Psych · General adult psychiatry — mood disorders
Treatment-resistant depression
Also known as TRD · Treatment refractory depression · Refractory major depression · Difficult-to-treat depression · Antidepressant non-response · STAR*D sequential depression treatment
Exam-exhaustive fellowship reference on treatment-resistant depression — operational definitions and staging, pseudo-resistance, STAR*D sequential logic, switch and augmentation (lithium, T3, atypical antipsychotics), ECT, rTMS, ketamine/esketamine, psychotherapy, medical exclusion, and measurement-based care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Treatment-resistant depression (TRD) is a high-yield fellowship topic because it tests whether you can re-diagnose under pressure, define an adequate trial, sequence next steps with named drugs and monitoring, and escalate to ECT/rTMS/ketamine without folklore. Examiners punish both premature polypharmacy and endless incomplete trials while suicide risk smoulders.[1][6][19]
Overview and definition
TRD is a treatment-outcome construct layered on a depressive disorder diagnosis (usually MDD), not a freestanding DSM-5-TR or ICD-11 diagnosis. The most widely used operational definition for exams is failure of two or more adequate antidepressant trials (different agents or mechanisms, therapeutic dose, sufficient duration, verified adherence) in the current episode, with non-response or non-remission on measurement.[6]
Outcomes language you must use precisely. Response commonly means ≥50% reduction on a severity scale (e.g. PHQ-9, HAM-D, MADRS); remission means near-absent symptoms / scale below a remission threshold with functional recovery; partial response is meaningful improvement that is not remission; non-response is failure to meet the response threshold after an adequate trial; relapse/recurrence is symptom return after remission (timing definitions vary by trial). Response is not success if residual symptoms leave the patient disabled or suicidal. STAR*D taught that incomplete remission is common and costly.[1][2][20]
Adequate trial (exam mantra). Right diagnosis, right drug, therapeutic dose, about 4–6 weeks (sometimes longer if slow partial response), verified adherence, addressed substances and medical confounders, and measured outcome — before declaring failure.[2][17]
Classification and staging
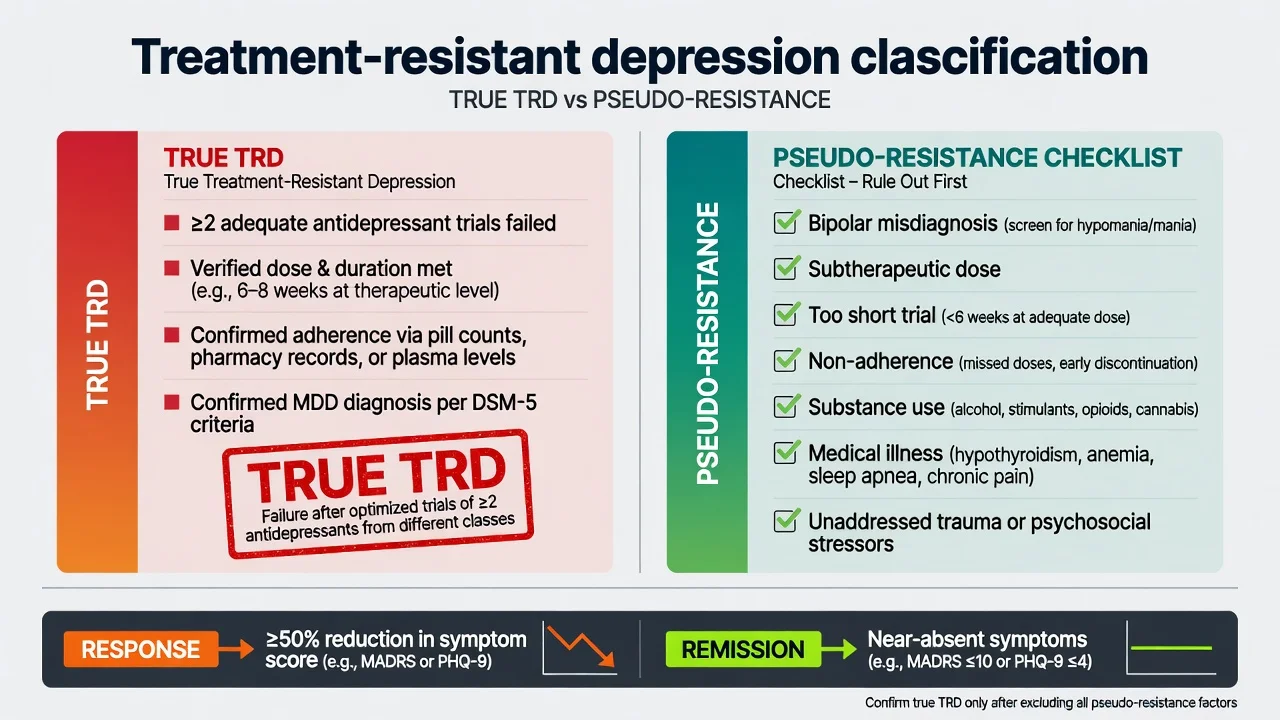
True TRD (construct)
- Confirmed depressive diagnosis (usually MDD)
- ≥2 adequate antidepressant trials failed
- Dose, duration, adherence verified
- Outcome measured (not 'felt a bit better')
Pseudo-resistance
- Misdiagnosis (bipolar, mixed features, medical)
- Subtherapeutic dose or too-short trial
- Non-adherence / intolerance without optimisation
- Ongoing substances, untreated OSA, thyroid disease
Staging concepts
- Thase–Rush-style stages by number/type of failed trials
- European multi-axial staging (resistance + chronicity)
- ATHF-style structured treatment history quality
