Psych · General adult psychiatry — anxiety disorders
Separation anxiety disorder
Also known as SeAD · Adult separation anxiety disorder (ASAD) · Separation anxiety disorder of childhood (historical framing) · School refusal — separation pathway
Exam-exhaustive fellowship reference on separation anxiety disorder across the lifespan — DSM-5-TR and ICD-11 criteria, child vs adult duration thresholds, removal of onset-before-18 rule, NCS-R/WMH epidemiology, adult under-recognition, attachment and maintenance mechanisms, panic and grief comorbidity, differentials, family-based CBT and graded separation exposure, SSRI role with paediatric trial anchors (CAMS, fluoxetine), and multi-board stepped care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Separation anxiety disorder (SeAD) is the most familiar “childhood” anxiety label that fellowship examiners now weaponise as a lifespan disorder. FRANZCP MEQs and MRCPsych CASC reward criteria with duration by age band, adult attachment figures (partner, children), family accommodation as a maintaining factor, and the explicit statement that adult SeAD is still missed in clinic. ABPN items test the panic-link literature and paediatric combination treatment (CAMS). MD/DNB vivas expect the eight symptom domains and school-refusal differentials cold.[1][4][6][11]
Overview and definition
SeAD is a syndrome of developmentally inappropriate and excessive fear or anxiety concerning separation from those to whom the individual is attached. Fear, anxiety, or avoidance is persistent, causes clinically significant distress or impairment, and is not better explained by another mental disorder. The core clinical question is not “is the person attached?” but whether separation cues trigger out-of-proportion alarm, avoidance of independent function, and disability relative to developmental and cultural expectations.[3][4][5]
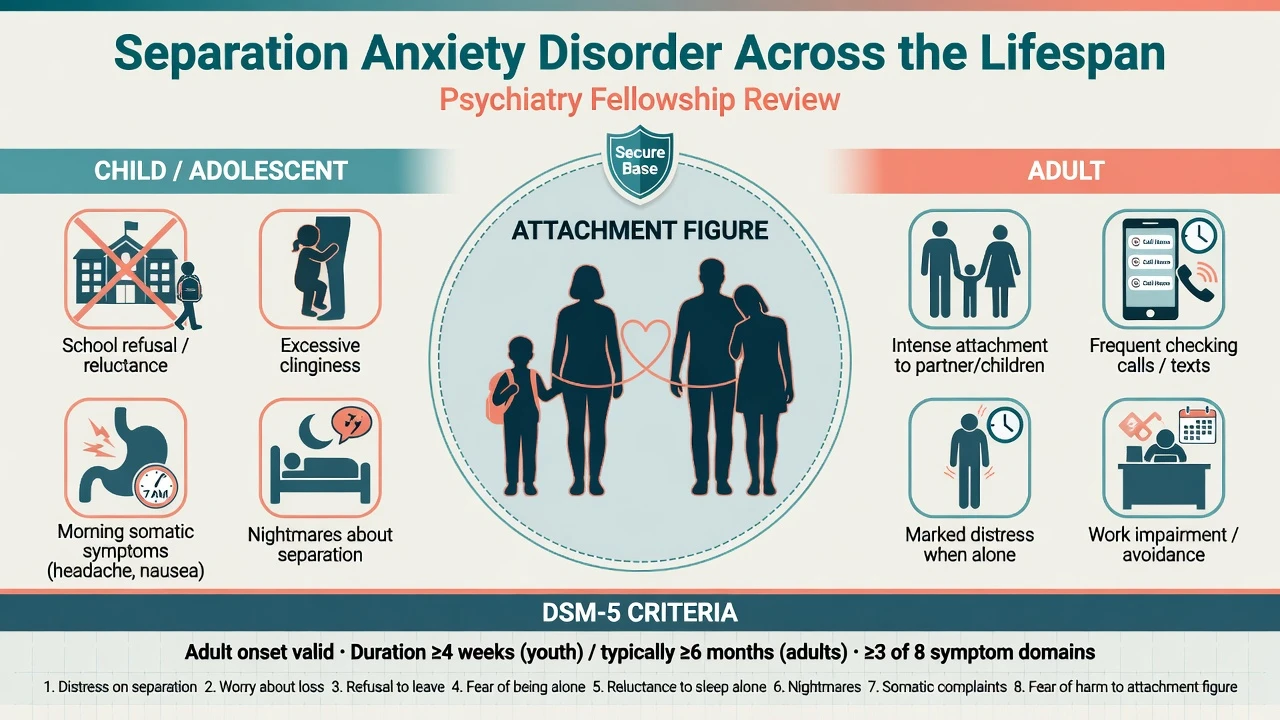
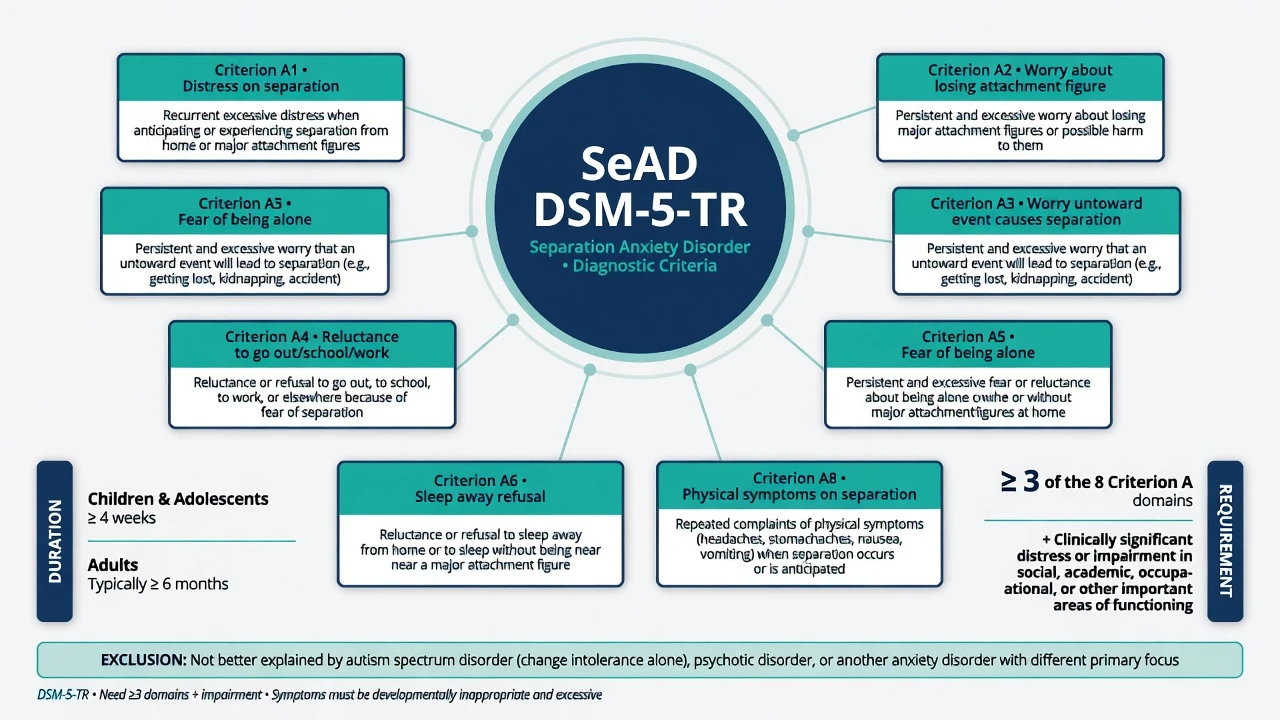
DSM-5-TR structure you must reproduce. Developmentally inappropriate and excessive fear or anxiety concerning separation from attachment figures, evidenced by at least three of eight domains: (1) recurrent excessive distress when anticipating or experiencing separation; (2) persistent and excessive worry about losing major attachment figures or about possible harm to them; (3) persistent and excessive worry about experiencing an untoward event that causes separation; (4) persistent reluctance or refusal to go out, away from home, to school, to work, or elsewhere because of fear of separation; (5) persistent and excessive fear of or reluctance about being alone or without major attachment figures at home or in other settings; (6) persistent reluctance or refusal to sleep away from home or to go to sleep