Psych · General adult psychiatry — somatic symptom and related disorders
Somatic symptom disorder
Also known as SSD · Somatisation · Somatization disorder · Somatoform disorder · Medically unexplained symptoms · Bodily distress disorder · Functional somatic syndromes · PHQ-15
Exam-exhaustive fellowship reference on somatic symptom disorder — DSM-5-TR criteria and the medically unexplained pivot, ICD-11 bodily distress framing, discriminators vs illness anxiety/FND/factitious/malingering, PHQ-15 assessment, collaborative stepped care, CBT evidence, pharmacotherapy humility, and avoiding iatrogenic harm. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Somatic symptom disorder is a high-yield general adult and consultation-liaison interface topic for FRANZCP, MRCPsych, ABPN, and MD/DNB. Examiners test the DSM-5 nosological pivot, discriminators (especially illness anxiety, FND, factitious/malingering), PHQ-15, alliance-preserving communication, stepped care, CBT trial names, pharmacotherapy humility, and recognition that iatrogenesis is part of the pathophysiology of disability.[1][3][6]
Overview and definition
DSM-5-TR SSD requires: (1) one or more somatic symptoms that are distressing or result in significant disruption of daily life; (2) excessive thoughts, feelings, or behaviours related to the somatic symptoms or associated health concerns, manifested by at least one of disproportionate and persistent thoughts about the seriousness of symptoms, persistently high level of anxiety about health or symptoms, or excessive time and energy devoted to these symptoms or health concerns; (3) although any one symptom may not be continuously present, the state of being symptomatic is typically persistent (usually more than 6 months).[1][2]
Clinical essence for viva. The diagnostic focus shifted from what is missing on investigations to how the person thinks, feels, and behaves in relation to symptoms. A patient with documented rheumatoid arthritis, inflammatory bowel disease, or cancer can still meet SSD criteria if health-related cognitions, affect, and behaviours are excessive relative to the medical picture and drive disability. Conversely, multiple normal scans do not automatically equal SSD without B-criteria and impairment.[1][2][3]
Why this matters. Dualistic “real vs psychological” language is both clinically harmful and nosologically obsolete. Fellowship answers lead with a both–and model: symptoms are genuine experiences; attention, threat appraisal, mood, sleep, and care systems amplify suffering and disability.[6][11]
Classification map
SSD (DSM-5-TR)
- Distressing somatic symptoms present
- Disproportionate thoughts/feelings/behaviours (B criteria)
- Usually ≥6 months symptomatic state
- Medical disease can coexist
Illness anxiety disorder
- Preoccupation with having/acquiring serious illness
- Somatic symptoms absent or only mild
- Care-seeking or care-avoidant behaviours
- High health anxiety core
ICD-11 framing
- Bodily distress disorder: distressing symptoms + excessive attention/behaviours
- Severity graded (mild/moderate/severe)
- Hypochondriasis retained as health-anxiety construct
- State which manual you are using
Legacy map
- Somatisation / undifferentiated somatoform → often SSD
- Pain disorder → often SSD with predominant pain
- Hypochondriasis → IAD or SSD depending on symptom load
- Do not diagnose by normal investigations alone
ICD-11. Bodily distress disorder emphasises re-experiencing of distressing bodily symptoms with excessive attention and related behaviours, with severity grading. Hypochondriasis captures health-anxiety presentations. Fink’s empirical bodily distress work supports multi-organ symptom clustering as clinically coherent even when specialty labels (IBS, fibromyalgia, non-cardiac chest pain) fragment care pathways.[7][6]
Mayou’s critique (examinable). DSM-5 SSD is broader than DSM-IV somatisation disorder and can pathologise adaptive illness concern if B-criteria and impairment are applied loosely. Document excessiveness and functional impact, not mere appropriate worry about real disease.[3]
