Psych · General adult psychiatry — substance/medication-induced psychosis
Substance/medication-induced psychotic disorder
Also known as Substance-induced psychosis · SIP · Drug-induced psychosis · Medication-induced psychotic disorder · Cannabis-induced psychosis · Methamphetamine-associated psychosis · MAP · Stimulant psychosis · Steroid-induced psychosis · Corticosteroid psychosis · Toxic psychosis
Exam-exhaustive fellowship reference on substance/medication-induced psychotic disorder — DSM-5-TR and ICD-11 criteria, temporal rules versus primary psychosis, cannabis and stimulant and corticosteroid pathways, conversion risk (Starzer, Niemi-Pynttäri, Murrie), acute and definitive management with named doses, dual-diagnosis integrated care, and exam discriminators. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Substance/medication-induced psychotic disorder (SIP/MIP) is one of the highest-yield discriminators in fellowship psychosis stations. Examiners do not want a lay list of "drugs that make you crazy." They want a registrar who can rebuild the timeline, separate intoxication, SIP, primary psychosis with comorbidity, and delirium, name conversion risk by substance, start a dose-levelled antipsychotic plan, and refuse the twin errors of "just drugs — discharge" and "lifelong schizophrenia on day one."[1][4][15]
Overview and definition
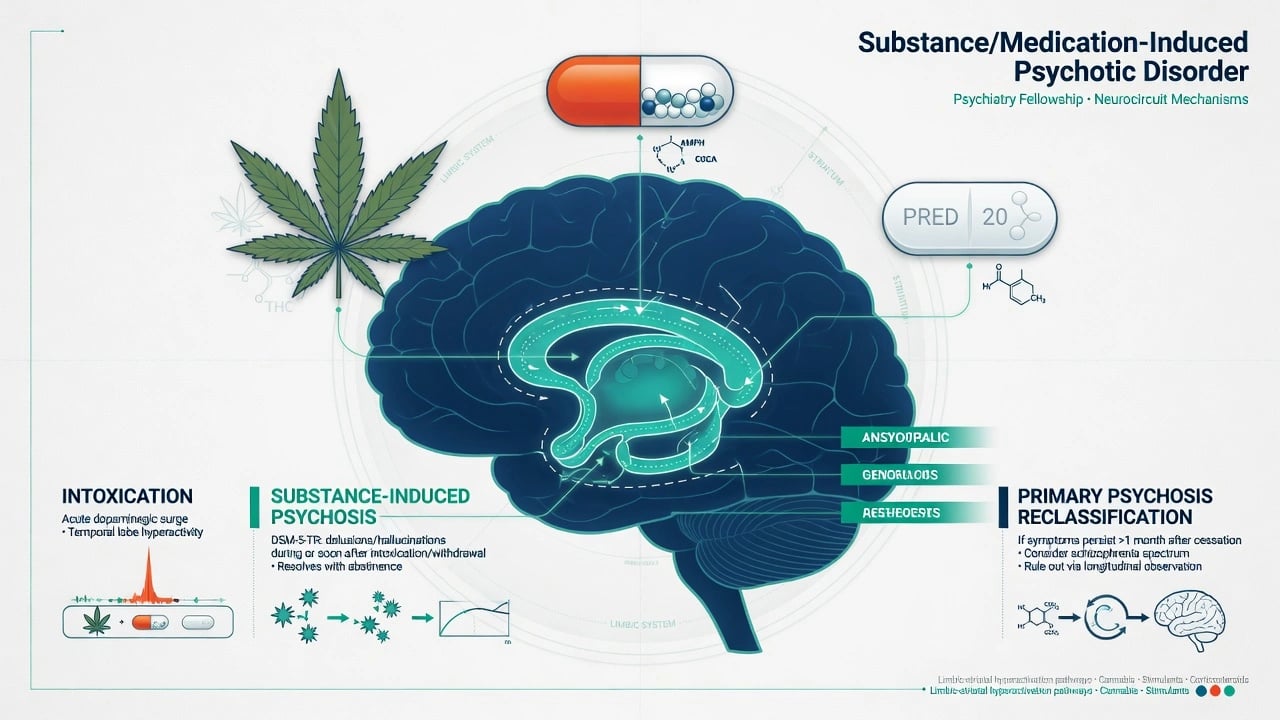
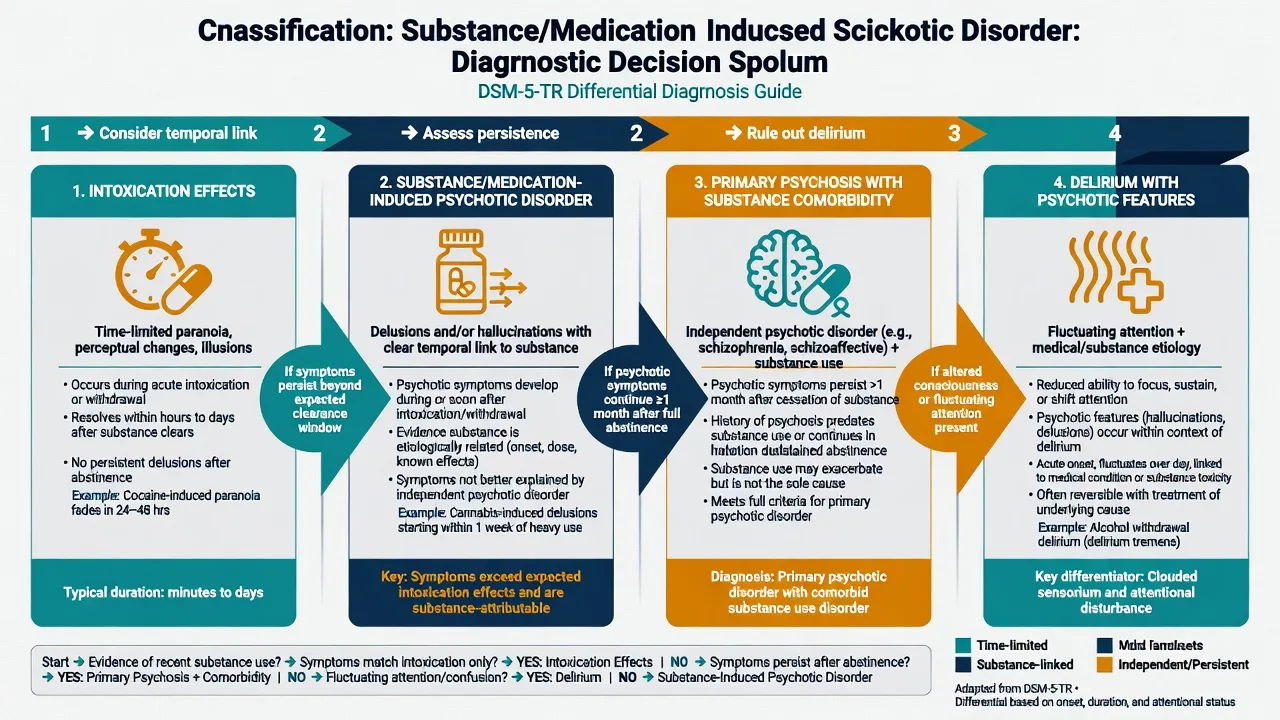
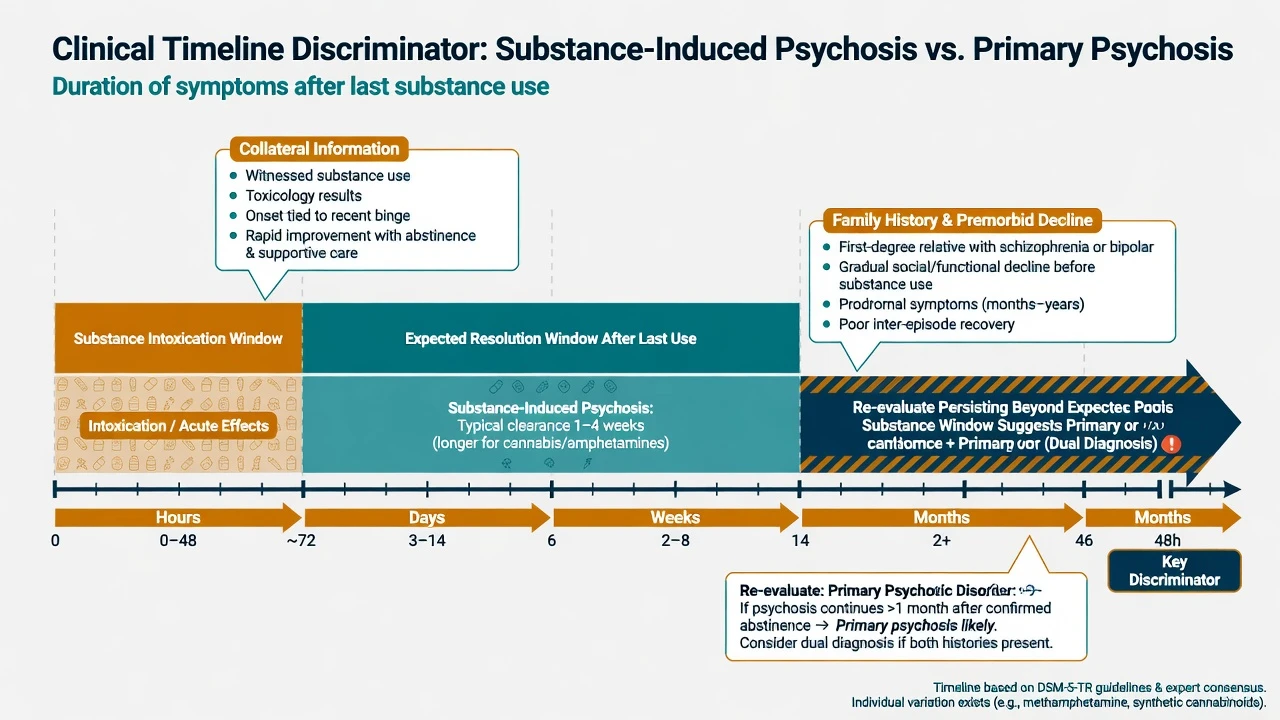
DSM-5-TR framing (examiner skeleton). Substance/medication-induced psychotic disorder requires: (1) prominent delusions and/or hallucinations; (2) evidence from history, examination or labs that symptoms developed during or soon after substance intoxication or withdrawal, or after exposure to a medication capable of producing the symptoms; (3) the disturbance is not better explained by a psychotic disorder that is not substance/medication-induced (for example, symptoms precede onset of use, or persist for a substantial period after cessation of acute intoxication/withdrawal effects); (4) the disturbance does not occur exclusively during the course of delirium; and (5) the disturbance causes clinically significant distress or impairment.[4][15]
Specifiers commonly taught: onset during intoxication versus withdrawal; name the substance (cannabis, amphetamine-type, cocaine, alcohol, hallucinogen, sedative/hypnotic/anxiolytic, other, or unknown; medication-induced when a prescribed agent is causal).[4][15]
ICD-11 places substance-induced psychotic disorder among substance-induced mental disorders, with the substance coded. Medication-induced psychotic presentations (for example high-dose glucocorticoids) sit in the medical-psychiatric interface and are examined under the same timeline logic.[15][18]
What SIP is not. A single positive urine drug screen (UDS) is not a diagnosis. Transient intoxication paranoia that resolves as the drug clears is not automatically SIP of clinical severity. Primary schizophrenia with concurrent cannabis use is not "proved" SIP because the UDS is green for THC.[4][5]
