Psych · General adult psychiatry — anxiety disorders
Specific phobia
Also known as Simple phobia (historical) · Phobic disorder — specific · Animal phobia · Blood-injection-injury phobia · Situational phobia · One-session treatment / Öst OST
Exam-exhaustive fellowship reference on specific phobia — DSM-5-TR and ICD-11 criteria; five type specifiers; epidemiology; fear acquisition and maintenance; blood-injection-injury physiology and applied tension; in vivo exposure and one-session treatment; limited pharmacotherapy role; differentials from SAD, panic/agoraphobia, OCD and PTSD; NICE/Canadian/WFSBP/ANZ stepped care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Specific phobia is a high-frequency community anxiety diagnosis that is under-treated until life forces contact with the cue (flying for work, blood tests, dental care, parenting a dog-owning household). FRANZCP MEQs and MRCPsych CASC reward criteria with type specifier, BII physiology, exposure ingredients, and the explicit statement that medications are not first-line. ABPN items test one-session treatment, applied tension, and differentials from agoraphobia and social anxiety.[1][3][4][11]
Overview and definition
Specific phobia is a syndrome of marked fear or anxiety about a specific object or situation (for example flying, heights, animals, receiving an injection, seeing blood). The phobic stimulus almost always provokes immediate fear or anxiety; it is actively avoided or endured with intense fear; the fear is out of proportion to the actual danger and to the sociocultural context; it is persistent, typically lasting 6 months or more; and it causes clinically significant distress or impairment — after substance effects, medical mimics, and competing mental disorders have been reasonably excluded.[1][3]
DSM-5-TR structure you must reproduce. Marked fear or anxiety about a specific object or situation. The phobic object or situation almost always provokes immediate fear or anxiety. The object or situation is actively avoided or endured with intense fear or anxiety. The fear or anxiety is out of proportion to the actual danger posed by the specific object or situation and to the sociocultural context. The fear, anxiety, or avoidance is persistent, typically lasting 6 months or more. The fear, anxiety, or avoidance causes clinically significant distress or impairment. The disturbance is not better explained by symptoms of another mental disorder, including fear/avoidance of social situations (social anxiety disorder), situations related to obsessions (OCD), reminders of traumatic events (PTSD), separation (separation anxiety), or panic-like cues/agoraphobic situations.[1]
