Psych · General adult psychiatry — mood disorders
Seasonal and atypical depression
Also known as Seasonal affective disorder · SAD · Winter depression · Seasonal pattern specifier · Atypical features depression · Depression with atypical features · Reverse vegetative depression
Exam-exhaustive fellowship reference on seasonal pattern major depression (SAD) and depression with atypical features — DSM-5-TR/ICD framing, circadian mechanisms, light therapy parameters, Can-SAD, bupropion XL prevention, SSRIs, CBT-SAD, MAOI historical evidence, differentials, and guideline deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Seasonal and atypical presentations are high-yield specifier topics. Examiners test whether you treat them as freestanding folklore diagnoses or as operational DSM/ICD constructs nested inside major depression (or bipolar depression). FRANZCP MEQs want light parameters, preventive bupropion timing, and bipolar screens. MRCPsych papers love atypical feature lists and MAOI teaching. CASC stations often involve explaining a light box or autumn prevention plan to a patient who thinks they have "just winter blues."[8][17]
Definition and classification
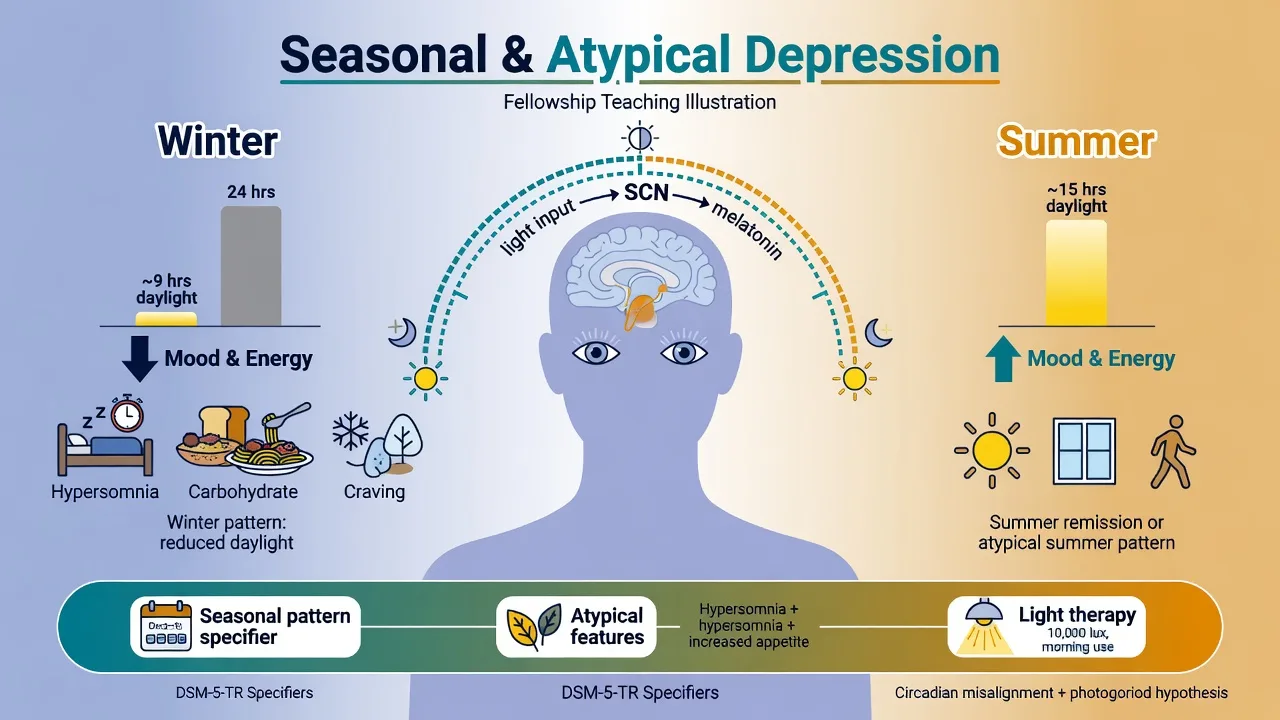
Seasonal affective disorder (SAD) in contemporary nosology is not a separate freestanding DSM-5-TR disorder. It is major depressive disorder (or bipolar disorder) with seasonal pattern. Clinically, "SAD" still denotes recurrent winter (or, less often, summer) major depressive episodes with predictable remissions.[8][11]
DSM-5-TR seasonal pattern — reproduce precisely. There is a regular temporal relationship between onset of major depressive episodes and a particular time of year (e.g. autumn/winter). Full remissions (or a change from depression to mania/hypomania) also occur at a characteristic time of year (e.g. spring). In the last 2 years, two major depressive episodes have occurred that demonstrate the seasonal relationship, and no nonseasonal major depressive episodes have occurred