Classification and the four-layer model
Intoxication effects
- During/shortly after use
- Often partial insight recovering as drug clears
- Supportive care may suffice if mild
- Still assess risk and other substances
Substance/medication-induced psychotic disorder
- Temporal link to intoxication/withdrawal/medication
- Prominent delusions/hallucinations with impairment
- May need short-term antipsychotic
- High conversion risk for some substances — follow-up mandatory
Primary psychosis + substance use
- Psychosis independent of recent-use window
- Premorbid decline, family history more common
- EIS/FEP multi-element care
- SUD treatment is secondary prevention
Delirium with psychotic features
- Fluctuating attention and awareness
- Medical instability or withdrawal risk
- Treat underlying cause first
- Do not lock a primary SIP label
Duration rules examiners expect. Nosology uses clinical judgment, not a universal stopwatch. Teaching pearl used across boards: if psychotic symptoms persist substantially beyond the expected physiological window of intoxication or withdrawal for that substance (commonly framed in teaching as roughly about 1 month of persistence after cessation for many substances, with shorter windows for some short-acting agents), reclassify toward primary psychotic disorder or dual pathway rather than pure SIP. Always pair with premorbid course and family history — not the calendar alone.[4][5][15]
Epidemiology and conversion risk
Headline conversion numbers
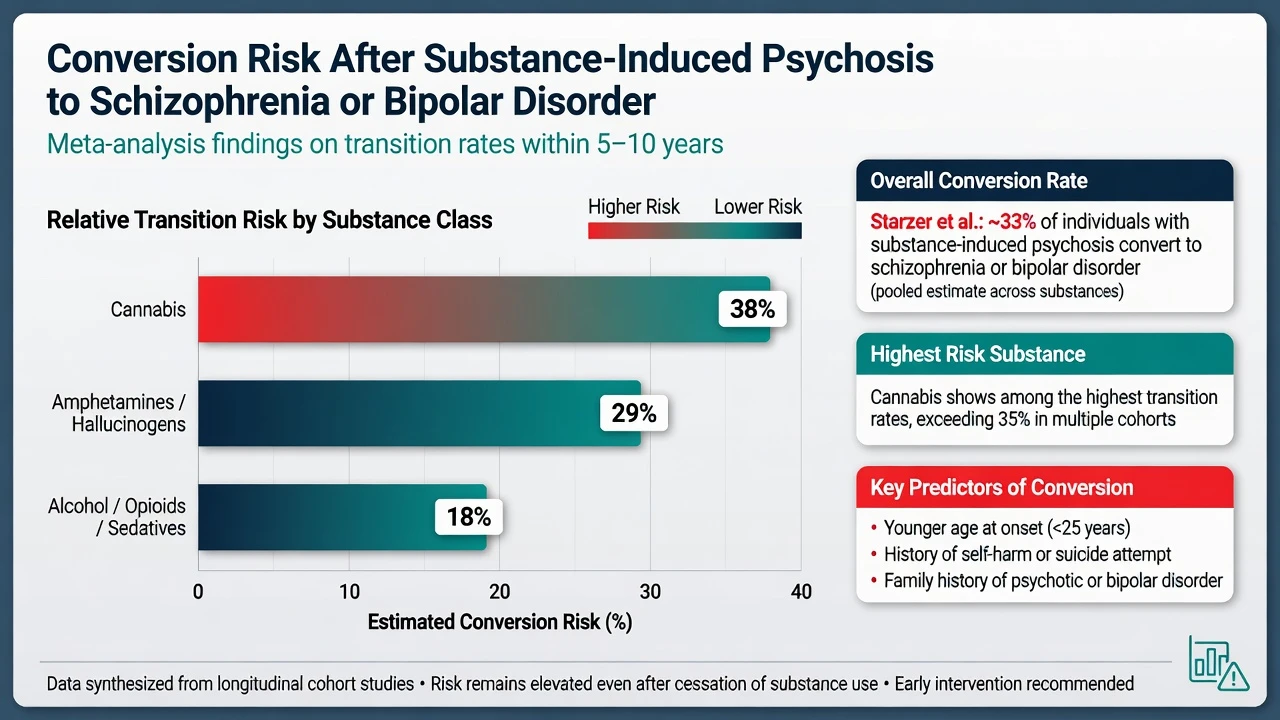
Danish register work (Starzer and colleagues) found roughly one in three people with SIP later received schizophrenia-spectrum or bipolar diagnoses, with cannabis-induced psychosis at the top of the conversion hierarchy. Finnish inpatient register data (Niemi-Pynttäri and colleagues) similarly showed substantial conversion into schizophrenia, varying by substance. Murrie and colleagues' systematic review and meta-analysis estimated pooled transition to schizophrenia after SIP around one quarter, with higher rates for cannabis, hallucinogens and amphetamines than for alcohol, opioids or sedatives.[1][2][3]
Clinical implication. SIP is not a throwaway ED diagnosis. It is a high-risk first presentation that often belongs on an early-intervention or dual-diagnosis follow-up pathway, especially for cannabis and stimulant SIP in young people.[1][3][15]
Pathophysiology (viva depth)
Dopamine as final common pathway. Howes and Kapur's dopamine hypothesis version III remains the cleanest viva scaffold: multiple upstream factors (including substance exposure) can produce striatal hyperdopaminergia that maps onto positive psychotic symptoms. Stimulants are the pharmacological demonstration case; cannabis (THC via CB1 networks) modulates circuits that interface with dopamine and glutamate; glucocorticoids perturb mood, sleep and cognition with dose-related neuropsychiatric risk.[11][13][18]