- Staging guides intensity — not a substitute for formulation
Related labels
- Difficult-to-treat depression (broader service term)
- Chronic depression / persistent depressive disorder
- Partial responders with residual symptoms
- Treatment-intolerant (failed trials from adverse effects)
Staging systems vary; say which framework you are using and do not invent numeric cut-offs not supported by your source. Gaynes and colleagues summarise definition heterogeneity and the practical need for clear operational criteria in research and care.[6]
Epidemiology and risk factors
Numbers examiners expect
In STAR*D, roughly one-third of outpatients remitted with first-step citalopram under systematic measurement-based care; subsequent steps still helped some patients, but absolute remission rates fell as treatment resistance accumulated.[1][2]
Predictors of poorer response include greater severity and chronicity, anxious distress, early trauma, medical comorbidity, substance use, prior treatment failures, and residual symptoms after partial response. TRD is over-represented in suicide deaths relative to remitters — risk assessment is continuous, not a one-off checkbox.[1][19]
Pathophysiology and mechanisms
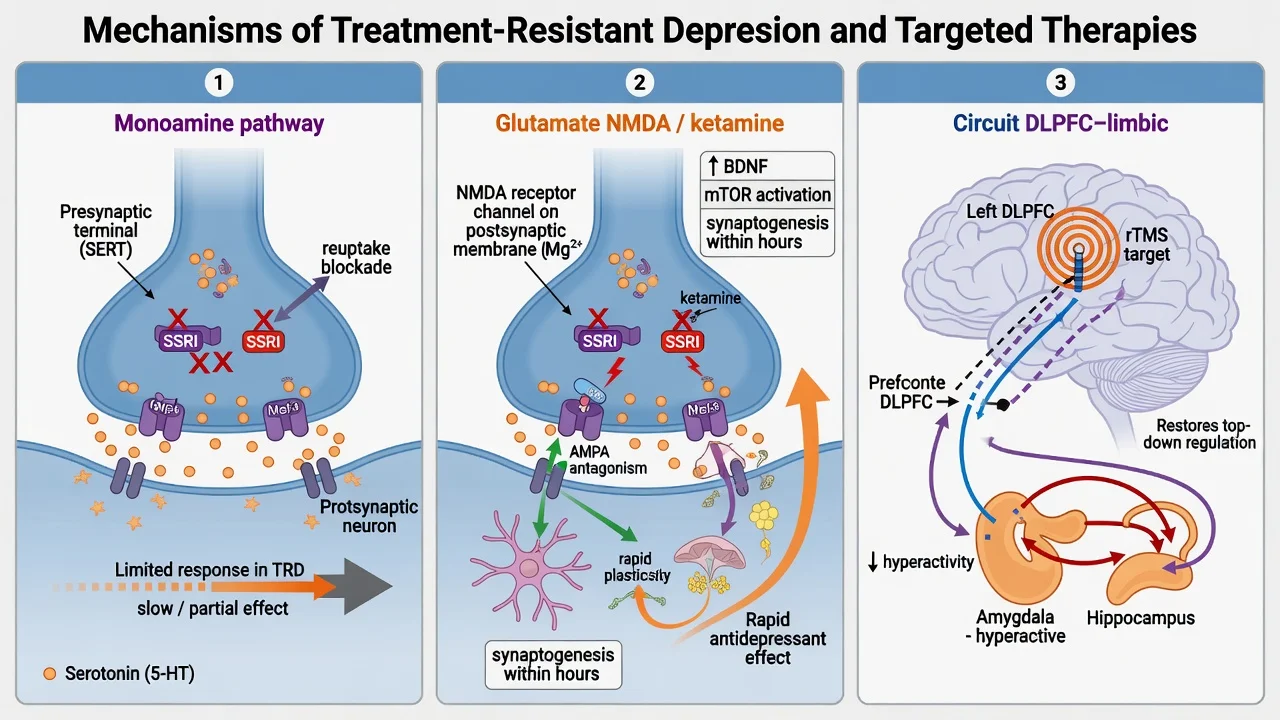
Monoamine model — necessary but incomplete. SSRIs/SNRIs/TCAs/MAOIs act primarily on 5-HT, noradrenaline and/or dopamine signalling. Limits that matter in TRD: delayed clinical response despite rapid reuptake blockade; substantial non-remission; residual symptoms despite "response."[17]
Glutamate / NMDA and plasticity. Subanaesthetic ketamine produced rapid antidepressant effects in treatment-resistant major depression, supporting glutamatergic and synaptic plasticity models beyond classical monoamines.[7][8] Esketamine programmes extend this into regulated clinical pathways with monitoring infrastructure.[9][10]
Circuit model and neuromodulation targets. Prefrontal–limbic dysregulation is a group-level research framing; high-frequency rTMS over left dorsolateral prefrontal cortex (DLPFC) is the classic exam target for non-invasive stimulation in MDD/TRD pathways.[12][13][18]
Psychological maintaining factors. Avoidance, rumination, interpersonal role strain, and behavioural inactivation sustain residual symptoms — pharmacological escalation without psychotherapy often underperforms the combined plan.[19]
Clinical presentation
Patients referred as "TRD" may present with persistent low mood and anhedonia despite multiple scripts; residual insomnia, anxiety, cognitive fog, and anergia after partial response; chronic passive death wishes or intermittent active ideation; functional collapse (work, relationships, self-care) out of proportion to a "mild" scale score if the patient minimises symptoms; and treatment-emergent activation, mixed features, or covert bipolarity mislabelled as unipolar TRD.[1][19]