during that same period. Lifetime seasonal major depressive episodes substantially outnumber nonseasonal episodes. Do not apply the specifier if the pattern is better explained by seasonally linked psychosocial stressors alone (e.g. annual unemployment every winter) without a true biological-seasonal pattern.[8][11][17]
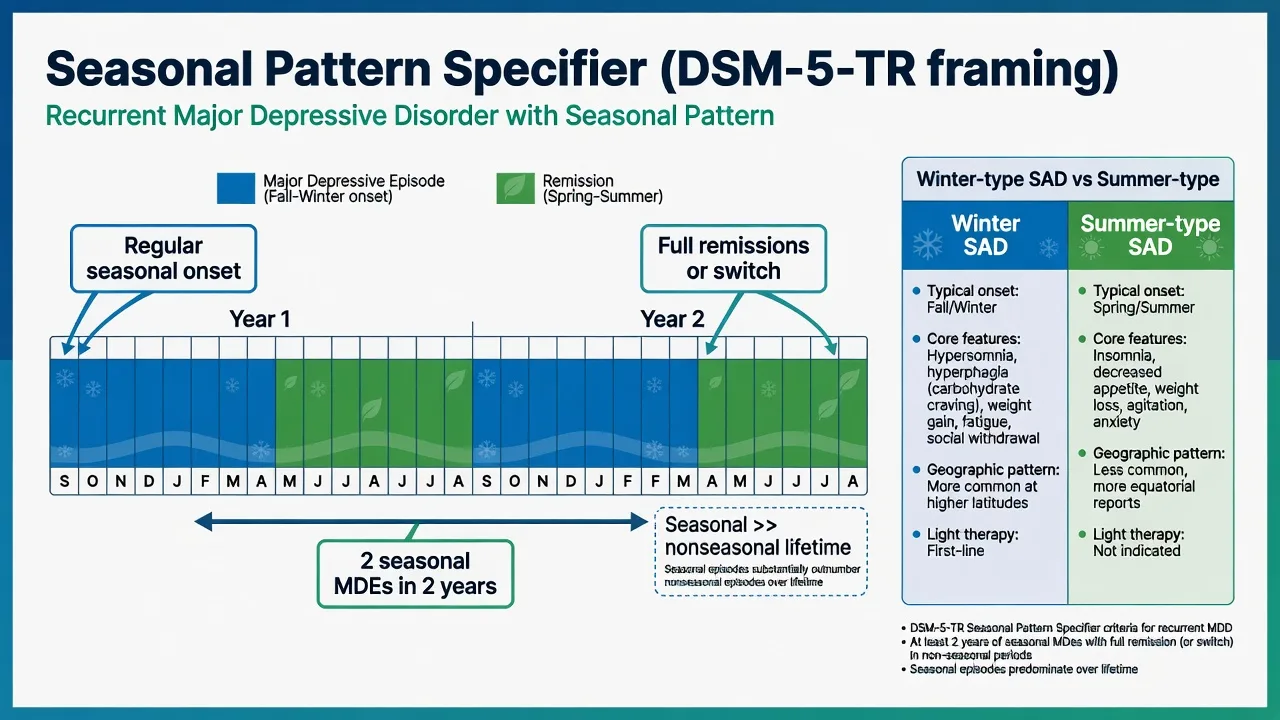
Winter-type vs summer-type. Winter-type SAD is the classic exam entity: fall–winter onset, spring–summer remission, often with hypersomnia, hyperphagia and carbohydrate craving. Summer-type seasonal depression is rarer and may show more insomnia/agitation; do not force winter light-therapy algorithms uncritically onto summer pattern illness without reformulating triggers (heat, light excess, schedule change).[8][11]
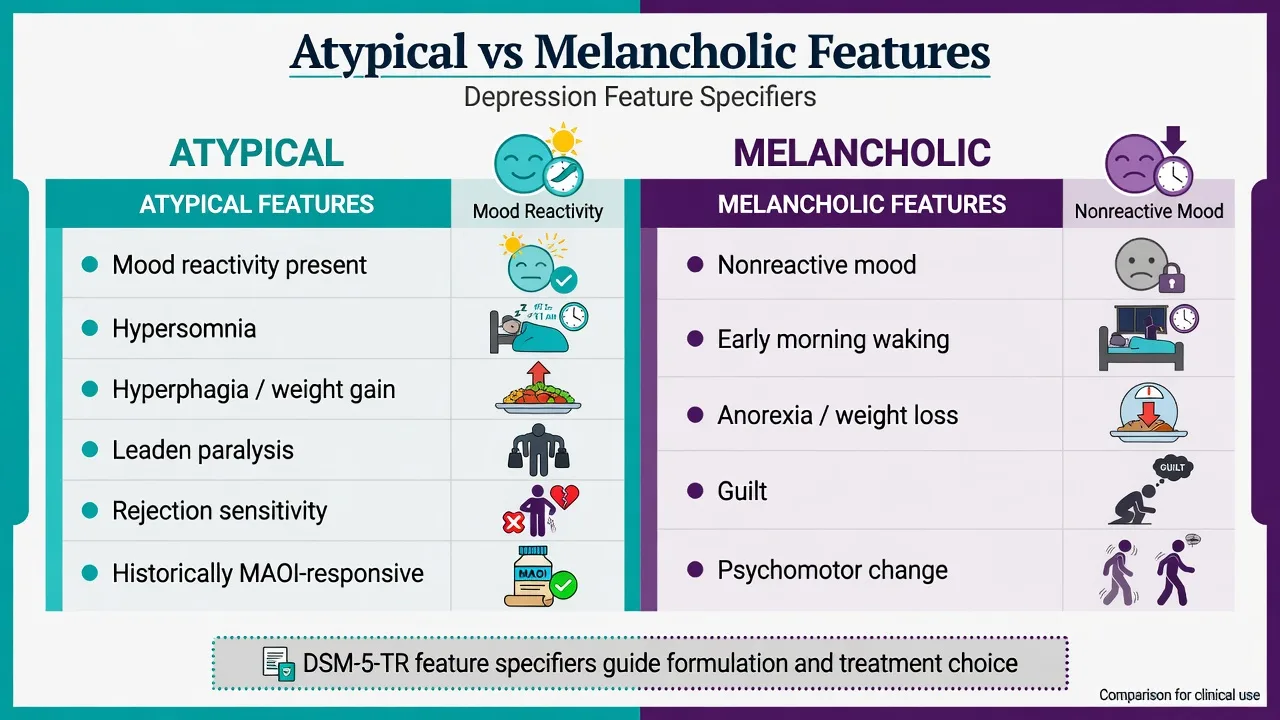
Atypical features specifier (DSM-5-TR). Mood reactivity (mood brightens to actual or potential positive events) is mandatory, plus two or more of: significant weight gain or increase in appetite; hypersomnia; leaden paralysis (heavy, leaden feelings in arms or legs); long-standing pattern of interpersonal rejection sensitivity resulting in social/occupational impairment. The rejection sensitivity criterion can be trait-like and is not restricted only to depressive episodes. Atypical features are a feature specifier, not a separate disease, and they can co-occur with seasonal winter depression (shared reverse vegetative phenotype).[13][16]
ICD-11. Use depressive episode/disorder with course and symptom qualifiers; state which manual you are using when an examiner asks about "seasonal affective disorder" as a named entity versus a pattern of recurrence.[17]
Seasonal pattern
- Course specifier on MDD or bipolar disorder
- Predictable onset/remission by season
- Two-year seasonal rule + lifetime predominance
- Light therapy and autumn prevention are high-yield
Atypical features
- Feature specifier on a depressive episode
- Mood reactivity is required
- Reverse vegetative cluster + rejection sensitivity