without being near a major attachment figure; (7) repeated nightmares involving the theme of separation; (8) repeated complaints of physical symptoms when separation from major attachment figures occurs or is anticipated. Duration: at least 4 weeks in children and adolescents and typically 6 months or more in adults. Distress or impairment required. Not better explained by another mental disorder (for example autism-related change resistance alone, psychosis-related fears, agoraphobia without separation focus, or generalised anxiety without separation predominance).[3][4]
The examinable DSM-5 shift. Earlier DSM editions framed SeAD as a disorder usually first diagnosed in infancy, childhood, or adolescence and required onset before 18 years in a way that systematically suppressed adult recognition. DSM-5 lifted the age-of-onset restriction, relocated SeAD into the Anxiety Disorders chapter, and made explicit that the disorder can begin in adulthood. Adult attachment figures are often spouses, partners, or children rather than only parents.[3][4][5][6]
ICD-11. Separation anxiety disorder emphasises marked and excessive fear or anxiety about separation from attachment figures that is out of proportion to the situation and developmental context, with avoidance or endurance under distress and clinically significant impairment. When duration language is examined, name which system you are applying — the child/adolescent 4-week versus adult typically 6-month DSM thresholds remain the highest-yield multi-board anchors.[3][4]
Classification
Youth SeAD
- Duration ≥4 weeks
- Attachment figures usually parents/caregivers
- School refusal/reluctance common
- Somatic morning symptoms classic
Adult SeAD
- Duration typically ≥6 months
- Partner/children often primary figures
- Checking, travel refusal, cannot be alone
- Still widely under-diagnosed
Normal attachment
- Developmentally expected protest
- Settles with support/time
- No marked impairment threshold
- Cultural norms matter
Related traps
- Dependent personality ≠ SeAD
- Panic-when-alone may still be SeAD
- Grief/PTSD can co-travel
- ASD change intolerance alone ≠ SeAD
Severity is graded by avoidance breadth, school/work days lost, accommodation intensity, multi-comorbidity load, and risk — not by a laboratory value.[4][5][6]
Epidemiology and risk factors
Headline numbers every candidate must own
NCS-R data established that adult SeAD is not rare and that most adult cases do not simply represent untreated childhood persistence. World Mental Health survey analyses confirm cross-national burden with both paediatric-onset and adult-onset pathways and associations with childhood adversities and traumatic exposures. Anxiety-clinic samples report substantial rates of adult SeAD among patients already labelled with other anxiety diagnoses — a direct service-level warning about dual diagnosis and formulation quality.[1][2][6][7]