High-acuity TRD phenotypes. Melancholic severity, psychotic depression, catatonia, and life-threatening poor intake change the algorithm toward ECT, not another incomplete SSRI switch.[11][19]
Differential diagnosis — and the pseudo-resistance checklist
Bipolar / mixed
- Prior hypo/mania is decisive when present
- Family history, postpartum mania, early highly recurrent course
- Mixed features during depression
- Do not escalate unipolar antidepressant monotherapy
Substance / medication
- Alcohol, cannabis, stimulants, sedatives
- Steroids, interferon, some antihypertensives
- Timeline locked to exposure
- Treat dual formulation in parallel
Medical / organic
- Hypothyroidism, B12, anaemia, OSA
- Neurological disease, stroke, Parkinson
- Delirium with dysphoria — fluctuation
- Late first onset or focal signs → investigate
Other psychiatric
- PTSD, OCD, primary anxiety with demoralisation
- Personality (borderline affective instability)
- ADHD with chronic underachievement
- Grief / adjustment mislabelled as TRD
Differential discriminators must be stated explicitly — lists without discriminators fail fellowship exams.[6][19]
Clinical and bedside assessment
Structure the TRD reassessment interview: (1) confirm current episode criteria and severity (MSE language, function, psychosis, catatonia); (2) bipolar screen every time; (3) reconstruct treatment history (agent, dose, duration at therapeutic dose, adherence, side-effects, response/partial/none, reason stopped); (4) substances, trauma, medical/medication list, perinatal status, supports; (5) suicide and self-neglect risk with means, intent, plan, protective factors; (6) capacity and least-restrictive legal pathway if risk is high (jurisdiction-specific statutes — do not invent section numbers); (7) collateral and prior records when available.[2][19][20]
Measurement-based care. Serial PHQ-9 (or clinician-rated HAM-D/MADRS in trials) plus CGI and side-effect review. PHQ-9 item 9 is a screen for passive/active thoughts — not a complete risk assessment.[2][20]
Investigations
Typical adult set before next-step agents: TSH, FBC, U&E, LFT; glucose/lipids and BMI if starting atypical antipsychotic or metabolic risk present; ECG when cardiac risk, older age, TCA planned, high-dose citalopram/escitalopram, or lithium pathway; pregnancy test when relevant; urine drug screen when substance contribution is plausible; B12/folate if indicated; sleep study referral when OSA suspected; neuroimaging only for late first onset, focal neurology, or cognitive red flags — not routine classic TRD work-up. Before lithium: renal function, electrolytes, thyroid, pregnancy status, ECG as indicated; plan serum level monitoring.[17][19]
Management — acute risk and resuscitation
Manage acute suicidal crisis with collaborative safety planning, means restriction, and care intensity matched to dynamic risk. Medical emergencies of TRD treatments include lithium toxicity, serotonin syndrome, NMS (if antipsychotics used), TCA overdose, and hypertensive crisis on classical MAOIs with dietary/drug interactions.[19]
