Psych · General adult psychiatry — anxiety disorders
Social anxiety disorder
Also known as Social phobia · SAD · Generalised social anxiety disorder · Performance-only social anxiety · Fear of negative evaluation
Exam-exhaustive fellowship reference on social anxiety disorder — DSM-5-TR and ICD-11 criteria; performance-only specifier; epidemiology; Clark and Wells cognitive model; differentials including AVPD and ASD; LSAS SPIN Mini-SPIN; CBT exposure and CBGT; SSRI/SNRI dosing; phenelzine and moclobemide; benzodiazepine limits; refractory pathways; NICE/Canadian/WFSBP/ANZ stepped care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Social anxiety disorder (SAD; social phobia) is a high-yield general adult anxiety topic. FRANZCP MEQs demand criteria including the performance-only specifier, organic/substance exclusion, named CBT ingredients, and a drug with dose. MRCPsych CASC tests plain-language explanation of fear of negative evaluation, medication counselling, and why alcohol is not treatment. ABPN items test LSAS/SPIN concepts, SSRI evidence, and CBGT versus phenelzine history. This topic is written so a candidate who has read nothing else can answer those questions at consultant depth.[1][2][5]
Overview and definition
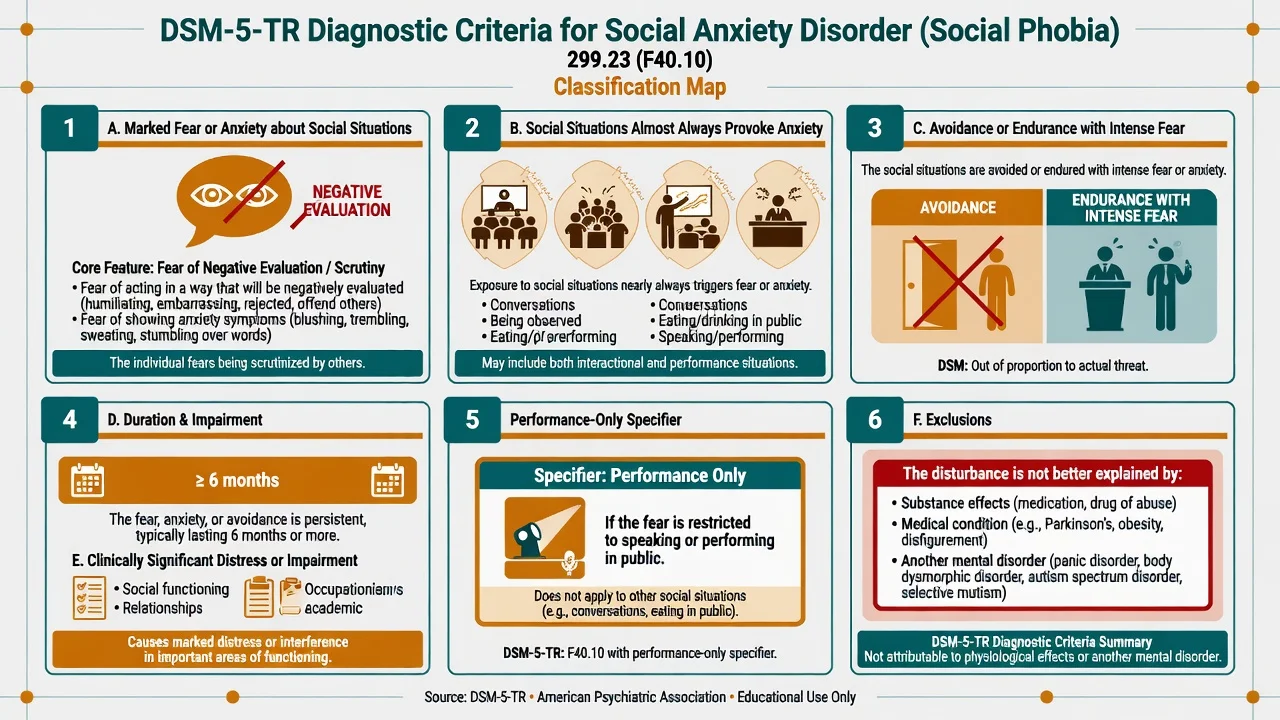
SAD is a syndrome of marked fear or anxiety about social situations in which the person is exposed to possible scrutiny by others, driven by fear of negative evaluation (humiliation, embarrassment, rejection, or offending others). Feared situations almost always provoke anxiety; they are avoided or endured with intense fear; the fear is out of proportion to the actual threat and sociocultural context; it is persistent (typically 6 months or more); and it causes clinically significant distress or impairment — after substance effects, medical mimics, and competing mental disorders have been reasonably excluded.[1][2][3]
DSM-5-TR structure you must reproduce. Marked fear or anxiety about one or more social situations in which the individual is exposed to possible scrutiny by others (for example social interactions, being observed, and performing in front of others). The individual fears that they will act in a way or show anxiety symptoms that will be negatively evaluated. The social situations almost always provoke fear or anxiety. The situations are avoided or endured with intense fear or anxiety. The fear or anxiety is out of proportion to the actual threat posed by the social situation and to the sociocultural context. The fear, anxiety, or avoidance is persistent, typically lasting 6 months or more. The fear, anxiety, or avoidance causes clinically significant distress or impairment. The disturbance is not attributable to a substance or another medical condition, and is not better explained by another mental disorder (for example panic disorder, body dysmorphic disorder, autism spectrum disorder). If another medical condition is present (for example Parkinson disease, obesity, disfigurement from burns), the fear/anxiety/avoidance is clearly unrelated or is excessive.[2][3]
Performance-only specifier. Specify if the fear is restricted to speaking or performing in public. Interactional situations (conversations, parties, eating with others) are not the focus. This specifier matters for formulation, beta-blocker discussion in selected performance contexts, and not over-pathologising normal stage nerves without impairment — but examiners still expect full criteria for the disorder label.[2][3]
