Psych · General adult psychiatry — psychosis
Treatment-resistant schizophrenia
Also known as TRS · Treatment refractory schizophrenia · Clozapine-eligible schizophrenia · Ultra-treatment-resistant schizophrenia · TRRIP treatment resistance · Clozapine-resistant schizophrenia
Exam-exhaustive fellowship reference on treatment-resistant schizophrenia — TRRIP criteria, pseudo-resistance, LAI before labelling, clozapine pathway core, ultra-treatment resistance, ECT augmentation, psychosocial care, and regional guideline deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Treatment-resistant schizophrenia (TRS) is a high-stakes fellowship topic because examiners test whether you can stop cycling non-clozapine polypharmacy, define an adequate trial, prove adherence (including LAI), consent to clozapine monitoring, and escalate ultra-resistance without folklore. The dedicated clozapine topic deepens monitoring minutiae; this topic remains self-sufficient for TRRIP logic, clozapine core pathway, and post-clozapine options.[1][10][12]
Overview and definition
TRS is a treatment-outcome construct layered on a schizophrenia-spectrum diagnosis, not a freestanding DSM-5-TR or ICD-11 code. The modern operational language is TRRIP (Treatment Response and Resistance in Psychosis): confirmed diagnosis, clinically significant ongoing symptoms, inadequate response to at least two different antipsychotics given at an adequate dose and duration with adherence assessed, after pseudo-resistance is excluded.[1][12]
Outcomes language. Response commonly means clinically meaningful reduction in target symptoms (often framed as about 20% or greater improvement on a total scale in research, with functional context); non-response is failure to meet the agreed threshold after an adequate trial; remission is more stringent near-absence of active positive symptoms with functional recovery; partial response is real improvement that is not enough. Response without function is not success.[1][12]
Adequate trial (exam mantra). Right diagnosis, right drug, therapeutic dose for typically around 6 weeks at that dose (document local practice), verified adherence (history, collateral, plasma level, or LAI), addressed substances and medical confounders, and measured outcome — before declaring failure.[1][12]
Classification and staging
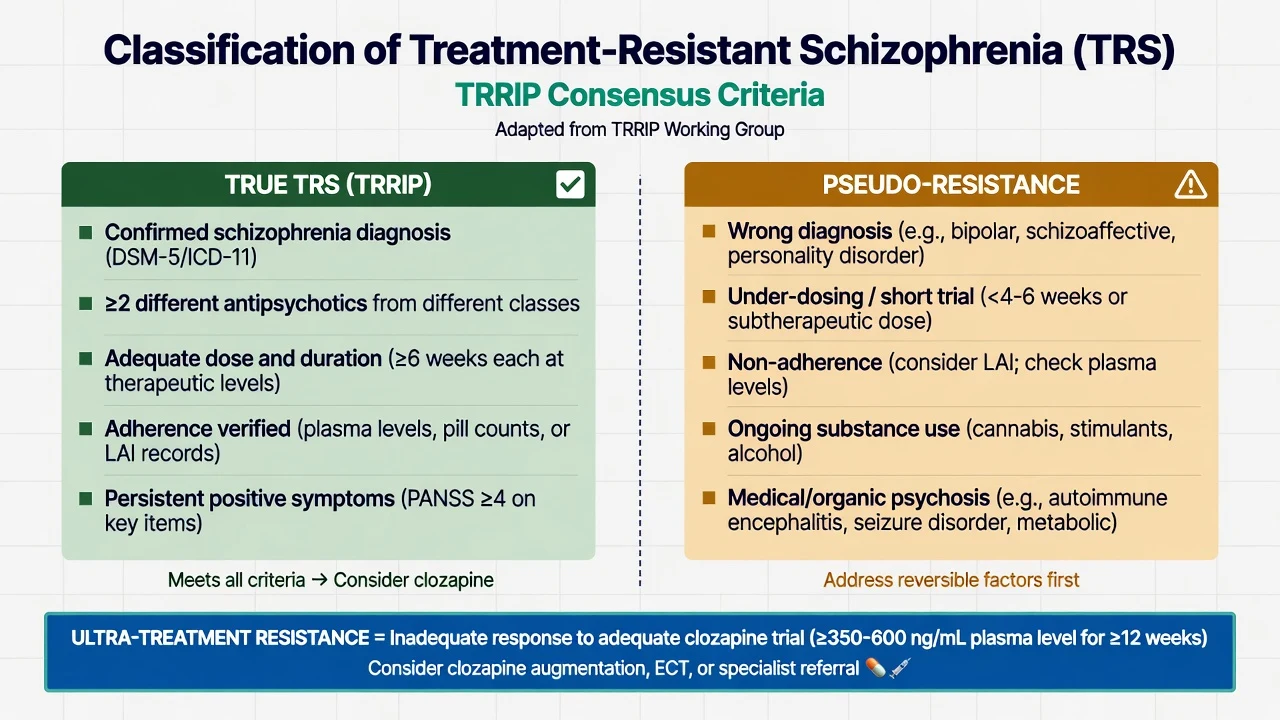
True TRS (TRRIP)
- Confirmed schizophrenia-spectrum diagnosis
- ≥2 different antipsychotics failed
- Adequate dose and duration each trial
- Adherence verified; symptoms persist
Pseudo-resistance
- Misdiagnosis (bipolar, organic, substance)
- Subtherapeutic dose or too-short trial
- Covert non-adherence — consider LAI/levels
- Untreated medical contributors
Ultra-treatment resistance
- Inadequate response after adequate clozapine
- Check plasma level and duration first
- Then augmentation / ECT pathways