Cannabis. Systematic reviews and dose–response meta-analyses link higher frequency and higher-THC products to increased psychotic outcomes and to population-level incidence variation (Di Forti / EU-GEI). Adolescent onset amplifies long-term risk framing in longitudinal literature. This is not "one joint equals schizophrenia" — it is dose, potency, age and vulnerability interacting.[6][7][8][9]
Methamphetamine / amphetamine-type stimulants (ATS). Prospective work (McKetin and colleagues) shows dose-related psychotic symptoms in chronic users and elevated violent behaviour risk during use periods. Methamphetamine-associated psychosis (MAP) can recur with re-exposure — examiners like the kindling language if you keep it evidence-tethered.[11][12]
Corticosteroids / medications. High-dose systemic glucocorticoids produce a spectrum from insomnia and irritability through mania to frank psychosis. Risk rises with dose. Management is co-owned with the medical team (taper or alternate regimen when safe) plus psychotropics as bridge.[18]
Clinical presentation
Common MSE pattern. Persecutory delusions, referential ideas, auditory hallucinations; visual and tactile phenomena (including formication with stimulants) appear more often than in classic primary schizophrenia teaching cases. Affect may be anxious, irritable or labile rather than flat. Insight is often partial and may recover faster than in established schizophrenia if the substance is stopped — but do not rely on that hope for discharge planning.[4][11]
Cannabis-associated SIP. Young adult, high-THC product, paranoia and anxiety prominent, often first contact with services. Family may minimise "just weed." Conversion risk is among the highest — take it seriously.[1][8]
Stimulant / MAP. Intense paranoia, agitation, sleeplessness, possible aggression; medical toxicity (hypertension, hyperthermia, cardiac risk) may dominate the first hour. Crash phase brings dysphoria and suicide risk.[11][12]
Steroid-induced. Medical ward context (COPD flare, autoimmune disease, oncology). Insomnia, grandiosity or mixed features, then psychosis. Check the drug chart every time.[18]
Polysubstance and synthetics. Synthetic cannabinoids and cathinones can produce severe, medically unstable presentations. UDS may miss them — timeline and collateral remain essential.[4][11]
Differential diagnosis — discriminators, not lists
| Feature | Favours SIP | Favours primary psychosis + use | Favours delirium / organic |
|---|---|---|---|
| Onset | Close temporal link to use/med | Premorbid decline; use secondary or incidental | Hours–days with medical insult |
| Attention | Usually relatively preserved | Usually preserved | Fluctuating |
| Family history of psychosis | Less often | More often | Variable |
| After abstinence | Clears within expected window | Persists weeks+ | Tracks medical course |
| Hallucination type | Visual/tactile more common | Auditory more classic | Mixed; misperceptions |