Epidemiology and burden
Exam-facing burden anchors
Multiple distressing somatic symptoms are common in primary care and medical clinics. Higher PHQ-15 scores associate with functional impairment, depression and anxiety comorbidity, and increased health-care utilisation.[4][5] Depression and musculoskeletal pain co-travel clinically; optimising antidepressant care plus structured self-management improves both domains in primary-care trials (SCAMP), underscoring integrated rather than siloed care.[17] Psychiatric services are often the “missing P” when chronic pain and somatic disability systems escalate medications without formulation.[18]
Risk contexts. Childhood adversity and trauma, insecure attachment, prior medical illness, health-system fragmentation, and iatrogenic reinforcement (repeated negative work-ups without a positive explanation) enrich risk. Female predominance appears in many multi-symptom series; always avoid stereotyping the individual patient.[6][7]
Pathophysiology and maintaining model
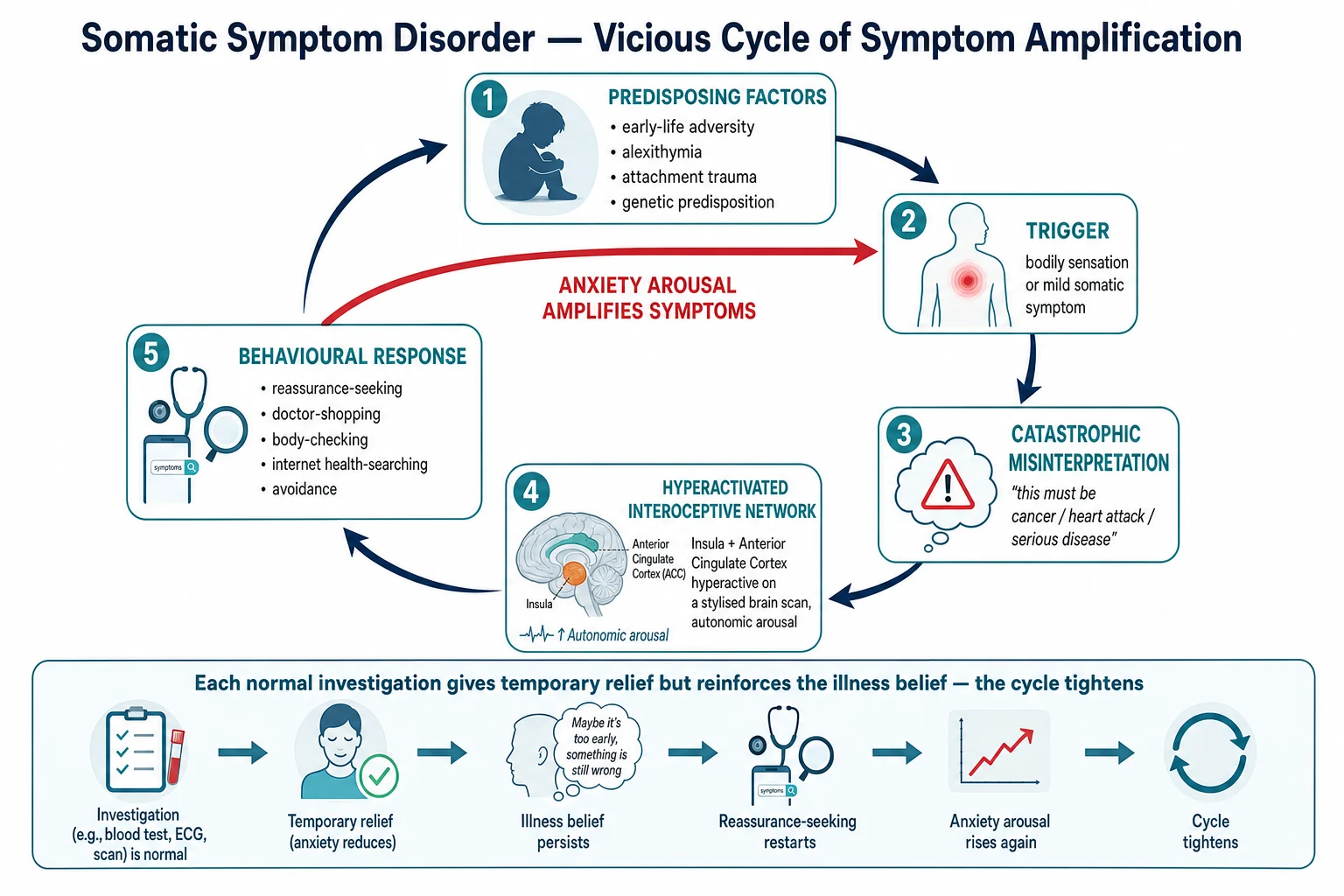
Viva-ready mechanisms (no speculative single biomarker claim): Both–and biology — peripheral sensations, inflammatory disease, injury, and autonomic arousal can all generate real symptoms; central processing, attention, and affect shape intensity and disability.[6] Attentional amplification and catastrophising — selective attention to bodily signals and catastrophic illness interpretations fuel anxiety and help-seeking — the cognitive model underpinning health-anxiety CBT trials.[11][13] Safety behaviours — body checking, pulse/oxygen monitoring, online symptom searching, reassurance-seeking, activity avoidance, and repeated emergency presentations reduce short-term anxiety and prevent disconfirmation.[11][6] Mood–sleep–pain loops — depression and insomnia amplify symptom salience; fear-avoidance produces deconditioning when pain is prominent.[17][18] Iatrogenic reinforcement — unfocused investigation cascades without a collaborative formulation increase threat beliefs and medical risk (contrast, radiation, procedures, false positives). This is examinable as part of the disorder’s ecology, not merely “bad medicine.”[6][15]
Clinical presentation
Typical stems: multi-year multi-system symptoms with high distress; high GP and ED utilisation; “negative” medical admissions; post-scare escalation after a minor lab abnormality; predominant pain with disability out of proportion to imaging; family and workplace conflict about legitimacy of symptoms.[4][6][15]
MSE focus. Affect (anxious, depressed, frustrated, sometimes angry); health beliefs (overvalued vs delusional certainty); body-focused attention and checking; insight into psychological maintaining factors (often limited early); suicide risk; substance use; secondary-gain exploration without accusation. Ideas of serious illness that are firmly held but without other psychotic features usually remain in the SSD/IAD spectrum rather than primary psychosis.[1][5]
Cultural presentation. Many cultures encode distress somatically. Cultural idioms do not automatically equal SSD; diagnose when excessiveness, impairment, and B-criteria are met after culturally informed assessment.[6][16]
Differential diagnosis
| Construct | Discriminators | Classic trap |
|---|---|---|
| Evolving medical disease | Red flags, pattern change, objective progression | Closing the organic door permanently |
| Illness anxiety disorder | Minimal somatic symptoms + high health anxiety | Calling every health-anxious patient “SSD” |
| Depression / GAD / panic | Mood/worry primary; panic attacks discrete | Missing comorbidity that drives disability |
| OCD | Multi-theme obsessions/compulsions, rituals beyond health | Missing pure illness-OCD needing ERP |
| Psychosis | Primary delusions/hallucinations/thought disorder | Overcalling psychosis for overvalued health beliefs |