Management — definitive and stepwise
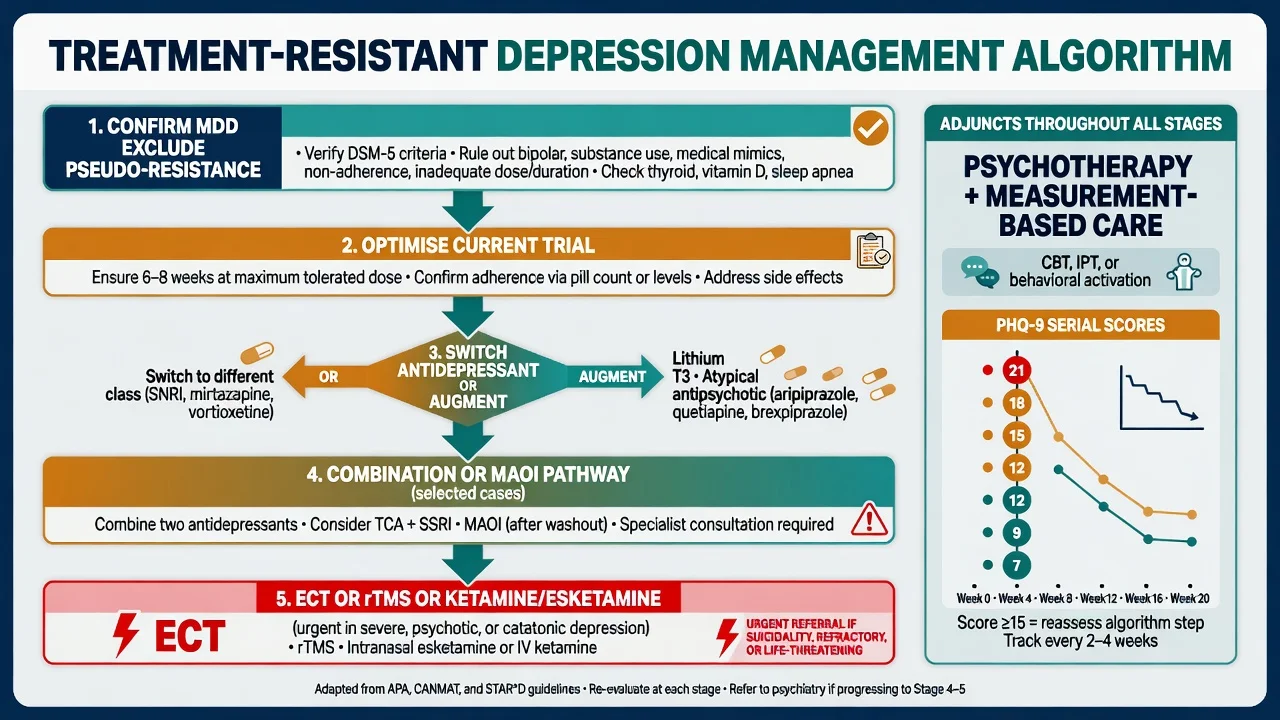
Step 0 — Stop calling it TRD until the checklist is clean
Optimise the current agent if the trial was never adequate. Fix adherence barriers (sexual side-effects, cost, cognition). Treat alcohol/substance use. Correct hypothyroidism. Re-open bipolar differential.[6][17]
STAR*D sequential logic (core exam content)
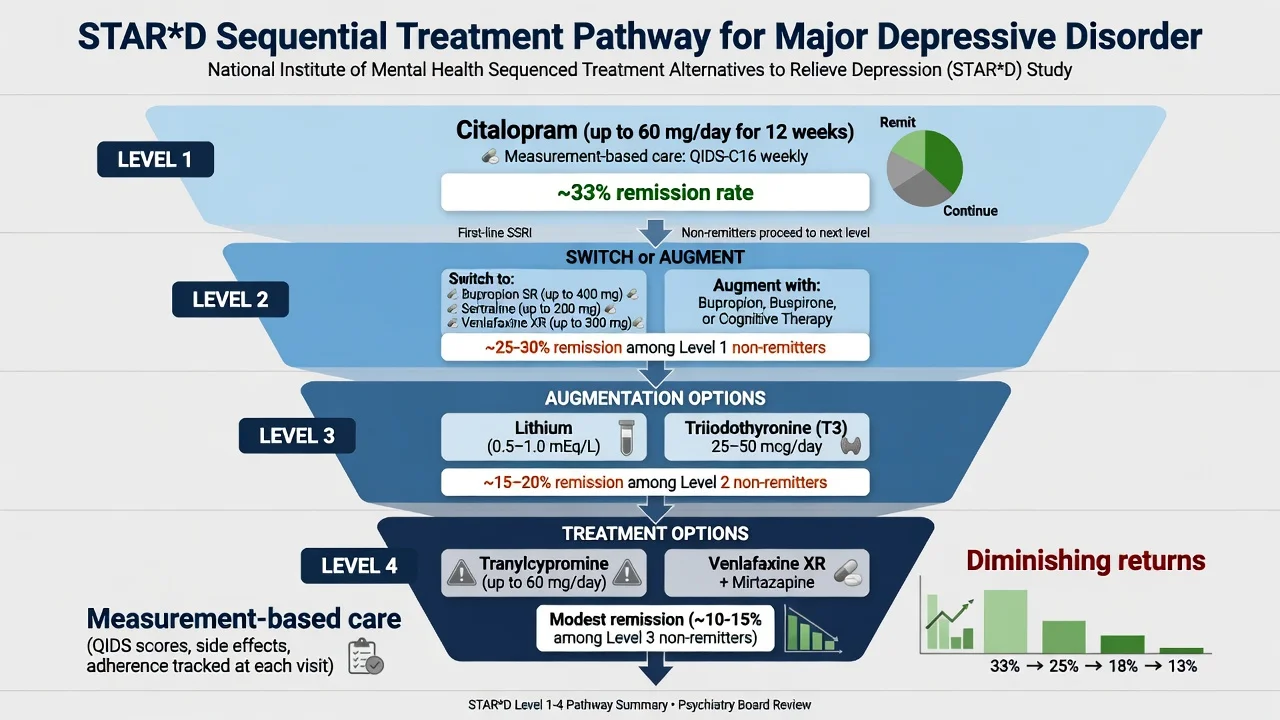
STAR*D was a large, multi-step effectiveness programme in outpatients with non-psychotic MDD using measurement-based care.[1][2]
- Level 1 — citalopram: roughly one-third remitted under systematic dose adjustment and measurement.[2]
- Level 2 switch (bupropion-SR, sertraline, or venlafaxine-XR after SSRI failure): similar remission rates across switch options in the published comparison — choose by residual symptoms and tolerability, not a mythical single best switch agent.[3]
- Level 3 augmentation included lithium versus T3 after two failed medication treatments — both are legitimate next steps with different monitoring burdens.[4]
- Level 4 compared tranylcypromine versus venlafaxine plus mirtazapine after three failed trials — modest remission, substantial intolerance risk on the MAOI path; specialist skill required.[5]
- Cumulative lesson: plan steps prospectively; re-check diagnosis at each failure; aim for remission; expect diminishing absolute gains.[1]
Switch versus augment
Prefer switch when there is zero response or intolerance to the current agent, when the side-effect profile drives change, or when class fit is wrong (e.g. need activating vs sedating). Prefer augment when there is partial response with residual symptoms, when the patient prefers not to lose hard-won gains, and when an evidence-based augmenter is available with feasible monitoring. Confirm diagnosis, adherence, dose, substances, and therapy engagement before either move.[3][16][17]
VAST-D randomised veterans unresponsive to an antidepressant to switch to bupropion, augment with bupropion, or augment with aripiprazole — a modern real-world comparison of switch vs augment strategies examiners may reference alongside STAR*D.[16]
Augmentation — lithium, T3, atypical antipsychotics
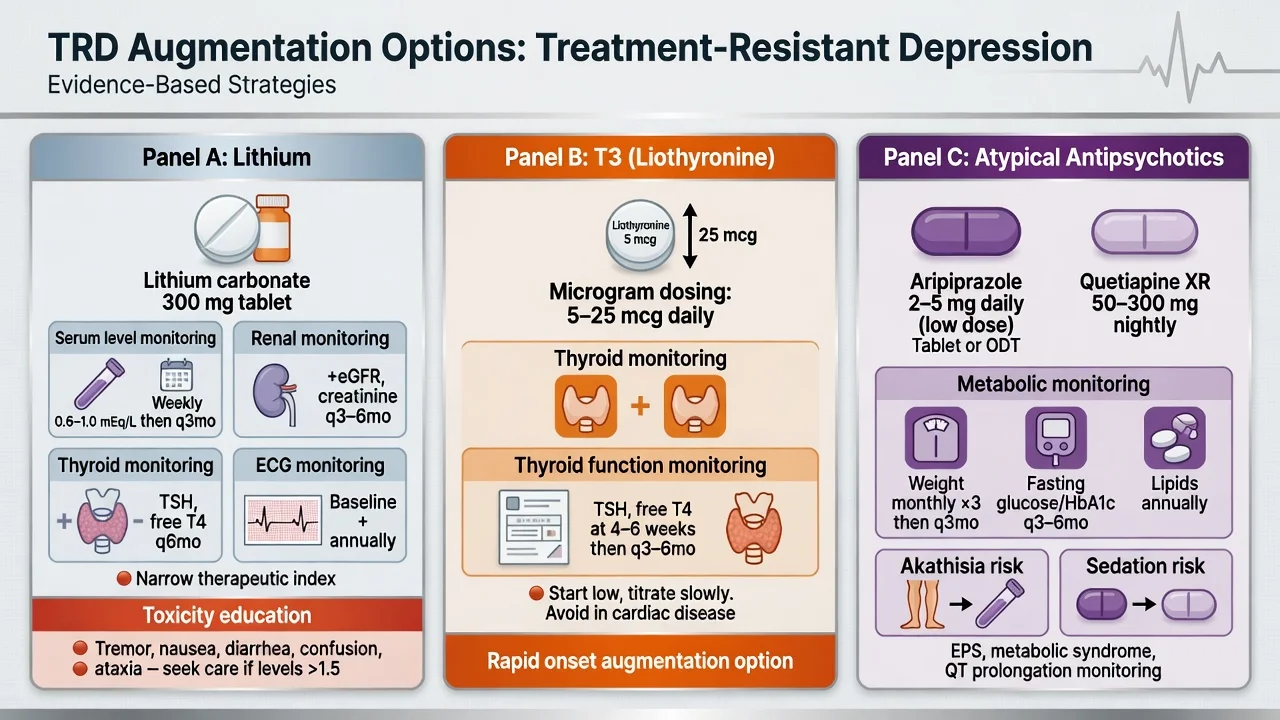
Lithium augmentation. Meta-analytic evidence supports lithium to accelerate and augment antidepressants in depressive disorders.[15] STAR*D included lithium versus T3 after two failed medication steps.[4] Exam-level adult practice points: start low (often 250–450 mg elemental lithium carbonate equivalent orally daily depending on formulation and age), titrate to a maintenance serum level typically around 0.4–0.8 mmol/L for augmentation contexts (individualise; older adults lower), check levels after dose changes and with intercurrent illness, monitor renal function, electrolytes, thyroid, educate on toxicity and dehydration, and discuss teratogenicity when relevant. Exact starting formulations and targets follow local product information and guideline context.[15][17][19]
