Psych · General adult psychiatry — anxiety disorders
Selective mutism
Also known as SM · Elective mutism (historical, outdated) · Situational mutism · Anxiety-related failure to speak
Exam-exhaustive fellowship reference on selective mutism — DSM-5-TR and ICD-11 criteria, anxiety-chapter reclassification, epidemiology, behavioural inhibition and social-evaluative mechanisms, differentials from SAD, ASD and language disorders, SMQ/SSQ assessment, first-line behavioural/CBT school-inclusive packages (IBTSM, Oerbeck), fluoxetine adjunct evidence, school liaison, multi-board stepped care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Selective mutism (SM) is a low-prevalence, high-impact anxiety presentation that fellowship examiners use to test whether candidates still think like 1980s "elective mutism" physicians or like contemporary anxiety clinicians. FRANZCP MEQs and MRCPsych CASC reward criteria with the one-month / not first-school-month traps, school-inclusive behavioural plans, and fluoxetine evidence literacy. ABPN items probe DSM-5 reclassification and SAD overlap. MD/DNB vivas expect differentials from language disorder and autism cold.[1][2][3]
Overview and definition
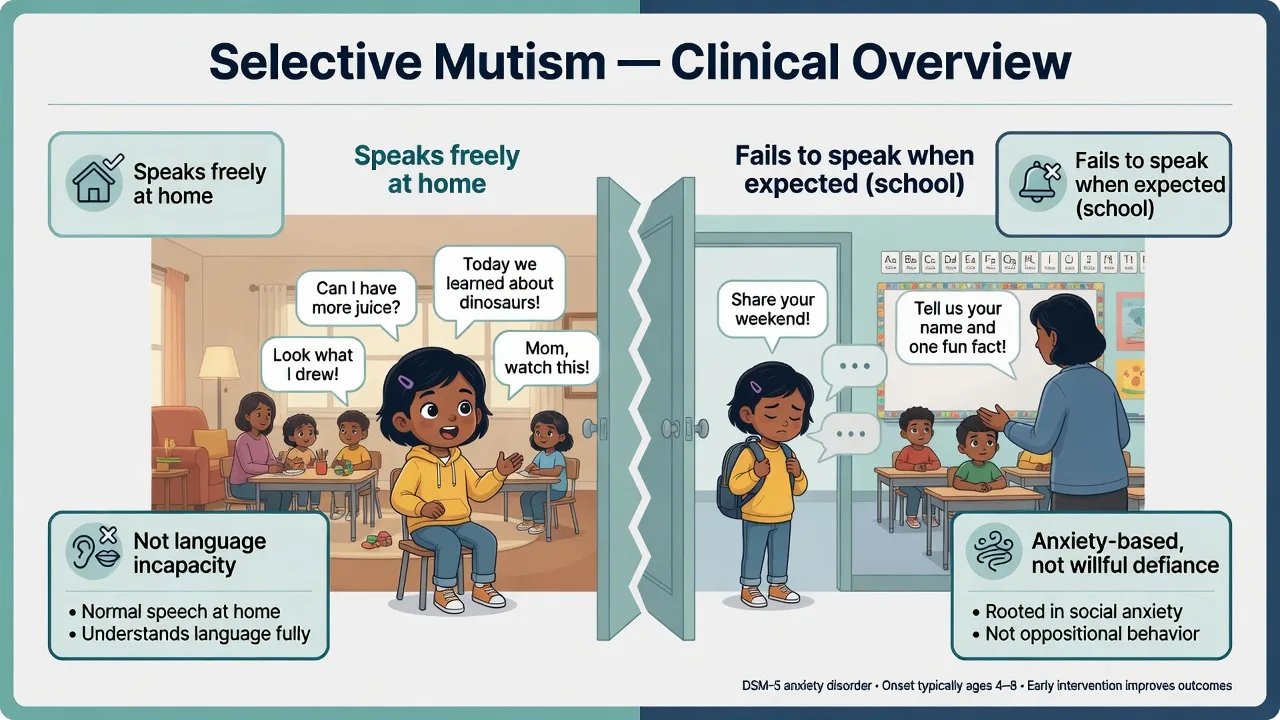
SM is a syndrome of consistent failure to speak in specific social situations in which speaking is expected, despite demonstrated ability to speak in other situations. The silence is context-bound, not a global absence of language capacity. Distress or functional interference is required. The clinical question is not "can this child produce words?" but "under what stimulus conditions does speech fail, and what maintains that pattern?"[1][2]
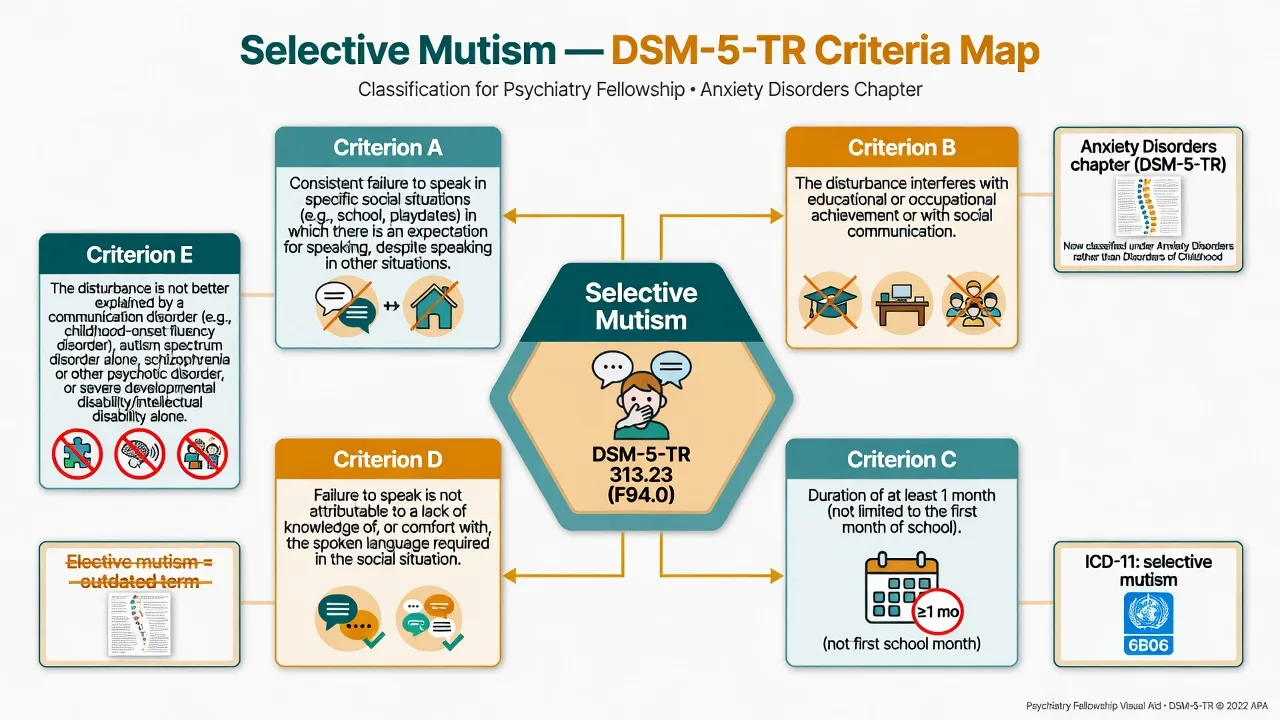
DSM-5-TR structure you must reproduce. (A) Consistent failure to speak in specific social situations in which there is an expectation for speaking (for example school) despite speaking in other situations. (B) The disturbance interferes with educational or occupational achievement or with social communication. (C) The duration of the disturbance is at least 1 month (not limited to the first month of school). (D) The failure to speak is not attributable to a lack of knowledge of, or comfort with, the spoken language required in the social situation. (E) The disturbance is not better explained by a communication disorder (for example childhood-onset fluency disorder) and does not occur exclusively during the course of autism spectrum disorder, schizophrenia, or another psychotic disorder.[1][2]
The examinable nosology shift. Earlier DSM framed "elective mutism" among other disorders of infancy, childhood, or adolescence and carried an oppositional connotation. DSM-5 renamed the disorder selective mutism, relocated it to the Anxiety Disorders chapter, and aligned it with social-evaluative fear and behavioural inhibition literature. Saying "elective" in a viva is a scoring liability unless you are correcting the historical term.[1][2]