- Historical MAOI preferential response literature
Melancholic features
- Nonreactive mood / near-total anhedonia
- Early waking, anorexia, guilt, psychomotor change
- Often stronger biological treatment and ECT signals
- Do not mix with atypical in the same episode framing
Winter blues (sub-syndromal)
- Seasonal mood change without full MDE criteria
- SPAQ screens seasonality, does not diagnose MDD
- Lifestyle light exposure may help
- Escalate if full episode criteria emerge
Epidemiology and risk
Numbers candidates should own
Epidemiological reviews show substantial variation depending on whether case definition requires full major depressive episodes or broader seasonal symptom scales. Latitude associations appear in aggregate data but are not absolute — genetic, cultural and daylight-behaviour factors modify risk, and some high-latitude populations do not show the expected excess.[11][12][20]
Risk factors: personal history of mood disorder, family history, prior seasonal episodes, limited daylight exposure (indoor occupation, high latitude winters), and younger adult onset with recurrence. Comorbidity with anxiety, binge-eating patterns, and bipolar spectrum illness is clinically important. Southern hemisphere literature is thinner than northern; do not assume identical month mapping when examining Australian patients — map to local photoperiod, not northern-hemisphere month names alone.[8][11][17]
Pathophysiology
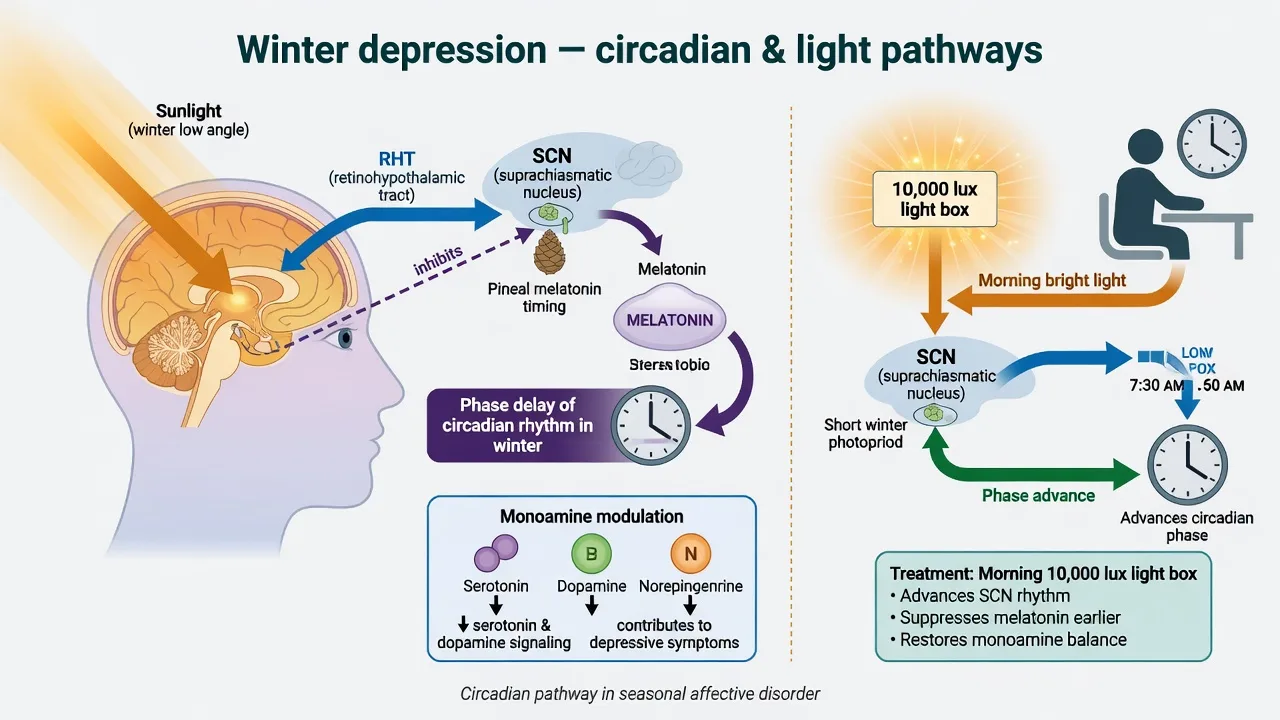
Circadian / phase-shift model. Winter photoperiod reduction can delay circadian phase relative to the sleep–wake schedule. The retinohypothalamic tract conveys light to the suprachiasmatic nucleus; melatonin timing is a readable phase marker. Lewy and colleagues advanced a circadian basis for winter depression in which appropriately timed light (typically morning) can phase-advance rhythms and improve mood.[10]