| Exam red flags | Intoxication signs | Negative symptoms, formal thought disorder lasting | Fever, focal neurology, seizure |
| Caton and colleagues showed demographic, family and clinical differences between early-phase primary psychotic disorders with concurrent substance use and SIP; follow-up work showed substantial diagnostic stability, with a minority of SIP reclassifying — often because psychosis persisted without ongoing use. Use the table discriminators above together with that longitudinal logic, not any single cell alone.[4][5] |
Also exclude: affective psychosis (especially mania after stimulants or steroids), autoimmune encephalitis and other organic psychoses when red flags fire, alcohol withdrawal delirium versus alcohol hallucinosis, OCD with poor insight, trauma-related phenomena without true delusions.[4][15][18]
Assessment
Structure the interview like a reconstruction, not a checkbox: rebuild timeline (first use, pattern, last use clock time, route, estimated dose/potency, onset of psychosis relative to use, prior SIP episodes); assess premorbid function; obtain collateral (family, friends, ambulance, records — self-report alone is unreliable in acute paranoia); document MSE examples, insight and capacity; assess risk (suicide including post-stimulant crash, violence, vulnerability, absconding, child protection, driving, weapons); diagnose the SUD axis independently when criteria are met; apply local Mental Health Act principles for involuntary treatment when risk and capacity criteria are met — do not invent section numbers for the wrong jurisdiction.[4][11][15]
Investigations
- Vital signs, capillary glucose, focused neurological exam; UDS / serum toxicology are supportive, not dispositive (false negatives for synthetics/timing and clinical over-reading both common).[4][15]
- Before antipsychotics: weight/BMI, BP, glucose or HbA1c, lipids, FBC, U&E, LFT, ECG for QTc; pregnancy test when applicable.[14][15]
- Escalate neuroimaging, EEG, autoimmune panel, infectious serology when red flags (late onset, fever, seizure, focal signs, rapid cognitive decline, catatonia).[15]
- Steroid cases: review full medication list and medical plan for taper feasibility.[18]
Acute / emergency management
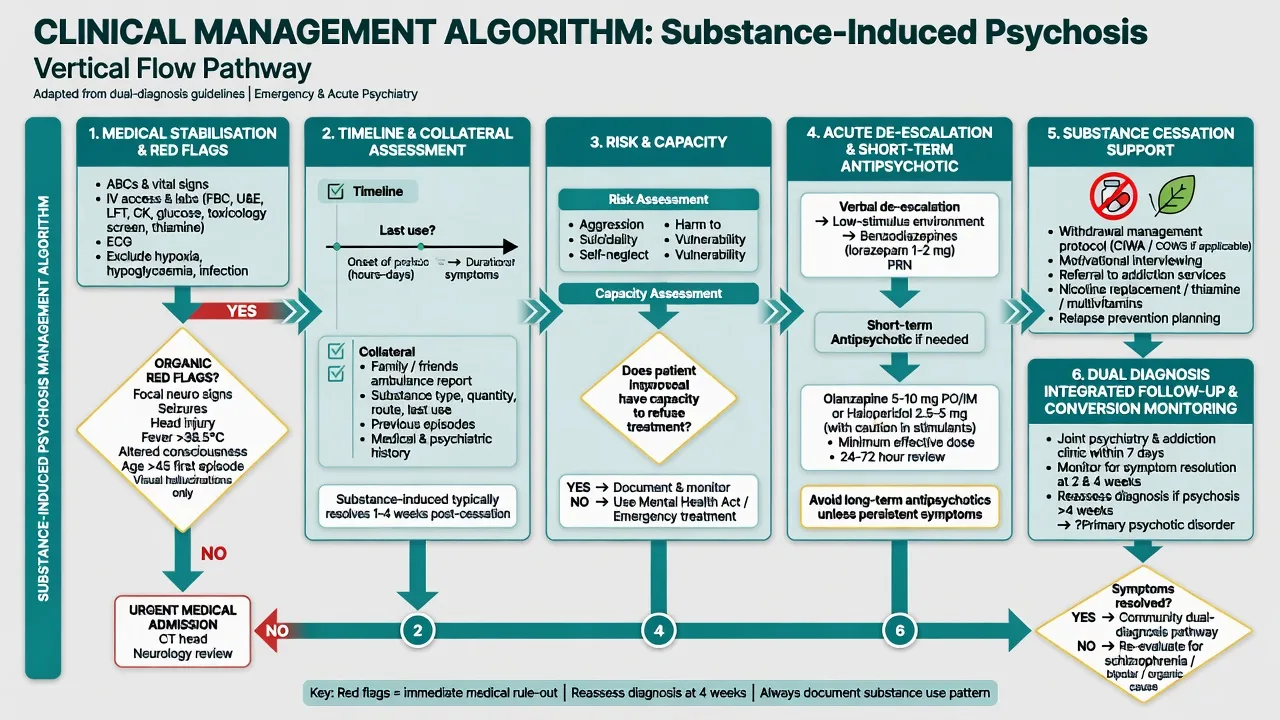
Acute sequence: medical first for stimulant toxicity, alcohol withdrawal risk, head injury, hypoxia or hypoglycaemia; low-stimulus environment and staff safety; de-escalation before pharmacological restraint when safe; benzodiazepines for severe agitation when indicated — example lorazepam 1–2 mg oral or IM, repeat with observation for oversedation/airway per local rapid-tranquillisation protocol; antipsychotic when psychosis/agitation persists after medical clearance (named starts below); avoid intramuscular olanzapine combined with parenteral benzodiazepines (cardiorespiratory caution in many protocols); document legal status, contact family, and restrict means if suicide risk is active.[11][14][15]
