Psych · General adult psychiatry — personality disorders
Schizotypal personality disorder
Also known as STPD · Schizotypal PD · Schizotypal disorder · Cluster A personality disorder · Schizophrenia-spectrum personality
Exam-exhaustive fellowship reference on schizotypal personality disorder — DSM-5-TR criteria and ICD-11 severity/trait framing; schizophrenia-spectrum adjacency and conversion risk; epidemiology; mechanisms; differentials versus schizophrenia, ASD, schizoid and paranoid PD; alliance-first psychosocial care; limited low-dose antipsychotic evidence; comorbidity treatment. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Schizotypal personality disorder (STPD) is a high-yield Cluster A and schizophrenia-spectrum interface topic. Examiners test operational criteria, discrimination from frank psychosis and autism spectrum disorder, conversion risk without fatalism, and whether you can build an alliance with a wary, eccentric patient without therapeutic nihilism or unreviewed antipsychotics.[1][2][12]
Overview and definition
STPD describes an enduring pattern of acute discomfort with close relationships, reduced capacity for close relationships, cognitive or perceptual distortions, and eccentricities of behaviour, beginning by early adulthood and present across contexts, causing distress or impairment. It is not a synonym for “weird,” and it is not interchangeable with schizophrenia — reality testing is largely intact outside brief stress-related micropsychotic phenomena.[1][2]
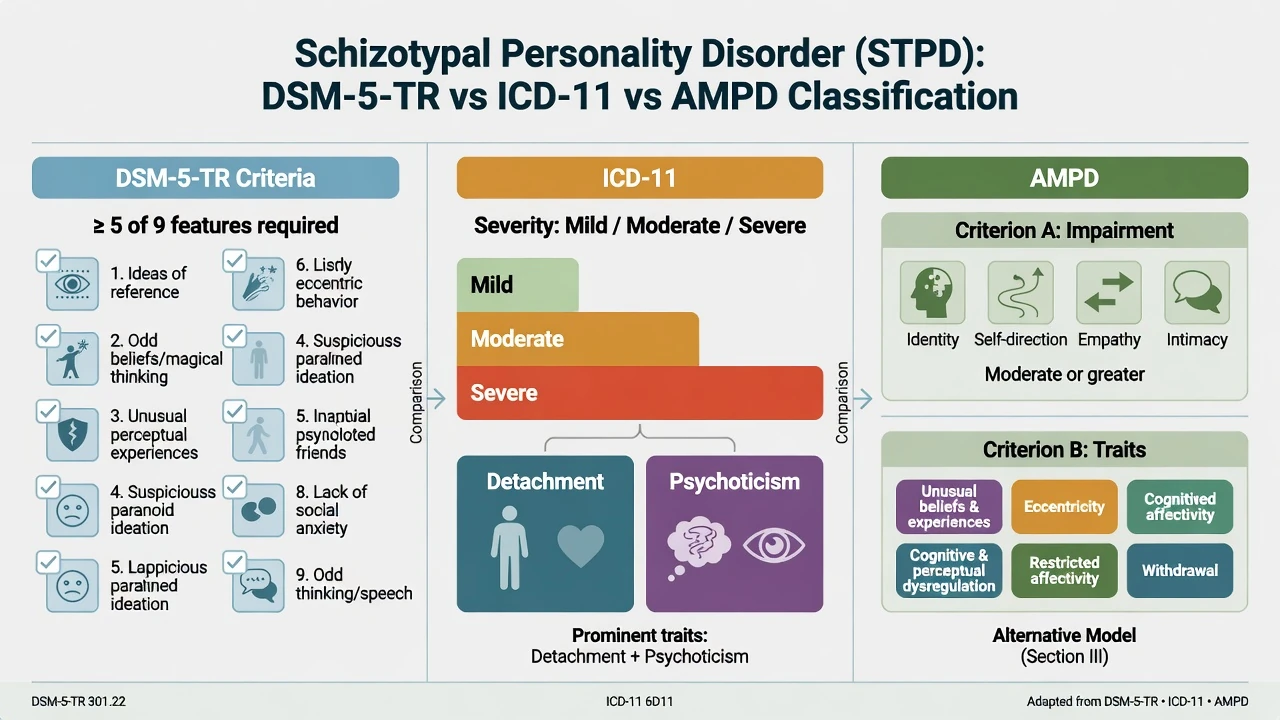
DSM-5-TR categorical diagnosis (exam-critical). After general personality disorder criteria are met, STPD requires a pervasive pattern indicated by five or more of nine features: ideas of reference (excluding delusions of reference); odd beliefs or magical thinking that influence behaviour and are inconsistent with subcultural norms; unusual perceptual experiences including bodily illusions; odd thinking and speech (vague, circumstantial, metaphorical, over-elaborate, or stereotyped); suspiciousness or paranoid ideation; inappropriate or constricted affect; behaviour or appearance that is odd, eccentric, or peculiar; lack of close friends or confidants other than first-degree relatives; and excessive social anxiety that does not diminish with familiarity and tends to be associated with paranoid fears rather than negative judgments about self.[1][2]
ICD-11 and spectrum framing. Personality dysfunction is graded by severity (mild, moderate, severe) with trait domain qualifiers — features of STPD often map onto detachment and psychoticism-related traits. Some teaching systems also discuss ICD “schizotypal disorder” as a schizophrenia-spectrum construct rather than a pure personality category. Fellowship answers must name which manual is in use and that ICD-11 is severity-first, whereas classic MCQ stems still use DSM’s ≥5 of 9 rule.[1][13]
