Psych · General adult psychiatry — OCRD / BFRB
Trichotillomania and excoriation disorder
Also known as Hair-pulling disorder · Skin-picking disorder · Pathologic skin picking · Dermatillomania · BFRB · Body-focused repetitive behaviour · Neurotic excoriation · OCRD
Exam-exhaustive fellowship reference on trichotillomania and excoriation (skin-picking) disorder — DSM-5-TR OCRD criteria; automatic vs focused styles; differentials vs alopecia areata and OCD/BDD; MGH-HPS/SPS; habit reversal training and ComB/ACT-enhanced BT; adult NAC RCTs (Grant 2009/2016) vs paediatric NAC null (Bloch); limited SSRI signal; clomipramine and olanzapine specialist options; trichobezoar and infection emergencies. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Trichotillomania (hair-pulling disorder) and excoriation (skin-picking) disorder are high-yield general adult OCRD topics at the FRANZCP, MRCPsych, and ABPN interface. Examiners test OCRD placement, automatic versus focused styles, dermatologic differentials, first-line habit reversal training, the adult N-acetylcysteine (NAC) evidence base, the paediatric NAC null trial, limited SSRI efficacy relative to behaviour therapy, and medical complications including infection and trichobezoar.[5][12]
Overview and definition
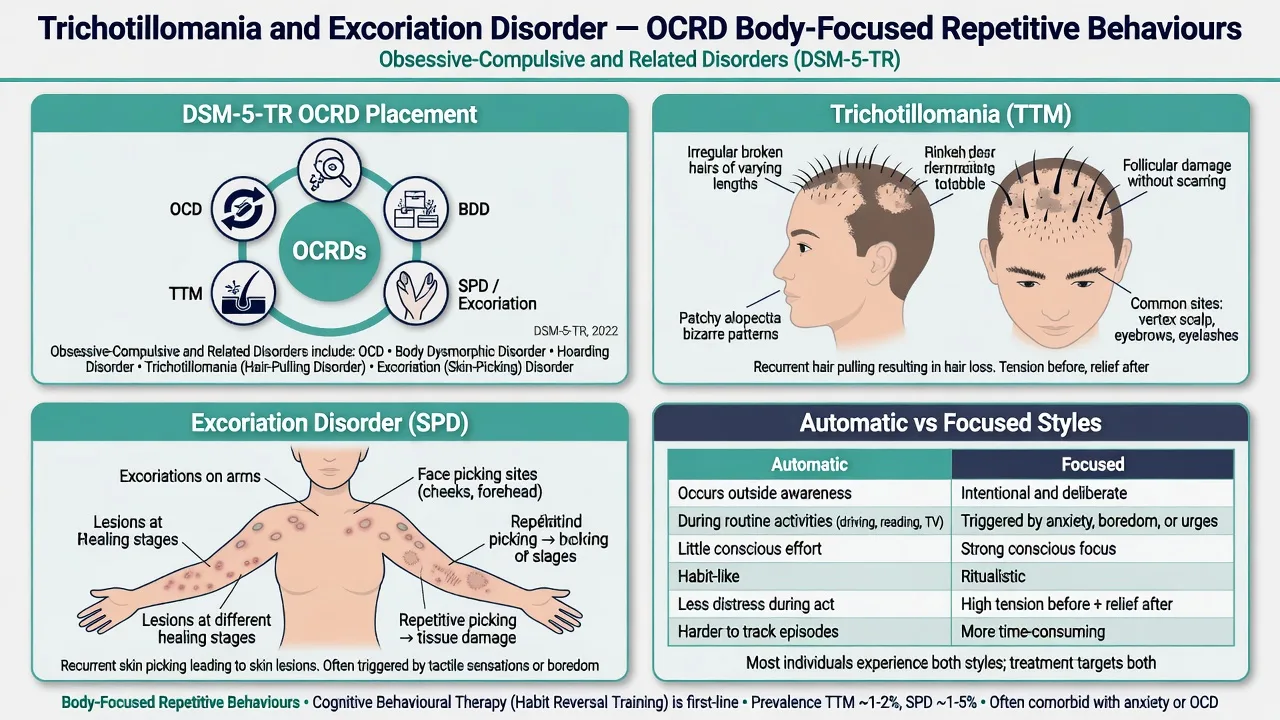
Trichotillomania is recurrent pulling out of one's own hair resulting in hair loss, with repeated attempts to decrease or stop pulling, and clinically significant distress or impairment, not better explained by another medical condition or mental disorder.[12]
Excoriation (skin-picking) disorder is recurrent skin picking resulting in skin lesions, with repeated attempts to decrease or stop, and clinically significant distress or impairment, not attributable to substances, another medical condition, or better explained by another mental disorder (for example psychosis or BDD-driven appearance “repair”).[12][13]