Definitive management
Substance and medication interventions
- Cease the culprit substance as the primary disease-modifying step when achievable; use motivational interviewing, brief intervention, and structured SUD pathways.[16]
- Cannabis: frequency and high-THC continuation after psychosis onset associate with worse course; cessation support is secondary prevention, not optional lifestyle chat.[10]
- Stimulants: psychosocial package (contingency management, CBT-based programmes) has the best evidence base for use disorder; pharmacotherapy for methamphetamine use disorder remains limited — treat psychosis and medical risk concurrently, not sequentially.[11][16]
- Corticosteroids: taper or switch with the treating team when medically safe; psychotropics bridge severe affective/psychotic symptoms.[18]
Antipsychotic pharmacotherapy (name dose, route, monitoring)
For ongoing psychotic symptoms after medical stabilisation, start a second-generation antipsychotic at a cautious first-episode-style dose, obtain baselines, and review early. Example oral starts examiners expect you to name: olanzapine 5–10 mg at night (sedation helpful; metabolic monitoring from day one); risperidone 1–2 mg daily with titration (EPS/prolactin vigilance); aripiprazole 10 mg daily (akathisia education; relatively favourable metabolic profile). Dose selection should respect international consensus ranges and local formulary; first presentations and young people are often more sensitive — start low, monitor, do not "blast."[14][15]
Trial length. Assess response over roughly 2–6 weeks at a therapeutic dose with adherence support for persistent primary-leaning pictures; pure short SIP may clear faster as the substance clears — do not continue high-dose polypharmacy out of habit.[14][15]
How long to continue after remission of SIP? No single universal duration rule equals schizophrenia maintenance dogma. Shared decision-making: higher conversion-risk substances (cannabis, amphetamines), incomplete abstinence, family history, and residual symptoms argue for longer supervised treatment and dual-aware follow-up (months, often into the year+ range); clean timeline, rapid full recovery with confirmed abstinence, and no risk factors may allow earlier supervised taper with a written early-warning plan. Reclassify promptly if psychosis persists offline from substance use.[1][3][5][15]
Dual diagnosis interface
Historical sequential care ("treat addiction first" or "treat mental illness only after perfect abstinence") fails service users and fails exams. Integrated models (Drake and colleagues) and dual-diagnosis guidance emphasise concurrent treatment of severe mental illness and substance misuse, stage-matched motivational work, and no-wrong-door systems. Cochrane synthesis of psychosocial interventions for SMI plus substance misuse shows modest/complex evidence — clinically you still deliver concurrent, coordinated care rather than ping-pong exclusion.[16][17][15]