| FND / conversion | Voluntary motor/sensory pattern with incompatibility signs | Labelling all unexplained neurology “somatisation” |
| Factitious disorder | Intentional production, sick-role motivation | Accusing without evidence |
| Malingering | Intentional production for external incentive | Using the label as a discharge weapon |
Always keep the organic door ajar. Known SSD does not immunise against stroke, malignancy, autoimmune disease, endocrine crisis, or medication toxicity. Pattern change is a hard stop for pure psychosocial framing.[6]
Clinical and bedside assessment
Alliance first. Open with: symptoms are real; the goal is to reduce suffering, restore function, and keep you safe — not to prove the symptoms are imaginary. Premature dualism ends the interview clinically even if it continues socially.[6]
History structure. Onset and course; symptom map (sites, variability); functional impact (work, relationships, self-care); prior work-ups and procedures; what findings would change management if tests were repeated; health beliefs and feared diagnoses; checking/reassurance/online searching; appointment pattern; substances and sedatives/opioids if pain-dominant; trauma history when appropriate; family accommodation; prior psychological care fidelity.[4][6][15]
Scales. PHQ-15 measures somatic symptom severity and supports monitoring; it does not alone diagnose SSD. Pair with PHQ-9 and anxiety screens. Systematic review supports the PHQ somatic/anxiety/depression suite in medical and primary-care populations.[4][5]
Risk. Suicide and self-harm assessment is mandatory when depression, chronic pain, or hopelessness are present. Vulnerability (elder abuse, coercive care-seeking dynamics) may matter in complex families.[5][18]
Coordination. Identify a single coordinating clinician (usually GP) and agree re-investigation thresholds with medical teams. This is core care, not optional admin.[6][15]
Investigations and measurement-based care
Investigations should be hypothesis-driven, guided by red flags and change over time — not exhaustive “to prove it is psychological.” Ordering tests solely as a negotiation tool without a clinical question often worsens outcomes.[6]
Before SSRI/SNRI/TCA: consider pregnancy status, metabolic baseline as indicated, ECG when cardiac risk/TCA planned, and drug–drug interactions (serotonergic stacking).[9][12]
Track function (work days, walk tolerance, sleep, social activity) and serial PHQ-15/mood scores. Zero-symptom extinction as the only success metric predicts demoralisation and care escalation.[4][10]
Acute and emergency management
In crisis, stop unfocused polypharmacy escalation (especially opioids + benzodiazepines). Acute severe distress still deserves humane care; dual diagnosis or high utilisation is not a licence for contemptuous minimalism.[18]
Capacity and Mental Health Act issues are jurisdiction-specific; apply capacity principles when the person refuses essential medical care under health-anxiety avoidance or when severe depression incapacitates decision-making.[6]
Definitive management — care principles and stepped care

Care principles (always state these)
Henningsen-style principles for functional somatic syndromes translate cleanly to SSD practice: (1) take symptoms seriously — validate experience; (2) positive, non-dualistic explanation — brain–body amplification, not “fake”; (3) limit unnecessary tests and specialist shopping — use pre-agreed thresholds; (4) schedule regular, time-limited reviews rather than only PRN crisis visits; (5) set functional goals (sleep, graded activity, work return) rather than total symptom extinction alone; (6) coordinate care — one primary clinician letter/plan shared across teams.[6][15]
High-utilising somatising patients benefit from structured psychosocial interventions and coordinated medical care rather than endless diagnostic churn.[15]
Stepped care ladder
| Step | Setting | Core interventions |
|---|---|---|