Classification and nosology
DSM-5-TR STPD
- ≥5 of 9 cognitive-perceptual, interpersonal, disorganised features
- General PD criteria required
- Reality testing largely intact
- Cluster A odd/eccentric teaching box
ICD-11 PD framing
- Severity first: mild / moderate / severe
- Trait domains (detachment, psychoticism-related features)
- Dimensional formulation language for stepped care
- Named patterns optional depending on local teaching
AMPD (DSM Section III)
- Criterion A: self and interpersonal impairment
- Criterion B: psychoticism + detachment often central
- Useful for formulation stations
- Avoid trait word-salad without impairment
Schizophrenia spectrum adjacency
- Shared vulnerability signals in families and research
- Not automatic progression to schizophrenia
- Monitor functional decline and conviction
- Frank psychosis leaves the PD-only lane
STPD versus schizophrenia — the viva trap
Schizophrenia requires frank psychotic symptoms (delusions, hallucinations, disorganisation), duration and functional thresholds, and often progressive deterioration. STPD shows trait-level oddness with largely preserved reality testing and better baseline function. A subset of people with schizotypal disorder or high schizotypy transition toward psychosis — probabilistic, never a reason to withhold care or to over-treat eccentricity with lifelong high-dose antipsychotics.[1][2][14]
Epidemiology and risk factors
Headline epidemiology candidates must own
Large epidemiologic surveys document personality disorder as a substantial population burden, with STPD typically among the less prevalent named PDs yet enriched in specialty and psychosis-spectrum services.[6][7][8][10] Global meta-regression work reinforces that personality disorder is not a Western curiosity and remains method-sensitive.[9]
Risk and aetiology. Family history of schizophrenia-spectrum illness, childhood adversity/trauma amplifying cognitive-perceptual severity, social isolation, and cannabis/stimulant use are clinically important. Twin data show structured genetic and environmental contributions to personality disorder risk architecture, including Cluster A–relevant liability shared across related traits.[1][11]
Pathophysiology and mechanisms
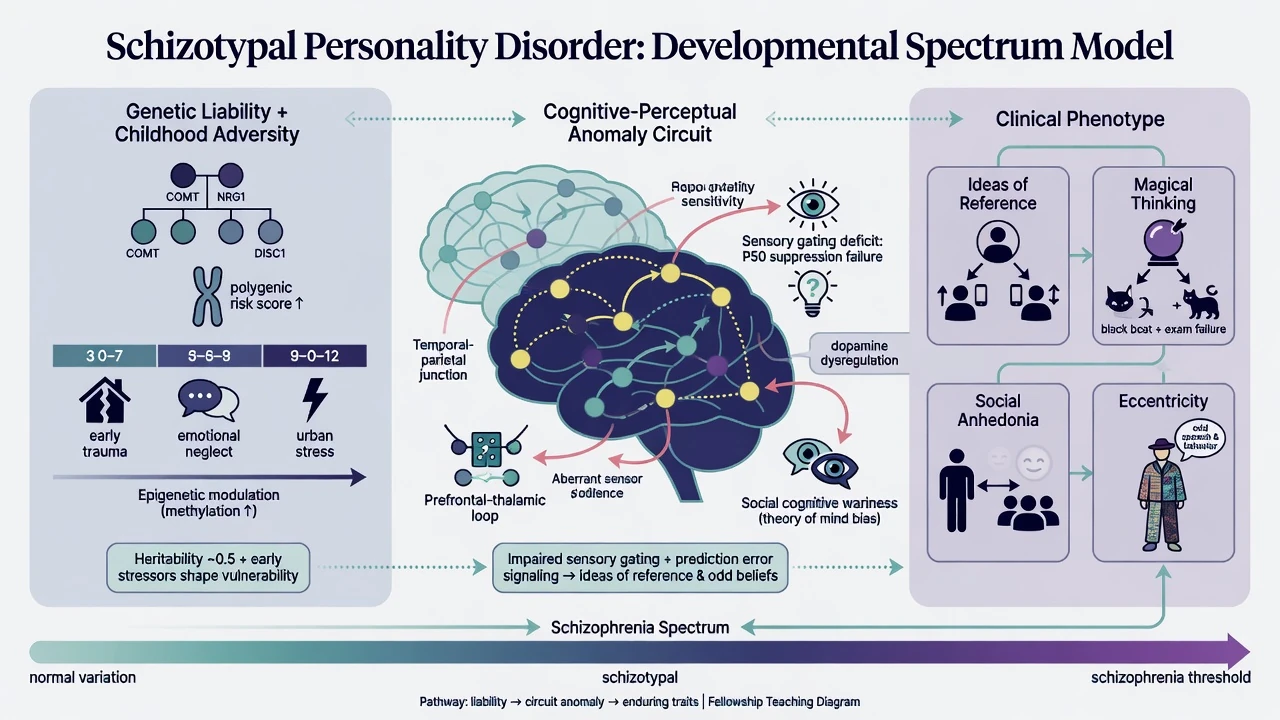
Spectrum model. STPD is best taught as a clinical phenotype on the schizophrenia continuum: ideas of reference, magical thinking, unusual perceptions, social anhedonia, odd speech, and interpersonal wariness without meeting full psychosis thresholds.[1][2]
Neurobiology (keep humble). Reviews implicate sensory gating anomalies, dopaminergic hypotheses, and social-cognitive network differences at the group level. These findings inform formulation and research; they do not diagnose STPD in an individual and must never replace longitudinal history and collateral.[1][2]