- Not a synonym for 'difficult personality'
Related labels
- Treatment-intolerant (stopped for adverse effects)
- Partial responders with residual positives
- Primary early vs secondary later resistance
- Clozapine-intolerant (cannot take clozapine)
Kane and colleagues' clinical guidance summarises identification and management of TRS for everyday practice; use TRRIP language for research-grade clarity and viva precision.[1][12]
Epidemiology and risk factors
Numbers examiners expect
A clinically important minority of people with schizophrenia meet treatment-resistance criteria. FEP-linked work describes both early (primary) resistance and later (secondary) resistance patterns, with predictors including male sex, earlier onset, poorer premorbid function, longer untreated psychosis, substance use, and multi-domain symptom burden.[14][15] Meta-analytic work on clozapine response rates shows meaningful benefit when clozapine is used properly in TRS populations — delay is a system failure, not cautious excellence.[6][7]
TRS drives excess disability, service use, and suicide risk when untreated or under-treated; physical morbidity from polypharmacy and cardiometabolic disease is part of the burden you must name.[8][10]
Pathophysiology and mechanisms
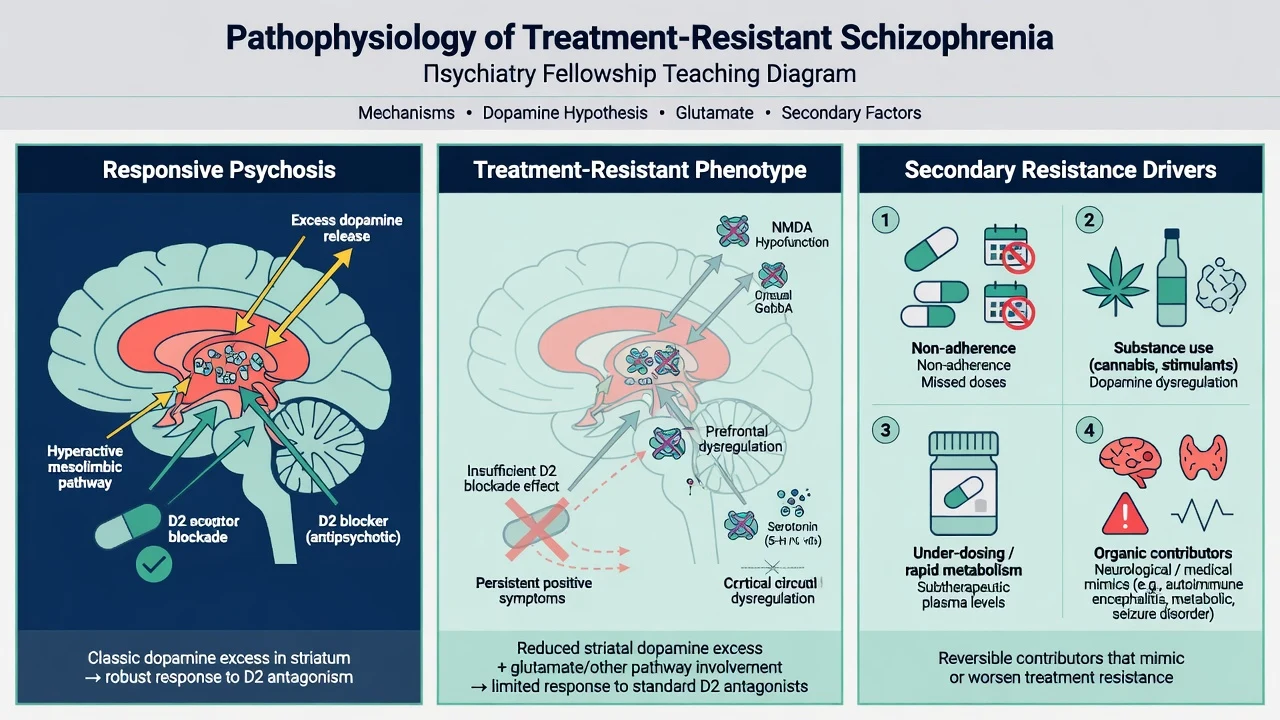
Dopamine hypothesis version III. Multiple upstream hits can converge on striatal dopamine dysregulation as a final common pathway for positive symptoms and D2-blocker response. That model explains why most antipsychotics work for many patients — and why pure D2 blockade fails when the biology is not primarily hyperdopaminergic or when secondary drivers dominate.[18]
Treatment-resistant phenotype (conceptual). Research frameworks contrast antipsychotic-responsive psychosis (more classic striatal dopamine excess) with non-responsive illness that may involve greater glutamate and other circuit contributions. Exam use: justify clozapine's multi-receptor profile and why stacking another standard D2 antagonist after two adequate failures is weak logic.[1][18]
Secondary resistance drivers. Non-adherence, substances (especially high-potency cannabis and stimulants), under-dosing, rapid metabolism without level-guided adjustment, and organic mimics produce pseudo-resistance that looks like TRS until you re-check the basics.[1][12]
Psychosocial maintenance. High expressed emotion, isolation, trauma, cognitive deficits, and lack of structured rehabilitation sustain functional non-recovery even when positive symptoms partially improve — pharmacology alone is incomplete care.[19]
Clinical presentation
Patients referred as "TRS" may show persistent delusions and hallucinations despite multiple scripts; revolving-door admissions with "failed" orals that were never absorbed; multi-domain non-recovery (negative symptoms, cognitive impairment, depression, unemployment); high suicide risk with demoralisation; or forensic risk when paranoia and command hallucinations remain active.[10][12]
