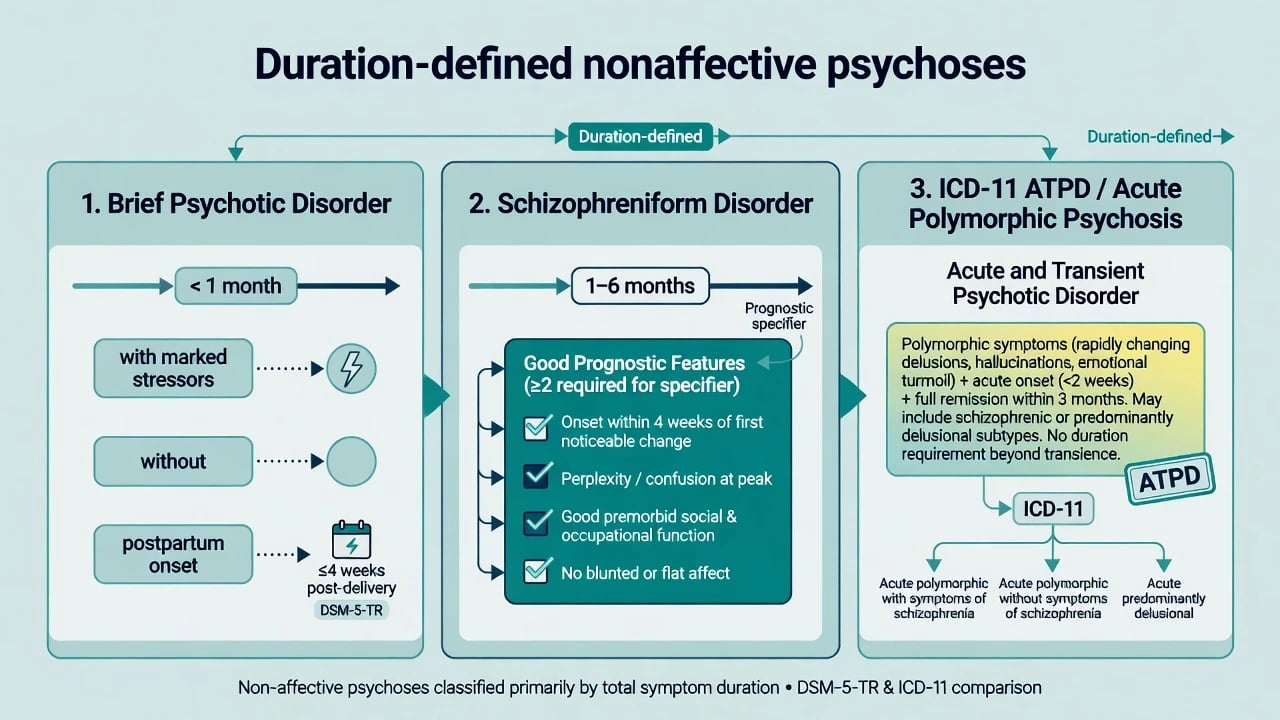
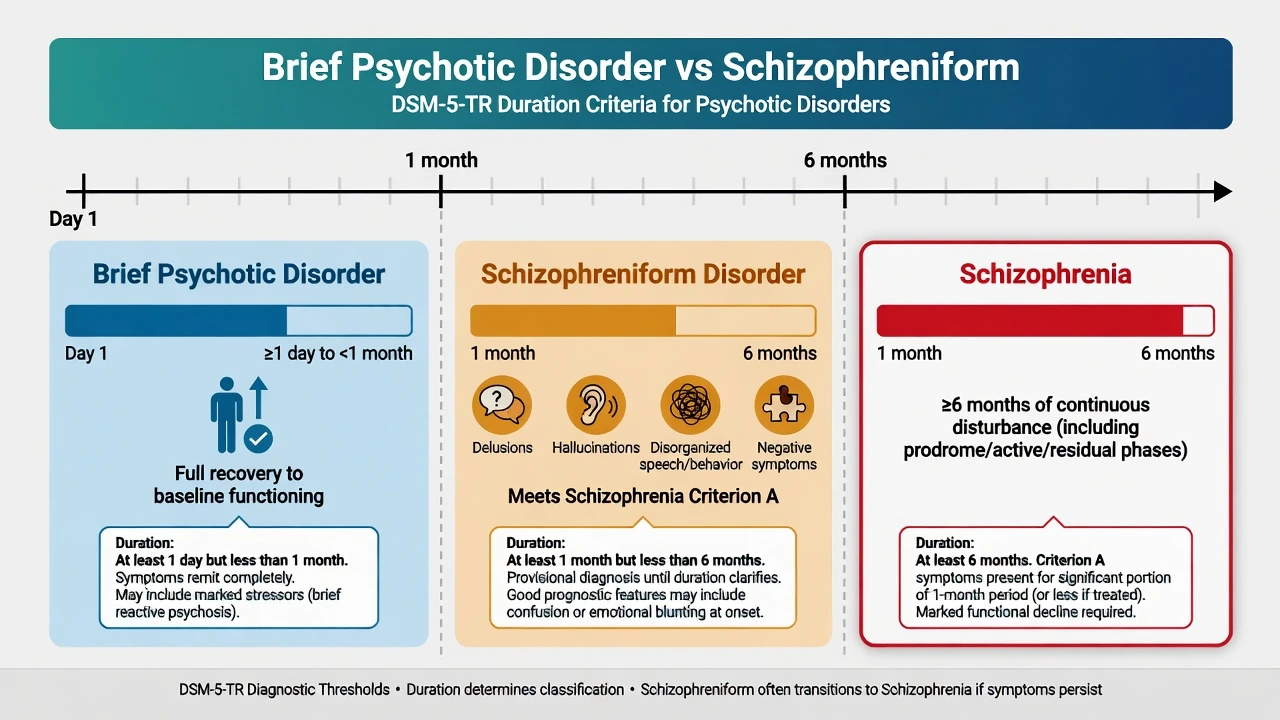
Brief psychotic disorder (BPD) requires the sudden presence of one or more of: delusions, hallucinations, disorganised speech, or grossly disorganised or catatonic behaviour, lasting at least 1 day but less than 1 month, with eventual full return to the premorbid level of functioning. Mood, substance, and medical causes must be excluded as primary explanations. Specifiers capture clinical colour: with marked stressor(s) (historically “brief reactive psychosis”), without marked stressor(s), and with postpartum onset.[8][7][16]
Schizophreniform disorder requires a schizophrenia-like Criterion A symptom pattern (two or more core psychotic domains, with at least one of delusions, hallucinations, or disorganised speech in standard DSM framing) lasting at least 1 month but less than 6 months. If the episode is ongoing and has not yet reached 6 months, the diagnosis is often labelled provisional. If symptoms later cross 6 months (with functional criteria as for schizophrenia), the diagnosis is revised to schizophrenia.[16][2]
Why the constructs exist. They encode the clinical reality that not every first nonaffective psychosis is lifelong schizophrenia, while still forcing clinicians to treat the acute syndrome seriously and to follow the longitudinal clock.[8][1]
Classification and duration map
| Construct | Duration (DSM-5-TR operational teaching) | Defining recovery / course note |
|---|---|---|
| Brief psychotic disorder | ≥1 day and less than 1 month | Full return to premorbid function expected by definition |
| Schizophreniform disorder | ≥1 month and less than 6 months | May recover fully or convert; provisional if ongoing |
| Schizophrenia | ≥6 months (including prodrome/active/residual as operationalised) | Persistent multi-domain illness pattern |
Good prognostic features (schizophreniform) — recite for viva
Specify with good prognostic features when at least two of the following are present (standard DSM teaching list): (1) onset of prominent psychotic symptoms within 4 weeks of the first noticeable change in usual behaviour or functioning; (2) confusion or perplexity at the height of the psychotic episode; (3) good premorbid social and occupational functioning; (4) absence of blunted or flat affect. Without these, specify without good prognostic features. Good features raise hope for recovery but do not justify withholding acute treatment.[2][8][16]
ICD-11 ATPD (regional/manual awareness)
ICD-11 groups many short-lived nonaffective psychoses under acute and transient psychotic disorders (ATPD), including acute polymorphic presentations that may shift day to day. Do not force-fit identical day counts across manuals in a stem that specifies ICD; state which system you are using and map conceptual overlap with BPD/schizophreniform rather than inventing a perfect crosswalk.[4][5][8]