ICD-11. Social anxiety disorder emphasises marked and excessive fear or anxiety that occurs consistently in one or more social situations such as social interactions, being observed, or performing in front of others, with concern about negative evaluation and avoidance or endurance with intense distress, plus duration and impairment thresholds in the manual you are using. When duration language is examined, name which system you are applying — DSM-5-TR’s typically-6-months threshold is the classic exam anchor.[1][2]
Classification
Core criteria spine
- Fear of scrutiny / negative evaluation
- Social situations almost always provoke anxiety
- Avoidance or endurance with intense fear
- Typically ≥6 months + distress/impairment
Situation types
- Interaction (conversations, parties)
- Observation (eating, writing, being watched)
- Performance (speaking, exams, music)
- Performance-only specifier if restricted
Exclusions
- Substance-induced (alcohol, stimulants)
- Medical (e.g. essential tremor-related secondary fear)
- Better explained by panic, BDD, ASD, psychosis, depression alone
Related constructs
- Normal shyness without impairment
- Avoidant personality (traits may coexist)
- Selective mutism continuum in youth
- Stage fright without disorder threshold
Severity in practice is graded by breadth of feared situations, degree of avoidance, disability, comorbidity and risk rather than by a laboratory value. Stepped-care pathways use severity and complexity to match intensity of psychological and pharmacological treatment.[6][7][8]
Epidemiology and risk factors
Headline numbers every candidate must own
SAD contributes substantial educational, occupational and relationship disability. Many people present years after onset, often when depression, alcohol use or work failure forces help-seeking. Prevalence estimates vary with threshold, culture and whether subthreshold social fears are counted — examiners may ask why rates differ across surveys.[1][4][5]
Risk factors include behavioural inhibition temperament, family history of anxiety, overcontrolling or critical parenting climates, peer rejection and bullying, social learning of threat appraisal, and female sex in many community samples. Suicide risk is not zero and rises with depression, hopelessness, substance use and isolation — never discharge on the assumption that “shyness” is safe.[1][4][5]
Pathophysiology
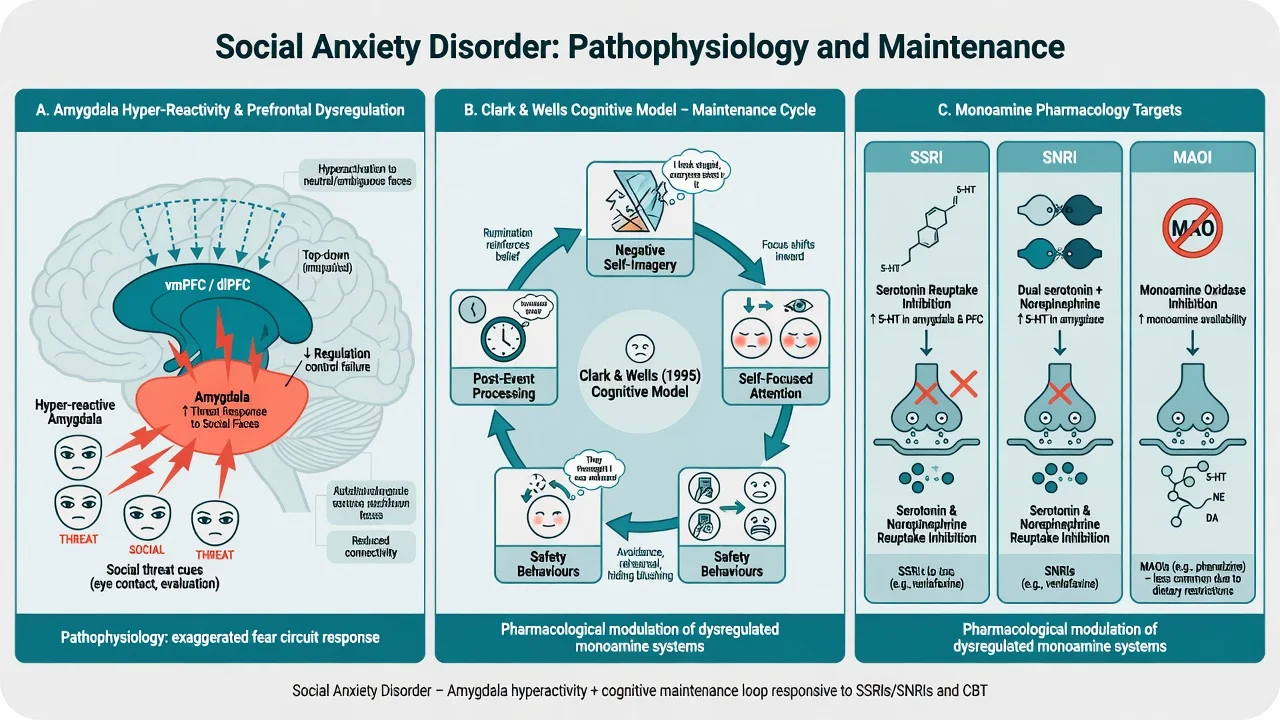
Circuit framing (viva depth, not diagnostic imaging). Group-level models emphasise amygdala hyper-reactivity to social threat cues (including faces and evaluation contexts) with insufficient prefrontal top-down regulation. Imaging is not an individual diagnostic test for SAD.[1]
Transmitter pharmacology that changes prescribing. Serotonergic systems are primary SSRI targets; SNRIs add noradrenergic effects. Monoamine oxidase inhibition (phenelzine) has strong historical RCT support in social phobia but carries dietary and interaction burden. Benzodiazepines facilitate GABA rapidly but promote dependence and can block extinction learning if used as the only strategy.[16][20]
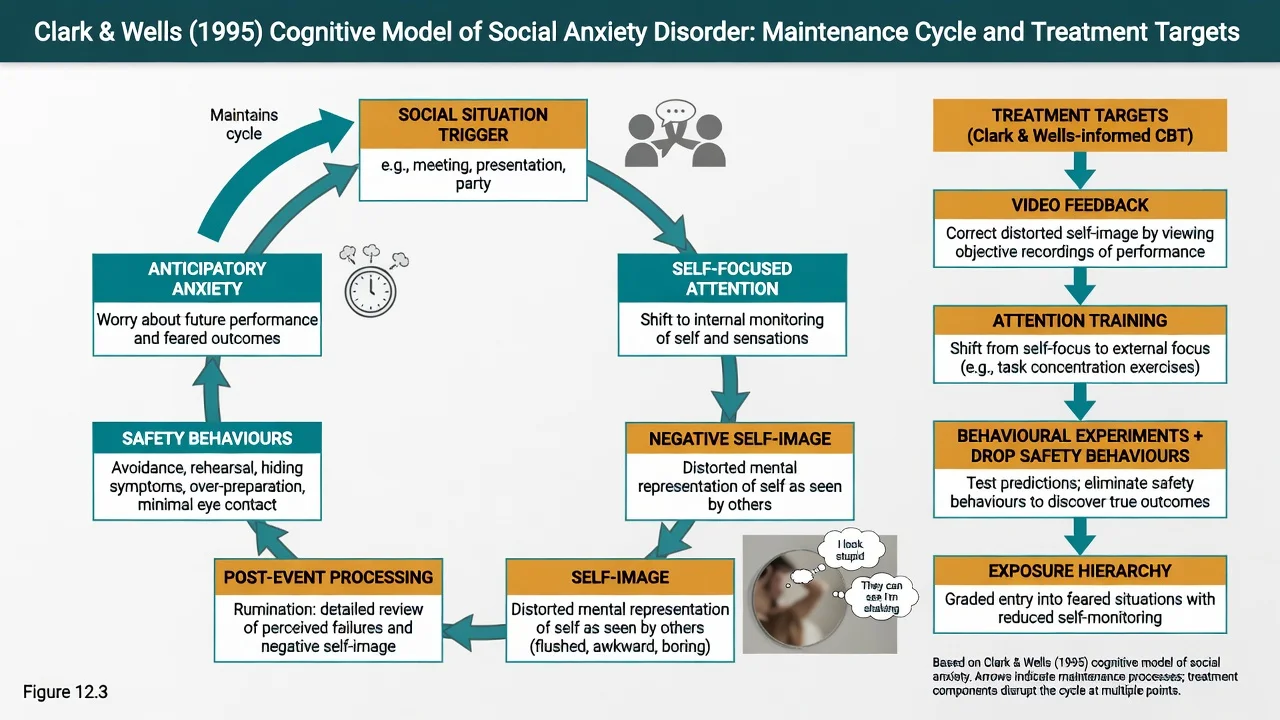