High-acuity TRS phenotypes. Command hallucinations with compliance risk, severe paranoia driving planned violence, catatonia, and dangerous self-neglect change the setting and legal pathway immediately — risk management and senior review first.[10][11]
Clozapine non-response presentation. Persistent positive symptoms after an adequate clozapine trial (dose, duration, plasma level, adherence) define the ultra-resistant pathway — not three weeks at 100 mg with missed bloods.[16][17]
Differential diagnosis — and the pseudo-resistance checklist
Bipolar / schizoaffective
- Mood episode primacy and cyclicity
- Family history of bipolarity
- Antidepressant-induced mania history
- Do not call pure TRS without mood formulation
Substance / medication
- Cannabis, methamphetamine, alcohol
- Steroids, stimulants, anticholinergics
- Timeline locked to exposure
- Treat dual formulation in parallel
Medical / organic
- Autoimmune encephalitis red flags
- Seizure-related psychosis, endocrine
- Delirium with fluctuation
- Late first onset or focal signs → investigate
Other psychiatric
- OCD with poor insight
- PTSD with dissociative phenomena
- Delusional disorder boundaries
- Personality-driven mistrust without true psychosis
Discriminators must be stated explicitly — lists without discriminators fail fellowship exams.[1][10]
Clinical and bedside assessment
Structure the TRS reassessment interview: (1) confirm schizophrenia-spectrum diagnosis and current symptom domains (MSE language for positives, negatives, disorganisation, cognition, mood); (2) reconstruct treatment history (agent, dose, duration at therapeutic dose, adherence method, side-effects, response/partial/none, reason stopped, prior LAI, prior plasma levels); (3) substances, trauma, medical/medication list, smoking status; (4) suicide, violence, vulnerability, self-neglect risk with means, intent, plan, protective factors; (5) capacity and least-restrictive legal pathway if risk is high (jurisdiction-specific statutes — do not invent section numbers); (6) collateral and prior records; (7) clozapine readiness (monitoring access, constipation history, cardiac risk, pregnancy when relevant).[1][10][12]
Measurement. Serial CGI and a structured symptom scale (PANSS/BPRS conceptually in research settings) plus functional review. Document adherence method every time you declare a trial failed.[1][12]
Investigations
Typical adult set before next-step antipsychotics or clozapine: FBC with absolute neutrophil count; U&E; LFT; glucose/HbA1c and lipids; BMI/waist; ECG; pregnancy test when relevant; urine drug screen when substance contribution is plausible; consider plasma antipsychotic level for adherence/pseudo-resistance; smoking status documentation (CYP1A2 induction for clozapine interpretation). Neuroimaging, EEG, or autoimmune panels when red flags (late first onset, focal neurology, seizure, rapid cognitive decline) — not automatic for classic multi-episode TRS without new red flags.[10][11][12]