Risk factors include behavioural inhibition, anxious attachment patterns, parental anxiety and accommodation, loss, divorce, migration, family conflict, and trauma. SeAD is among the most common anxiety presentations in children younger than 12 in many clinical series; in adults it is commoner than many registrars expect because it is not on their default checklist.[1][2][4][5]
Pathophysiology
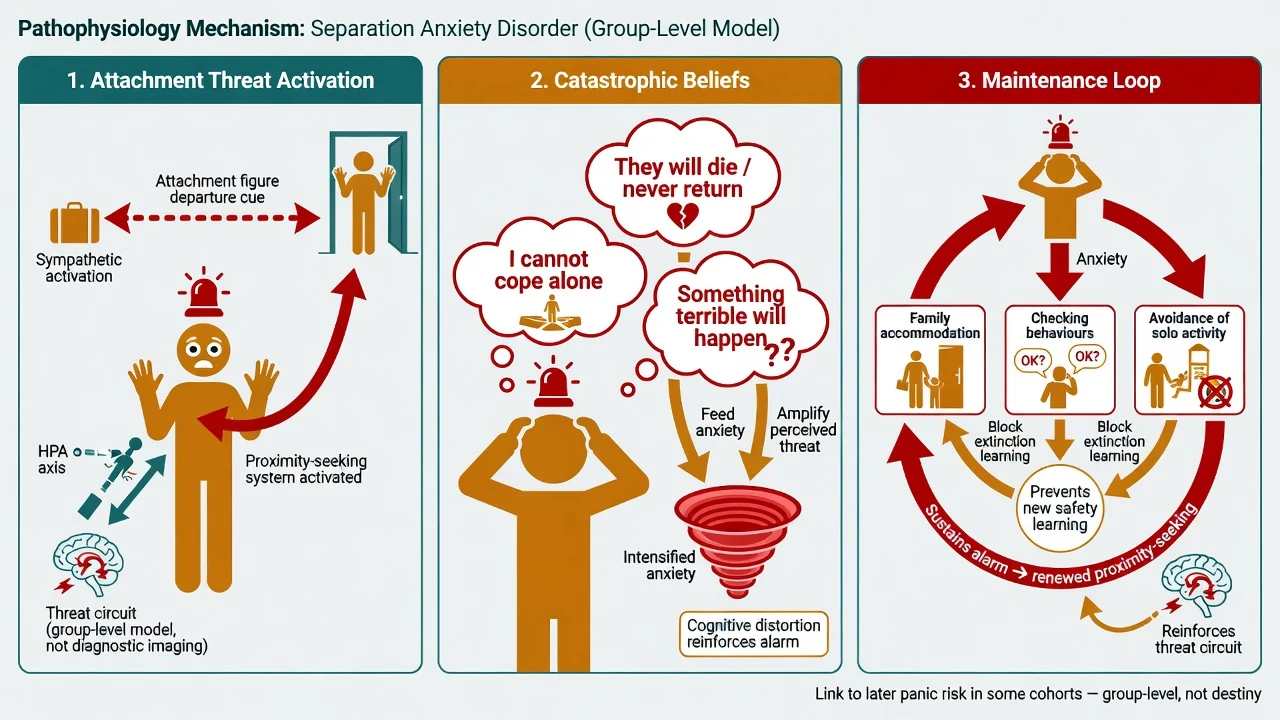
Attachment-system framing (clinical, not pop psychology). Separation from an attachment figure activates proximity-seeking and threat appraisal. In SeAD the threshold for alarm is lowered and the predicted cost of separation is inflated (“they will die”; “I cannot survive alone”). Adult presentations re-map the same system onto partners and offspring.[4][5][9]
Acquisition and cognitive content. Direct loss experiences, vicarious threat learning, and parental modelling of catastrophic separation appraisals contribute. Children with SeAD show threat-laden cognitions about harm and coping failure; parents often hold beliefs that the child cannot cope without them, which fuels accommodation.[4][9][10]
Maintenance. Reassurance-seeking, frequent checking (calls, location tracking), refusal of solo sleep or travel, and family rearrangements that remove every separation opportunity prevent extinction. This is why “being kind” without a graded plan can become iatrogenic chronicity.[4][10]
Circuits (viva depth, not diagnostic imaging). Group-level models emphasise amygdala-centred threat appraisal with insufficient prefrontal regulation and autonomic arousal during separation cues. Imaging does not diagnose SeAD in an individual patient.[9][14]
Panic interface. The historical separation-anxiety hypothesis of panic has meta-analytic support that childhood SeAD elevates later panic risk, without meaning every panic patient “was a clingy child” or that SeAD and panic are the same disorder. Adult patients may present with panic attacks when alone whose cognitive content is still attachment-harm or inability to cope without the figure — formulate both strands.[8][9]
Clinical presentation
Children. Excessive distress at school drop-off, shadowing parents at home, refusal of playdates/camps, nightmares with separation themes, and recurrent abdominal pain or headache on school mornings that improve when allowed to stay home. Teachers report clinginess to a preferred adult and inability to settle after the parent leaves.[1][4][10]
Adolescents. May intellectualise (“I just prefer being home”) while refusing school trips, sleeping alone, or allowing parents to travel. Excessive texting and location-checking are modern safety behaviours.[4][5]