Psychological and social mechanisms. Attachment disruption, trauma, and chronic invalidation or bullying can amplify paranoid social anxiety and magical meaning-making. Cultural belief systems must be distinguished from pathological magical thinking that is idiosyncratic and impairing.[1][2]
Clinical presentation
Core adult presentation combines cognitive-perceptual oddness (ideas of reference, magical beliefs, unusual perceptions), interpersonal deficits (few confidants, discomfort with closeness), and disorganised eccentricity (odd speech, appearance, constricted or inappropriate affect). On MSE, listen for overvalued ideas versus fixed delusions, residual insight, metaphorical or vague speech without formal thought disorder thresholds, and social anxiety with a paranoid quality that does not extinguish easily with familiarity.[1][2]
Settings examiners use. Community clinics see depression and workplace friction in an eccentric loner; early psychosis services see attenuated positives with lifelong schizotypal traits; ED sees substance-amplified paranoia or self-neglect crises; GP settings see “odd but functioning” patients referred after relationship or vocational collapse.[1][2]
Differential diagnosis
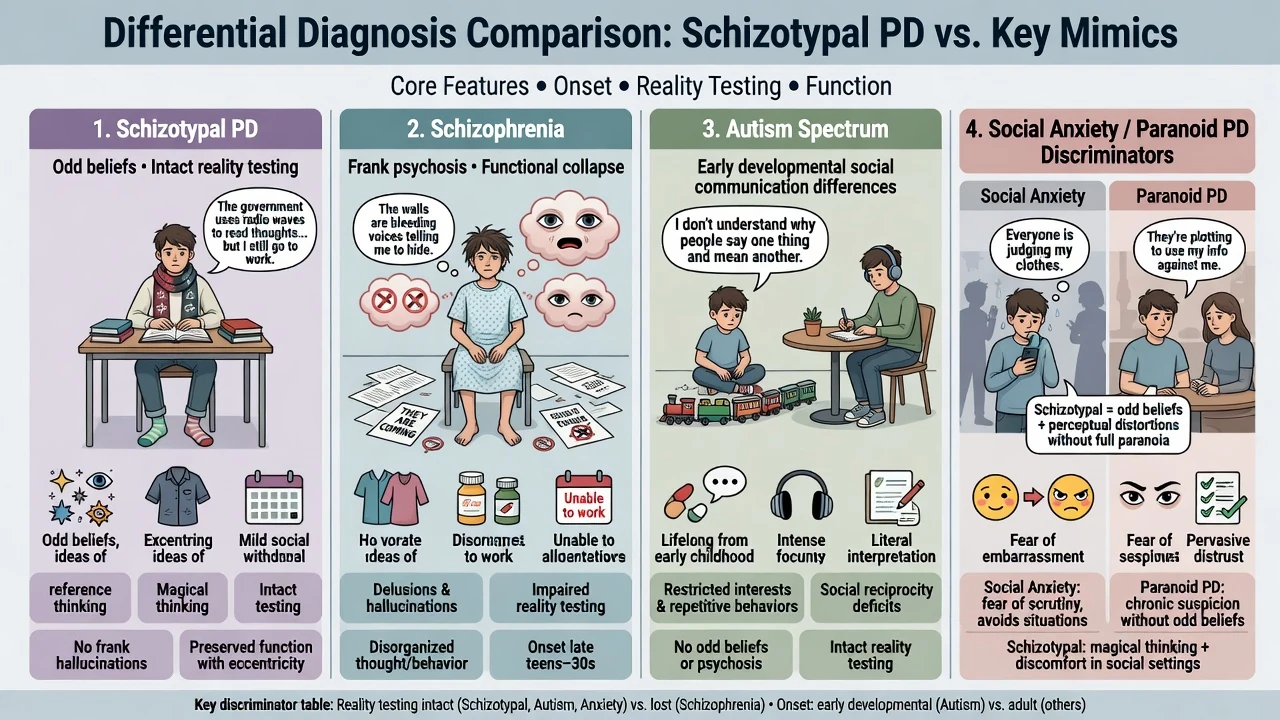
vs schizophrenia
- Schizophrenia: frank delusions/hallucinations, disorganisation, functional collapse thresholds
- STPD: trait oddness, largely intact reality testing
- Course and conviction decide
- Emerging psychosis leaves PD-only management
vs CHR / APS
- CHR: recent attenuated positives plus functional decline meeting UHR rules
- STPD: enduring pattern from early adulthood
- Both can coexist — dual formulation
- Use structured UHR tools when thresholds approached
vs ASD
- ASD: early developmental social communication differences, restricted/repetitive patterns, sensory profile
- STPD: magical thinking and ideas of reference less typical of classic ASD framing
- Dual formulation possible
- Do not force either/or from one interview
vs schizoid / paranoid PD / SAD
- Schizoid: detachment without cognitive-perceptual oddness
- Paranoid PD: distrust without broader oddness/magic
- SAD: self-conscious fear of scrutiny; STPD social anxiety often paranoid-toned
- Comorbidity still common
Also keep OCD with poor insight or magical thinking, substance-induced perceptual anomalies, PTSD dissociative phenomena, and late-onset organic change (TBI, frontotemporal syndromes, epilepsy, endocrine) on the board. The exam skill is discriminators plus comorbidity, not exclusive single labels.[1][2][12][15]
Clinical and bedside assessment
Structure the interview: developmental and school history; lifelong versus recent oddness; family history of psychosis; substance use (especially cannabis and stimulants); trauma; relationship and occupational function; prior treatments; current distress targets; collateral from family or workplace when possible.[1][2]