Practical dual plan elements: one shared formulation (psychosis pathway + SUD pathway); named case coordinator with joint mental health and AOD goals; MI/CBT for substance use plus family psychoeducation; crisis plan covering both psychosis relapse and substance binge; EIS/FEP referral when first presentation or high conversion-risk profile.[15][16][17]
Psychosocial and recovery
Family education reduces chaos and improves detection of early warning signs. Sleep, nutrition, and housing stabilisation matter. Vocational and education goals should not wait for mythical total purity. Link to related FEP pathway content when this is a first psychotic contact.[15]
Subtypes and high-yield scenarios
- Cannabis-induced psychotic disorder — high conversion; potency and frequency counselling; EIS interface.[1][8][9]
- Methamphetamine-associated psychosis — medical toxicity, violence risk, dose relationship, recurrent binges.[11][12]
- Steroid/medication-induced psychosis — CL psychiatry, drug chart, co-managed taper.[18]
- Alcohol-related psychotic presentations — separate withdrawal delirium (medical emergency) from alcohol-induced psychotic disorder; thiamine and withdrawal protocols where indicated.[2][15]
- Persistent psychosis after documented abstinence — reclassify toward primary psychosis; full FEP package.[5]
Complications and pitfalls
Classic examinable errors: discharging high-risk SIP without follow-up; withholding antipsychotics because UDS is positive; missing delirium/encephalitis red flags; missing steroids on the medication list; overcalling lifelong schizophrenia on first night of intoxication; under-dosing risk assessment in stimulant paranoia; iatrogenic metabolic harm from unmonitored olanzapine/polypharmacy; and sequential dual-diagnosis service exclusion.[1][14][15][16][18]
Prognosis and disposition
Better prognostic features: clear temporal link, rapid abstinence, good premorbid function, no family history, short episode, older age relative to adolescent peak.[1][4]
Worse: young age, cannabis or amphetamine SIP, ongoing use, self-harm after SIP, premorbid decline, incomplete recovery.[1][3]
Disposition ladder: medical resus → psychiatric inpatient when risk/incapacity → community dual-diagnosis / EIS step-down with written crisis plan. Half of conversions in long register follow-up occur over years — plan longitudinal dual-aware care, not a single clinic letter.[1]
Special populations
Adolescents need high-THC cannabis counselling, family engagement, school and safeguarding; older adults need intensified organic work-up and medication review; pregnancy needs capacity assessment, safeguarding of fetus/infant, specialist perinatal liaison, and careful medication choice with teratogenicity discussion — no casual polypharmacy; ID / autism presentations require attention to baseline communication style and avoidance of diagnostic overshadowing; cultural / Indigenous contexts need non-stigmatising dual formulation and family/community structures without moralising substance use while holding risk; forensic interface uses intoxication and violence assessment principles, with fitness and responsibility issues kept jurisdiction-specific — state principles, not invented statutes.[1][8][12][15]