Adults. Marked distress when a partner works away, inability to be alone at home, repeated calls, travel refusal, or over-involvement that impairs work. Attachment figures may be spouse, romantic partner, adult children, or parents. Onset may follow loss, relationship threat, migration, or medical illness in the attachment figure. Adult SeAD remains under-recognised in clinical practice despite DSM-5 clarification.[4][5][6][7]
MSE language. Anxious affect when separation is discussed; thought content of catastrophe to self or attachment figure; perception normal; cognition intact; insight partial to good. Quote the patient’s words (for example “If she flies I know the plane will crash and I will not cope”).[4][5]
Differential diagnosis
GAD
- Worry multi-domain
- Not predominantly separation-linked
- Can co-occur
- Ask what worry is about first
Panic / agoraphobia
- Fear of panic sensations or escape
- Multiple situation classes
- May co-occur with SeAD
- Alone-panic can still be SeAD-content
Social anxiety
- Fear of scrutiny/evaluation
- Not primarily attachment separation
- School refusal can be either/both
- Performance vs cling content
Personality / other
- Dependent PD: pervasive interpersonal pattern
- ASD: change intolerance broader
- PTSD/grief: trauma-loss cluster
- Psychosis: delusional harm beliefs
Discriminators score marks. School refusal is a behaviour, not a diagnosis — map SeAD, social anxiety, depression, bullying, learning disorder, and medical illness. Dependent personality describes enduring interpersonal patterns across contexts; SeAD is an anxiety syndrome organised around separation threat and can exist with or without personality pathology.[4][5][8][13]
Clinical and bedside assessment
Structure the interview: map attachment figures; walk the eight symptom domains; confirm duration by age band; onset pathway (childhood persistence vs adult-onset); safety behaviours and family accommodation; school attendance or work function; sleep arrangements; checking frequency; trauma/loss timeline; depression and suicide risk; substances; prior therapy quality.[1][4][6]
Document MSE and risk. Suicide risk is driven mainly by comorbid depression, hopelessness, and academic/relationship collapse, not by the SeAD label alone. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles when risk and capacity thresholds are met — statutes are jurisdiction-specific; do not invent section numbers.[13][14]
Measurement. DSM-5 severity measures for separation anxiety disorder (child and adult versions) support monitoring. Adult symptom questionnaires such as ASA-27 concepts appear in research and specialised assessment. Youth broadband anxiety screens (for example SCARED/RCADS-type tools) help case-finding but do not replace criteria. Build a separation hierarchy with SUDs (0–100) for exposure work.[4][5][13]