ICD-11. Selective mutism emphasises marked selectivity of speaking that is inconsistent with language competence, is persistent, and causes impairment. When boards ask duration language, name the system — the DSM ≥1 month / not first school month rule remains the highest-yield multi-board trap.[2]
Classification
Selective mutism
- Speaks some settings
- Fails when speech expected
- ≥1 month duration rule
- Anxiety disorders chapter
Social anxiety (no SM)
- Fear of evaluation
- May still speak (softly)
- Avoidance broader
- Often comorbid with SM
Language / hearing
- Limited capacity across settings
- Not purely situational
- Needs SLP/audiology
- Can co-exist with SM
ASD / psychosis
- Broader social-comm deficits
- Restricted interests (ASD)
- Thought disorder rare youth
- SM not exclusive explanation
Severity is graded by number of mute contexts, school participation, need for others to speak for the child, multi-comorbidity, and risk — not by a laboratory value.[1][3]
Epidemiology and risk factors
Headline numbers every candidate must own
School-based sampling established that SM is uncommon but not mythical, and that affected children show substantial social anxiety and academic impact relative to peers. Onset is typically in early childhood; presentation to services often coincides with preschool or school entry when speech is demanded by non-family adults. Immigrant and bilingual populations show elevated rates in some series — criterion D exists specifically so examiners and clinicians do not mislabel ordinary second-language discomfort as SM.[1][3][11]
Risk factors include behavioural inhibition, parental and familial anxiety (including social anxiety), modelling of reticence, and environments that accommodate silence by answering for the child. Family studies support excess social anxiety among parents of children with SM.[1][11][12]
Pathophysiology
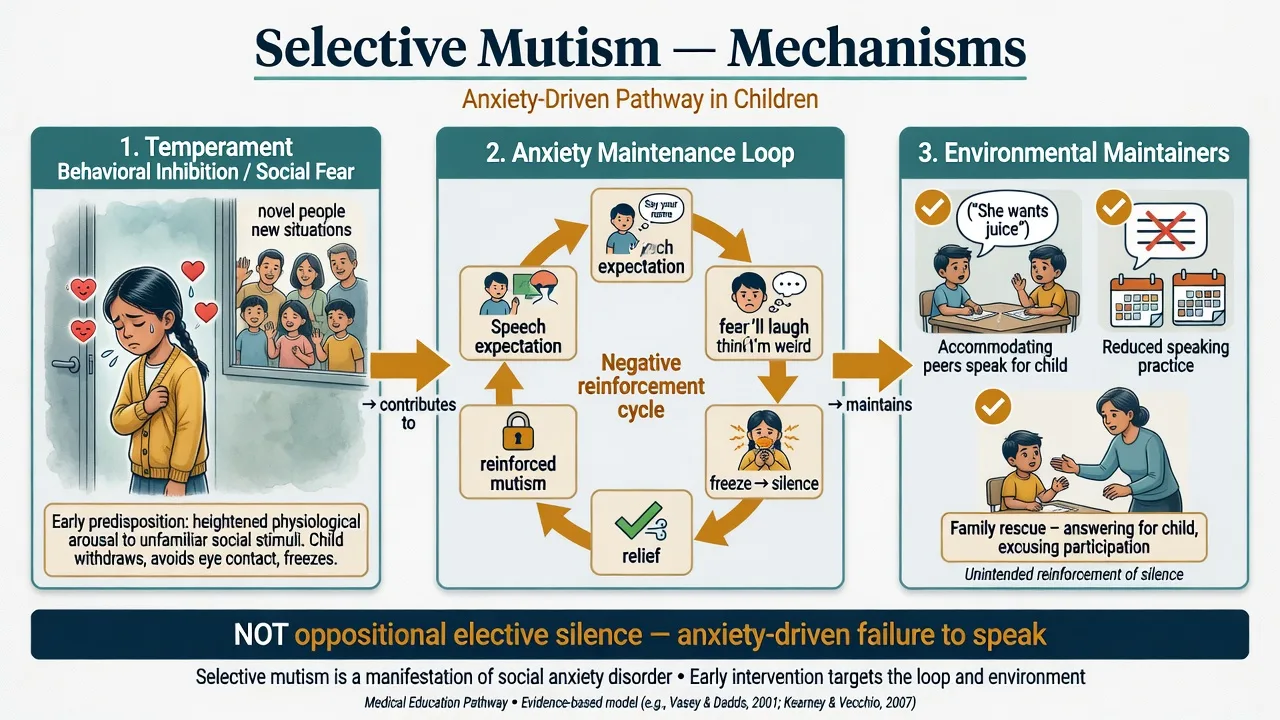
Anxiety and behavioural inhibition. Contemporary models place SM on a continuum with social-evaluative anxiety and temperamental inhibition to the unfamiliar. The child anticipates negative evaluation or inability to perform speech under scrutiny; physiological freezing and mutism reduce immediate distress and are therefore reinforced.[1][2][12]
Stimulus control of speech. Speech becomes under tight environmental control: high probability at home with selected people; near-zero probability with teachers, peers, or certain relatives. This is learning theory, not a character defect.[1][4]
Maintenance by accommodation. When classmates, parents, or teachers systematically speak for the child, the need to emit speech under anxiety is removed and extinction of mutism cannot occur. Well-meaning rescue is a maintaining factor — the same conceptual class as family accommodation in OCD or SeAD.[4][5][6]