Evidence and guidelines (named)
- Starzer 2018 — conversion rates and predictors after SIP.[1]
- Niemi-Pynttäri 2013 — large Finnish conversion register.[2]
- Murrie 2020 — meta-analysis of transition by substance class.[3]
- Caton 2005/2007 — discrimination and stability of SIP vs primary with concurrent use.[4][5]
- Moore, Marconi, Di Forti, Schoeler — cannabis risk, potency, incidence, post-onset continuation.[6][7][8][9][10]
- McKetin — methamphetamine dose–psychosis and violence.[11][12]
- Howes–Kapur — dopamine final common pathway.[13]
- Gardner — antipsychotic dosing consensus.[14]
- RANZCP schizophrenia and related disorders guideline (Galletly) — substance comorbidity and psychosis care principles in ANZ.[15]
- Drake integrated dual treatment; Hunt Cochrane — dual diagnosis care framing.[16][17]
- Brown and Chandler — corticosteroid neuropsychiatric effects.[18]
Regional deltas. RANZCP emphasises comprehensive psychosis care including substance comorbidity. NICE dual-diagnosis principles stress concurrent care and avoiding exclusion. APA framing similarly rejects sequential "treat one first only" systems. Local rapid-tranquillisation and Mental Health Act details vary — state principles and cite local protocol in clinical practice.[15][16]
Exam pearls
- Timeline + collateral beat a single UDS.[4]
- Cannabis SIP is high conversion risk — never dismiss as trivial.[1][3]
- Persistence substantially beyond expected substance window → reclassify.[5]
- Steroids: always check the drug chart.[18]
- Integrated dual care, not sequential ping-pong.[16]
- Name agent, dose, route, monitoring for any antipsychotic started.[14]
- Do not invent Mental Health Act section numbers across jurisdictions — state local principles only.[15]
- Follow-up duration should respect conversion lag of years, not hours.[1]
Region notes
ANZ (primary). Use RANZCP schizophrenia and related disorders guidance for psychosis care and substance comorbidity principles; local health service dual-diagnosis and EIS pathways; jurisdiction-specific Mental Health Act for involuntary treatment. Methamphetamine ("ice") presentations are high-yield in Australian ED psychiatry.[11][15]
UK. MRCPsych expects SIP vs primary discriminators, NICE-aligned dual-diagnosis concurrent care language, and CASC communication without moralising.[4][16]
US / ABPN. DSM-5-TR criteria language; medication-induced psychosis including steroids; integrated dual disorder treatment concepts.[16][18]
India / MD-DNB / NEET-SS. Classic viva on cannabis and stimulant psychosis, steroid psychosis on medical wards, and conversion risk; dose-levelled antipsychotic answers required.[1][14][18]