Investigations
Routine neuroimaging is not indicated for classic SeAD. Investigate somatic complaints when red flags suggest organic disease. Obtain baseline labs and ECG as clinically indicated before SSRI therapy (age, cardiac history, overdose risk, polypharmacy). Measurement-based care tracks school days attended, minutes alone tolerated, checking counts, and PHQ-9/GAD-7 for comorbidity.[11][13][14]
Management — acute and safety
Acute separation meltdown (drop-off, partner departure). Validate distress, keep the plan predictable, avoid both harsh forced extinction without preparation and total capitulation that resets learning. Short-term safety first; then resume graded steps.[10][13]
Suicidal crisis or SSRI activation. Same-day risk assessment, safety plan, caregiver involvement for youth, and early review after antidepressant initiation — especially under 25 years where activation and suicidal ideation monitoring is mandatory exam language.[11][12][14]
Management — definitive
Psychological therapy (first-line)
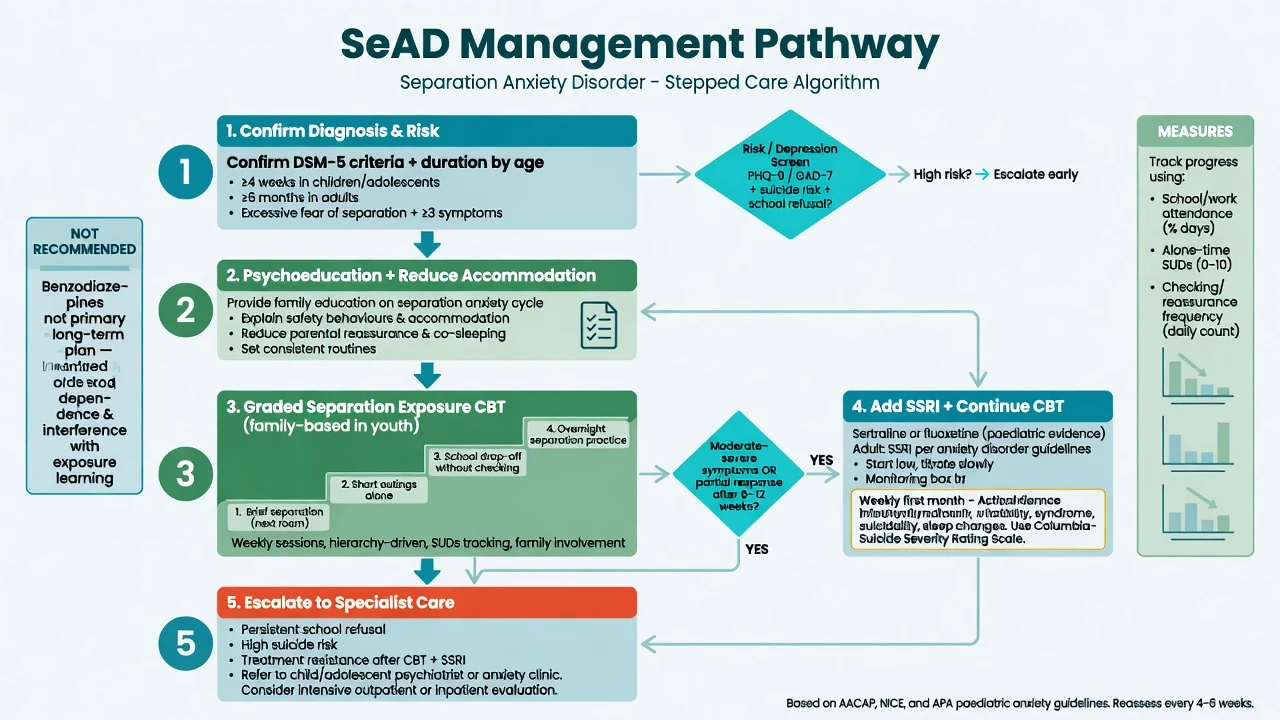
Core ingredients. Psychoeducation on attachment-threat and maintenance; collaborative hierarchy of separation situations; in vivo graded exposure to being alone, school/work attendance, sleep separation, and attachment-figure absences; cognitive work on probability/cost of catastrophe; response prevention for checking and reassurance; planned reduction of family accommodation with caregiver coaching.[4][10][13]
Youth-specific evidence. Family-based cognitive-behavioural treatment targeting separation anxiety has randomised support compared with a more generic anxiety program in school-age children, underscoring that SeAD-focused family work is not optional padding.[10]
Adult work. Exposure to solo time and attachment-figure absence with strict limits on checking; couple/family sessions when accommodation is systemic; treat comorbid panic, depression, and grief explicitly. Adult SeAD will not improve if the formulation never names separation fear and only titrates an SSRI for “GAD.”[4][5][6][9]
Long-term CBT outcome literature for anxiety-related disorders supports durability when treatment quality is adequate; residual avoidance predicts return of fear — plan booster separations after holidays and illness.[13][14]
Pharmacotherapy
There is no medication with a unique SeAD-only labelled monopoly in the way candidates sometimes invent; use the anxiety-disorder evidence base. SSRIs are the first-line medication class when severity, comorbidity, or incomplete psychological response warrants medication.[11][12][13][14]