Monoamine seasonality. Serotonergic and other monoamine systems show seasonal variation in some human studies; this is a bridging hypothesis between light input and antidepressant pharmacology, not a diagnostic blood test.[8][10]
Atypical features biology. Classic teaching contrasts atypical depression with more hypercortisolaemic melancholia and notes preferential historical response to MAOIs versus TCAs. Use this at viva level without claiming a single pathognomonic biomarker.[13][14][16]
Psychological maintaining factors. Seasonal catastrophic beliefs, behavioural withdrawal, reduced activity and social isolation maintain winter depression. Rejection sensitivity maintains interpersonal crises in atypical presentations and maps to CBT/IPT targets.[6][15]
Clinical presentation
Winter SAD. Depressed mood and anhedonia with prominent reverse vegetative features: hypersomnia, carbohydrate craving, weight gain, low energy, afternoon worsening, social withdrawal. Onset often clusters in autumn/early winter; improvement in spring is part of the history you must elicit across multiple years.[8][11]
Atypical features episode. Mood can lift temporarily to positive events (reactivity) yet overall episode remains impairing. Patients describe leaden limb heaviness, long sleeps, increased appetite, and lifelong sensitivity to perceived rejection that damages relationships and work.[13][16]
Bipolar seasonal pattern. Winter depression with spring hypomania is an examiner classic. Always screen elevated periods, reduced sleep need, grandiosity and risky behaviour before calling the illness "unipolar SAD."[17]
Differential diagnosis
Bipolar depression
- Prior mania/hypomania decisive
- Seasonal switches common in some patients
- Antidepressant or light may unmask elevation
- Stabiliser-first framing when bipolar
Sleep / circadian disorders
- Delayed sleep-phase disorder
- OSA with hypersomnia and weight gain
- Shift-work disorder
- Primary hypersomnia syndromes
Medical mimics
- Hypothyroidism
- Anaemia, B12 deficiency
- Vitamin D low as contributor, not sole diagnosis
- Medication effects (steroids, etc.)