Management — acute risk and resuscitation
Manage acute agitation with least-restrictive de-escalation and local rapid tranquillisation protocols (see dedicated RT topic). Medical emergencies during multi-drug pathways include NMS, severe EPS/akathisia mislabelled as agitation, clozapine myocarditis, agranulocytosis sepsis, and ileus.[10][11]
Legal status follows capacity, risk, and local Mental Health Act principles — name that statutes are jurisdiction-specific and do not invent section numbers in multi-region answers.[10]
Management — definitive and stepwise
Step 0 — Stop calling it TRS until the checklist is clean
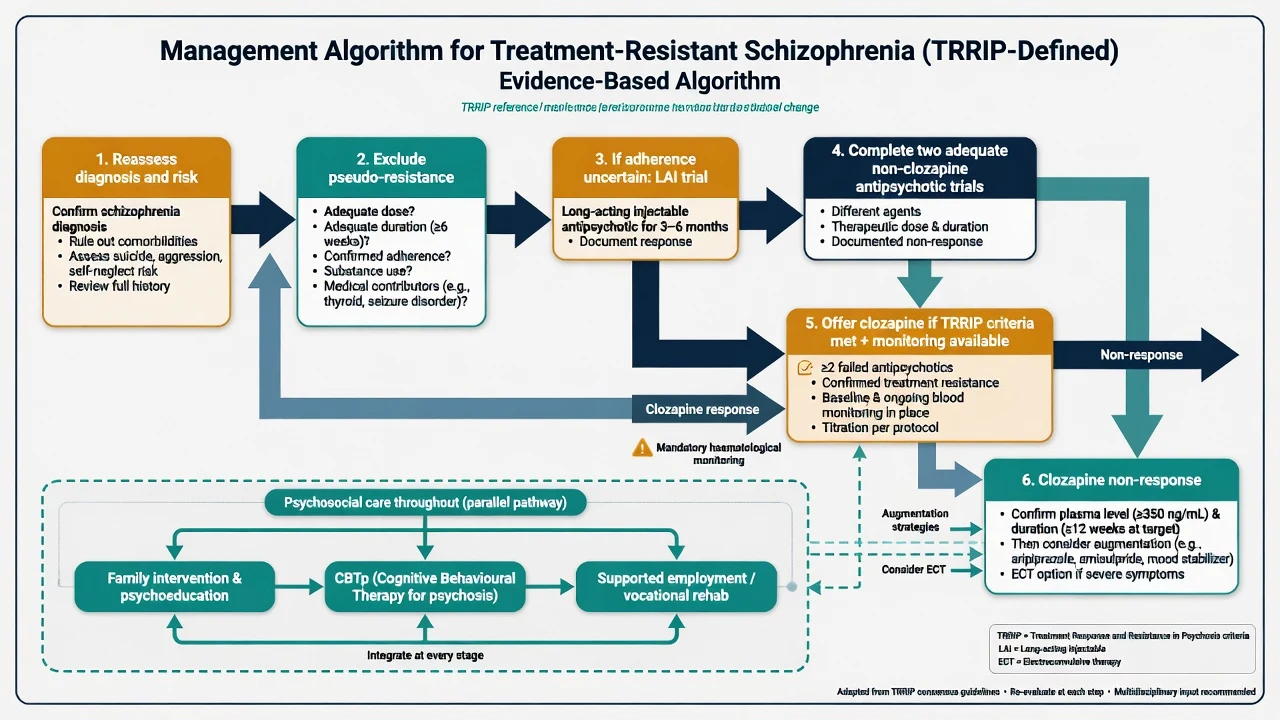
Optimise the current agent if the trial was never adequate. Fix adherence barriers. Treat substances. Correct medical confounders. Re-open bipolar and organic differentials.[1][12]
LAI before the TRS stamp
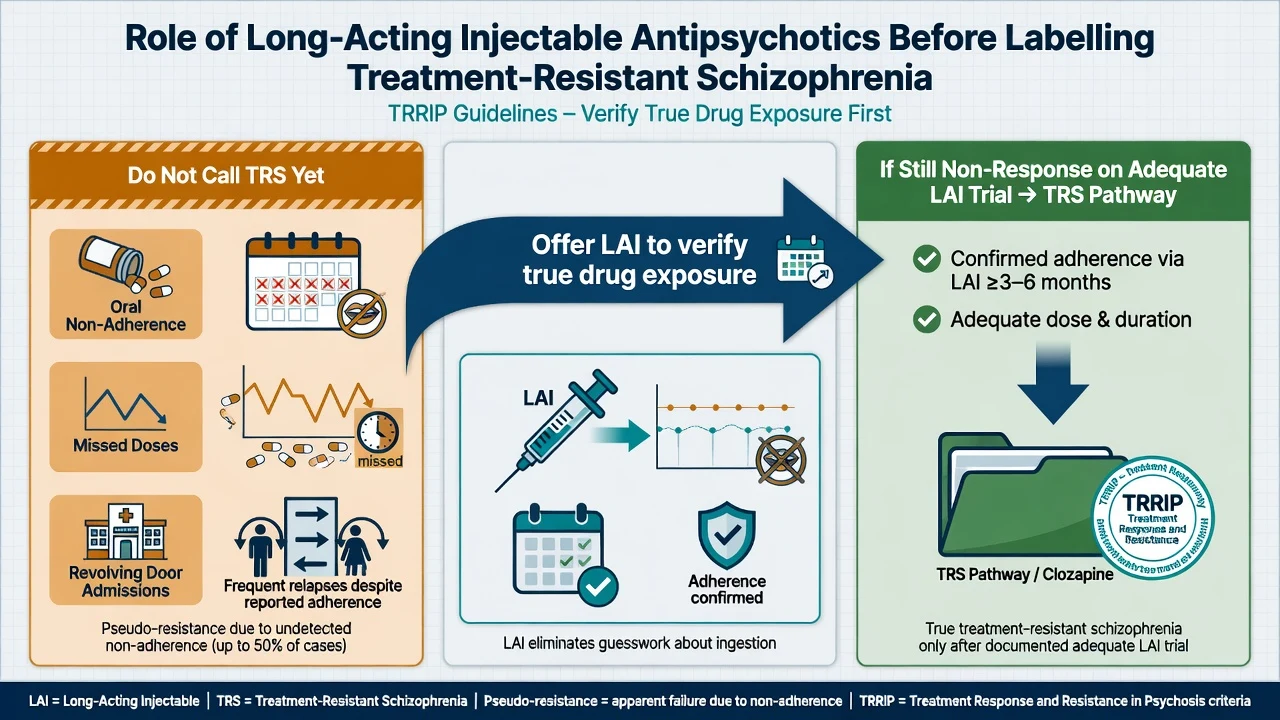
Covert non-adherence is a classic generator of pseudo-resistance. Long-acting injectables reduce covert non-ingestion and have meta-analytic support for relapse prevention versus oral formulations in randomised comparisons (effect sizes vary by design; real-world signals are often stronger).[20] Offer LAI when adherence-related relapse is likely, when the patient prefers fewer daily decisions, and before permanently labelling TRS if exposure was never proved. LAI is not a substitute for clozapine once true TRS is established.[10][12][20]
Two adequate non-clozapine trials
Use two different antipsychotics at therapeutic dose for adequate duration with adherence verified. Algorithmic FEP work shows that sequential prospective trials clarify true non-response rates and support earlier clozapine consideration when criteria are met.[13] Prefer agents the patient has not truly failed; avoid token doses and three-day "trials." CATIE reminds that effectiveness includes tolerability and continuation, not only acute scale change.[4]
Offer clozapine when TRRIP is met
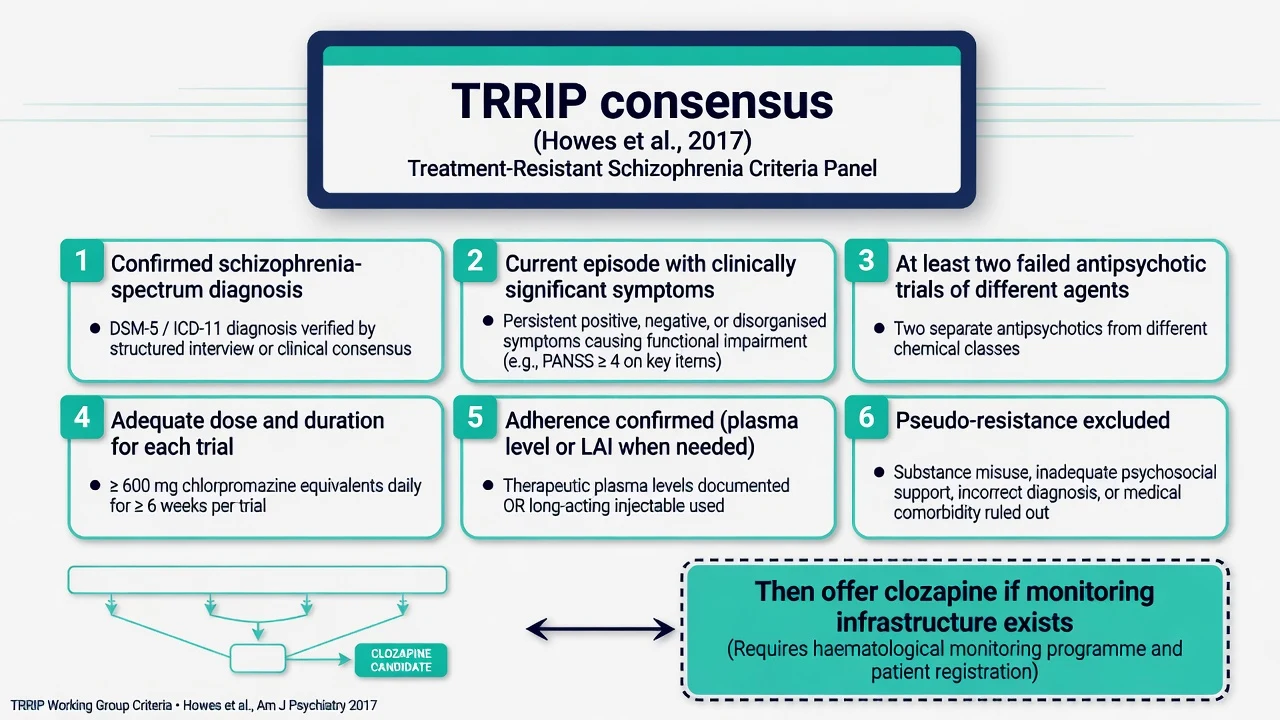
Kane 1988 established clozapine superiority in rigorously defined treatment-resistant schizophrenia versus chlorpromazine. CATIE phase 2 (effectiveness of clozapine versus other atypicals after prior atypical non-response) and modern meta-analyses support clozapine as the evidence-based agent once true TRS is defined.[2][3][5][6] Network meta-analysis of antipsychotics in TRS populations continues to place clozapine as the preferred specialised option; Siskind response-rate data support meaningful response proportions when clozapine is used properly.[5][6][7]