Circuits (viva depth only). Group-level threat-appraisal models (amygdala-centred reactivity with insufficient top-down regulation) are discussed at fellowship level; imaging does not diagnose SM in an individual patient.[2][14]
Clinical presentation
Classic child. Speaks freely at home, may be "a chatterbox" with parents, yet produces no or minimal speech at school for months. May whisper to one peer, use gestures, pull a parent to answer, or freeze with a blank face when addressed by the teacher. Academic assessment is compromised because oral responses cannot be sampled.[1][3]
Associated features. Blushing, gaze aversion, rigidity, clinginess at drop-off, school-morning somatic complaints, and broader social anxiety symptoms. Some children speak to pets or soft toys more readily than to peers.[1][2]
MSE language. In clinic the child may be silent with the examiner yet animated with a parent behind a one-way observation or on home video. Affect is anxious/inhibited with strangers; thought form and content usually age-appropriate when speech is obtained in safe settings; insight limited in young children. Quote collateral: "She talks non-stop in the car but has not said a word to her teacher all term."[1][3]
Adolescents and residual patterns. Residual SM may present as extreme reluctance to speak in class, phone calls, or shops with high social anxiety — formulate whether residual SM criteria, pure SAD, or both apply.[2][12]
Differential diagnosis
SAD without SM
- Fear of scrutiny central
- Speech usually present
- Avoidance multi-domain
- High co-occurrence
ASD
- Broader social-comm deficits
- RRBs / sensory issues
- Speech oddities not only mute
- Can dual-diagnose carefully
Language / hearing
- Deficit across settings
- Audiology/SLP findings
- Criterion D language comfort
- Treat comorbidity
Trauma / ODD / psychosis
- Trauma-linked onset pattern
- ODD: wilful without freeze anxiety
- Psychosis: rare youth cluster
- Safeguarding if indicated
Discriminators score marks. Global language incapacity is not SM. Pure oppositional refusal without anxiety signs is not the default SM formulation. ASD may co-travel; SM does not "explain away" autism, and autism does not automatically absorb every instance of situational mutism.[1][2][12]
Clinical and bedside assessment
Structure the interview around a speech map: who, where, volume (full voice / whisper / non-verbal only), and since when. Confirm duration ≥1 month and that silence is not limited to the first month of school. Obtain language developmental history, bilingual exposure, hearing, trauma, bullying, ASD traits, family anxiety, and accommodation inventory (who answers for the child).[1][2][3]