Both are body-focused repetitive behaviours (BFRBs) — a clinically useful umbrella that also includes onychophagia and related grooming excesses — and both sit with OCD, BDD, and hoarding in the obsessive-compulsive and related disorders chapter of DSM-5-TR.[12]
Clinical essence for viva. These are not “bad habits” or vanity. They are neurobehavioural disorders with habit-learning and affective-regulation components. Patients often present late because of shame, camouflage (hats, makeup, long sleeves), and under-asking by clinicians.[7][12]
ICD-11. Expect body-focused repetitive behaviour disorder framing among obsessive-compulsive or related disorders; state which manual you are using when boundaries with OCD or stereotypic movement disorder are examined.[12]
Classification and symptom map
TTM core features
- Recurrent hair pulling with hair loss
- Repeated failed stop attempts
- Distress or functional impairment
- Sites: scalp, brows, lashes, body hair
SPD core features
- Recurrent picking with skin lesions
- Repeated failed stop attempts
- Scarring, pigment change, infection risk
- Sites: face, arms, hands, cuticles, scalp
Automatic style
- Outside full awareness
- Sedentary contexts (TV, reading, driving)
- Sensory/habit-like
- Needs awareness training first
Focused style
- Conscious urge or tension
- Affect regulation (anxiety, boredom, anger)
- May include searching rituals
- Needs urge management and ACT elements
Most patients show mixed styles across settings. Exam answers that only discuss “impulse control” without automatic/focused phenomenology are incomplete.[12]
Epidemiology and risk factors
Headline epidemiology (exam numbers)
Large convenience surveys of US adults place current trichotillomania around 1.7% with high comorbidity (anxiety, depression, OCD, PTSD, ADHD), and current skin-picking disorder around 2.1% with similarly high comorbidity rates.[7][13] Classic college data found full DSM-III-R lifetime criteria near 0.6%, with higher rates of hair loss from pulling that did not meet full criteria — teaching that threshold definitions matter.[6]