T3 (liothyronine) augmentation. STAR*D compared T3 with lithium after two failed treatments.[4] Typical exam framing: low microgram dosing (often start 25 micrograms orally daily, adjust cautiously), monitor for thyrotoxic symptoms, resting tachycardia, and thyroid function — specialist or experienced use preferred if endocrine comorbidity exists.[4][17]
Atypical antipsychotic augmentation. Meta-analysis of placebo-controlled trials supports adjunctive atypical antipsychotics for MDD non-response, with trade-offs in adverse effects.[14] Common exam agents: aripiprazole start 2–5 mg orally daily (often 5–15 mg target range) with akathisia/activation monitoring and relatively lower metabolic risk than some peers; quetiapine XR often 50 mg at night building toward 150–300 mg, watching sedation, metabolic syndrome and orthostasis; olanzapine–fluoxetine in selected regional protocols with high metabolic risk, sometimes useful in psychotic depression contexts. Always monitor weight, glucose, lipids, EPS/akathisia, sedation, and QTc risk context. Discuss metabolic harm honestly — efficacy is not free.[14][17]
Combination antidepressants and MAOI pathway
Venlafaxine plus mirtazapine was a STAR*D level-4 option after multiple failures — use with attention to blood pressure, sedation, and serotonergic load.[5] Classical MAOIs (e.g. tranylcypromine) require dietary tyramine education, washout rules from prior serotonergic agents, and specialist familiarity; they remain examinable for atypical/anergic TRD phenotypes historically responsive to MAOIs, not first-line community care.[5]
Psychotherapy in TRD
CBT, behavioural activation, IPT, and related bona fide therapies remain core, not optional decoration after the third drug. Residual cognitive and interpersonal maintaining factors often explain incomplete pharmacological remission. Mindfulness-based cognitive therapy is particularly discussed for relapse prevention in recurrent depression. Combine therapy with medication when severity, chronicity, or preference supports it.[19]
ECT
ECT has the strongest short-term efficacy signal among somatic treatments for severe depressive disorders in systematic review.[11] Indications in the TRD pathway: severe melancholic or psychotic depression; catatonia; urgent high suicide risk; dangerous poor intake; prior excellent ECT response; pregnancy with severe depression when risks favour ECT; and true pharmacotherapy resistance after adequate trials. Work-up: informed consent (benefits, cognitive risks, anaesthetic/cardiac risks), medical review, labs/ECG as indicated, medication review (lithium, anticonvulsants, benzodiazepines), cognitive baseline. Electrode placement (right unilateral vs bitemporal) balances efficacy and cognitive adverse effects. Continuation/maintenance ECT is discussed after late remission in highly recurrent illness.[11][18][19]
rTMS
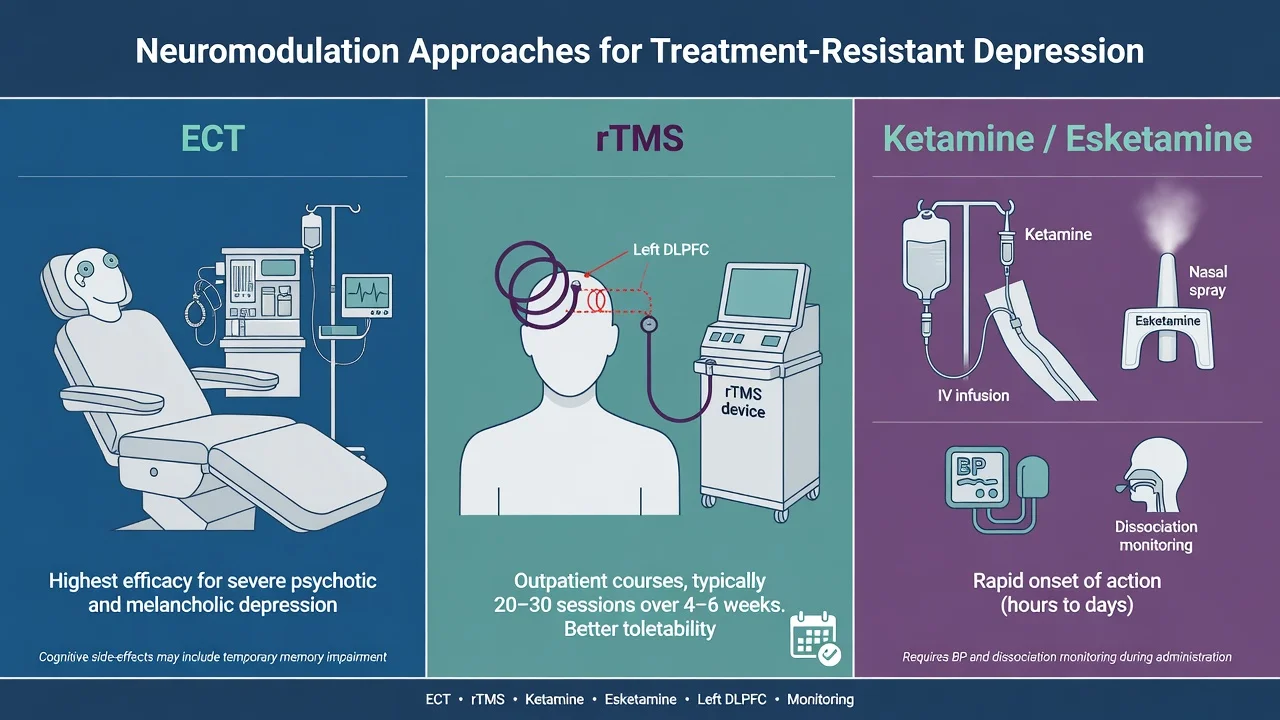