InterSePT showed clozapine superior to olanzapine for suicidal behaviour in schizophrenia and schizoaffective disorder — examiners expect you to name this even when the presentation is high suicide risk rather than classic multi-trial TRS alone.[8]
Clozapine pathway core (self-sufficient; pointer for depth)
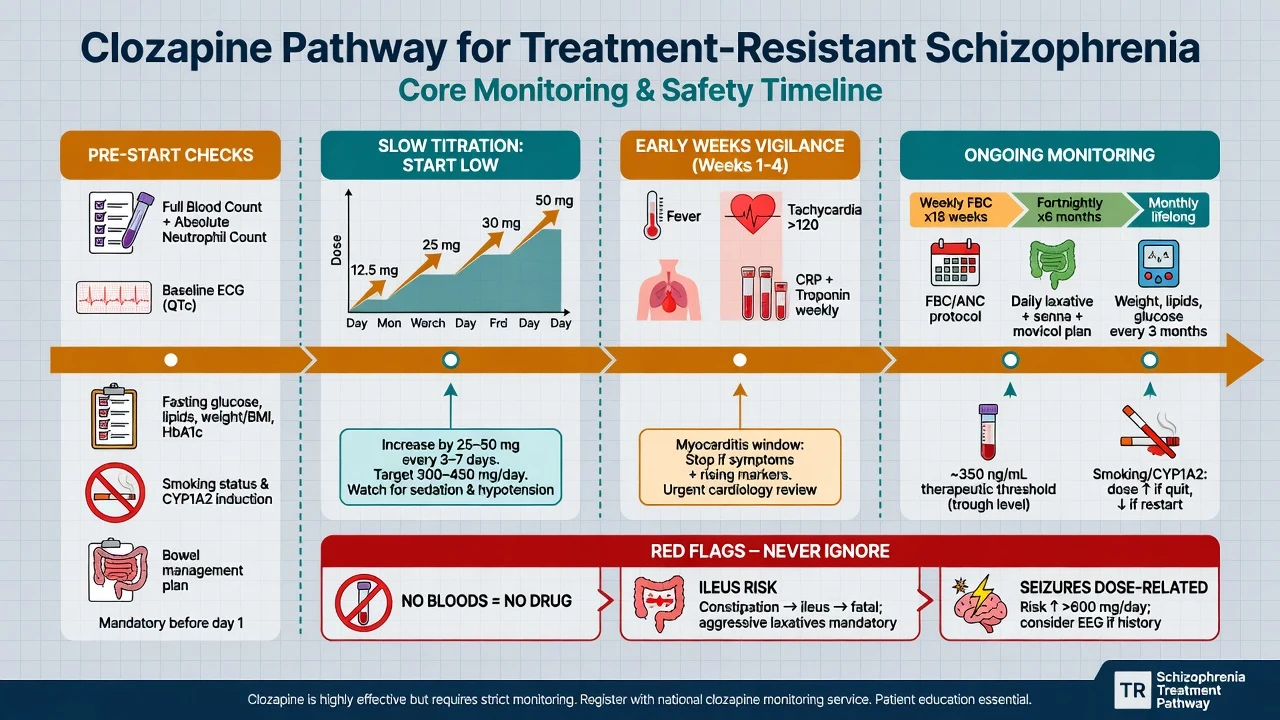
Pre-start. Confirm TRRIP-eligible indication; capacity/consent or legal framework; baseline FBC with ANC; metabolic panel; ECG; CRP ± troponin as per local myocarditis protocol; bowel history and prophylactic laxative plan; smoking status; drug interactions (classically fluvoxamine raises levels via CYP1A2); pregnancy status when relevant; and service readiness for protocol bloods.[10][11][12]
Titration (exam outline — confirm local product information). Start low (commonly 12.5 mg orally once or twice on day 1 in adult protocols, then titrate slowly by small increments every few days as tolerated). Target doses for many adults often fall in the 300–450 mg/day range, individualised; some need higher with level guidance. Watch orthostasis, sedation, tachycardia, and constipation from day one.[10][12]
Plasma level teaching threshold. Many services discuss a trough around 350 ng/mL (0.35 mg/L) as a concentration–response teaching point before declaring clozapine failure — individualise and use local units and laboratory methods. Smoking induces CYP1A2 and lowers levels; smoking cessation can raise levels and toxicity risk — dose-adjust proactively.[12]
Monitoring pillars. No recent valid bloods → no dispensing. Early weeks: myocarditis vigilance (fever, unexplained tachycardia, chest pain, rising CRP/troponin — stop and investigate). Lifelong: neutropenia protocol per local registry; metabolic monitoring; constipation prevention (ileus kills); seizure risk rises with dose/level. For full monitoring calendars, rechallenge rules, and interaction tables, see the dedicated clozapine topic — do not skip the non-negotiables here.[10][11][12]
Ultra-treatment resistance
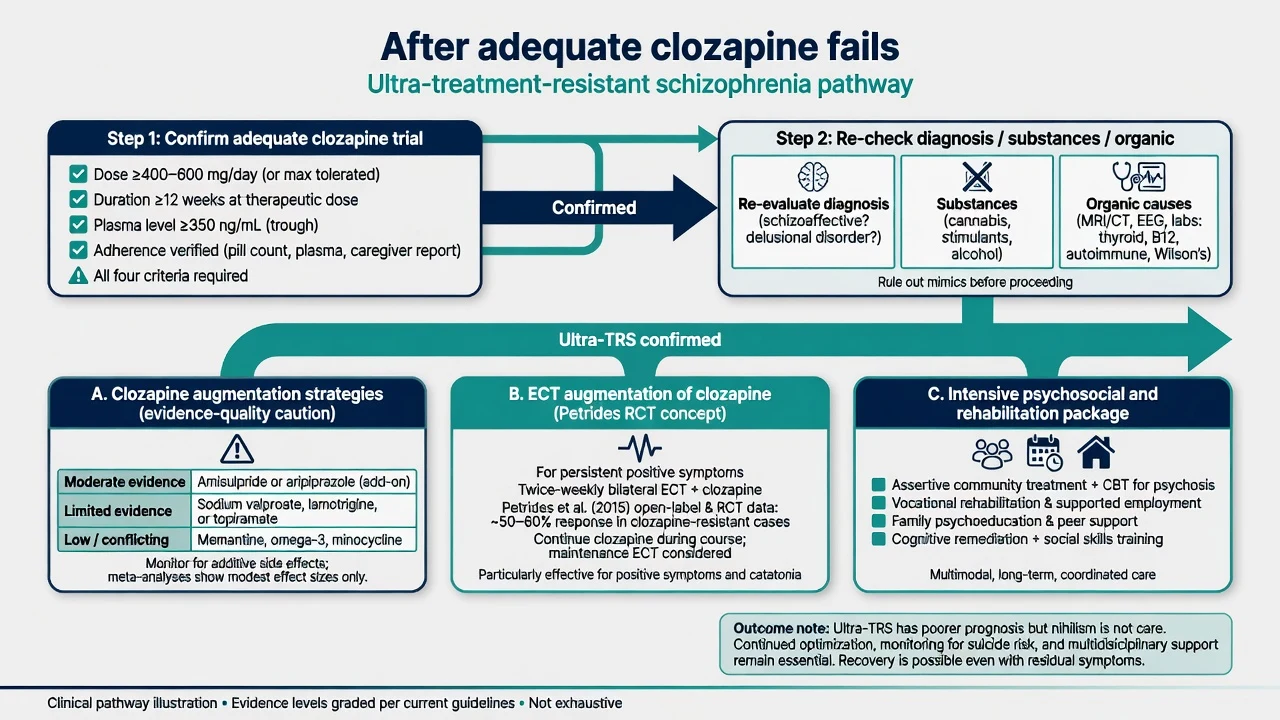
Ultra-treatment-resistant schizophrenia (also called clozapine-resistant schizophrenia in many papers) means inadequate response after an adequate clozapine trial. Definitions vary; Campana and colleagues synthesise characteristics and definition heterogeneity — exam gold is: confirm dose, duration (often around 3 months at therapeutic dose/level in clinical teaching), plasma level, and adherence before you escalate.[16][17]
Augmentation. Wagner meta-review of clozapine augmentation shows that evidence quality is mixed and often modest; name the agent, rationale, and additive adverse effects rather than stacking three antipsychotics by habit. Common examiner options include adding a second antipsychotic (e.g. amisulpride or aripiprazole in selected protocols) or other specialist strategies — always with metabolic, cardiac, and EPS monitoring and a stop rule if no benefit.[16]