Psychological models that change therapy choice. The Clark and Wells cognitive model highlights self-focused attention, negative self-imagery of how one appears to others, safety behaviours that prevent disconfirmation of fears, and post-event processing (mental replaying of “failures”). Anticipatory anxiety and avoidance complete the loop. Rapee–Heimberg-type models emphasise perceived audience standards and likelihood of negative evaluation. These models dictate treatment targets: attention training, video feedback, dropping safety behaviours, and behavioural experiments — not unstructured “talk about confidence.”[1][6]
Clinical presentation
Core features combine fear of negative evaluation with anticipatory anxiety, somatic signs of scrutiny fear (blushing, sweating, tremor, voice shaking, nausea, urge to escape), and avoidance or endurance of interaction, observation or performance situations. Post-event rumination (“I looked stupid”) and safety behaviours (over-rehearsal, mental reviewing, alcohol before social events, avoiding eye contact, speaking little) maintain the disorder.[1][5]
MSE language. Affect anxious or constrained; thought content themes of humiliation and scrutiny; perception usually normal; cognition intact; insight typically preserved that the fear is excessive, though shame may impede disclosure. Quote the patient’s words (e.g. “If I speak, they will see me shake and think I am incompetent”).[1]
Atypical presentations examiners test. Pure performance subtype (musician, oral exams); late first onset; perinatal social withdrawal; older adult isolation mistaken for “preference for solitude”; cultural shame or honour idioms; adolescents with school refusal; high-functioning professionals who drink to network.[2][3]
Differential diagnosis
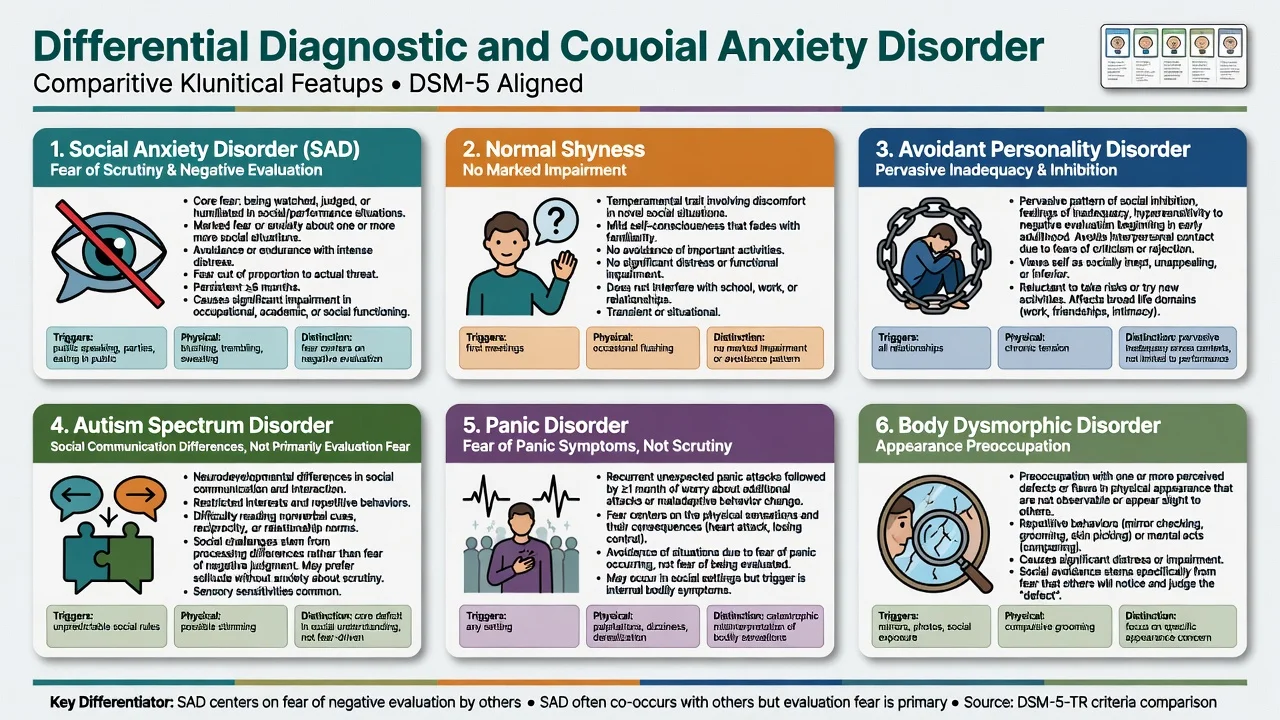
Normal shyness
- Mild self-consciousness that fades with familiarity
- No marked avoidance of important activities
- No clinically significant impairment
- Does not meet duration/impairment criteria
Avoidant personality disorder
- Pervasive social inhibition and inadequacy from early adulthood
- Broader identity/interpersonal pattern
- May coexist with SAD — both can be diagnosed when each is met
- Do not collapse into one label
Autism spectrum
- Social communication differences and restricted interests
- Not primarily driven by fear of negative evaluation
- Sensory and reciprocity differences
- Can be comorbid; assessment needs both lenses
Panic / GAD / BDD / depression
- Panic: fear of attacks/sensations more than scrutiny
- GAD: multi-domain free-floating worry
- BDD: appearance defect belief drives avoidance
- MDD: low mood/anhedonia dominate withdrawal
Also keep OCD (obsessional content/rituals), PTSD (trauma-linked), schizophrenia-spectrum negative or paranoid features, substance-induced anxiety, essential tremor or stuttering with secondary evaluation fear, and illness anxiety on the board. Discriminators, not lists, score marks.[1][5][7]
Clinical and bedside assessment
Structure the interview: feared situations (interaction, observation, performance); content of feared evaluation; anticipatory anxiety and post-event processing; avoidance map; safety behaviours including alcohol and benzodiazepines; duration; onset and developmental history (behavioural inhibition, bullying, selective mutism); depression and suicide risk; bipolar screen before antidepressants; trauma; ASD traits; BDD screen; substances; medical and medication history; perinatal status; function at education/work/relationships; prior treatments and adequacy (therapy type, exposure quality, drug, dose, duration, adherence).[1][7]