Epidemiology and risk
Numbers and framing candidates must own
Strictly defined brief and schizophreniform labels are less common than schizophrenia in many high-income services, but acute remitting nonaffective psychoses are enriched in some sociocultural settings — Susser and Wanderling’s classic epidemiology of nonaffective acute remitting psychosis (NARP) remains a viva staple for “developing country / acute remitting” stems.[1][17]
Population studies of psychotic disorders show a broader psychosis spectrum than clinic schizophrenia counts alone suggest.[17] Even “transient” ATPD is not harmless: register data show excess mortality compared with population expectations and warrant physical-health and suicide attention.[6]
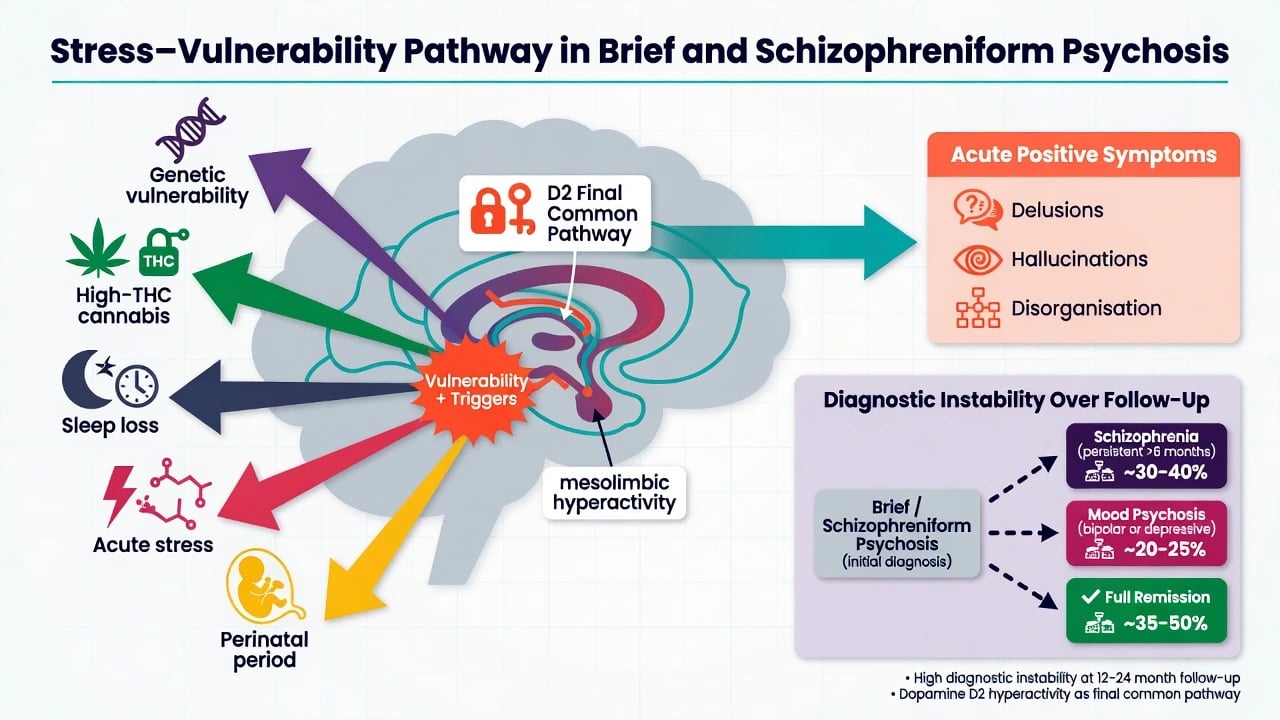
Risk amplifiers. High-potency cannabis contributes to variation in psychotic disorder incidence; continued cannabis after onset worsens relapse trajectories in early psychosis cohorts.[19] Acute stress, sleep loss, migration, trauma, and the perinatal window colour presentation and specifier choice without automatically proving a purely reactive illness.[8][7]
Pathophysiology and mechanisms
There is no unique “brief-psychosis-only circuit.” Viva-safe synthesis: (1) stress–vulnerability — acute stress may unmask latent psychosis liability; marked stressors specify BPD but do not prove pure psychogenesis; (2) dopamine final common pathway language explains positive symptoms and why D2-modulating antipsychotics often reduce acute intensity; (3) heterogeneity — diagnostic shifts over years show mixed destinations (schizophrenia, affective psychosis, or durable remission), so treat the syndrome while keeping the differential open; (4) substance and sleep as common accelerants, especially high-THC cannabis in first presentations.[8][1][15][3][5][7][19]
Clinical presentation
Onset. BPD is classically abrupt (hours to days). Schizophreniform may be abrupt or subacute over weeks. Polymorphic ATPD presentations can show rapidly shifting delusions, emotional turmoil, and perplexity — do not confuse this with delirium until you have checked attention and medical status.[4][8]
MSE language. At peak: delusions and/or hallucinations; disorganised speech or behaviour; possible catatonia; affect may be perplexed, fearful, or incongruent; sensorium should be clear if this is primary functional psychosis. Confusion/perplexity is a good-prognostic cue in schizophreniform teaching, not a free pass for unassessed delirium.[2][16]