Clinical samples often appear female-predominant for adult TTM, while some population surveys show nearer sex parity for current TTM diagnosis; SPD surveys more often show female predominance among identified cases. Onset is typically childhood or adolescence with a chronic waxing-and-waning course if untreated.[7][12]
Pathophysiology and maintaining model
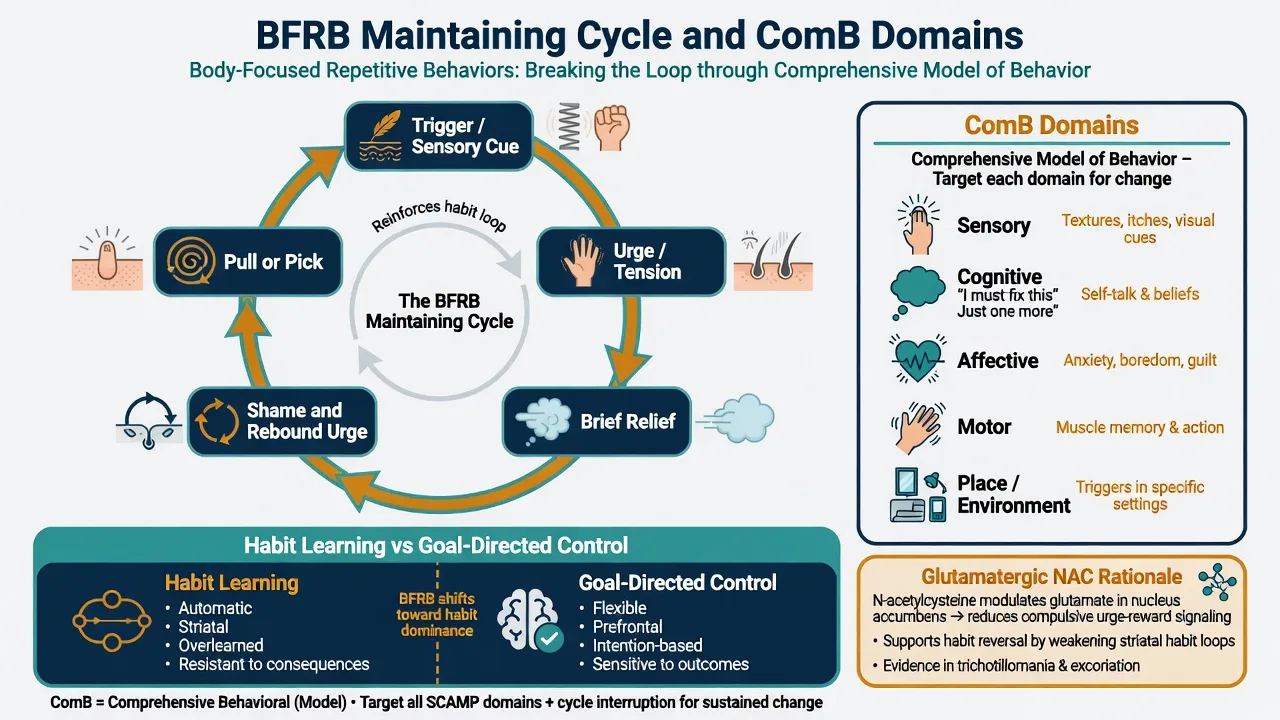
Behavioural model (viva-ready). A sensory cue or affective state triggers an urge or automatic motor sequence; the pull or pick produces brief relief or sensory satisfaction; shame and rebound urge strengthen the loop. Stimulus control and competing responses interrupt the sequence; acceptance-based strategies reduce fusion with urges.[9][11][12]
ComB (Comprehensive Behavioral) map. Assessment and treatment target Sensory, Cognitive, Affective, Motor, and Place/environment domains (SCAMP teaching), individualising the package rather than offering generic “stop picking” advice.[11]
Glutamatergic pharmacologic teaching. NAC is framed as a glutamate modulator that may restore extracellular glutamate balance relevant to compulsive habit circuits (nucleus accumbens teaching). This is a mechanistic hypothesis supporting trials — not proof of a simple “glutamate deficiency.”[1][3][14]
OCRD neighbourhood. Shared family loading and phenomenology with OCD exist, but treatment hierarchy diverges: behaviour therapy/HRT has the strongest effects for TTM, whereas SSRI effects are smaller than for classic OCD.[4][5][12]
Clinical presentation
TTM. Irregular patches with broken hairs of varying length (including tonsure or “Friar Tuck” teaching patterns on the scalp), sparse brows/lashes, and camouflage. Pre-pull rituals may include tactile searching for a “wrong” hair; post-rituals may include examining the root, biting, or swallowing hair (trichophagia).[12]