Paediatric anchors (must be examinable). The CAMS trial in childhood anxiety disorders (including separation, social, and generalised anxiety) found that combination CBT plus sertraline was superior to either monotherapy, with both active treatments superior to placebo on primary outcomes. In CAMS-style practice, sertraline is commonly started at 25 mg orally once daily in youth and titrated under specialist supervision toward an effective tolerated range often 50–200 mg/day, with monitoring for activation, suicidality, sleep change, headache, and gastrointestinal effects.[11]
Fluoxetine has randomised placebo-controlled support in childhood anxiety disorders: typical exam-level framing is start 10 mg orally once daily, with titration (commonly toward 10–20 mg/day or higher as protocolised and tolerated in trial contexts) and the same activation/suicidality review discipline.[12]
Adults. When medication is indicated, use SSRI dosing as for other anxiety disorders — for example sertraline 25–50 mg orally daily starting dose, titrate toward 50–200 mg/day; or escitalopram 5–10 mg orally daily start toward 10–20 mg/day — review early for activation and suicide risk, then at 4–6 weeks for response, with longer courses for anxiety than for a brief reactive stressor. SNRIs are alternatives when SSRIs fail or are not tolerated, consistent with broad anxiety guidelines.[13][14]
Benzodiazepines. Not a primary long-term plan. Short-term bridging in rare selected crises risks dependence and can blunt extinction learning if used as the main strategy. Prefer skills, exposure, and SSRI/CBT pathways.[13][14]
Regional notes
ANZ / FRANZCP. Adult SeAD under-recognition is an ANZ academic theme — name attachment figures and duration explicitly in formulations. Route youth through CAMHS/psychology; adult community and private psychology for exposure work; GP shared care for SSRI monitoring.[6][13] UK / MRCPsych. NICE-aligned psychological first-line ethos for child anxiety; CASC tests plain-language explanation of school return plans and why indefinite parental bed-sharing is not the treatment.[10][13] US / ABPN. CAMS combination superiority and adult-onset validity after DSM-5 are classic items; panic-link meta-analysis is an advanced pearl.[8][11] India / MD-DNB / NEET-SS. Expect eight domains, dual duration thresholds, school-refusal differentials, and SSRI start doses at viva.[3][4][11]
Subtypes and scenarios
- Primary-school SeAD with school refusal: family-based CBT, graded classroom return, medical review of somatic symptoms as needed.[10][11]
- Adolescent nocturnal/trip refusal: hierarchy including sleep-alone steps and short overnight exposures.[4][10]
- Adult-onset after loss or migration: screen grief, PTSD, and depression; still treat separation exposure actively.[2][5][6]