Document a full Mental State Examination. Risk is mandatory when depression, hopelessness, substance use or severe isolation is present. Capacity is decision-specific. Involuntary care uses local Mental Health Act principles — least restrictive, statute-bound; do not invent section numbers for the wrong jurisdiction.[7]
Investigations and measurement-based care
Baseline before pharmacotherapy (typical adult set). TSH when clinically indicated; full blood count; urea and electrolytes; liver function as indicated; ECG when cardiac risk or QT-active agents; pregnancy test when relevant; urine drug screen when substance contribution is plausible. Neuroimaging is for neurological red flags — not routine for classic adolescent-onset SAD.[7][8]
Liebowitz Social Anxiety Scale (LSAS). Clinician-administered or self-report formats rate fear and avoidance across social interaction and performance situations; widely used as a trial endpoint and monitoring tool. Know its role (severity/monitoring) rather than inventing cut-offs you cannot defend from memory.[1][10]
SPIN (Social Phobia Inventory). Seventeen-item self-report scale with published psychometric properties for social phobia severity monitoring (total score range concept 0–68). Mini-SPIN is a three-item brief screen used in primary care and epidemiology contexts — useful for case-finding, not a stand-alone diagnosis and not a suicide risk assessment.[18]
Serial LSAS or SPIN plus side-effect and risk review is expected measurement-based care.[7][18]
Management — acute risk and resuscitation
Acute severe anticipatory anxiety before an unavoidable high-stakes performance. Calm environment, clear explanation, exclude medical emergency. A short course of a benzodiazepine may be used for severe distress with a documented indication, short duration, no automatic repeats, and a plan to establish SSRI/SNRI and/or CBT. Example exam-level short-term agents: lorazepam 0.5–1 mg orally or clonazepam 0.25–0.5 mg orally with strict limits — always individualise for age, respiratory disease, and substance history. Do not convert this into maintenance monotherapy.[7][8][20]
Suicidal crisis with comorbid depression. Safety plan, means restriction, intensify setting, treat both syndromes — an SSRI/SNRI may cover both social anxiety and depression once acute safety is addressed.[1][7]
Management — definitive and stepwise
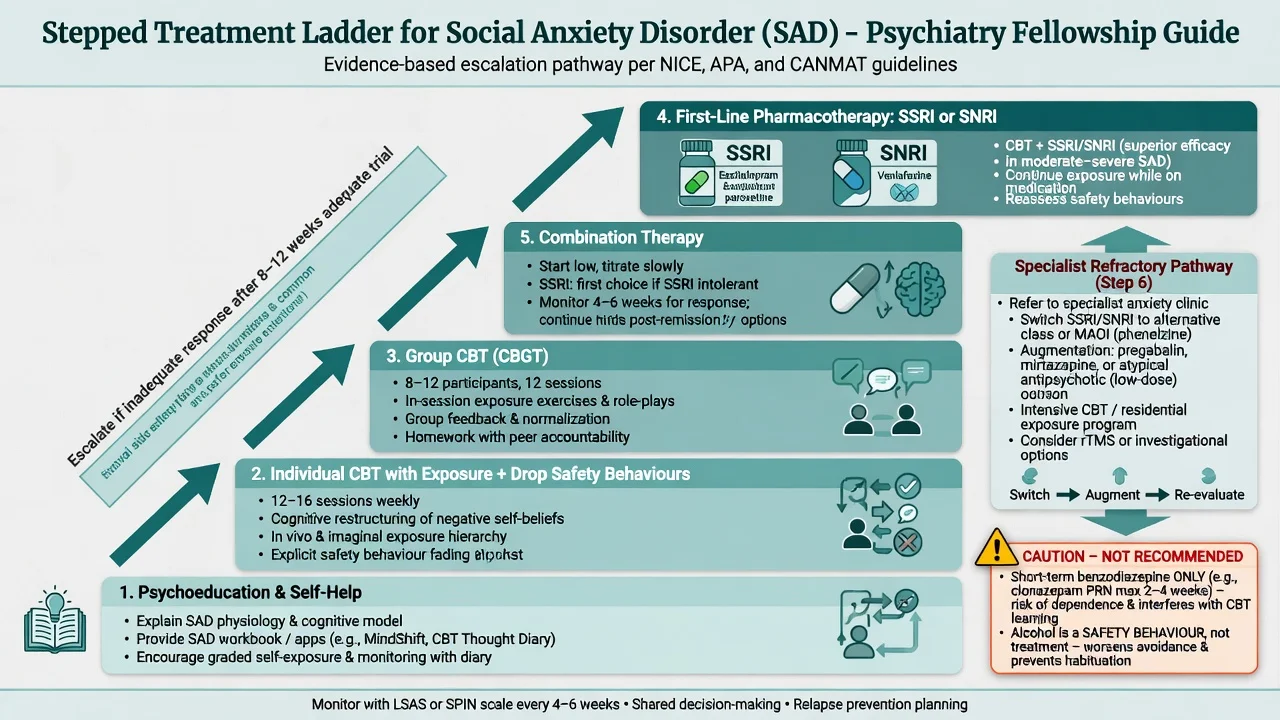
Stepped care principles
Match intensity to severity, disability, preference and comorbidity. Psychoeducation and guided self-help suit mild presentations with motivation. Moderate-to-severe SAD typically warrants high-intensity individual CBT and/or an antidepressant (SSRI or SNRI). Combination treatment is reasonable when severity, chronicity or partial response supports it. Specialist escalation is for high risk, diagnostic complexity, treatment resistance, or heavy substance comorbidity.[6][7][8]