ICD-11. Specific phobia emphasises marked and excessive fear or anxiety that occurs consistently on exposure or anticipation of a specific object or situation, with avoidance or endurance under intense distress, and clinically significant impairment. When duration language is examined, name which system you are applying — DSM-5-TR’s typically-6-months threshold is the classic exam anchor for both adults and children.[1][3]
Classification
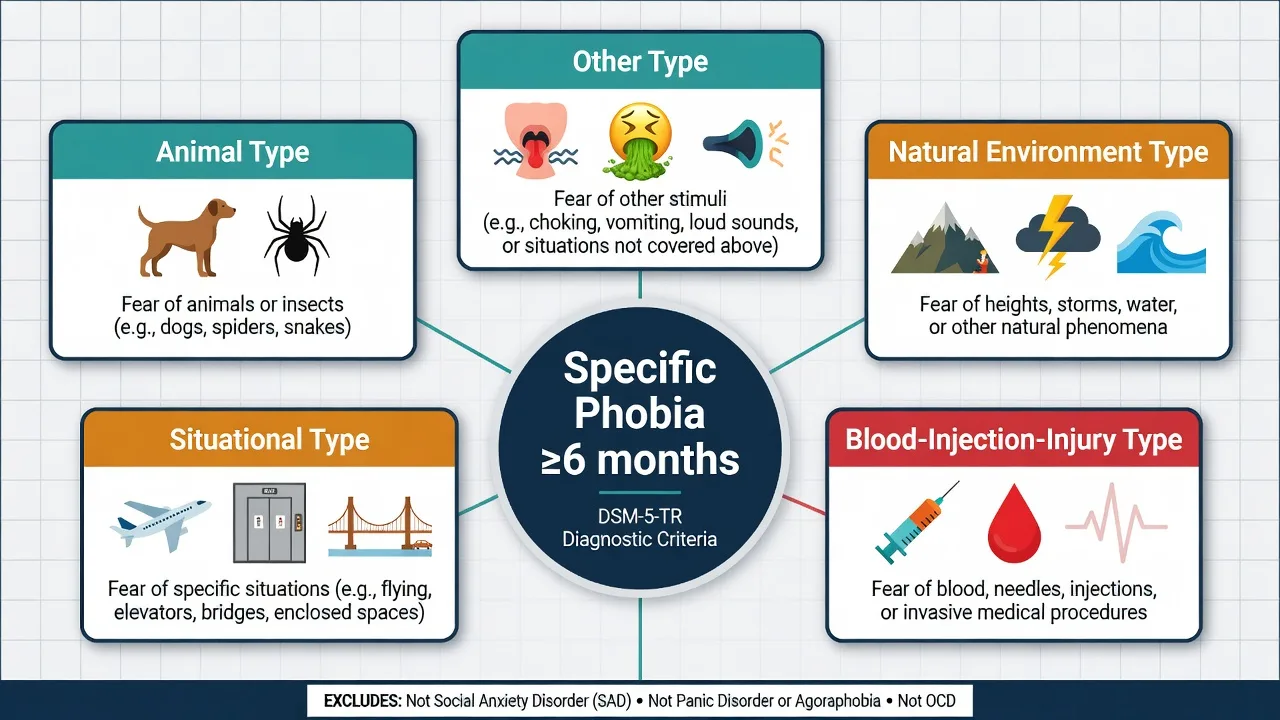
Animal
- Spiders, insects, dogs, snakes, birds
- Often childhood onset
- Classic OST candidates
- Preparedness common
Natural environment
- Heights, storms, water, dark
- May cluster (heights + water)
- Occupational/travel impact
- Distinguish from situational elevators
Blood-injection-injury
- Blood, injections, injury, invasive procedures
- Vasovagal / faint risk
- Applied tension + exposure
- Medical/dental care avoidance
Situational / other
- Flying, elevators, enclosed spaces, bridges
- Other: choking, vomiting, loud sounds, costumed characters
- Situational ≠ agoraphobia (breadth)
- Emetophobia high functional load
If multiple phobias are present, specify each clinically relevant type. Severity is graded by avoidance, disability, multi-phobia load, and comorbidity rather than by a laboratory value.[1][2][16]
Epidemiology and risk factors
Headline numbers every candidate must own
World Mental Health survey data show specific phobia is highly prevalent cross-nationally, often begins early, and contributes substantial role impairment when stimuli cannot be avoided. Community surveys such as NEMESIS map subtype distributions of specific fears and full phobias. Dental fear and phobia are common relative to other fear subtypes and drive delayed oral care.[2][16][17]
Risk factors include behavioural inhibition, family history of anxiety/phobia, direct aversive conditioning, vicarious learning (watching others fear), informational transmission (warnings, media), and evolutionary preparedness for certain cues. Comorbid depression is clinically important — it elevates disability and is not “just secondary annoyance.”[1][3][15]
Pathophysiology
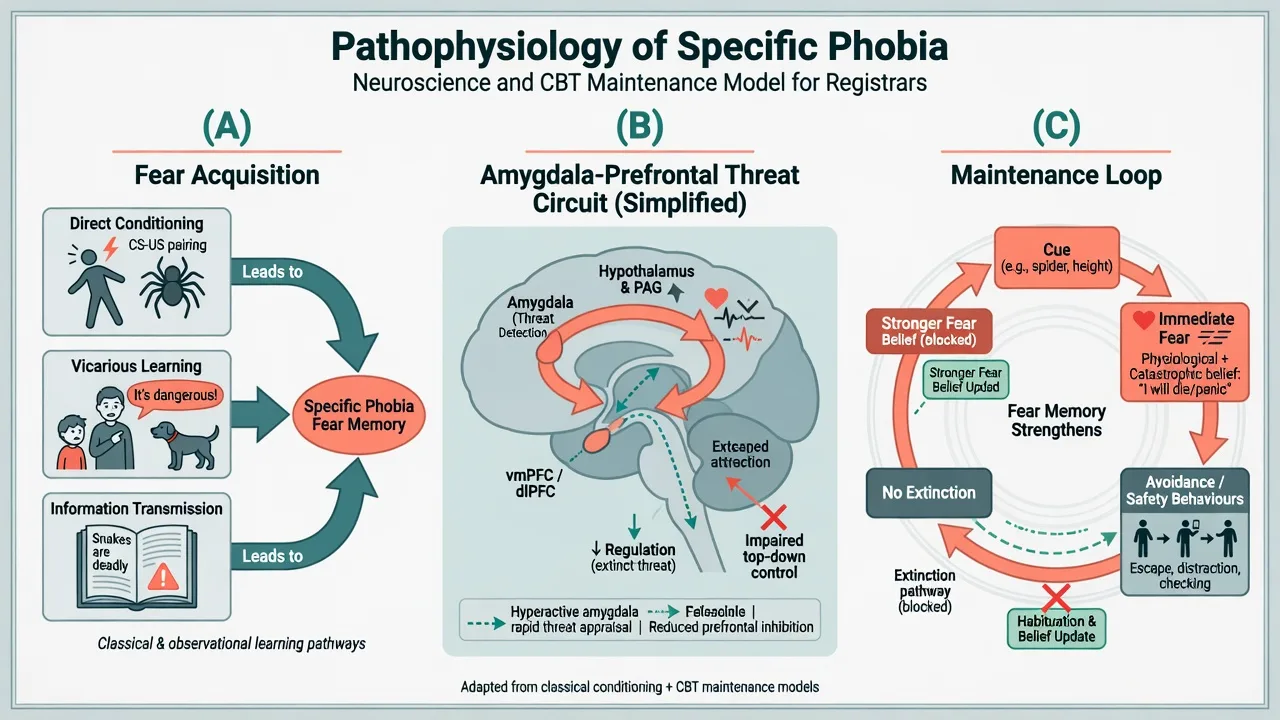