Personality / anxiety overlap
- Borderline affective instability vs episode
- Social anxiety with rejection fears
- Atypical rejection sensitivity can be trait-like
- Formulate both axes when comorbid
Also exclude substance-related winter worsening (alcohol, cannabis) and nonseasonal recurrent MDD with coincidental cold-weather stress. [8][17]
Assessment
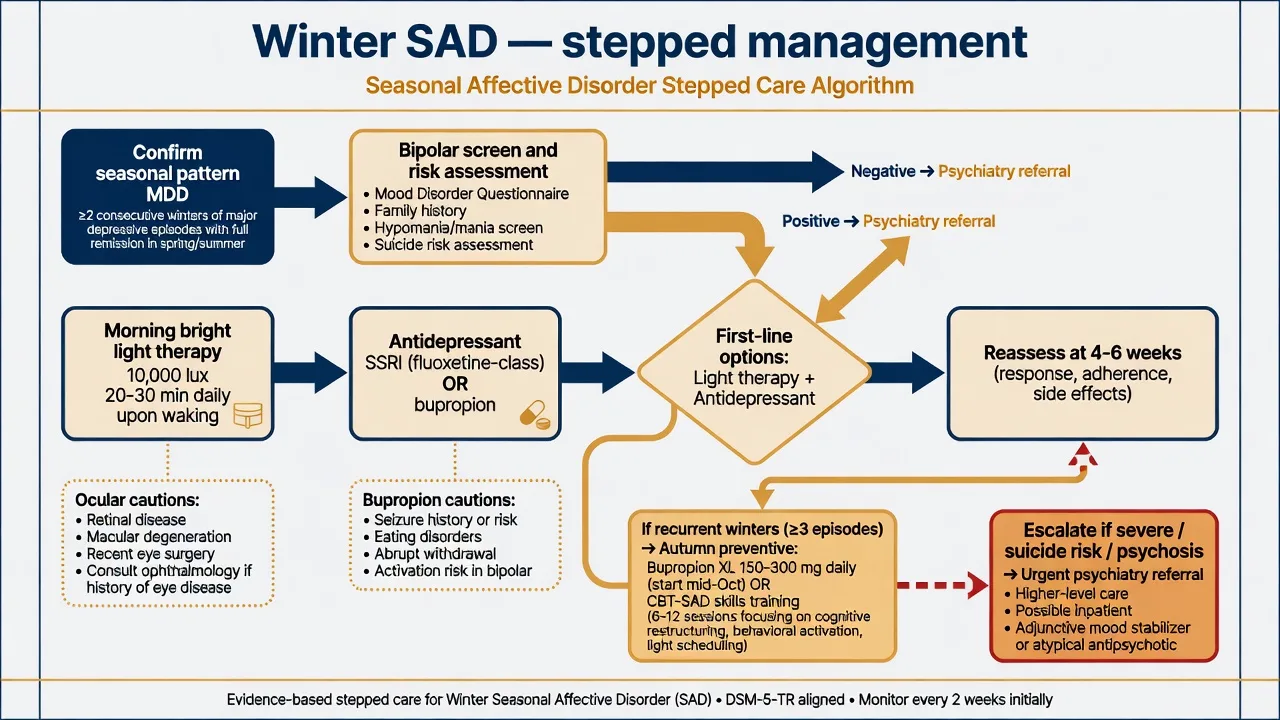
Structure history with a month-by-month mood chart across at least two years: onset month, remission month, inter-episode function, nonseasonal episodes, postpartum or travel-related shifts, and light exposure (occupation, latitude, holidays). Complete a bipolar screen and full suicide risk assessment every time criteria for a major depressive episode are met.[8][17]
SPAQ (Seasonal Pattern Assessment Questionnaire) is a research/clinical screening tool for seasonality of mood and behaviour; it does not replace DSM/ICD diagnosis of a major depressive episode. PHQ-9 remains useful for severity tracking within an episode.[11][17]
Ocular history before bright light therapy: retinal disease, recent eye surgery, photosensitising drugs (e.g. some antipsychotics, antibiotics, St John's wort combinations) — seek ophthalmology advice when risk is non-trivial.[1][8]
Investigations
As for MDD: TSH, FBC, electrolytes, metabolic panel as indicated; pregnancy test when relevant; consider sleep study if OSA is plausible given hypersomnia and weight gain. Do not order melatonin profiles or specialized chronobiology assays as routine diagnostic tests for SAD in general adult clinics.[8][17]
Acute risk management
If light therapy or an antidepressant precipitates elevated mood, reassess for bipolar spectrum illness, stop or modify the offending intervention, and manage per bipolar protocols.[2][17]
Definitive management — seasonal pattern
Bright light therapy
Light therapy has meta-analytic support in mood disorders, with the strongest clinical tradition in winter SAD.[1]
Exam parameters (classic stem set). Use a tested bright light box delivering about 10,000 lux of white light at the recommended distance. Sit with eyes open, facing toward the box without staring into the bulbs, typically for about 20–30 minutes shortly after waking in the morning for winter-type SAD. Response often begins within 1–2 weeks if the dose and timing are adequate. Evening light can worsen insomnia or phase delay and is usually avoided for classic winter phase-delay phenotypes.[1][2][8]
Adverse effects. Headache, eyestrain, irritability, insomnia, and rare hypomanic switch. Counsel ocular cautions and stop-rules for agitation or elevated mood.[1][2]
Can-SAD (landmark). In winter SAD, bright light therapy and fluoxetine showed comparable effectiveness in a randomized trial, giving examiners a clean "light versus SSRI" evidence hook. Choice then depends on preference, severity, access to a quality light box, comorbidity, and prior response.[2]
Antidepressants in seasonal MDD
When light is inaccessible, insufficient, declined, or the episode is moderate–severe, use a standard evidence-based antidepressant with measurement-based care. A practical named start for many adults: fluoxetine 20 mg orally each morning (as in Can-SAD framing), or sertraline 50 mg orally daily, titrating after early safety review toward a therapeutic dose with 4–6 weeks at an adequate dose before declaring failure. Monitor activation, sexual side-effects, hyponatraemia risk in older adults, and early suicidality after initiation.[2][18][17]