Recovery signature in BPD. By definition, functioning returns to the premorbid baseline within a month of onset of the episode — residual negative syndrome or progressive functional collapse should make you re-examine the label and trajectory.[7][8]
Postpartum onset. Brief psychotic disorder can be specified with postpartum onset; still dual-track with bipolar/postpartum psychosis pathways and mother–infant safety as non-negotiable priorities.[10]
Differential diagnosis
| Differential | Points toward this | Points toward BPD / schizophreniform |
|---|---|---|
| Schizophrenia | Duration ≥6 months; progressive multi-domain course | Clock still under 6 months; recovery possible |
| Mood disorder with psychosis | Full mania/MDD with psychosis confined to mood | Psychosis without full syndromal mood episode |
| Substance-induced psychosis | Clear intoxication/withdrawal timeline | Persists beyond substance window |
| Medical / autoimmune / delirium | Fluctuating attention, fever, neurology | Clear sensorium after work-up |
| Attenuated / CHR | Subthreshold intensity/insight | Frank Criterion A-level psychosis |
| Cultural/dissociative phenomena | Culturally sanctioned, limited disability | Distress, disability, loss of reality testing |
Diagnostic instability is the rule, not the exception. First-admission schizophreniform cases frequently reclassify over follow-up; decade-scale diagnostic shifts after first psychosis admission are well documented; ATPD stability is limited over the long term; brief psychotic episode outcome syntheses show mixed remitting and progressing courses.[2][3][5][7]
Clinical and bedside assessment
Structure as clock + risk + organic screen + substances + collateral + capacity.[10][11]
- Date the onset of frank psychosis and of first functional change — duration decides the DSM label.
- Map stressors, perinatal status, sleep, cannabis/stimulants, trauma, migration, and family history of psychosis/bipolar.
- Risk: suicide, violence, absconding, vulnerability, child/infant protection.
- Capacity and least-restrictive legal pathway under local statute (do not invent foreign section numbers).
- Collateral — families often date onset better than the patient.
- Explicitly checklist good prognostic features when schizophreniform is considered.[2][10]
Investigations
Before antipsychotics, complete a physical-health baseline aligned with schizophrenia-spectrum standards.[10][11]
- Bloods: FBC, U&E/eGFR, LFT, fasting glucose or HbA1c, lipids; TFT when indicated
- ECG: QTc and cardiac risk before many antipsychotics
- BMI/BP/waist; pregnancy test when relevant
- Toxicology with timeline interpretation — negative does not exclude recent use
- CT/MRI, EEG, autoimmune work-up when atypical, late-onset, focal, seizure-associated, or cognitively collapsing