Acquisition. Classical conditioning pairs a neutral cue with aversive outcome; observational/vicarious learning and verbal threat information can establish fear without personal injury. Preparedness accounts for why animal and height fears are common without requiring dramatic trauma histories in every case.[1][3]
Circuits (viva depth, not diagnostic imaging). Group-level models emphasise rapid amygdala-centred threat appraisal with insufficient prefrontal top-down regulation and autonomic activation. Imaging is not an individual diagnostic test.[3]
Maintenance. Avoidance and safety behaviours (looking away, gripping rails, using alcohol before flights, insisting on distraction during blood draws) prevent extinction and preserve catastrophic predictions (“I will faint and die”; “the plane will crash”). Hypervigilance to phobic cues and anticipatory anxiety complete the loop.[3][4]
BII special physiology. Unlike typical phobic sympathetic arousal alone, blood-injection-injury fear often involves a biphasic response with risk of vasovagal syncope. This is why applied tension (raising blood pressure via muscle tensing) is preferred over applied relaxation as the skill package for many BII patients.[9][10]
Clinical presentation
Core features are cue-bound immediate fear, anticipatory anxiety when exposure is expected, and a clear avoidance map. Somatic signs include tachycardia, sweating, tremor, dyspnoea, and urge to escape; BII may add dizziness, nausea, and fainting history. Patients usually retain insight that the fear is excessive but still cannot approach.[1][3]
MSE language. Affect anxious when the cue is discussed; thought content of catastrophe specific to the object; perception normal; cognition intact; insight typically preserved. Quote the patient’s words (e.g. “If I see blood I will pass out and never wake up”).[1][3]
High-yield presentations. Flying phobia blocking career travel; elevator/bridge fears miscalled “agoraphobia”; needle phobia delaying chemotherapy or vaccination; dental phobia with oral sepsis; emetophobia with restrictive eating; multi-phobia clusters; childhood animal phobia persisting into adulthood.[1][17]
Differential diagnosis
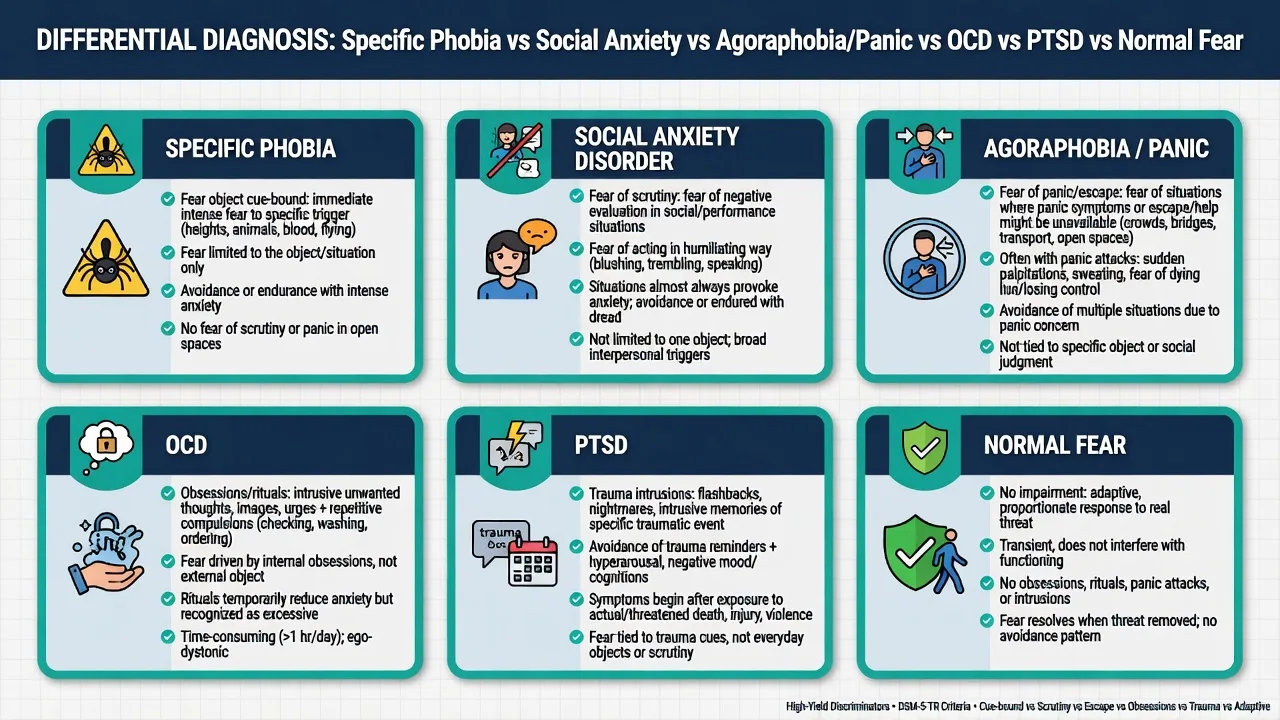
Normal / developmental fear
- Age-appropriate, fades with time
- No marked impairment
- No persistent avoidance of needed activities
- Below duration/impairment threshold
Social anxiety disorder