Collateral is mandatory. Teacher report of speech frequency and peer interaction; home video demonstrating speech capacity; SLP when language disorder is possible. Clinic silence alone never proves SM without the multi-setting pattern.[3][4]
Measurement. Selective Mutism Questionnaire (SMQ) parent ratings and School Speech Questionnaire (SSQ) teacher ratings appear in treatment trials (including Bergman and Oerbeck packages) and support measurement-based care. Anxiety scales track comorbidity.[5][6][7]
Document risk (mainly via comorbid depression/hopelessness), safeguarding concerns, and assent/consent appropriate to age. Involuntary care for pure SM alone is rare; use local Mental Health Act principles only when comorbid risk and capacity thresholds are met — do not invent section numbers.[13]
Investigations
Audiology if hearing not recently documented. Speech-language evaluation when criterion D or developmental language concerns exist. Routine brain imaging or EEG is not indicated for classic early-onset SM. Investigate if language regression, focal neurology, or psychotic features appear. Baseline labs as indicated before SSRI pharmacotherapy; pregnancy testing when relevant in adolescents.[1][10][13]
Management — acute and safety
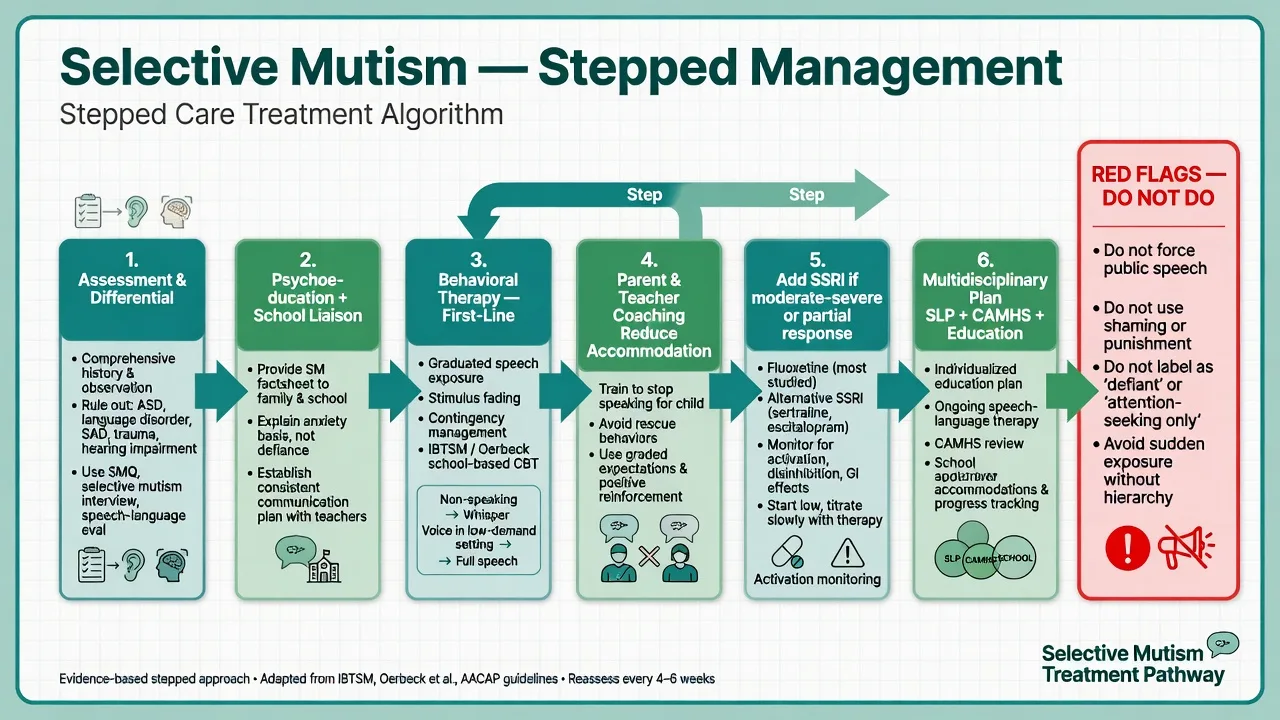
Do not force public speech. Forcing a child to perform under audience pressure is not graded exposure; it can intensify anxiety and confirm catastrophic predictions. Exposure is collaborative, hierarchical, and reinforced.[4][5]
Safeguarding and medical. If mutism onset maps to trauma, abuse, or severe neglect, prioritise protection pathways alongside anxiety care. If comorbid depression or SSRI activation with suicidal ideation emerges, same-day risk review.[10][13]
Management — definitive
Behavioural and CBT packages (first-line)
Psychoeducation for family and school: SM is anxiety-driven, not elective stubbornness. Build a speaking hierarchy (non-verbal responding → mouthing → whispering to parent in school → brief word to teacher → peer speech). Core techniques include stimulus fading (gradually introduce new listeners while speech is already occurring), shaping, contingency management, defocused communication, and dropping accommodation (others stop answering for the child). Sessions often need to occur in school, not only in clinic.[4][5][6]
Integrated Behavior Therapy for Selective Mutism (IBTSM). Bergman and colleagues' randomised controlled pilot (children aged 4–8, IBTSM versus waitlist) showed significant reductions in SM symptoms and gains in speech, supporting a manualised behavioural package with parent involvement and graduated verbal exposure tasks.[5]