| 1 | Primary care | Validation; PHQ-15/mood screen; scheduled visits; re-investigation thresholds; sleep and activity advice |
| 2 | Psychological | CBT adapted for health anxiety / multi-symptom presentations; treat panic/avoidance |
| 3 | Psychiatric meds | Target comorbid depression/anxiety; cautious analgesic antidepressants if pain phenotype |
| 4 | Specialist | C-L psychiatry, multidisciplinary pain/functional services, intensive programmes for severe disability |
| Safety layer | All steps | Suicide risk; medical red flags; deprescribe high-risk polypharmacy |
Psychological therapies — first-line psychological signal
- Barsky and Ahern (JAMA RCT): CBT for hypochondriasis reduces health anxiety versus control — foundational exam citation for cognitive-behavioural work on illness fears and behaviours.[11]
- Greeven et al.: CBT and paroxetine both outperform waitlist/placebo-type comparators in hypochondriasis; CBT is a durable psychological first-line option.[12]
- CHAMP (Tyrer et al., Lancet): adapted CBT for health anxiety in medical clinic patients improved outcomes and was cost-effective in a multicentre RCT — high-yield FRANZCP/MRCPsych name.[13]
- Fallon et al.: modern RCT framework of medication and CBT strategies for hypochondriasis — know that mono- and combined strategies are studied; read the stem before claiming a universal winner.[14]
- Cochrane (van Dessel): non-pharmacological interventions for somatoform disorders / MUPS show modest benefits; CBT-family approaches dominate the evidence base — set realistic expectations.[8]
- Kleinstäuber meta-analysis: short-term psychotherapy for multiple medically unexplained physical symptoms yields small-to-moderate effects.[10]
- Sumathipala et al.: structured CBT versus structured care for MUS is adaptable across cultural settings — useful MD/DNB and global health exam angle.[16]
- Barsky 2013 high-utilising RCT: targeted treatments for high-utilising somatising patients reduce utilisation burdens in randomised design — supports service models beyond “another scan.”[15]
- SCAMP (Kroenke): optimised antidepressant therapy plus pain self-management improves depression and pain in primary care when depression and musculoskeletal pain co-occur.[17]
Generic supportive counselling without cognitive work on threat appraisals and behaviour change (checking, avoidance, reassurance) is an exam failure mode.[11][13]
Pharmacotherapy — humility first
Cochrane review of pharmacological interventions for somatoform disorders finds limited, low-certainty signals. Do not treat “somatisation” with escalating polypharmacy as if it were antipsychotic-responsive psychosis.[9]
When medication is used, target comorbid depression/anxiety and selected symptom phenotypes. Exam-facing oral spines (confirm local product information): sertraline often 25–50 mg daily, titrate as tolerated toward antidepressant range (monitor activation, sexual side effects, hyponatraemia in older adults, suicide risk discussion in younger patients); paroxetine often 10–20 mg daily start then titrate (studied vs CBT in hypochondriasis; watch discontinuation symptoms and interactions); duloxetine common spine 30 mg daily for about 1 week then 60 mg daily when used for pain/depression phenotypes (nausea, blood pressure, withdrawal, serotonergic interactions); amitriptyline often 10–25 mg at night with slow titration for some pain-predominant presentations (anticholinergic effects, falls, cardiac risk, overdose lethality). Individualise for age, comorbidities, pregnancy, and interactions. Pharmacotherapy is adjunct, not a substitute for collaborative care and CBT access.[9][12][17]
Avoid as default long-term strategy: benzodiazepines for chronic somatic anxiety; automatic opioid escalation for chronic non-cancer pain without functional goals (detail and SPACE/CDC evidence live in the pain psychiatry hub).[18]
Communication scripts (CASC-ready)