Mental State Examination. Thought content (ideas of reference, magical beliefs, overvalued ideas vs delusions); perception; thought form (vagueness, metaphor without frank formal thought disorder); affect (inappropriate or constricted); appearance/mannerisms; insight; alliance capacity and paranoid wariness. Document capacity as decision-specific.[1]
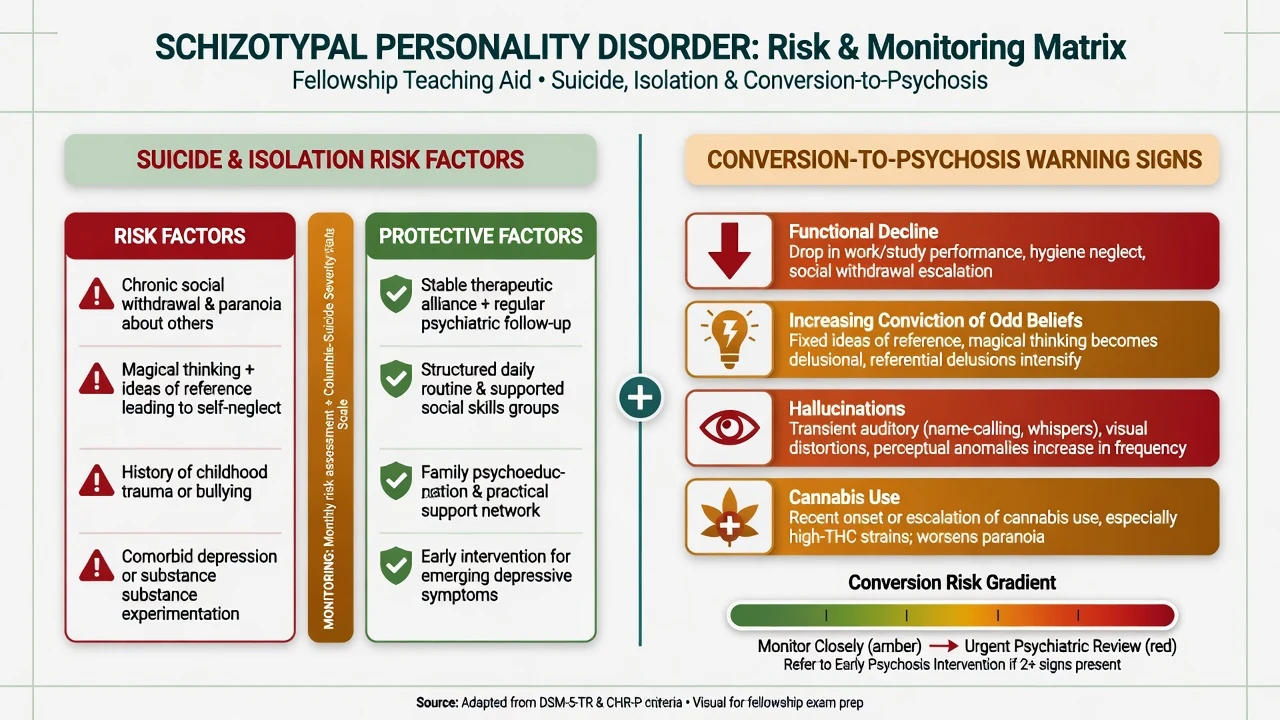
Risk domains. Suicide and self-harm rise with comorbid depression and isolation. Self-neglect and exploitation vulnerability matter in severe presentations. Violence risk is uncommon as a stereotype but can relate to paranoid threat appraisal — formulate context, not label fatalism.[1][2]
When recent functional decline and attenuated psychotic symptoms dominate, assess against clinical high-risk / ultra-high-risk frameworks (CAARMS/SIPS tradition) and collaborate with early intervention services rather than freezing the case as “personality forever.” Transition risk in CHR samples is substantial at group level but far from universal — use Fusar-Poli-era meta-analytic humility.[14][15]
Investigations
STPD has no laboratory gold standard. Investigate to exclude mimics, manage substances, and prepare for any medication: urine drug screen when relevant; FBC, U&E, LFT, TSH, glucose/lipids as baseline; pregnancy test when applicable; ECG and metabolic baseline before antipsychotics; cognitive screen and neuroimaging or EEG when late-onset change, focal neurology, seizures, or significant cognitive decline fire. Screen systematically for depression, anxiety, OCD, ASD, and evolving psychosis because they change treatment more than the personality label alone.[1][2][3]
Management — acute crisis and resuscitation
Immediate priorities. Medical stabilisation of intoxication, overdose, dehydration, or self-neglect. De-escalate; environmental calm; pharmacological rapid tranquillisation only when needed for imminent harm per local emergency protocols with monitoring — not as long-term “oddness sedation.”[2][4]
If frank psychosis emerges. Switch to a psychosis pathway (assessment, safety, antipsychotic treatment algorithms, early intervention) — do not hide behind a PD label.[2][15]
Crisis psychiatry stance. Validate distress without colluding with fixed false beliefs; still treat medical and psychiatric comorbidity with the same standard of care as any other patient. Avoid pejorative exclusion (“personality — no service”) when acute risk or treatable illness is present.[1][5]
Management — definitive and stepwise
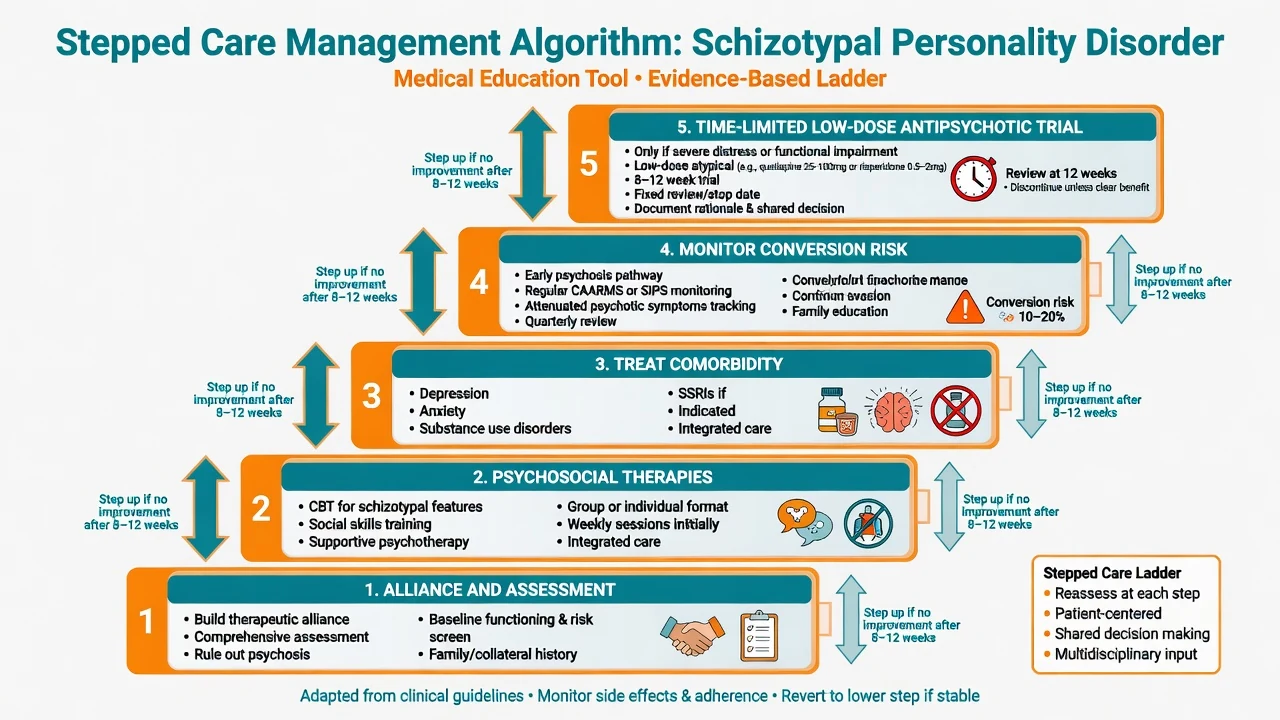
What the evidence actually supports