ECT augmentation. Petrides and colleagues demonstrated benefit of ECT augmentation in clozapine-resistant schizophrenia in a prospective randomised study — discuss for persistent positive symptoms after true clozapine failure, with informed consent covering cognitive and anaesthetic risks.[9]
Psychosocial care (not optional decoration)
Family intervention and psychoeducation, cognitive behavioural therapy for psychosis (CBTp) for persistent symptoms, cognitive remediation, supported employment (Individual Placement and Support models), assertive community treatment/intensive case management, and housing support remain PORT-level essentials. Medication without psychosocial care is incomplete TRS management.[19][10]
Regional guideline deltas
RANZCP schizophrenia guidelines emphasise early intervention, physical health monitoring, psychosocial packages, and timely clozapine for treatment resistance within Australian and New Zealand service models. Mental Health Acts differ by jurisdiction — learn principles for your rostered state/territory or New Zealand setting; do not invent section numbers.[10]
Specific subtypes and scenarios
Primary early resistance. Non-response from early illness — move to clozapine once two adequate trials are truly complete; do not spend years "trying every SGA."[13][14]
Secondary later resistance. Later loss of response — re-check adherence, substances, medical illness, and supersensitivity/polypharmacy issues before adding a third non-clozapine agent.[14][15]
Clozapine-intolerant. Agranulocytosis history, myocarditis, or other absolute barriers — specialist path with careful risk–benefit of rechallenge (see clozapine topic), ECT, and intensive psychosocial care; do not abandon the patient.[12][16]
Predominant negative/cognitive symptoms. Clozapine may help some domains but functional recovery needs cognitive remediation, rehabilitation, and medical exclusion of secondary negatives (EPS, depression, substances).[19]
Forensic / high-risk violence TRS. Secure setting may be required; still apply TRRIP and clozapine logic; risk formulation is continuous.[10]
Complications and pitfalls
Classic errors: declaring TRS after 10 days of half-dose olanzapine; three concurrent non-clozapine antipsychotics without a clozapine offer; starting clozapine on Friday without weekend bloods plan; stopping clozapine after partial response because "bloods are annoying."[10][12]
Prognosis and disposition
Clozapine produces meaningful response in a substantial proportion of TRS patients in meta-analytic summaries — still the best evidence agent, not a guarantee of full recovery.[6][7] Ultra-TRS has poorer symptomatic prognosis; functional recovery may lag symptom change and still deserves rehabilitation investment.[17] Disposition ladder: CMHT / clozapine clinic → intensive community → voluntary inpatient → involuntary inpatient under local law when risk and capacity thresholds are met → forensic pathways when required → rehabilitation and supported accommodation. After response, do not stop clozapine casually — relapse risk is high.[10][12]