Preventive pharmacotherapy — bupropion XL
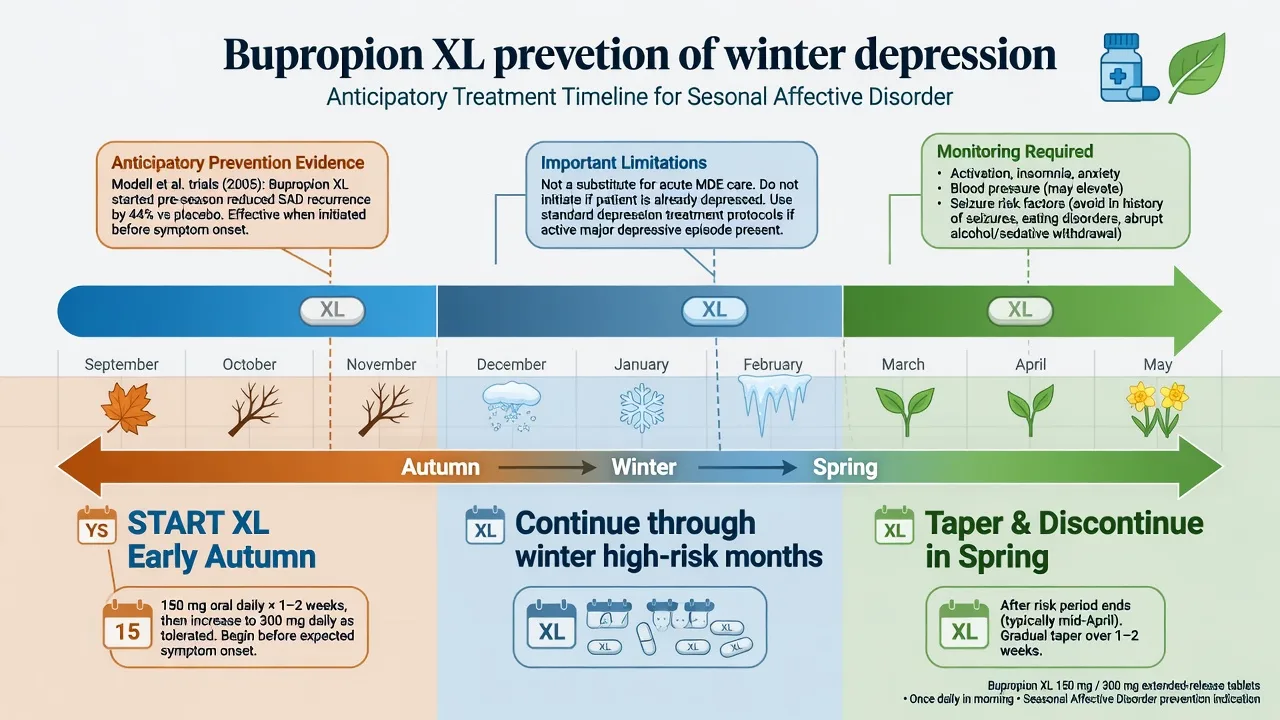
For patients with recurrent winter major depressive episodes, anticipatory treatment with bupropion extended-release (XL) begun in autumn before expected onset reduces the risk of a seasonal episode. Modell and colleagues demonstrated prevention with bupropion XL across randomized trials; subsequent Cochrane synthesis of second-generation antidepressants for prevention supports efficacy of this strategy, with bupropion the principal agent studied.[3][4][9]
Practical regimen examiners expect. Start in early autumn (timing individualised to the patient's historical onset), e.g. bupropion XL 150 mg orally once daily, then increase to 300 mg orally once daily if tolerated and indicated by product guidance and clinical response/prevention plan; continue through the winter risk period; taper and stop in spring after the risk window. This is prevention, not a reason to withhold acute care if the patient is already in a major depressive episode.[3][4][9]
Safety. Seizure risk (dose-related; avoid in active eating disorders with purging, abrupt alcohol/sedative withdrawal, known seizure disorder unless specialist-led), blood pressure rise, insomnia, activation, and interaction checks. Not first-line in pregnancy without specialist risk–benefit discussion.[3][18]
Psychological therapy — CBT for SAD
CBT adapted for SAD targets seasonal negative beliefs and winter behavioural withdrawal. In randomized work by Rohan and colleagues, CBT and light therapy produced comparable acute outcomes; follow-up across subsequent winters suggested CBT may confer more durable protection against recurrence for some patients than light alone — a high-yield viva contrast (skills that persist vs a device that must be reused each winter).[6][7]
Cochrane reviews of preventive light and preventive psychological therapies note limited evidence quality for broad prevention claims beyond well-studied pathways; do not oversell unfocused "winter counselling" as equivalent to protocolized CBT-SAD or evidence-based medication prevention.[5]
Lifestyle adjuncts
Scheduled outdoor morning light, exercise, sleep regularisation, and equator-directed travel can help but are adjuncts. Full major depressive episode criteria still warrant structured treatment.[8][19]
RANZCP mood disorder guidance frames depression within formulation-driven stepped care; light therapy and seasonal patterns sit inside broader MDD/bipolar pathways rather than as a hobbyist side protocol. Map winter months to southern hemisphere photoperiods for Australian and New Zealand patients.[17]
Definitive management — atypical features
Historical pharmacology. Classic Columbia/New York trials showed phenelzine superior to imipramine in probable atypical depression, establishing the teaching that MAOIs preferentially help the atypical feature set relative to TCAs.[13][14]
Modern first-line practice. Most patients still start with an SSRI/SNRI or bupropion (helpful when hypersomnia, weight gain and anergia dominate and seizure risk is low), plus psychotherapy, because MAOI diet/drug constraints and toxicity risk reserve irreversible MAOIs for specialist refractory pathways. Moclobemide (reversible MAOI-A) is regionally available with fewer dietary constraints than phenelzine but is not a free pass on interactions.[16][18]