SPD. Excoriations at different healing stages, scabs, scars, and post-inflammatory pigment change on reachable sites. Picking may target perceived bumps, rough skin, or “imperfections” without meeting full BDD criteria — but BDD comorbidity must be screened.[12][13]
Functional impact. Time spent, work/school avoidance, intimate relationship avoidance, and secondary depression/anxiety are common. Do not minimise impairment because the behaviour “sounds minor.”[7][12]
Differential diagnosis
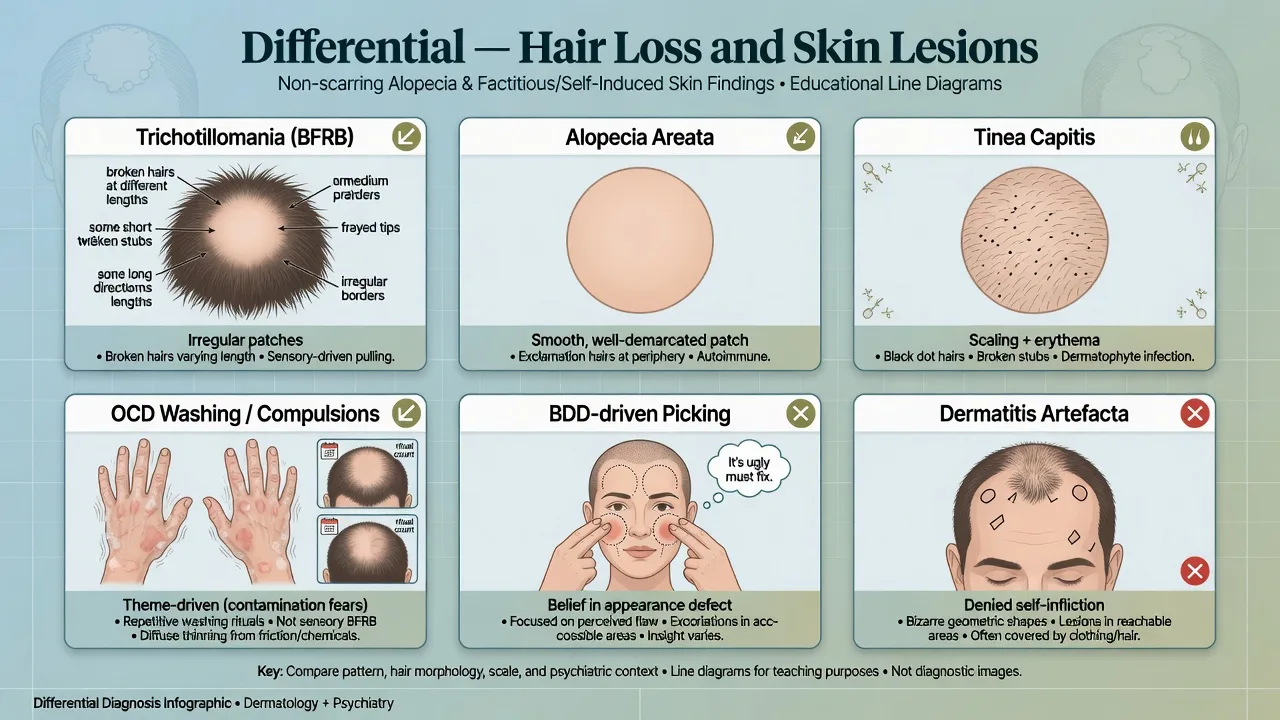
Alopecia areata
- Smooth bald patch
- Exclamation-mark hairs
- No pulling history/rituals
- Autoimmune course
Tinea / scarring alopecia
- Scale, inflammation, black dots
- Loss of follicular ostia if scarring
- KOH/culture/biopsy pathway
- Not a pure psychiatric diagnosis
OCD
- Multi-theme obsessions/compulsions
- Contamination washing may damage skin/hair
- Not primarily sensory BFRB logic
- Can co-occur — formulate both
BDD / artefacta / substance
- BDD: defect belief drives picking
- Dermatitis artefacta: denial of self-infliction
- Stimulants may worsen picking
- Pruritic dermatoses need medical treatment
Also discriminate stereotypic movement disorder (especially in intellectual disability), tics, and self-harm with primary intent to injure rather than grooming/BFRB sensory logic.[12]
Clinical and bedside assessment
History. Sites, hours per day, awareness (automatic vs focused), triggers, rituals, trichophagia, infection history, camouflage, school/work impact, family accommodation, prior treatment fidelity (was true HRT delivered?), substances, and comorbidity screen (OCD, BDD, ADHD, mood, anxiety, other BFRBs).[7][12]
MSE. Visible hair loss or lesions; affect (shame, depression); risk to self; insight into behaviour as a problem; absence of primary psychosis when claiming “bugs under skin” (delusional infestation is a different pathway).[12]
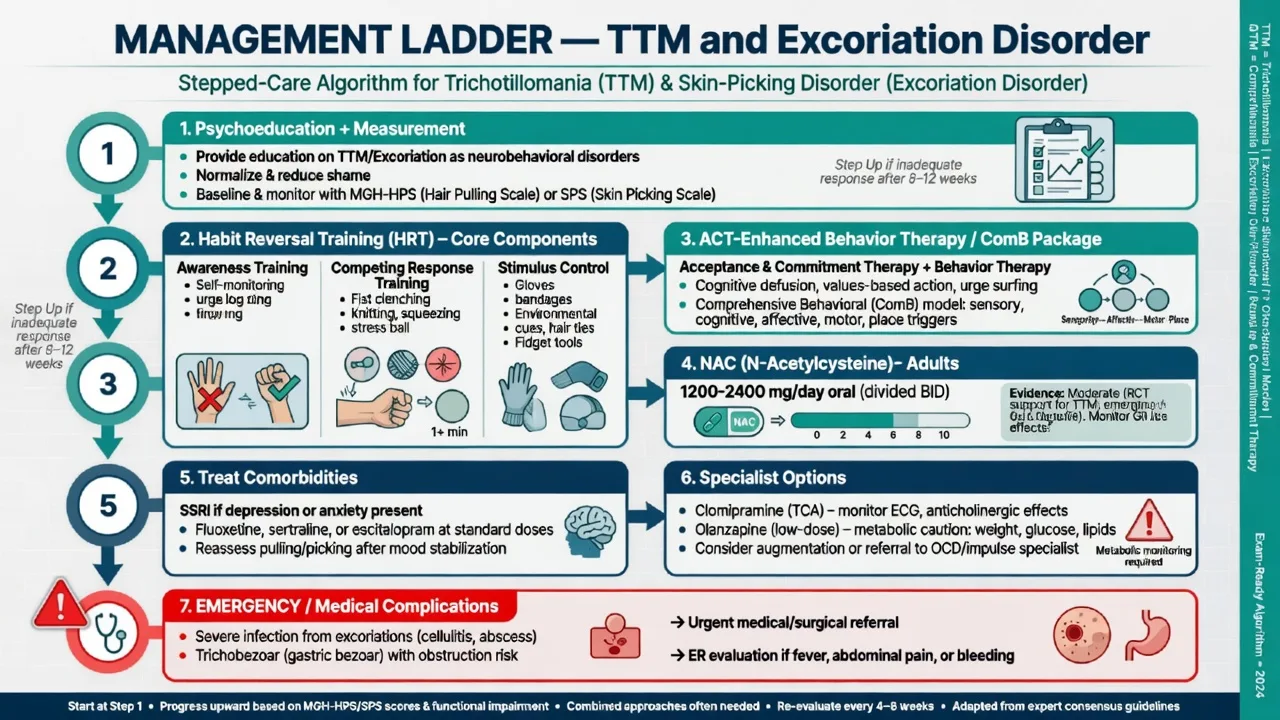
Scales (concept-level). Massachusetts General Hospital Hair Pulling Scale (MGH-HPS) tracks TTM severity; Skin Picking Scale / SPS-R concepts track SPD severity; CGI is used in trials. Scales track response and do not diagnose alone.[1][3][12]