- Fear of negative evaluation under scrutiny
- Interaction/performance focus
- Not primarily fear of the object itself
- May coexist with performance fears
Panic / agoraphobia
- Fear of panic sensations or restricted escape
- Multiple situation classes
- Not limited to one discrete cue class
- Situational specific phobia is narrower
OCD / PTSD / medical
- OCD: obsessions + rituals drive avoidance
- PTSD: trauma-linked intrusion cluster
- Medical: arrhythmia, hypoglycaemia, vestibular disease
- Substance-induced anxiety
Discriminators score marks. A person who avoids only aeroplanes may still have specific phobia; a person who avoids public transport, open spaces, crowds and being alone outside for fear of panic/escape is agoraphobia until proven otherwise.[1][3][11]
Clinical and bedside assessment
Structure the interview: identify the specific cue(s); confirm almost-always immediate fear; map avoidance and safety behaviours; duration (typically ≥6 months); onset and acquisition story; multi-phobia inventory; BII faint history; dental/medical care delays; substances used to endure; depression and suicide risk; trauma screen; function at work/travel/parenting; prior exposure quality if any therapy tried.[1][4][11]
Document MSE and risk. Suicide risk is mainly via comorbid depression and hopelessness, not the phobia label alone. Capacity is decision-specific (e.g. refusing blood tests). Involuntary care uses local Mental Health Act principles when risk and capacity thresholds are met — statutes are jurisdiction-specific; do not invent section numbers.[11][15]
Measurement. Subjective units of distress (SUDs, 0–100) build hierarchies and track exposure. Phobia-specific inventories and dental fear scales support monitoring; none replace criteria-based diagnosis.[4][14]
Investigations
Routine brain imaging is not indicated for classic early-onset cue-bound phobia. Investigate when late abrupt onset, focal neurology, unexplained syncope (beyond typical vasovagal BII pattern), cardiac symptoms, or substance clues appear. Baseline labs/ECG only as indicated before any pharmacotherapy. Measurement-based care uses SUDs, avoidance ratings and functional goals (completed flight, tolerated blood draw).[3][11]
Management — acute and safety
Vasovagal reaction during BII exposure or procedures. Lie flat/legs elevated as clinically appropriate; protect airway; apply applied-tension skill set once stable; do not force upright confrontation during frank syncope.[9][10]