Oerbeck home- and school-based intervention. A randomised controlled trial of a home- and school-based programme using defocused communication and behavioural techniques demonstrated increased speech versus waitlist, with greater gains in younger children — a direct early-intervention pearl. Longer-term follow-up work supports durability of gains for many treated children.[6][7]
Historical psychosocial literature (Cohan review) already favoured behavioural/cognitive-behavioural approaches over purely psychodynamic or non-specific therapy as the evidence-leaning lane — modern trials refine that trajectory.[4]
Pharmacotherapy — adjunct, not default monotherapy
For mild SM with good engagement, psychological/school intervention alone is preferred. For moderate–severe SM, multi-setting mutism, or partial psychological response, an SSRI may be added under specialist/CAMHS supervision within broader paediatric anxiety practice.[8][9][10][13]
Fluoxetine is the most studied agent in SM specifically. Black and Uhde's double-blind placebo-controlled study of fluoxetine in elective/selective mutism supported benefit with acceptable short-term safety signals for that era's sample. Dummit and colleagues' open trial reported improvement in children with SM and comorbid anxiety on fluoxetine. Kaakeh and Stumpf summarise SSRI-focused pharmacotherapy for SM with fluoxetine as the dominant studied option.[8][9][10]
Exam-level dosing example (specialist-supervised, individualised). Fluoxetine 5–10 mg orally once daily to start in young children (liquid formulations often used for fine titration), titrate slowly toward a tolerated effective paediatric range commonly discussed in the 10–20 mg/day order (individualise by age, weight, and response; some older youth require higher doses as in broader anxiety care). Monitor activation, suicidality, sleep, GI effects, and mania early after start/titration; review frequently in the first weeks. Do not declare failure before an adequate trial at a therapeutic dose with concurrent behavioural work. Other SSRIs may be considered by analogy to paediatric anxiety evidence when fluoxetine is unsuitable, with the same activation monitoring culture.[8][9][10][13]
Canadian anxiety CPGs and WFSBP anxiety guidance provide system-level context for CBT-first anxiety care and careful SSRI use; SM remains a specialist childhood anxiety niche within that framework.[13][14]
Regional notes
ANZ / FRANZCP. CAMHS or private child psychiatry/psychology with school liaison; GP shared care for uncomplicated recovery maintenance. Name jurisdiction-specific Mental Health Act only if comorbid high-risk illness meets coercion thresholds — pure SM rarely does.[5][6][13] UK / MRCPsych. NICE-aligned psychological first-line ethos for childhood anxiety; CASC tests plain-language explanation to parents that this is anxiety, not naughtiness, and that graded school speech practice is the plan.[4][13] US / ABPN. IBTSM and fluoxetine trial names are classic item material; DSM-5 anxiety-chapter placement is a definition item.[2][5][8] India / MD-DNB / NEET-SS. Expect criteria, duration trap, differentials (ASD, language), and behavioural-first then SSRI adjunct at viva.[1][2][4]