High-frequency rTMS to left DLPFC has sham-controlled evidence for acute antidepressant effects, including a landmark multisite trial and subsequent meta-analytic support for response/remission rates over sham.[12][13] CANMAT ranks neurostimulation options by line of treatment and evidence quality for clinicians sequencing care.[18] Exam framing: outpatient courses, better cognitive tolerability than ECT, lower absolute efficacy ceiling in the most severe psychotic/melancholic presentations where ECT remains preferred. Contraindications include non-removable ferromagnetic hardware in the head and uncontrolled seizure disorders (screen carefully).[12][18]
Ketamine and esketamine
Zarate and colleagues showed rapid antidepressant effects of subanaesthetic ketamine versus placebo in treatment-resistant major depression.[7] Murrough and colleagues confirmed efficacy in a two-site RCT of IV ketamine versus an active psychoactive control in TRD.[8] Intranasal esketamine combined with a newly initiated oral antidepressant improved outcomes in TRD, and continuation of esketamine plus oral antidepressant reduced relapse among responders in a randomised withdrawal design.[9][10]
Practice points for exams. Specialist setting; blood pressure and dissociation monitoring during and after dosing; not a take-home unmonitored oral antidepressant; access and funding vary by region; misuse and bladder/cognitive long-term concerns are part of informed consent for repeated ketamine exposure; combine with ongoing oral antidepressant and psychosocial care rather than using as monotherapy folklore.[8][9][10][18]
Regional guideline deltas
RANZCP mood disorder guidelines emphasise formulation-driven care, bipolar exclusion, staged pharmacological and psychological treatment, and appropriate use of ECT and other physical treatments within Australian and New Zealand service models.[19]
Specific subtypes and scenarios
Psychotic depression. Antidepressant plus antipsychotic, or ECT as a primary option when severity or speed requires it — do not leave on SSRI monotherapy.[11][19]
Anxious distress. May prefer agents/augmentation strategies addressing anxiety residual symptoms; still re-check for bipolar mixed features and substance use.[17][19]
Comorbid substance use. Dual formulation; TRD labels are unstable while heavy alcohol continues.[6][19]
Failed atypical antipsychotic augmentation. Reassess metabolic harm, consider lithium if not tried, ECT/rTMS/esketamine pathway, and psychotherapy intensity — avoid stacking three antipsychotics without formulation.[14][18]
Complications and pitfalls
Classic errors: declaring TRD after 10 days of half-dose sertraline; adding quetiapine for sleep without a depression plan; MAOI without washout education; framing ECT as punishment or pure last resort; starting esketamine without monitoring infrastructure.[5][11][19]
Prognosis and disposition