Special populations
Youth / EIS
- Algorithmic trials then timely clozapine
- Family engagement mandatory ideal
- Substance use formulation
- Specialist early psychosis pathway
Older adults
- Medical comorbidity and polypharmacy
- Anticholinergic constipation and falls risk
- Slower titration and lower targets often
- Organic vigilance for late-onset psychosis
Pregnancy
- Untreated TRS is not zero-harm
- Specialist perinatal psychiatry
- Clozapine risk–benefit individualised
- ECT may be considered in selected severe cases
Cultural safety
- Explanatory models and stigma
- Interpreter and family decision styles
- FRANZCP cultural safety expectations
- Do not pathologise culturally normative distress
Population-specific monitoring changes first-line next steps — state them explicitly at viva.[10][11]
Evidence, guidelines and controversies
Landmark pillars: TRRIP 2017 terminology;[1] Kane 1988 clozapine superiority;[2] CATIE effectiveness context and CATIE phase 2 clozapine arm;[3][4] Samara network meta-analysis in TRS;[5] Siskind clozapine meta-analyses and response rates;[6][7] InterSePT suicide outcomes;[8] Petrides ECT augmentation;[9] RANZCP and APA 2020 guidelines;[10][11] Kane clinical guidance 2019;[12] Agid sequential algorithm;[13] Lally and Demjaha resistance patterns in FEP;[14][15] Wagner augmentation meta-review;[16] Campana ultra-TRS synthesis;[17] Howes–Kapur dopamine framework;[18] PORT psychosocial recommendations;[19] Kishimoto LAI meta-analysis.[20]
Controversies to handle calmly: how early to offer clozapine; whether a failed LAI is mandatory before TRS labelling when adherence is already proved by levels; modest effect sizes of many clozapine augmenters; access equity for clozapine clinics and ECT; and definition heterogeneity for ultra-TRS across trials.[12][16][17]
Exam pearls
RESIST
RESIST is a memory scaffold for the TRS reassessment sequence — still apply full formulation and risk assessment.[1][12][10]
References
- [1]Howes OD, McCutcheon R, Agid O, et al. Treatment-Resistant Schizophrenia: Treatment Response and Resistance in Psychosis (TRRIP) Working Group Consensus Guidelines on Diagnosis and Terminology Am J Psychiatry, 2017.PMID 27919182
- [2]Kane J, Honigfeld G, Singer J, et al. Clozapine for the treatment-resistant schizophrenic. A double-blind comparison with chlorpromazine. Arch Gen Psychiatry, 1988.PMID 3046553
- [3]McEvoy JP, Lieberman JA, Stroup TS, et al. Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior atypical antipsychotic treatment Am J Psychiatry, 2006.PMID 16585434