- SeAD plus panic when alone: dual formulation; interoceptive work if panic maintenance is active; do not drop separation targets.[8][9]
- Complicated grief interface: separation fears and reunion yearning can entangle — treat both processes.[5][9]
- Perinatal: distinguish normal protective bonding from impairing inability to tolerate any separation; prefer psychological first-line; medication only with perinatal risk-benefit framing.[13][14]
Complications and pitfalls
Missing adult SeAD; colluding with lifelong accommodation; mislabelling as dependent personality only; chronic benzodiazepines; under-dosed “try one drop-off” exposures labelled as failed CBT; ignoring depression and suicide risk; over-pathologising culturally normative interdependence without impairment; failing to liaise with schools.[4][6][10][13]
Prognosis and disposition
Childhood SeAD may remit, persist into adulthood, or evolve into other anxiety and mood disorders. Early quality treatment improves attendance and family function. Adult SeAD often becomes chronic when unrecognised; response improves when separation exposure and comorbidity are both treated. Mild-moderate cases suit primary care plus psychology; specialist CAMHS or adult anxiety pathways for entrenched school refusal, high suicide risk, complex trauma, or failed adequate trials.[1][2][4][10][11]
Special populations
Preschool and school-age. Developmental norms for separation protest are higher in toddlers — require intensity, persistence, and impairment for disorder threshold.[3][4]
Intellectual disability and autism. Adapted hierarchies, visual supports, carer coaching; do not equate change intolerance alone with SeAD, but do not miss true separation fear when present.[4][13]
Older adults. Late-life attachment anxiety when a spouse is hospitalised; medical mimics; falls and confusion risk with benzodiazepines.[13][14]
Pregnancy and lactation. Prefer exposure-based psychological care; if SSRI needed, use perinatal psychiatry principles and shared decision-making rather than abrupt untreated severe illness.[13][14]
Cultural formulation. Expected interdependence varies; diagnose on impairment and excess relative to cultural context. Indigenous ANZ care requires cultural safety and appropriate family engagement.[2][6]
Evidence and guidelines
Epidemiology anchors: Shear NCS-R; Silove WMH paediatric- and adult-onset analyses; clinic prevalence work from Silove and colleagues. Nosology: Bögels adult SeAD review; Silove lifespan DSM-5 commentary; Manicavasagar adult SeAD syntheses and ANZ under-recognition argument. Mechanisms and comorbidity: Kossowsky panic meta-analysis; Milrod pathogenesis framing. Treatment: Schneider family-based CBT RCT for child SeAD; CAMS (CBT, sertraline, combination); Birmaher fluoxetine childhood anxiety trial; Canadian anxiety CPG and WFSBP anxiety guidelines for system-level stepped care and pharmacologic class positioning.[1][2][4][5][8][10][11][12][13][14]