Do say: “Your symptoms are real. When the brain’s threat and attention systems stay on high alert, symptoms and disability can intensify even when serious disease has been reasonably excluded or is stable. Our job is to treat the whole picture — medical safety, mood, sleep, and the habits (checking, emergency visits) that keep the alarm system loud.”[1][6][11]
Do not say: “It is all in your head,” “there is nothing wrong,” or “we will keep scanning until we find something.” Those lines destroy alliance and invite iatrogenesis.[6]
Subtypes and scenarios
Primary-care high utilizer. Multi-system symptoms, high PHQ-15, normal work-ups → scheduled GP visits, single-clinician coordination, CBT referral, treat depression/anxiety, pre-agreed re-test thresholds.[4][15]
SSD with predominant pain. Formulate pain–depression–sleep–fear-avoidance loops; psychological therapies and cautious SNRI/TCA; avoid sedative/opioid cascades; consider multidisciplinary pain input.[17][18]
Post-scare health anxiety with residual symptoms. After negative oncology or cardiac work-up, some patients retain high illness fear with ongoing bodily focus — may sit near IAD or SSD depending on symptom load; CBT for health anxiety is first-line psychological care.[11][13]
Inpatient C-L after “negative” admission. Lead with validation and red-flag review; document shared medical plan; avoid last-day pejorative “functional” dump without follow-up structure.[6]
Doctor shopping. Fragmented care is a maintaining factor; write a clear shared care letter rather than competing specialists.[6][15]
Complications and pitfalls
- Dualistic dismissal language.[6]
- Missing new organic disease in a known somatising patient.[6]
- Endless unfocused investigations without positive formulation.[6][15]
- Polypharmacy (opioids, benzos, multiple psychotropics) without targets.[9][18]
- Premature SSD label in older multi-morbid adults.[3]
- Factitious/malingering accusations without careful evidence.[1]
- Treating only depression while ignoring health-anxiety behaviours — or vice versa.[11][17]
Prognosis and disposition
Course is often chronic and fluctuating. Best outcomes track engagement, treated mood/anxiety, reduced iatrogenic reinforcement, GP continuity, and improved function rather than zero symptoms.[6][10]
Disposition. Shared care: GP continuity + psychology/CBT + psychiatry for complex comorbidity, risk, or failed step-2 care; C-L and multidisciplinary services for severe disability. Provide a flare plan (who to contact, what symptoms reopen medical review, how to use scheduled visits).[6][15]
Special populations
Youth. Functional symptoms, school avoidance, family reinforcement systems; developmental formulation; cautious medication; family-inclusive CBT principles.[6]
Older adults. Multi-morbidity — do not label every symptom cluster as SSD; higher TCA anticholinergic and fall risk; hyponatraemia with SSRIs; always re-check organic differentials.[3][9]
Pregnancy and lactation. Prioritise psychological care and obstetric liaison; any antidepressant needs individualised perinatal risk–benefit discussion.[9]
Cultural formulation. Bodily idioms of distress may be culturally coherent; avoid over-pathologising while still treating disability, depression, and harmful care patterns.[6][16]
Intellectual disability. Diagnostic overshadowing and communication barriers for pain; collateral and behavioural observation matter.[6]
Evidence, guidelines and regional differences
Landmark pillars: Dimsdale SSD nosology;[1][2] Mayou critique;[3] Kroenke PHQ-15 and PHQ suite review;[4][5] Henningsen FSS management;[6] Fink bodily distress;[7] van Dessel Cochrane non-pharmacological;[8] Kleinstäuber pharmacological Cochrane and psychotherapy meta-analysis;[9][10] Barsky CBT;[11] Greeven CBT/paroxetine;[12] Tyrer CHAMP;[13] Fallon med+CBT;[14] Barsky high-utilising trial;[15] Sumathipala CBT;[16] SCAMP;[17] Howe/Sullivan missing psychiatric services.[18]