Psychotherapy evidence. Cognitive therapy can match phenelzine and beat placebo in atypical depression in controlled work by Jarrett and colleagues — do not imply only MAOIs work.[15]
Named MAOI example (specialist). Phenelzine often started around 15 mg orally three times daily with slow titration under specialist supervision, strict tyramine diet, washout rules with other serotonergic agents, and education on hypertensive crisis. Never combine with SSRIs/SNRIs/meperidine-type opioids. This is viva/MEQ depth, not automatic first prescription in primary care.[13][16]
Subtypes and scenarios
| Scenario | Key move |
|---|---|
| Unipolar winter SAD, mild–moderate | Morning 10,000 lux light ± CBT-SAD; monitor risk |
| Recurrent winters, currently well in summer | Plan autumn bupropion XL prevention or CBT skills maintenance |
| Bipolar with winter depression | Mood stabiliser primacy; light only with switch monitoring |
| Atypical features, nonseasonal | SSRI/bupropion + CBT; MAOI if refractory specialist care |
| Severe/psychotic seasonal depression | Do not rely on light alone; consider admission/ECT pathway as for severe MDD |
| Adolescent winter depression | Family involvement, school function, careful SSRI monitoring if used |
Complications and pitfalls
- Calling every winter low mood "SAD" without MDE criteria or the two-year rule.[11]
- Missing bipolarity; light or antidepressant-induced hypomania.[2][17]
- Under-dosing light (wrong lux, evening-only use, eyes closed the whole time, irregular adherence).[1][8]
- Starting preventive bupropion only after the winter episode is entrenched and calling that "prevention."[3][4]
- Assuming atypical features equal mild illness — chronicity and impairment can be severe.[16]
- MAOI interaction disasters when "remembering the old teaching" without infrastructure for safe use.[13]
Prognosis and disposition
Without prevention, winter episodes commonly recur. Residual seasonality and incomplete summer recovery raise next-winter risk. Disposition: educated primary care management of uncomplicated light-responsive illness; secondary care for bipolar risk, high suicide risk, treatment resistance, or diagnostic complexity. Functional recovery (work, relationships) is an outcome equal to PHQ-9 change.[7][9][17]
Special populations
Adolescents. School decline in winter months; parental supervision of light devices; careful risk–benefit if antidepressants used; family psychoeducation.[17]
Pregnancy. Untreated depression harms mother and fetus; light therapy is an attractive non-drug option for selected patients with specialist obstetric-psychiatric collaboration; medication decisions are individualised.[17][19]
Older adults. Ocular disease limits light intensity options; SSRI hyponatraemia; medical comorbidity; still treat full episodes actively.[17]
Shift workers / polar work. Photoperiod disruption may mimic or worsen seasonal patterns — reformulate circadian contribution and occupational health measures.[8][10]
Evidence and guidelines (exam names)
- Golden 2005 — light therapy meta-analysis in mood disorders.[1]
- Can-SAD (Lam 2006) — light ≈ fluoxetine in winter SAD.[2]
- Modell 2005 — bupropion XL prevention of seasonal episodes.[3]
- Cochrane 2019 — SGA prevention; light prevention evidence base caveats.[4][5]
- Rohan 2015/2016 — CBT vs light acute parity; multi-winter durability signals for CBT.[6][7]