Systematic reviews of STPD diagnosis and treatment (Kirchner and colleagues) and GRADE-style updates on schizotypal disorder treatment (Gundersen and colleagues) emphasise limited trial quality, the primacy of careful diagnosis and monitoring, and cautious individualised intervention rather than a single disease-modifying standard drug.[2][4] Jakobsen’s systematic review of antipsychotics for schizotypy/STPD finds signals for low-dose antipsychotic benefit on cognitive-perceptual symptoms in some studies, with overall low-to-moderate certainty and important adverse-effect trade-offs.[3] Cluster A psychosocial and pharmacological meta-analytic work (Cheli 2025) continues to show sparse, heterogeneous evidence — structure and engagement still beat nihilism.[5]
Psychological and psychosocial approaches
Name a coherent package: slow alliance-building with transparent boundaries; supportive psychotherapy; CBT adaptations targeting ideas of reference, social anxiety, and unhelpful meaning-making without aggressive belief confrontation early; social skills training; vocational support; family psychoeducation where accepted; schema-informed or other structured PD therapies when broader personality pathology and service availability allow (Bamelis schema RCT is broader PD evidence, not an STPD-only mega-trial).[5][16]
Pharmacotherapy — only for targets you can name
No drug is approved as disease-modifying for STPD itself.[2][3][4] Treat:
- Major depression / anxiety with standard pathways. Example adult plan when an examiner forces a named comorbid regimen (individualise): sertraline 50 mg orally daily, early review for activation and adherence, titrate toward 50–150 mg as tolerated — this treats depression/anxiety, not “curing STPD.” Limited dispensing if overdose risk is high.[2][5]
- Substance use disorders with motivational and integrated dual care; cannabis reduction is a high-yield conversion-risk lever.[15]
- Severe cognitive-perceptual symptoms may justify a time-limited low-dose second-generation antipsychotic trial with written target, baseline metabolic panel and ECG risk assessment as indicated, metabolic monitoring, and a stop/review date (for example low-dose risperidone or another local first-line agent per product information — individualise; do not invent off-label megadoses). Evidence certainty is limited; shared decision-making is mandatory.[3][4]
Avoid chronic benzodiazepines for social oddness and avoid stacking multiple antipsychotics without review.[3][4]
Care system and multi-agency work
Match intensity to risk and function: outpatient psychology/psychiatry, CMHT, dual-diagnosis pathways, and early psychosis services when UHR thresholds are approached. Write a monitoring plan for conversion warning signs (rising conviction, hallucinations, functional drop, hygiene collapse, cannabis escalation). Consistency and patience beat charismatic one-off confrontations of magical beliefs.[14][15]