Severe distress mid-exposure. Pause intensity, re-establish collaboration, resume graded steps — abandoning the entire plan after one under-dosed session is a common failure mode.[4][5]
Management — definitive
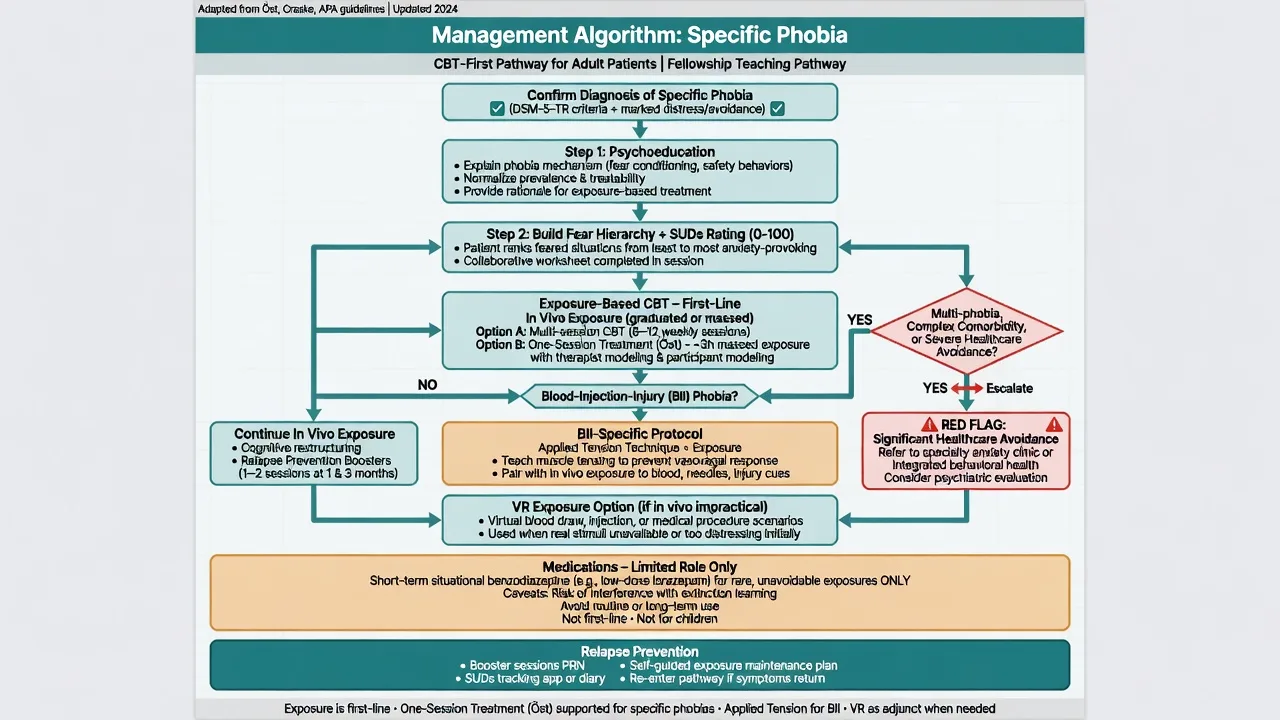
Exposure-based CBT (first-line)
Psychoeducation on fear acquisition and maintenance; collaborative hierarchy ranked by SUDs; in vivo exposure preferred when safe and feasible; drop safety behaviours; remain until fear declines (habituation/extinction learning) or prediction error is processed; between-session homework; cognitive work on overestimated probability/cost of catastrophe. Imaginal exposure and virtual reality can bridge when real cues are inaccessible (flying simulators, height scenes) — evidence continues to evolve as an adjunct, not a replacement for behavioural principles.[4][5][14]
Meta-analytic evidence supports psychological treatments for specific phobia, with exposure-based approaches central. Long-term CBT outcome literature for anxiety-related disorders supports durability when treatment quality is adequate, with residual symptoms predicting relapse risk across anxiety care.[5][13]
One-session treatment (Öst OST)
One-session treatment is therapist-directed, massed exposure typically lasting up to about 3 hours in a single prolonged session (sometimes with follow-up), using graduated steps, therapist modelling, participant modelling, and overlearning (approaching beyond the original goal). It is a high-yield fellowship pearl for animal and other discrete phobias in adults and has RCT and review support in youth.[6][7][8][18]
OST is not “one quick chat.” It is intensive behavioural work requiring preparation, consent, medical considerations (especially BII), and planned maintenance practice.[6][7]
Blood-injection-injury: applied tension
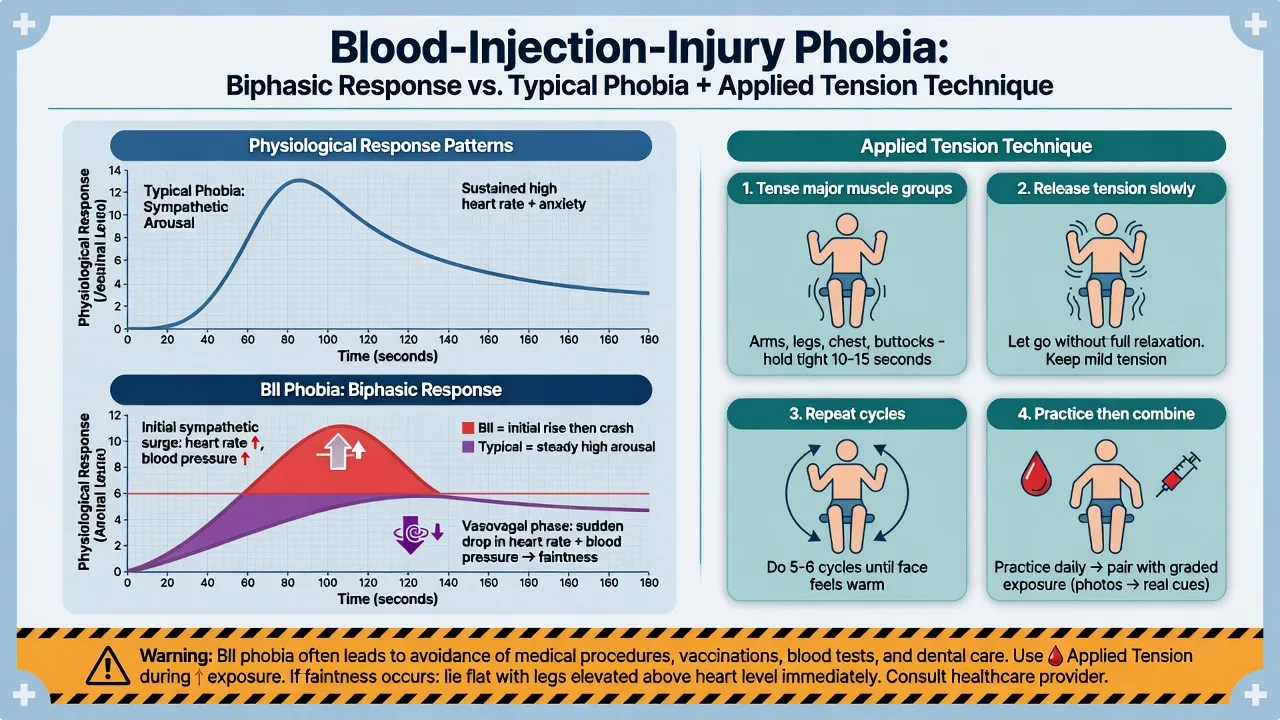
Teach patients to tense major muscle groups (arms, legs, trunk) for roughly 10–15 seconds, release without full relaxation collapse, and cycle the tension while monitoring light-headedness — then combine with graded exposure to blood/injection/injury cues. Trials support applied tension, exposure, and combinations for blood phobia; applied tension addresses the physiology that pure relaxation can worsen.[9][10]
Pharmacotherapy — limited role