- Do not delay acute containment for non-urgent imaging when organic yield is otherwise low
Management — acute and emergency
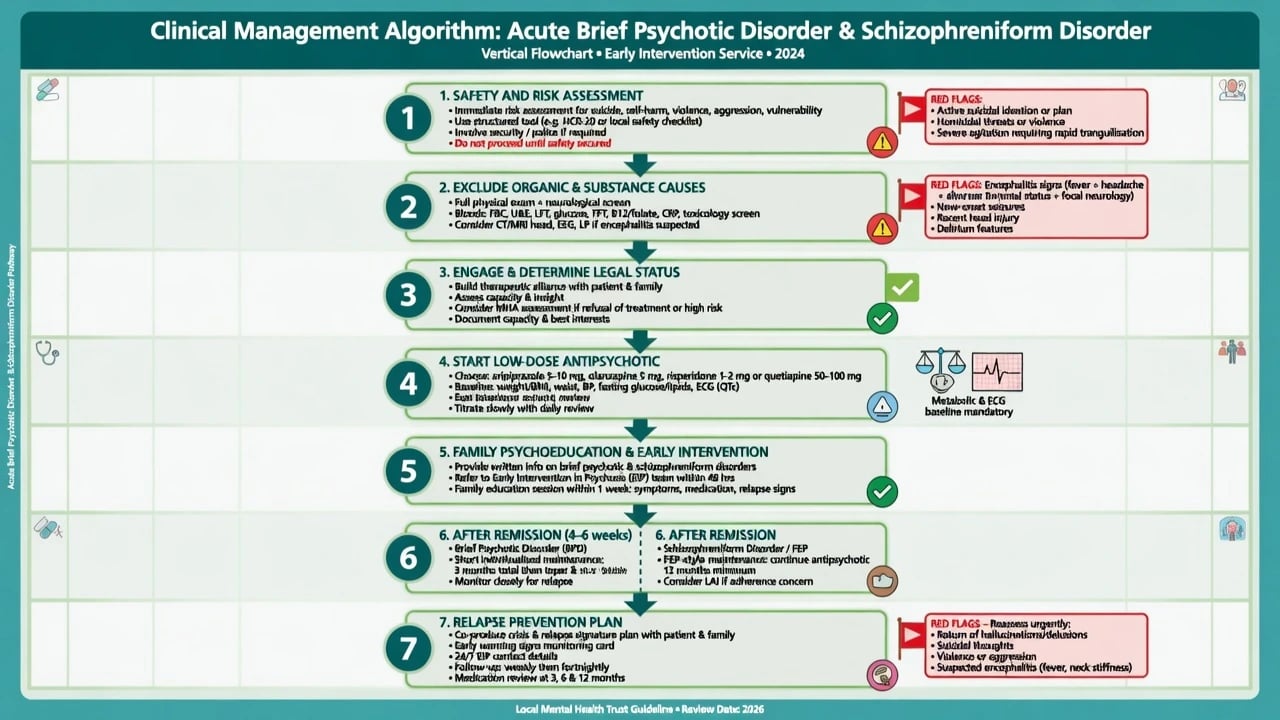
Setting. Use the least-restrictive environment that is still safe. Admit when risk, diagnostic uncertainty with organic concern, or failed community containment demands it.[10]
Agitation. De-escalate; oral before IM when safe; follow local rapid-tranquillisation protocol.[10][11]
Medical mislabel. Fever, fluctuating attention, new neurology, seizures, dysautonomia — rethink delirium/encephalitis rather than “non-compliant brief psychosis.” After antipsychotics, watch for NMS and severe EPS.[10]
Management — definitive and stepwise
Acute antipsychotic treatment (FEP principles)
These diagnoses are managed within early psychosis pathways, not with undergraduate “wait and see” romanticism. Multi-element early intervention services outperform treatment-as-usual for early-phase psychosis on multiple outcomes.[12][10]
EUFEST enrolled first-episode schizophrenia and schizophreniform disorder and supports pragmatic antipsychotic choice with effectiveness and tolerability trade-offs rather than a single perfect molecule.[9] International consensus dosing and schizophrenia-spectrum guidelines inform start-low, go-slow first-episode practice.[18][11]
Illustrative adult oral FEP frameworks (individualise to product information, age, sex, comorbidity, prior response) — dose ranges informed by EUFEST-era practice, consensus dosing, and RANZCP/APA monitoring standards:[9][18][10][11]
| Agent | Typical adult oral start / early target | Key monitoring |
|---|---|---|
| Risperidone | Often 1–2 mg daily; titrate carefully toward 2–4+ mg | Prolactin, EPS |
| Aripiprazole | Often 5–10 mg daily; common early targets 10–15 mg | Akathisia |
| Olanzapine | Often 5–10 mg nightly; titrate toward 10–20 mg if needed | Weight, glucose, lipids |
| Amisulpride / others | Local formulary and experience | Endocrine, EPS, QTc as relevant |
| Dose frameworks above are illustrative first-episode ranges — always individualise and document shared decision-making.[9][18][10][11] |
Trial adequacy. Allow a fair window at a therapeutic dose with adherence checked (often on the order of weeks) before declaring failure; avoid high-dose polypharmacy “loading” that drives EPS and metabolic harm in first episode.[9][11]
Psychosocial package
Multi-element psychosocial care includes psychoeducation for patient and family, family intervention drawn from schizophrenia-spectrum evidence, CBTp access when engageable, a substance plan (especially cannabis cessation support), and vocational or education preservation as recovery goals.[10][12]
After remission — maintenance honesty