References
- [1]Starzer MSK, Nordentoft M, Hjorthøj C Rates and Predictors of Conversion to Schizophrenia or Bipolar Disorder Following Substance-Induced Psychosis Am J Psychiatry, 2018.PMID 29179576
- [2]Niemi-Pynttäri JA, Sund R, Putkonen H, et al. Substance-induced psychoses converting into schizophrenia: a register-based study of 18,478 Finnish inpatient cases J Clin Psychiatry, 2013.PMID 23419236
- [3]Murrie B, Lappin J, Large M, et al. Transition of Substance-Induced, Brief, and Atypical Psychoses to Schizophrenia: A Systematic Review and Meta-analysis Schizophr Bull, 2020.PMID 31618428
- [4]Caton CL, Drake RE, Hasin DS, et al. Differences between early-phase primary psychotic disorders with concurrent substance use and substance-induced psychoses Arch Gen Psychiatry, 2005.PMID 15699290
- [5]Caton CL, Hasin DS, Shrout PE, et al. Stability of early-phase primary psychotic disorders with concurrent substance use and substance-induced psychosis Br J Psychiatry, 2007.PMID 17267925
- [6]Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review Lancet, 2007.PMID 17662880
- [7]Marconi A, Di Forti M, Lewis CM, et al. Meta-analysis of the Association Between the Level of Cannabis Use and Risk of Psychosis Schizophr Bull, 2016.PMID 26884547
- [8]Di Forti M, Marconi A, Carra E, et al. Proportion of patients in south London with first-episode psychosis attributable to use of high potency cannabis: a case-control study Lancet Psychiatry, 2015.PMID 26359901
- [9]Di Forti M, Quattrone D, Freeman TP, et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study Lancet Psychiatry, 2019.PMID 30902669
- [10]Schoeler T, Petros N, Di Forti M, et al. Effects of continuation, frequency, and type of cannabis use on relapse in the first 2 years after onset of psychosis: an observational study Lancet Psychiatry, 2016.PMID 27567467
- [11]McKetin R, Lubman DI, Baker AL, et al. Dose-related psychotic symptoms in chronic methamphetamine users: evidence from a prospective longitudinal study JAMA Psychiatry, 2013.PMID 23303471
- [12]McKetin R, Lubman DI, Najman JM, et al. Does methamphetamine use increase violent behaviour? Evidence from a prospective longitudinal study Addiction, 2014.PMID 24400972
- [13]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [14]Gardner DM, Murphy AL, O'Donnell H, et al. International consensus study of antipsychotic dosing Am J Psychiatry, 2010.PMID 20360319
- [15]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [16]Drake RE, Mercer-McFadden C, Mueser KT, et al. Review of integrated mental health and substance abuse treatment for patients with dual disorders Schizophr Bull, 1998.PMID 9853791
- [17]Hunt GE, Siegfried N, Morley K, et al. Psychosocial interventions for people with both severe mental illness and substance misuse Cochrane Database Syst Rev, 2019.PMID 31829430
- [18]Brown ES, Chandler PA Mood and cognitive changes during systemic corticosteroid therapy Prim Care Companion J Clin Psychiatry, 2001.PMID 15014624