Australian and New Zealand practice emphasises stepped mental health care, cultural safety, and access to early psychosis intervention services when attenuated psychosis and functional decline emerge. Mental Health Act provisions are state/territory-specific — name least-restrictive principles, not invented section numbers.[15]
Specific subtypes and scenarios
STPD with comorbid depression. Common presentation pathway; treat depression fully while maintaining personality formulation.[1][2]
STPD at the CHR interface. Document attenuated positives, duration, functional change, family history, and substances; co-manage with early intervention when indicated.[14][15]
Substance-amplified oddness. Cannabis and stimulants can worsen referential and paranoid experiences — dual formulation and harm reduction are essential.[15]
Adolescent oddness. Distinguish normal developmental eccentricity, ASD, and emerging psychosis; do not casually lifelong-label a teenager from one interview.[12][15]
Cultural magical beliefs. Culturally sanctioned spiritual frameworks are not pathological by default; pathologise idiosyncratic, impairing, culturally incongruent magical thinking with collateral context.[1]
Complications and pitfalls
Classic pitfalls: missing ASD; missing OCD or social anxiety; unreviewed antipsychotics for chronic eccentricity; colluding with paranoid systems or, conversely, aggressively challenging beliefs on first contact and destroying alliance; late-onset organic change mislabelled as lifelong STPD; therapeutic nihilism.[2][12][3]
Prognosis and disposition
Course is often chronic with fluctuating severity. Many people remain non-psychotic with persistent interpersonal and occupational impairment; a minority transition to schizophrenia-spectrum psychosis, especially with functional decline and additional risk factors.[1][2][14] Better trajectories associate with treatment of depression/anxiety, reduced substance use, social support, and sustained structured psychosocial engagement.[2][5] Disposition is usually outpatient; brief admission for acute risk, severe self-neglect, or emerging psychosis. Reassess dynamically after relationship rupture, substance relapse, or new functional drop.[1][15]
Special populations
Adolescents and transition-age youth. Prioritise developmental history, ASD assessment, and early psychosis pathways when UHR criteria are met; avoid premature fatalistic personality labels.[12][15]
Older adults. New-onset oddness is an organic/mood red flag until proven otherwise.[1]
Pregnancy and parenting. Prioritise psychosocial care; any antipsychotic requires individualised risk–benefit counselling and product-information-level discussion; safeguarding of dependents is part of the plan when self-neglect or paranoia threatens care capacity.[2][3]