BPD that fully remits still needs a relapse prevention plan (sleep, substances, early warning signs, rapid re-access). Medication duration after a single fully remitted brief episode is individualised; some clinicians trial careful taper after short consolidation if risk is low and supports are strong — but FEP discontinuation literature shows high recurrence risk when antipsychotics stop after first-episode response in schizophrenia-spectrum samples, so do not oversell “one week of tablets then cure.”[13][14][20][7]
Schizophreniform without durable long remission should be treated closer to FEP/schizophrenia-spectrum maintenance until follow-up proves otherwise, because conversion risk is substantial and diagnostic shifts are common.[2][3][13]
Relapse-prevention meta-analysis in schizophrenia shows clear benefit of continued antipsychotic over placebo for preventing relapse — transferable caution when the working diagnosis sits on the spectrum and recovery is incomplete.[20]
Regional guidance
ANZ (RANZCP). Apply schizophrenia and related disorders guideline principles: comprehensive assessment, physical health, recovery orientation, least-restrictive care, early intervention, and antipsychotic use with metabolic monitoring — adapted to duration-defined labels that may still evolve.[10]
USA (APA). Schizophrenia practice guideline frameworks for antipsychotic choice, shared decision-making, and monitoring transfer when antipsychotics are used for schizophreniform/related presentations.[11]
UK/other. NICE early psychosis pathways inform CBTp, family work, and physical health checks. Always localise legal statutes. Core FEP standards still apply to BPD and schizophreniform presentations.[10][12]
Subtypes and special scenarios
BPD + marked stressor
- Brief reactive colour
- Still exclude organic/substance
- Do not assume pure stress cure
- Safety plan through recovery
BPD without stressor
- Higher suspicion for evolving spectrum illness
- Closer follow-up after remission
- Cannabis and sleep still matter
- Avoid premature lifelong label
Schizophreniform + good features
- Recite four good features
- Hopeful but not treatment-free
- Watch the 6-month clock
- Reassess diagnosis longitudinally
Postpartum-onset BPD
- Mother–infant safety first
- Dual-track bipolar postpartum psychosis
- Perinatal liaison
- Medication and lactation decisions localise
Complications and pitfalls
- Premature lifelong schizophrenia label before duration thresholds — stigma and career damage without nosologic necessity.[16][8]
- Under-treatment because “it is only brief” — suicide and violence still apply; ATPD mortality excess is a warning.[6][10]
- Missing organic encephalitis or substance-driven psychosis.[10]