Australian and New Zealand practice aligns with evidence-based CBT access (public and private pathways), first-line SSRI/SNRI prescribing, and cautious benzodiazepine stewardship within local formulary and PBS/PHARMAC constraints. Formulate culturally, including for Māori, Aboriginal and Torres Strait Islander peoples, using local cultural safety frameworks rather than stereotype checklists.[7][8]
First-line psychological therapy — CBT for SAD
CBT for SAD is not generic “build confidence.” High-yield ingredients examiners expect you to name: psychoeducation using a cognitive model; self-monitoring of anticipatory anxiety and post-event processing; external attention training; identification and dropping of safety behaviours; video feedback to correct distorted self-image; behavioural experiments testing predictions about negative evaluation; graded in vivo exposure hierarchy including social mishap experiments where appropriate; cognitive restructuring of probability/cost of negative evaluation; relapse prevention. Group CBT (CBGT, Heimberg model) has landmark comparative evidence versus phenelzine.[6][16][17]
Network meta-analysis of psychological and pharmacological interventions for adult SAD found individual CBT among the most effective options versus waitlist/psychological placebo, with pharmacotherapy also effective — use NMA as a comparative map for shared decisions, not as a single protocol for every patient.[6]
Typical high-intensity course concepts: about 12–16+ sessions (local protocols vary); homework and real-life exposure are essential; family or partner accommodation of avoidance may need addressing.[6]
First-line pharmacotherapy — agent, dose, monitoring
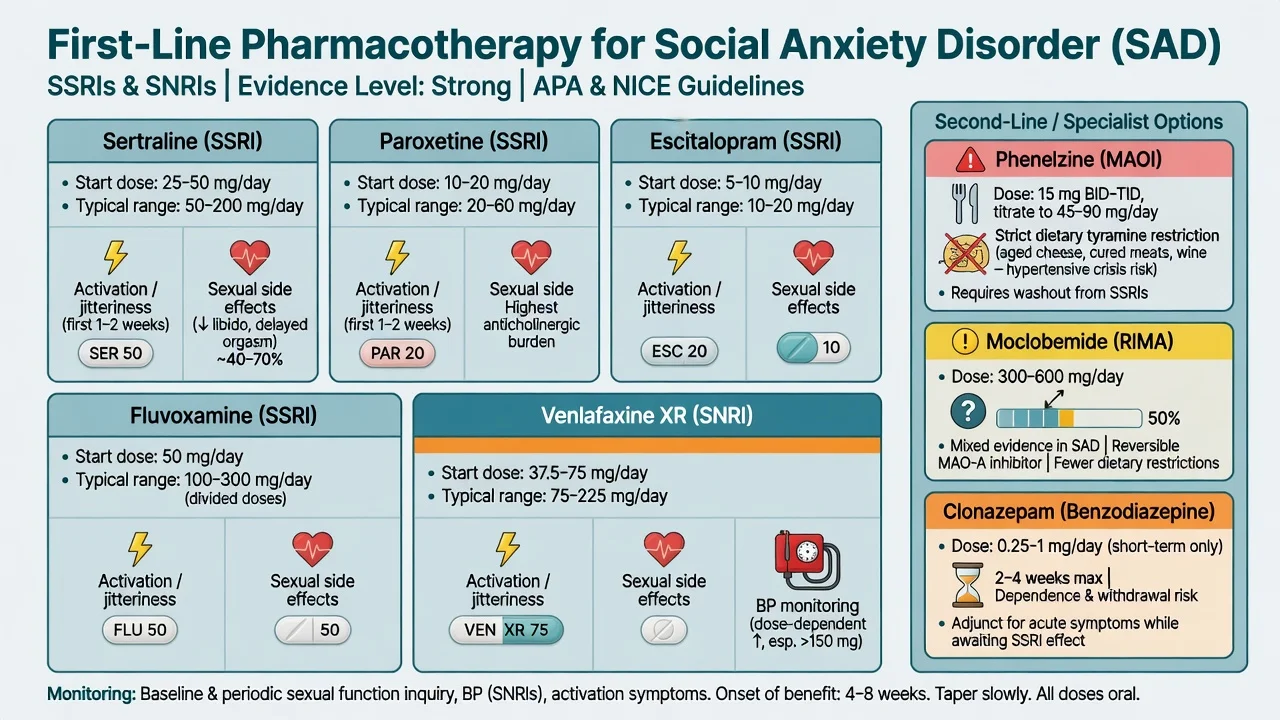
Doses below are typical adult oral starting and common therapeutic ranges for exam answers; individualise for age, hepatic/renal function, interactions and pregnancy. Cite local product information for legal prescribing.[7][8][20]
| Agent (class) | Typical start | Common therapeutic range | Key monitoring / notes |
|---|---|---|---|
| Sertraline (SSRI) | 25–50 mg daily | 50–200 mg daily | 20-week RCT efficacy; relapse-prevention evidence after response |
| Paroxetine (SSRI) | 10–20 mg daily | 20–50 mg daily | Landmark JAMA RCT in generalised social phobia; higher discontinuation syndrome risk |
| Escitalopram (SSRI) | 5–10 mg daily | 10–20 mg daily | Fixed-dose RCT evidence at 12 and 24 weeks; QTc caution at higher doses |
| Fluvoxamine (SSRI) | 50 mg daily | 100–300 mg daily (divided as labelled) | Double-blind RCT in social phobia; CYP interaction burden |
| Venlafaxine XR (SNRI) | 37.5–75 mg daily | 75–225 mg daily | RCT evidence in generalised social anxiety; BP monitoring |
| Typical adult oral ranges for exam use; individualise and check local product information.[9][10][12][13][14][15] |
Start low when anxiety is severe (initial activation/jitteriness is classic), review within 1–2 weeks for activation, akathisia and suicidality (especially under 25 years and with depression), then titrate. Declare an adequate trial only after about 8–12 weeks at a therapeutic dose with adherence checked in SAD literature — longer than many mood trials; do not declare failure after 10 days of half-dose.[9][10][12][20]