For pure specific phobia, medication is not first-line. Short-term benzodiazepines may be considered only as a situational bridge for rare unavoidable exposures (for example a single essential flight) with a stop plan — they risk dependence and can interfere with extinction learning if used as the main strategy. Example exam-level short-term option if used at all: lorazepam 0.5–1 mg orally timed before a defined exposure, single or few doses, no automatic repeats — individualise for age, respiratory disease, alcohol, and driving/flying safety rules. SSRIs/SNRIs treat comorbid depression or other anxiety disorders; they are not the default disease-modifying monotherapy for an isolated discrete phobia the way they are for SAD, panic or GAD.[4][11][12][14]
Canadian anxiety CPGs and WFSBP anxiety guidance frame stepped psychological care for anxiety disorders with pharmacotherapy positioned by syndrome; specific phobia remains the clearest “exposure first, drugs limited” teaching example.[11][12]
Regional notes
ANZ / FRANZCP. Prefer publicly funded or private psychology for exposure/OST; GP shared care for uncomplicated cases; liaison for medical-procedure phobias. Name jurisdiction-specific Mental Health Act only when coercion is considered for comorbid high-risk illness — pure phobia alone rarely meets involuntary thresholds.[4][11] UK / MRCPsych. NICE-aligned psychological first-line ethos; CASC tests plain-language explanation of exposure and why daily diazepam is not the plan.[4][11] US / ABPN. OST and applied tension are classic items; VR exposure appears in contemporary practice questions.[2][6][9][14] India / MD-DNB / NEET-SS. Expect type list, duration, BII pearl, and exposure steps at viva.[1][4]
Subtypes and scenarios
- Animal / discrete cues: prime OST candidates with modelling and overlearning.[6][7]
- Flying / situational: hierarchy from videos to airport to short flights; distinguish from agoraphobia.[1][4]
- BII / dental: applied tension + graded procedures; medical liaison.[9][17]
- Emetophobia / choking (other): high functional impact; careful medical exclusion; graded interoceptive and situational exposures.[1]
- Youth: intensive OST pathways with caregiver involvement; family accommodation is a maintaining factor.[8][18]
- Multi-phobia / complex comorbidity: sequence targets, treat depression, escalate specialist psychology/psychiatry.[11][15]
Complications and pitfalls