FRANZCP-facing practice emphasises collaborative primary care, C-L partnership, and quality use of medicines. Access to CBT with health-anxiety/SSD competence is often rate-limiting — use stepped primary-care models and secondary psychology where available. Prescribing follows TGA product information; Mental Health Act frameworks are state/territory-specific. Pain–opioid stewardship aligns with national quality-use principles (detailed opioid evidence in the pain psychiatry hub).[6][15][18]
Exam pearls
SSD CARE principles
Classic stems
- High-utilising multi-system symptoms, normal work-ups, high PHQ-15 → SSD formulation + scheduled GP care + CBT, not another unfocused scan by default.[4][8][15]
- Minimal symptoms, extreme cancer fear, body checking → think IAD / health-anxiety CBT (may still cite same trials).[11][13]
- Known IBD with disproportionate disability and endless ED visits despite stable objective markers → SSD can coexist with medical disease; collaborative plan + CBT + treat depression.[1][6]
- New night pain and weight loss in a “known somatiser” → re-open organic work-up first.[6]
References
- [1]Dimsdale JE, Creed F, Escobar J, et al. Somatic symptom disorder: an important change in DSM J Psychosom Res, 2013.PMID 23972410
- [2]Dimsdale JE, Levenson J What's next for somatic symptom disorder? Am J Psychiatry, 2013.PMID 24306336
- [3]Mayou R Is the DSM-5 chapter on somatic symptom disorder any better than DSM-IV somatoform disorder? Br J Psychiatry, 2014.PMID 25029686
- [4]Kroenke K, Spitzer RL, Williams JB The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms Psychosom Med, 2002.PMID 11914441
- [5]Kroenke K, Spitzer RL, Williams JB, et al. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: a systematic review Gen Hosp Psychiatry, 2010.PMID 20633738
- [6]Henningsen P, Zipfel S, Herzog W Management of functional somatic syndromes Lancet, 2007.PMID 17368156
- [7]Fink P, Toft T, Hansen MS, et al. Symptoms and syndromes of bodily distress: an exploratory study of 978 internal medical, neurological, and primary care patients Psychosom Med, 2007.PMID 17244846
- [8]van Dessel N, den Boeft M, van der Wouden JC, et al. Non-pharmacological interventions for somatoform disorders and medically unexplained physical symptoms (MUPS) in adults Cochrane Database Syst Rev, 2014.PMID 25362239
- [9]Kleinstäuber M, Witthöft M, Steffanowski A, et al. Pharmacological interventions for somatoform disorders in adults Cochrane Database Syst Rev, 2014.PMID 25379990
- [10]Kleinstäuber M, Witthöft M, Hiller W Efficacy of short-term psychotherapy for multiple medically unexplained physical symptoms: a meta-analysis Clin Psychol Rev, 2011.PMID 20920834
- [11]Barsky AJ, Ahern DK Cognitive behavior therapy for hypochondriasis: a randomized controlled trial JAMA, 2004.PMID 15039413
- [12]Greeven A, van Balkom AJ, Visser S, et al. Cognitive behavior therapy and paroxetine in the treatment of hypochondriasis: a randomized controlled trial Am J Psychiatry, 2007.PMID 17202549
- [13]Tyrer P, Cooper S, Salkovskis P, et al. Clinical and cost-effectiveness of cognitive behaviour therapy for health anxiety in medical patients: a multicentre randomised controlled trial Lancet, 2014.PMID 24139977
- [14]Fallon BA, Ahern DK, Pavlicova M, et al. A Randomized Controlled Trial of Medication and Cognitive-Behavioral Therapy for Hypochondriasis Am J Psychiatry, 2017.PMID 28659038
- [15]Barsky AJ, Ahern DK, Bauer MR, et al. A randomized trial of treatments for high-utilizing somatizing patients J Gen Intern Med, 2013.PMID 23494213
- [16]Sumathipala A, Siribaddana S, Abeysingha MR, et al. Cognitive-behavioural therapy v. structured care for medically unexplained symptoms: randomised controlled trial Br J Psychiatry, 2008.PMID 18700219
- [17]Kroenke K, Bair MJ, Damush TM, et al. Optimized antidepressant therapy and pain self-management in primary care patients with depression and musculoskeletal pain: a randomized controlled trial JAMA, 2009.PMID 19470987
- [18]Howe CQ, Sullivan MD The missing 'P' in pain management: how the current opioid epidemic highlights the need for psychiatric services in chronic pain care Gen Hosp Psychiatry, 2014.PMID 24211157