- Lewy 2006 — circadian basis of winter depression.[10]
- Quitkin/Liebowitz 1988; Jarrett 1999; Stewart 2007 — atypical features treatment literature.[13][14][15][16]
- RANZCP 2020 mood guidelines; CANMAT 2016 pharma and CAM/physical treatment sections.[17][18][19]
Exam pearls
WINTER care checklist
References
- [1]Golden RN, Gaynes BN, Ekstrom RD, et al. The efficacy of light therapy in the treatment of mood disorders: a review and meta-analysis of the evidence Am J Psychiatry, 2005.PMID 15800134
- [2]Lam RW, Levitt AJ, Levitan RD, et al. The Can-SAD study: a randomized controlled trial of the effectiveness of light therapy and fluoxetine in patients with winter seasonal affective disorder Am J Psychiatry, 2006.PMID 16648320
- [3]Modell JG, Rosenthal NE, Harriett AE, et al. Seasonal affective disorder and its prevention by anticipatory treatment with bupropion XL Biol Psychiatry, 2005.PMID 16271314
- [4]Gartlehner G, Nussbaumer-Streit B, Gaynes BN, et al. Second-generation antidepressants for preventing seasonal affective disorder in adults Cochrane Database Syst Rev, 2019.PMID 30883669
- [5]Nussbaumer-Streit B, Forneris CA, Morgan LC, et al. Light therapy for preventing seasonal affective disorder Cochrane Database Syst Rev, 2019.PMID 30883670
- [6]Rohan KJ, Mahon JN, Evans M, et al. Randomized Trial of Cognitive-Behavioral Therapy Versus Light Therapy for Seasonal Affective Disorder: Acute Outcomes Am J Psychiatry, 2015.PMID 25859764
- [7]Rohan KJ, Meyerhoff J, Ho SY, et al. Outcomes One and Two Winters Following Cognitive-Behavioral Therapy or Light Therapy for Seasonal Affective Disorder Am J Psychiatry, 2016.PMID 26539881
- [8]Westrin A, Lam RW Seasonal affective disorder: a clinical update Ann Clin Psychiatry, 2007.PMID 18058281
- [9]Westrin A, Lam RW Long-term and preventative treatment for seasonal affective disorder CNS Drugs, 2007.PMID 17927295
- [10]Lewy AJ, Lefler BJ, Emens JS, et al. The circadian basis of winter depression Proc Natl Acad Sci U S A, 2006.PMID 16648247
- [11]Magnusson A, Partonen T The diagnosis, symptomatology, and epidemiology of seasonal affective disorder CNS Spectr, 2005.PMID 16041294
- [12]Magnusson A An overview of epidemiological studies on seasonal affective disorder Acta Psychiatr Scand, 2000.PMID 10721866
- [13]Quitkin FM, Stewart JW, McGrath PJ, et al. Phenelzine versus imipramine in the treatment of probable atypical depression: defining syndrome boundaries of selective MAOI responders Am J Psychiatry, 1988.PMID 3278631
- [14]Liebowitz MR, Quitkin FM, Stewart JW, et al. Antidepressant specificity in atypical depression Arch Gen Psychiatry, 1988.PMID 3276282
- [15]Jarrett RB, Schaffer M, McIntire D, et al. Treatment of atypical depression with cognitive therapy or phenelzine: a double-blind, placebo-controlled trial Arch Gen Psychiatry, 1999.PMID 10232298
- [16]Stewart JW Treating depression with atypical features J Clin Psychiatry, 2007.PMID 17348764
- [17]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [18]Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [19]Ravindran AV, Balneaves LG, Faulkner G, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 5. Complementary and Alternative Medicine Treatments Can J Psychiatry, 2016.PMID 27486153
- [20]Kim K, Kim J, Jung S, et al. Global prevalence of seasonal affective disorder by latitude: A systematic review and meta-analysis J Affect Disord, 2025.PMID 40614973