After response, continuation reduces relapse: sertraline responders randomised to continuation versus switch to placebo showed benefit of staying on treatment over a further 24 weeks in a key maintenance study.[11] Practical teaching often continues effective medication for at least 6–12 months after response, longer if highly recurrent or disabling, then taper slowly with relapse monitoring.[7][8][11]
Phenelzine, moclobemide and benzodiazepines
Phenelzine (MAOI) has landmark comparative RCT evidence versus cognitive behavioural group therapy for social phobia at 12 weeks, with different long-term patterns after treatment discontinuation in follow-up work — specialist use only with tyramine diet, blood-pressure monitoring, and full interaction counselling (including washout from SSRIs).[16][17][20]
Moclobemide (reversible MAO-A inhibitor) has mixed controlled-trial results in social phobia; know it as a historical/regional option with weaker and less consistent evidence than first-line SSRIs in modern syntheses.[20]
Benzodiazepines (e.g. clonazepam studied in social phobia) can reduce symptoms short-term but dependence, cognitive impairment, falls, and interference with exposure learning make them unsuitable as routine long-term monotherapy. Use only as short bridge with stop date when severity demands it.[7][8][20]
Beta-blockers (e.g. propranolol) may be discussed for performance-only autonomic symptoms in selected situational contexts; they are not first-line disease-modifying treatment for generalised social anxiety disorder.[1][7]
Partial response, switching and refractory care
After non-response: re-check diagnosis (depression, BDD, ASD, substances, medical), adherence, dose, duration, and CBT quality (was exposure real or collusive support?). Switch SSRI↔SNRI or to another first-line agent when zero response or intolerance. Augmentation or switch strategies have been studied in refractory SAD (including randomised designs comparing strategies) — use specialist pathways rather than endless low-dose cycling.[19][20] Second-generation antipsychotics are not routine first-line anxiolytics for SAD.[7][8]
Specific subtypes and scenarios
Performance-only specifier. Formulate around public speaking/performance; graded exposure and CBT still first-line; situational beta-blocker discussion is an exam nuance, not a substitute for skills training.[2][3]
SAD with major depression. Extremely common. Treat both; SSRI/SNRI often covers both domains; suicide risk assessment is mandatory.[1][7]
SAD with alcohol use. Alcohol is a frequent safety behaviour before social events; address substance use in parallel; avoid simply replacing alcohol with unsupervised diazepam.[1][7]
SAD with avoidant personality traits. Comorbidity is common; treat the anxiety syndrome actively with CBT/meds rather than declaring “just personality” and withholding evidence-based care.[1][5]
Primary care versus specialist. Specialist psychiatry for high suicide risk, diagnostic uncertainty (ASD/BDD/psychosis interface), treatment resistance, complex trauma or substance comorbidity, or failed adequate primary-care trials.[7]
Complications and pitfalls
Classic pitfalls: colluding with lifelong avoidance; chronic benzo monotherapy; under-dosed or too-short SSRI trials; missing depression, BDD or ASD; sexual side-effects silently destroying adherence; MAOI dietary/interaction errors; mistaking shyness for SAD or vice versa; exposure that never drops safety behaviours.[6][7][20]