Subtypes and scenarios
- Preschool / nursery mutism: early intervention advantage (Oerbeck age effect).[6][7]
- School-entry classic: most common recognition; multi-agency plan.[3]
- SM + SAD: treat both strands; family anxiety loading common.[11][12]
- SM + ASD: dual formulation; adapt communication demands; do not collapse.[12]
- Bilingual families: apply criterion D rigorously before SM label.[1][2]
- Adolescent residual SM: transition planning; adult social anxiety continuity.[2]
- Treatment-resistant multi-setting mutism: intensify school-based exposure, review diagnosis, consider SSRI, specialist second opinion.[5][7][10]
Complications and pitfalls
Punitive "elective" framing; public forcing of speech; missing hearing/language/ASD; colluding with peers and parents who permanently speak for the child; single under-dosed clinic session labelled as failed CBT; SSRI without activation monitoring; ignoring parental anxiety that models and maintains silence; cultural misreading of quietness without impairment criteria.[1][4][10][12]
Prognosis and disposition
Untreated SM can persist with academic under-achievement and entrenched social anxiety. With early school-inclusive behavioural treatment, many children increase speech; younger age predicts better response in key trial data. Residual social anxiety is common and may need ongoing care. Oerbeck 5-year follow-up work is a high-yield evidence pearl for durability discussions. Disposition: psychology/CAMHS plus school plan first-line; step up for non-response, high comorbidity, safeguarding, or severe multi-setting mutism.[5][6][7]
Special populations
Very young children. Confirm developmental language milestones before SM diagnosis; early behavioural work preferred.[1][6]
Bilingual / immigrant families. Criterion D; cultural safety; interpreter use that does not permanently replace the child's own speech goals.[1][2]
Intellectual disability. Adapted hierarchy, carer coaching, realistic communication goals, capacity-informed care.[4]
Indigenous ANZ and cultural formulation. Quietness may be culturally patterned; require impairment and selective pattern, not stereotype. Use culturally safe engagement and local supports.[13]
Adolescents and transition. Residual mutism, phone/shop speaking hierarchies, SSRI stewardship, and adult service handover when needed.[2][10]
Evidence and guidelines
Landmark pillars: Viana integrative review; Muris and Ollendick DSM-5 anxiety reclassification review; Bergman school prevalence; Cohan psychosocial interventions review; IBTSM RCT pilot (Bergman 2013); Oerbeck RCT and 5-year follow-up; Black fluoxetine RCT; Dummit open fluoxetine series; Kaakeh SSRI focus; Chavira family SAD study; Muris SM–SAD–ASD relations; Canadian CPG and WFSBP anxiety guidelines for system context.[1][2][3][4][5][6][7][8][9][10][11][12][13][14]