Collateral and dermatology liaison. Family may observe automatic pulling the patient minimises. Dermatology helps exclude alopecia areata/tinea and manage secondary infection while psychiatry leads BFRB treatment.[12]
Investigations and measurement-based care
No biomarker diagnoses idiopathic TTM/SPD. Trichoscopy and dermatology work-up when the alopecia pattern is atypical. GI imaging/surgical pathway if trichophagia plus abdominal pain, early satiety, or obstruction signs — trichobezoar is examinable and dangerous.[12]
Before olanzapine (if ever used), obtain baseline weight, metabolic panel, and consider ECG per local antipsychotic monitoring. Pregnancy testing when relevant. Serial MGH-HPS/SPS plus functional measures support measurement-based care.[10][12]
Management — acute risk and resuscitation
Manage suicidal crisis and severe depression with standard emergency psychiatry pathways. Review stimulant regimens if picking escalated after initiation or dose increase. Do not use shaming confrontation as “motivation.”[7][12]
Management — definitive and stepwise
First-line psychological treatment — habit reversal and modern packages
Habit reversal training (HRT) is the core evidence-based psychological intervention: awareness training (self-monitoring of pulls/picks and antecedents), competing response training (incompatible motor response held for about one minute after urge or after an automatic episode is noticed), stimulus control (environmental redesign), and social support/reinforcement.[4][5][9]
Meta-analyses show behaviour therapy effects larger than serotonin reuptake inhibitor effects for trichotillomania; updated synthesis continues to favour BT/HRT packages for symptom reduction.[4][5]
ACT-enhanced HRT. Controlled evaluation of acceptance and commitment therapy plus habit reversal improved hair-pulling outcomes versus waitlist, targeting urge fusion and values-based action alongside competing responses.[9]