Exam pearls
SEPARATE — SeAD checklist
References
- [1]Shear K, Jin R, Ruscio AM, Walters EE, Kessler RC Prevalence and correlates of estimated DSM-IV child and adult separation anxiety disorder in the National Comorbidity Survey Replication Am J Psychiatry, 2006.PMID 16741209
- [2]Silove D, Alonso J, Bromet E, Gruber M, et al. Pediatric-Onset and Adult-Onset Separation Anxiety Disorder Across Countries in the World Mental Health Survey Am J Psychiatry, 2015.PMID 26046337
- [3]Silove D, Rees S Separation anxiety disorder across the lifespan: DSM-5 lifts age restriction on diagnosis Asian J Psychiatr, 2014.PMID 25453710
- [4]Bögels SM, Knappe S, Clark LA Adult separation anxiety disorder in DSM-5 Clin Psychol Rev, 2013.PMID 23673209
- [5]Manicavasagar V, Marnane C, Pini S, Abelli M, et al. Adult separation anxiety disorder: a disorder comes of age Curr Psychiatry Rep, 2010.PMID 20552302
- [6]Manicavasagar V, Silove D Why are we still missing adult separation anxiety disorder in clinical practice? Aust N Z J Psychiatry, 2016.PMID 27343899
- [7]Silove DM, Marnane CL, Wagner R, Manicavasagar VL The prevalence and correlates of adult separation anxiety disorder in an anxiety clinic BMC Psychiatry, 2010.PMID 20219138
- [8]Kossowsky J, Pfaltz MC, Schneider S, Taeymans J, et al. The separation anxiety hypothesis of panic disorder revisited: a meta-analysis Am J Psychiatry, 2013.PMID 23680783
- [9]Milrod B, Markowitz JC, Gerber AJ, Cyranowski J, et al. Childhood separation anxiety and the pathogenesis and treatment of adult anxiety Am J Psychiatry, 2014.PMID 24129927
- [10]Schneider S, Blatter-Meunier J, Herren C, In-Albon T, et al. The efficacy of a family-based cognitive-behavioral treatment for separation anxiety disorder in children aged 8-13: a randomized comparison with a general anxiety program J Consult Clin Psychol, 2013.PMID 23607501
- [11]Walkup JT, Albano AM, Piacentini J, Birmaher B, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety N Engl J Med, 2008.PMID 18974308
- [12]Birmaher B, Axelson DA, Monk K, Kalas C, et al. Fluoxetine for the treatment of childhood anxiety disorders J Am Acad Child Adolesc Psychiatry, 2003.PMID 12649628
- [13]Katzman MA, Bleau P, Blier P, Chokka P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders BMC Psychiatry, 2014.PMID 25081580
- [14]Bandelow B, Allgulander C, Baldwin DS, Costa DLDC, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for treatment of anxiety, obsessive-compulsive and posttraumatic stress disorders - Version 3. Part I: Anxiety disorders World J Biol Psychiatry, 2023.PMID 35900161