- [4]Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia N Engl J Med, 2005.PMID 16172203
- [5]Samara MT, Dold M, Gianatsi M, et al. Efficacy, Acceptability, and Tolerability of Antipsychotics in Treatment-Resistant Schizophrenia: A Network Meta-analysis JAMA Psychiatry, 2016.PMID 26842482
- [6]Siskind D, McCartney L, Goldschlager R, et al. Clozapine v. first- and second-generation antipsychotics in treatment-refractory schizophrenia: systematic review and meta-analysis Br J Psychiatry, 2016.PMID 27388573
- [7]Siskind D, Siskind V, Kisely S Clozapine Response Rates among People with Treatment-Resistant Schizophrenia: Data from a Systematic Review and Meta-Analysis Can J Psychiatry, 2017.PMID 28655284
- [8]Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT) Arch Gen Psychiatry, 2003.PMID 12511175
- [9]Petrides G, Malur C, Braga RJ, et al. Electroconvulsive therapy augmentation in clozapine-resistant schizophrenia: a prospective, randomized study Am J Psychiatry, 2015.PMID 25157964
- [10]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [11]Keepers GA, Fochtmann LJ, Anzia JM, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Am J Psychiatry, 2020.PMID 32867516
- [12]Kane JM, Agid O, Baldwin ML, et al. Clinical Guidance on the Identification and Management of Treatment-Resistant Schizophrenia J Clin Psychiatry, 2019.PMID 30840788
- [13]Agid O, Arenovich T, Sajeev G, et al. An algorithm-based approach to first-episode schizophrenia: response rates over 3 prospective antipsychotic trials with a retrospective data analysis J Clin Psychiatry, 2011.PMID 21457676
- [14]Lally J, Ajnakina O, Di Forti M, et al. Two distinct patterns of treatment resistance: clinical predictors of treatment resistance in first-episode schizophrenia spectrum psychoses Psychol Med, 2016.PMID 27605254
- [15]Demjaha A, Lappin JM, Stahl D, et al. Antipsychotic treatment resistance in first-episode psychosis: prevalence, subtypes and predictors Psychol Med, 2017.PMID 28395674
- [16]Wagner E, Löhrs L, Siskind D, et al. Clozapine augmentation strategies - a systematic meta-review of available evidence. Treatment options for clozapine resistance J Psychopharmacol, 2019.PMID 30696332
- [17]Campana M, Falkai P, Siskind D, et al. Characteristics and definitions of ultra-treatment-resistant schizophrenia - A systematic review and meta-analysis Schizophr Res, 2021.PMID 33454644
- [18]Howes OD, Kapur S The dopamine hypothesis of schizophrenia: version III--the final common pathway Schizophr Bull, 2009.PMID 19325164
- [19]Dixon LB, Dickerson F, Bellack AS, et al. The 2009 schizophrenia PORT psychosocial treatment recommendations and summary statements Schizophr Bull, 2010.PMID 19955389
- [20]Kishimoto T, Robenzadeh A, Leucht C, et al. Long-acting injectable vs oral antipsychotics for relapse prevention in schizophrenia: a meta-analysis of randomized trials Schizophr Bull, 2014.PMID 23256986