STAR*D shows that each failed step lowers the probability of subsequent remission, but some patients still remitted late — so nihilism is not evidence-based.[1] Residual symptoms predict relapse; maintenance of the effective regimen (pharmacological and psychological) is part of treatment, not optional aftercare. Disposition ladder: primary care collaborative care → CMHT / mood clinic → intensive community → day programmes → voluntary inpatient → involuntary inpatient when risk and capacity thresholds are met under local law → ECT suite / neuromodulation service.[1][19]
Special populations
Older adults
- Medical comorbidity and polypharmacy
- Hyponatraemia, falls, QTc, renal risk with lithium
- Start low, go slow on drugs
- ECT often highly effective in severe late-life depression
Pregnancy
- Untreated severe TRD is not zero-harm
- Risk–benefit of each agent individualised
- ECT may be preferred in severe high-risk illness
- Specialist perinatal liaison
Adolescents
- Fewer TRD trial data for many options
- Family involvement mandatory ideal
- SSRI + therapy principles first
- Specialist CAMHS pathway
Cultural safety
- Explanatory models and stigma
- Interpreter and family decision styles
- FRANZCP cultural safety expectations
- Do not pathologise culturally normative distress
Population-specific monitoring changes first-line next steps — state them explicitly at viva.[11][19]
Evidence, guidelines and controversies
Landmark pillars: STAR*D sequential remission and measurement-based care;[1][2] Level 2 switch equivalence lesson;[3] lithium vs T3 and level 4 MAOI/combo reports;[4][5] definition synthesis (Gaynes);[6] Zarate and Murrough ketamine;[7][8] Popova and Daly esketamine;[9][10] UK ECT Review Group;[11] O'Reardon rTMS and Berlim meta-analysis;[12][13] Nelson atypical AP meta-analysis;[14] Crossley lithium meta-analysis;[15] VAST-D;[16] CANMAT pharm and neurostimulation;[17][18] RANZCP 2020 mood guidelines.[19]
Controversies to handle calmly: heterogeneity of TRD definitions across trials; effect size of atypical antipsychotic augmentation versus metabolic harm; early use of ketamine/esketamine versus traditional lithium augmentation; STAR*D design limits (not a pure multi-arm RCT at every node); and access equity for neuromodulation.[6][14][16]
Exam pearls
RESIST
RESIST is a memory scaffold for the TRD reassessment sequence — still apply full formulation and risk assessment.[1][6][19]
References
- [1]Rush AJ, Trivedi MH, Wisniewski SR, Nierenberg AA, Stewart JW, Warden D, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report Am J Psychiatry, 2006.PMID 17074942
- [2]Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice Am J Psychiatry, 2006.PMID 16390886
- [3]Rush AJ, Trivedi MH, Wisniewski SR, Stewart JW, Nierenberg AA, Thase ME, et al. Bupropion-SR, sertraline, or venlafaxine-XR after failure of SSRIs for depression N Engl J Med, 2006.PMID 16554525
- [4]Nierenberg AA, Fava M, Trivedi MH, Wisniewski SR, Thase ME, McGrath PJ, et al. A comparison of lithium and T(3) augmentation following two failed medication treatments for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946176