Colluding with lifelong avoidance of necessary care; benzodiazepine monotherapy; missing BII vasovagal risk; misdiagnosing agoraphobia or SAD; under-dosed single “try sitting near a dog for 2 minutes” sessions labelled as failed exposure; ignoring depression and suicide risk; cultural dismissal of genuine impairment.[4][5][11][15]
Prognosis and disposition
Untreated course is often chronic with fluctuating life impact. With adequate exposure/OST, response rates are excellent for many discrete phobias; residual avoidance predicts return of fear — plan booster exposures. Uncomplicated cases suit primary care and psychology; specialist input for multi-phobia, severe healthcare refusal, high comorbidity, or failed quality exposure trials.[4][5][13][14]
Special populations
Children and adolescents. Distinguish developmental fears from disorder; school and family accommodation matter; OST has youth RCT and review support.[8][18]
Older adults. Late-onset red flags; falls risk with benzodiazepines; multifactorial fear of falling is not always simple specific phobia.[3][11]
Pregnancy and lactation. Prefer non-drug exposure approaches; untreated medical/needle phobia may block obstetric care — prioritise access.[4][11]
Intellectual disability. Adapted hierarchy, carer coaching, capacity assessment for procedures.[4][11]
Cultural formulation. Feared stimuli and shame about treatment-seeking vary; Indigenous ANZ care requires cultural safety and appropriate supports.[2][11]
Evidence and guidelines
Landmark pillars: Öst one-session treatment; Wolitzky-Taylor meta-analysis of psychological approaches; Choy adult treatment review; Ollendick youth OST RCT; Öst applied-tension blood-phobia trials; Wardenaar WMH epidemiology; Canadian CPG and WFSBP anxiety guidelines for system context; van Dis long-term CBT outcomes; Thng rapid review of adult interventions.[2][4][5][6][8][9][11][12][13][14]
Exam pearls
PHOBIA — specific phobia checklist
References
- [1]LeBeau RT, Glenn D, Liao B, Wittchen HU, et al. Specific phobia: a review of DSM-IV specific phobia and preliminary recommendations for DSM-V Depress Anxiety, 2010.PMID 20099272
- [2]Wardenaar KJ, Lim CCW, Al-Hamzawi AO, Alonso J, et al. The cross-national epidemiology of specific phobia in the World Mental Health Surveys Psychol Med, 2017.PMID 28222820
- [3]Craske MG, Stein MB Anxiety Lancet, 2016.PMID 27349358
- [4]Choy Y, Fyer AJ, Lipsitz JD Treatment of specific phobia in adults Clin Psychol Rev, 2007.PMID 17112646