Exam pearls
MUTE — selective mutism checklist
References
- [1]Viana AG, Beidel DC, Rabian B Selective mutism: a review and integration of the last 15 years Clin Psychol Rev, 2009.PMID 18986742
- [2]Muris P, Ollendick TH Children Who are Anxious in Silence: A Review on Selective Mutism, the New Anxiety Disorder in DSM-5 Clin Child Fam Psychol Rev, 2015.PMID 25724675
- [3]Bergman RL, Piacentini J, McCracken JT Prevalence and description of selective mutism in a school-based sample J Am Acad Child Adolesc Psychiatry, 2002.PMID 12162629
- [4]Cohan SL, Chavira DA, Stein MB Practitioner review: Psychosocial interventions for children with selective mutism: a critical evaluation of the literature from 1990-2005 J Child Psychol Psychiatry, 2006.PMID 17076747
- [5]Bergman RL, Gonzalez A, Piacentini J, Keller ML Integrated Behavior Therapy for Selective Mutism: a randomized controlled pilot study Behav Res Ther, 2013.PMID 23933108
- [6]Oerbeck B, Stein MB, Wentzel-Larsen T, Langsrud Ø, Kristensen H A randomized controlled trial of a home and school-based intervention for selective mutism - defocused communication and behavioural techniques Child Adolesc Ment Health, 2014.PMID 32878377
- [7]Oerbeck B, Overgaard KR, Stein MB, Pripp AH, Kristensen H Treatment of selective mutism: a 5-year follow-up study Eur Child Adolesc Psychiatry, 2018.PMID 29357099
- [8]Black B, Uhde TW Treatment of elective mutism with fluoxetine: a double-blind, placebo-controlled study J Am Acad Child Adolesc Psychiatry, 1994.PMID 7961338
- [9]Dummit ES 3rd, Klein RG, Tancer NK, Asche B, Martin J Fluoxetine treatment of children with selective mutism: an open trial J Am Acad Child Adolesc Psychiatry, 1996.PMID 8935208
- [10]Kaakeh Y, Stumpf JL Treatment of selective mutism: focus on selective serotonin reuptake inhibitors Pharmacotherapy, 2008.PMID 18225967
- [11]Chavira DA, Shipon-Blum E, Hitchcock C, Cohan S, Stein MB Selective mutism and social anxiety disorder: all in the family? J Am Acad Child Adolesc Psychiatry, 2007.PMID 18049296
- [12]Muris P, Ollendick TH Selective Mutism and Its Relations to Social Anxiety Disorder and Autism Spectrum Disorder Clin Child Fam Psychol Rev, 2021.PMID 33462750
- [13]Katzman MA, Bleau P, Blier P, Chokka P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders BMC Psychiatry, 2014.PMID 25081580
- [14]Bandelow B, Allgulander C, Baldwin DS, Costa DLDC, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for treatment of anxiety, obsessive-compulsive and posttraumatic stress disorders - Version 3. Part I: Anxiety disorders World J Biol Psychiatry, 2023.PMID 35900161