- [5]McGrath PJ, Stewart JW, Fava M, Trivedi MH, Wisniewski SR, Nierenberg AA, et al. Tranylcypromine versus venlafaxine plus mirtazapine following three failed antidepressant medication trials for depression: a STAR*D report Am J Psychiatry, 2006.PMID 16946177
- [6]Gaynes BN, Lux L, Gartlehner G, Asher G, Forman-Hoffman V, Green J, et al. Defining treatment-resistant depression Depress Anxiety, 2020.PMID 31638723
- [7]Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression Arch Gen Psychiatry, 2006.PMID 16894061
- [8]Murrough JW, Iosifescu DV, Chang LC, Al Jurdi RK, Green CE, Perez AM, et al. Antidepressant efficacy of ketamine in treatment-resistant major depression: a two-site randomized controlled trial Am J Psychiatry, 2013.PMID 23982301
- [9]Popova V, Daly EJ, Trivedi M, Cooper K, Lane R, Lim P, et al. Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study Am J Psychiatry, 2019.PMID 31109201
- [10]Daly EJ, Trivedi MH, Janik A, Li H, Zhang Y, Li X, et al. Efficacy of Esketamine Nasal Spray Plus Oral Antidepressant Treatment for Relapse Prevention in Patients With Treatment-Resistant Depression: A Randomized Clinical Trial JAMA Psychiatry, 2019.PMID 31166571
- [11]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [12]O'Reardon JP, Solvason HB, Janicak PG, Sampson S, Isenberg KE, Nahas Z, et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial Biol Psychiatry, 2007.PMID 17573044
- [13]Berlim MT, van den Eynde F, Tovar-Perdomo S, Daskalakis ZJ Response, remission and drop-out rates following high-frequency repetitive transcranial magnetic stimulation (rTMS) for treating major depression: a systematic review and meta-analysis of randomized, double-blind and sham-controlled trials Psychol Med, 2014.PMID 23507264
- [14]Nelson JC, Papakostas GI Atypical antipsychotic augmentation in major depressive disorder: a meta-analysis of placebo-controlled randomized trials Am J Psychiatry, 2009.PMID 19687129
- [15]Crossley NA, Bauer M Acceleration and augmentation of antidepressants with lithium for depressive disorders: two meta-analyses of randomized, placebo-controlled trials J Clin Psychiatry, 2007.PMID 17592920
- [16]Mohamed S, Johnson GR, Chen P, Hicks PB, Davis LL, Yoon J, et al. Effect of Antidepressant Switching vs Augmentation on Remission Among Patients With Major Depressive Disorder Unresponsive to Antidepressant Treatment: The VAST-D Randomized Clinical Trial JAMA, 2017.PMID 28697253
- [17]Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 3. Pharmacological Treatments Can J Psychiatry, 2016.PMID 27486148
- [18]Milev RV, Giacobbe P, Kennedy SH, Blumberger DM, Daskalakis ZJ, Downar J, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder: Section 4. Neurostimulation Treatments Can J Psychiatry, 2016.PMID 27486154
- [19]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [20]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941