- Abrupt antipsychotic stop after first good week without relapse plan.[13][14]
- High-dose rapid polypharmacy causing EPS/metabolic/NMS harm in first episode.[9][11]
- Ignoring diagnostic instability — failing to revise the label when the course declares itself.[3][5][7]
Prognosis and disposition
BPD remits by definition within a month of episode onset, but recurrence and later diagnostic evolution remain possible; outcome meta-analysis of brief psychotic episodes shows clinically important heterogeneity.[7]
Schizophreniform is a high-yield gateway diagnosis: many first-admission cases later meet schizophrenia or other enduring diagnoses; Naz and colleagues highlighted discriminators and the provisional nature of the label.[2] Decade-scale first-admission cohorts show substantial diagnostic shifts across the psychosis spectrum.[3]
ATPD shows limited long-term diagnostic stability in register follow-up; incidence studies also document reclassification over time.[4][5]
Disposition. Admit for high risk, severe behavioural disturbance, organic uncertainty, or failed community containment. Step down into early-intervention intensity with clear crisis contacts. Relapse cues: sleep collapse, substance restart, rising suspiciousness, treatment cessation, acute stress.[10][12][13]
Special populations
- Youth / FEP services: preferred pathway for first frank psychosis regardless of provisional duration label.[12][10]
- Perinatal: postpartum-onset specifier; infant safeguarding; mood-psychosis dual track.[10]
- Older adults: first brief psychosis demands intensified organic work-up.[10]
- Cultural formulation: polymorphic/possession-like content needs cultural humility plus risk and disability assessment.[8]
- Intellectual disability / autism: separate baseline oddity from new frank psychosis with collateral and developmental history.[10]
Exam pearls
Key takeaways
- Time thresholds separate BPD, schizophreniform, and schizophrenia — learn the 1-day / 1-month / 6-month spine cold.[16][8]
- Good prognostic features are examinable checklists; they modify hope, not the need for acute treatment.[2]
- Manage both as early psychosis: organic exclusion, risk, low-dose antipsychotic, family work, substance care.[10][12][9]
- Stability is limited — many cases convert; ATPD and schizophreniform cohorts reclassify over years.[2][3][5][7]
- After remission, plan relapse prevention with honest use of FEP discontinuation evidence; do not promise permanent cure from a short tablet course.[13][14][20]
References
- [1]Susser E, Wanderling J Epidemiology of nonaffective acute remitting psychosis vs schizophrenia. Sex and sociocultural setting Am J Psychiatry, 1994.PMID 8161289
- [2]Naz B, Bromet EJ, Mojtabai R Distinguishing between first-admission schizophreniform disorder and schizophrenia Schizophr Res, 2003.PMID 12765743