Prognosis and disposition
Without treatment, SAD is often chronic from adolescence with cumulative educational and occupational cost. With adequate CBT and/or SSRI/SNRI, many patients achieve meaningful response; residual avoidance predicts relapse, so relapse-prevention skills and adequate medication duration matter.[1][6][11]
Disposition ladder: GP shared care and primary psychological services; secondary community mental health for complex cases; inpatient care uncommon unless high risk, severe comorbidity, or medical complications of withdrawal. Functional recovery (work, education, relationships) is an outcome alongside scale change.[7]
Special populations
Children and adolescents. Early onset is typical; school refusal and peer avoidance are high-yield. Family accommodation of avoidance must be addressed. If medication is used, SSRI choice and activation/suicidality monitoring are mandatory; specialist CAMHS pathways preferred. Selective mutism may sit on a related spectrum of social fear/avoidance and needs its own assessment pathway.[1][3][7]
Older adults. Isolation may mask SAD; medical mimics and polypharmacy matter; avoid benzodiazepines; start low, go slow on SSRIs (hyponatraemia risk).[7][8]
Pregnancy and lactation. Untreated severe anxiety has maternal functional costs; discuss risks and benefits. Sertraline is frequently discussed as a pragmatic SSRI option when medication is needed; avoid benzodiazepines where possible, especially late pregnancy. Coordinate with obstetric care.[7]
Cultural formulation. Shame, honour, and face may shape presentation; FRANZCP cultural safety expectations in ANZ practice apply — formulate with the person, do not stereotype.[7]
Evidence, guidelines and regional differences
Landmark synthesis. Stein and Stein’s Lancet seminar remains a compact clinical overview of concept, burden and treatment framing.[1] Mayo-Wilson and colleagues’ Lancet Psychiatry network meta-analysis maps comparative efficacy of psychological and pharmacological options — individual CBT ranks highly among psychological interventions; use it to justify stepped choices, not league-table dogma for an individual patient.[6] Blanco and colleagues summarise evidence-based pharmacotherapy of SAD.[20]
Key RCTs and comparative trials to name. Paroxetine generalised social phobia (Stein JAMA); sertraline 20-week trial (Van Ameringen) and sertraline relapse prevention (Walker); escitalopram fixed-dose 12/24-week (Lader); venlafaxine XR (Liebowitz; Rickels); fluvoxamine (Stein); CBGT versus phenelzine (Heimberg 1998) with long-term outcome (Liebowitz 1999); refractory augmentation/switch RCT (Pollack 2014).[9][10][11][12][13][14][15][16][17][19]
Guidelines. Canadian CPG (Katzman et al.) and WFSBP Version 3 Part I (Bandelow et al.) are high-yield international anchors; NICE-style psychological emphasis shapes UK exams; ANZ practice maps onto these with local formulary and cultural safety overlays.[7][8]
Controversies. Optimal default of combination CBT+meds in moderate-severe SAD; residual role of MAOIs; beta-blockers for performance subtype; how aggressively to avoid all benzodiazepines versus time-limited bridging; threshold between shyness, performance fear and disorder.[2][6][20]
Exam pearls
SCRUTINY
Self-test: one-liner viva traps
- Core fear? Negative evaluation under scrutiny.