Cultural and Indigenous safety (ANZ). Cultural formulation prevents mislabelling culturally sanctioned beliefs as magical thinking pathology; structural context never erases individual functional impairment when true STPD criteria are met.[1][13]
Neurodiversity interfaces. ASD and STPD can co-occur or be confused — dual formulation beats forced single labels.[12]
Evidence, guidelines and controversies
Core evidence pillars for fellowship answers include clinical reviews of STPD (Rosell), systematic reviews of diagnosis/treatment (Kirchner) and GRADE treatment certainty (Gundersen), antipsychotic systematic review (Jakobsen), Cluster A intervention meta-analyses (Cheli), epidemiology (Torgersen, Lenzenweger NCS-R, Grant NESARC, Coid, Shadid), genetics/structure (Kendler twin PD architecture), spectrum/CHR interface (Fusar-Poli transition and prevention syntheses), broader PD psychotherapy context (Bamelis schema RCT), ASD interface (Lugnegård), and ICD-11 dimensional progress (Kim/Tyrer line).[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16]
Mature controversies. Whether STPD belongs primarily in personality or schizophrenia-spectrum chapters; how aggressively to medicate cognitive-perceptual symptoms given low-certainty evidence; whether dimensional ICD-11 should replace categorical STPD in clinical notes; and how to resource slow alliance work in stretched services.[2][4][13]
Exam pearls
SCHIZOTYPE — viva checklist
SCHIZOTYPE
≥5 of 9 DSM features after general PD criteria
Cognitive-perceptual oddness (reference, magic, illusions)
History longitudinal — not one weird interview
Intact reality testing vs frank psychosis
Zone of spectrum adjacency — monitor conversion
Organic exclusion for late-onset change
Therapy/alliance first; social skills and CBT adaptations
Youth: ASD and UHR differentials mandatory
Pharmacotherapy only for named targets with review dates
Evidence is limited — no disease-modifying drug
60-second oral summary
STPD is DSM ≥5 of 9 social/interpersonal deficits with cognitive-perceptual distortions and eccentricity beginning by early adulthood — spectrum-adjacent but not frank schizophrenia. Discriminate schizophrenia (conviction, collapse), ASD (developmental profile), schizoid (no odd perceptions), paranoid PD (distrust without broader oddness), and CHR when recent decline dominates. Assess risk for suicide with depression/isolation and monitor conversion signs. Treatment: slow alliance, psychosocial strategies, treat comorbidity (e.g. sertraline for depression), reduce cannabis, and only time-limited low-dose antipsychotic trials for severe cognitive-perceptual targets with review dates. If frank psychosis emerges, switch pathways. Evidence is limited; structure beats nihilism and polypharmacy theatre.[1][2][3][4][12][15]
References