- [3]Bromet EJ, Kotov R, Fochtmann LJ, et al. Diagnostic shifts during the decade following first admission for psychosis Am J Psychiatry, 2011.PMID 21676994
- [4]Castagnini A, Bertelsen A, Berrios GE Incidence and diagnostic stability of ICD-10 acute and transient psychotic disorders Compr Psychiatry, 2008.PMID 18396184
- [5]Castagnini A, Foldager L, Bertelsen A Long-term stability of acute and transient psychotic disorders Eur Arch Psychiatry Clin Neurosci, 2013.PMID 23028179
- [6]Castagnini A, Foldager L, Bertelsen A Excess mortality of acute and transient psychotic disorders: comparison with bipolar affective disorder and schizophrenia Acta Psychiatr Scand, 2013.PMID 23331302
- [7]Provenzani U, Salazar de Pablo G, Arribas M, et al. Clinical outcomes in brief psychotic episodes: a systematic review and meta-analysis Epidemiol Psychiatr Sci, 2021.PMID 35698876
- [8]Nugent KL, Paksarian D, Mojtabai R Nonaffective acute psychoses: uncertainties on the way to DSM-V and ICD-11 Curr Psychiatry Rep, 2011.PMID 21344285
- [9]Kahn RS, Fleischhacker WW, Boter H, et al. Effectiveness of antipsychotic drugs in first-episode schizophrenia and schizophreniform disorder: an open randomised clinical trial Lancet, 2008.PMID 18374841
- [10]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [11]Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Am J Psychiatry, 2020.PMID 32867516
- [12]Correll CU, Galling B, Pawar A, et al. Comparison of Early Intervention Services vs Treatment as Usual for Early-Phase Psychosis: A Systematic Review, Meta-analysis, and Meta-regression JAMA Psychiatry, 2018.PMID 29800949
- [13]Zipursky RB, Menezes NM, Streiner DL Risk of symptom recurrence with medication discontinuation in first-episode psychosis: a systematic review Schizophr Res, 2014.PMID 23972821
- [14]Robinson D, Woerner MG, Alvir JM, et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder Arch Gen Psychiatry, 1999.PMID 10078501
- [15]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [16]Tandon R, Gaebel W, Barch DM, et al. Definition and description of schizophrenia in the DSM-5 Schizophr Res, 2013.PMID 23800613
- [17]Perälä J, Suvisaari J, Saarni SI, et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population Arch Gen Psychiatry, 2007.PMID 17199051
- [18]Gardner DM, Murphy AL, O'Donnell H, et al. International consensus study of antipsychotic dosing Am J Psychiatry, 2010.PMID 20360319
- [19]Di Forti M, Quattrone D, Freeman TP, et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study Lancet Psychiatry, 2019.PMID 30902669
- [20]Leucht S, Tardy M, Komossa K, et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta-analysis Lancet, 2012.PMID 22560607