- Duration? Typically 6 months or more.
- Specifier? Performance-only when restricted to public speaking/performing.
- CBT ingredients? Attention training, drop safety behaviours, video feedback, behavioural experiments, graded exposure.
- First-line drugs? SSRI or SNRI (sertraline, paroxetine, escitalopram, fluvoxamine, venlafaxine XR).
- Landmark psych comparison? CBGT vs phenelzine (Heimberg 1998).
- Maintenance pearl? Continuing sertraline after response reduces relapse (Walker).
- Alcohol? Safety behaviour, not treatment.[1][6][10][11][16]
References
- [1]Stein MB, Stein DJ Social anxiety disorder Lancet, 2008.PMID 18374843
- [2]Heimberg RG, Hofmann SG, Liebowitz MR, Schneier FR, et al. Social anxiety disorder in DSM-5 Depress Anxiety, 2014.PMID 24395386
- [3]Bögels SM, Alden L, Beidel DC, Clark LA, et al. Social anxiety disorder: questions and answers for the DSM-V Depress Anxiety, 2010.PMID 20143427
- [4]Stein MB An epidemiologic perspective on social anxiety disorder J Clin Psychiatry, 2006.PMID 17092189
- [5]Moutier CY, Stein MB The history, epidemiology, and differential diagnosis of social anxiety disorder J Clin Psychiatry, 1999.PMID 10335673
- [6]Mayo-Wilson E, Dias S, Mavranezouli I, Kew K, Clark DM, et al. Psychological and pharmacological interventions for social anxiety disorder in adults: a systematic review and network meta-analysis Lancet Psychiatry, 2014.PMID 26361000
- [7]Katzman MA, Bleau P, Blier P, Chokka P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders BMC Psychiatry, 2014.PMID 25081580
- [8]Bandelow B, Allgulander C, Baldwin DS, Costa DLDC, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for treatment of anxiety, obsessive-compulsive and posttraumatic stress disorders - Version 3. Part I: Anxiety disorders World J Biol Psychiatry, 2023.PMID 35900161
- [9]Stein MB, Liebowitz MR, Lydiard RB, Pitts CD, et al. Paroxetine treatment of generalized social phobia (social anxiety disorder): a randomized controlled trial JAMA, 1998.PMID 9728642
- [10]Van Ameringen MA, Lane RM, Walker JR, Bowen RC, et al. Sertraline treatment of generalized social phobia: a 20-week, double-blind, placebo-controlled study Am J Psychiatry, 2001.PMID 11156811
- [11]Walker JR, Van Ameringen MA, Swinson R, Bowen RC, et al. Prevention of relapse in generalized social phobia: results of a 24-week study in responders to 20 weeks of sertraline treatment J Clin Psychopharmacol, 2000.PMID 11106135
- [12]Lader M, Stender K, Bürger V, Nil R Efficacy and tolerability of escitalopram in 12- and 24-week treatment of social anxiety disorder: randomised, double-blind, placebo-controlled, fixed-dose study Depress Anxiety, 2004.PMID 15274173
- [13]Liebowitz MR, Mangano RM, Bradwejn J, Asnis G, et al. A randomized controlled trial of venlafaxine extended release in generalized social anxiety disorder J Clin Psychiatry, 2005.PMID 15705011
- [14]Rickels K, Mangano R, Khan A A double-blind, placebo-controlled study of a flexible dose of venlafaxine ER in adult outpatients with generalized social anxiety disorder J Clin Psychopharmacol, 2004.PMID 15349004
- [15]Stein MB, Fyer AJ, Davidson JR, Pollack MH, et al. Fluvoxamine treatment of social phobia (social anxiety disorder): a double-blind, placebo-controlled study Am J Psychiatry, 1999.PMID 10327910
- [16]Heimberg RG, Liebowitz MR, Hope DA, Schneier FR, et al. Cognitive behavioral group therapy vs phenelzine therapy for social phobia: 12-week outcome Arch Gen Psychiatry, 1998.PMID 9862558
- [17]Liebowitz MR, Heimberg RG, Schneier FR, Hope DA, et al. Cognitive-behavioral group therapy versus phenelzine in social phobia: long-term outcome Depress Anxiety, 1999.PMID 10604081
- [18]Connor KM, Davidson JR, Churchill LE, Sherwood A, et al. Psychometric properties of the Social Phobia Inventory (SPIN). New self-rating scale Br J Psychiatry, 2000.PMID 10827888
- [19]Pollack MH, Van Ameringen M, Simon NM, Worthington JW, et al. A double-blind randomized controlled trial of augmentation and switch strategies for refractory social anxiety disorder Am J Psychiatry, 2014.PMID 24399428
- [20]Blanco C, Bragdon LB, Schneier FR, Liebowitz MR The evidence-based pharmacotherapy of social anxiety disorder Int J Neuropsychopharmacol, 2013.PMID 22436306