- [1]Rosell DR, Futterman SE, McMaster A, Siever LJ Schizotypal personality disorder: a current review Curr Psychiatry Rep, 2014.PMID 24828284
- [2]Kirchner SK, Roeh A, Nolden J, Hasan A Diagnosis and treatment of schizotypal personality disorder: evidence from a systematic review NPJ Schizophr, 2018.PMID 30282970
- [3]Jakobsen KD, Skyum E, Hashemi N, Schjerning O, et al. Antipsychotic treatment of schizotypy and schizotypal personality disorder: a systematic review J Psychopharmacol, 2017.PMID 28347257
- [4]Gundersen KB, Arnfred B, Albert N, Rasmussen AR, et al. Treatment of schizotypal disorder: A systematic review and GRADE evaluation of the certainty of evidence Schizophr Res, 2026.PMID 41421074
- [5]Cheli S, Wisepape CN, Witten CDY, Floridi M, et al. Psychosocial and pharmacological interventions for cluster a personality disorders: A systematic review and two exploratory meta-analyses Personal Disord, 2025.PMID 40111791
- [6]Torgersen S, Kringlen E, Cramer V The prevalence of personality disorders in a community sample Arch Gen Psychiatry, 2001.PMID 11386989
- [7]Lenzenweger MF, Lane MC, Loranger AW, Kessler RC DSM-IV personality disorders in the National Comorbidity Survey Replication Biol Psychiatry, 2007.PMID 17217923
- [8]Grant BF, Hasin DS, Stinson FS, Dawson DA, et al. Prevalence, correlates, and disability of personality disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions J Clin Psychiatry, 2004.PMID 15291684
- [9]Shadid J, Ferrari AJ, Bach B, Sellbom M, et al. The global epidemiology of personality disorder: a systematic review and meta-regression Lancet Psychiatry, 2025.PMID 41197646
- [10]Coid J, Yang M, Tyrer P, Roberts A, et al. Prevalence and correlates of personality disorder in Great Britain Br J Psychiatry, 2006.PMID 16648528
- [11]Kendler KS, Aggen SH, Czajkowski N, Røysamb E, et al. The structure of genetic and environmental risk factors for DSM-IV personality disorders: a multivariate twin study Arch Gen Psychiatry, 2008.PMID 19047531
- [12]Lugnegård T, Hallerbäck MU, Gillberg C Personality disorders and autism spectrum disorders: what are the connections? Compr Psychiatry, 2012.PMID 21821235
- [13]Kim YR, Tyrer P, Mulder R, King JD, et al. ICD-11 classification of personality disorder: there is no other way forward Br J Psychiatry, 2026.PMID 41906979
- [14]Fusar-Poli P, Bonoldi I, Yung AR, et al. Predicting psychosis: meta-analysis of transition outcomes in individuals at high clinical risk Arch Gen Psychiatry, 2012.PMID 22393215
- [15]Fusar-Poli P, Salazar de Pablo G, Correll CU, et al. Prevention of Psychosis: Advances in Detection, Prognosis, and Intervention JAMA Psychiatry, 2020.PMID 32159746
- [16]Bamelis LL, Evers SM, Spinhoven P, Arntz A Results of a multicenter randomized controlled trial of the clinical effectiveness of schema therapy for personality disorders Am J Psychiatry, 2014.PMID 24322378