- [5]Wolitzky-Taylor KB, Horowitz JD, Powers MB, Telch MJ Psychological approaches in the treatment of specific phobias: a meta-analysis Clin Psychol Rev, 2008.PMID 18410984
- [6]Ost LG One-session treatment for specific phobias Behav Res Ther, 1989.PMID 2914000
- [7]Zlomke K, Davis TE 3rd One-session treatment of specific phobias: a detailed description and review of treatment efficacy Behav Ther, 2008.PMID 18721635
- [8]Ollendick TH, Ost LG, Reuterskiöld L, Costa N, et al. One-session treatment of specific phobias in youth: a randomized clinical trial in the United States and Sweden J Consult Clin Psychol, 2009.PMID 19485591
- [9]Ost LG, Fellenius J, Sterner U Applied tension, exposure in vivo, and tension-only in the treatment of blood phobia Behav Res Ther, 1991.PMID 1684704
- [10]Ost LG, Sterner U, Fellenius J Applied tension, applied relaxation, and the combination in the treatment of blood phobia Behav Res Ther, 1989.PMID 2564772
- [11]Katzman MA, Bleau P, Blier P, Chokka P, et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders BMC Psychiatry, 2014.PMID 25081580
- [12]Bandelow B, Allgulander C, Baldwin DS, Costa DLDC, et al. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for treatment of anxiety, obsessive-compulsive and posttraumatic stress disorders - Version 3. Part I: Anxiety disorders World J Biol Psychiatry, 2023.PMID 35900161
- [13]van Dis EAM, van Veen SC, Hagenaars MA, Batelaan NM, et al. Long-term Outcomes of Cognitive Behavioral Therapy for Anxiety-Related Disorders: A Systematic Review and Meta-analysis JAMA Psychiatry, 2020.PMID 31758858
- [14]Thng CEW, Lim-Ashworth NSJ, Poh BZQ, Lim CG Recent developments in the intervention of specific phobia among adults: a rapid review F1000Res, 2020.PMID 32226611
- [15]Choy Y, Fyer AJ, Goodwin RD Specific phobia and comorbid depression: a closer look at the National Comorbidity Survey data Compr Psychiatry, 2007.PMID 17292703
- [16]Depla MF, ten Have ML, van Balkom AJ, de Graaf R Specific fears and phobias in the general population: results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS) Soc Psychiatry Psychiatr Epidemiol, 2008.PMID 18060338
- [17]Oosterink FM, de Jongh A, Hoogstraten J Prevalence of dental fear and phobia relative to other fear and phobia subtypes Eur J Oral Sci, 2009.PMID 19320722
- [18]Davis TE 3rd, Ollendick TH, Öst LG One-Session Treatment of Specific Phobias in Children: Recent Developments and a Systematic Review Annu Rev Clin Psychol, 2019.PMID 30550722