ComB. Comprehensive Behavioral treatment individualises strategies across SCAMP domains; a randomised clinical trial supports ComB for self-rated hair-pulling severity with generally maintained short-term gains.[11]
Generic supportive counselling without awareness training, competing response, and stimulus control is an exam failure mode.[5][12]
Pharmacotherapy — NAC first among drugs for many adults
| Agent | Exam dosing concept (adult oral) | Evidence anchor | Key caveats |
|---|---|---|---|
| N-acetylcysteine (NAC) | Often 1200 mg twice daily (range 1200–2400 mg/day in adult TTM RCT) | Grant 2009 TTM; Grant 2016 SPD | GI upset; paediatric RCT null; product quality varies |
| SSRI (e.g. fluoxetine, sertraline) | Depression/anxiety range first; OCD-range if true OCD comorbidity | Weaker core TTM signal vs BT | Do not declare “BFRB failure” without HRT |
| Clomipramine | Specialist titration (TCA/SRI) | Swedo 1989 vs desipramine | Anticholinergic, cardiac, seizure risk |
| Olanzapine | Low–moderate specialist doses | Van Ameringen 2010 RCT | Weight gain, metabolic syndrome |
| Typical adult oral exam ranges; individualise for age, pregnancy, hepatic/renal function, and interactions; check local product information.[1][3][8][10][14] |
Adult TTM NAC RCT (Grant 2009). Twelve-week double-blind trial: NAC 1200–2400 mg/day oral produced significantly greater reductions on MGH-HPS than placebo, with 56% much/very much improved versus 16% on placebo; improvement emerged around week 9; NAC was well tolerated in that sample.[1]
Adult SPD NAC RCT (Grant 2016). Randomised clinical trial in JAMA Psychiatry found NAC superior to placebo for skin-picking symptoms with good tolerability — the key pharmacologic exam anchor for excoriation disorder.[3]
Paediatric NAC null (Bloch 2013). Double-blind placebo-controlled add-on trial in children and adolescents with TTM found NAC did not separate from placebo. Do not automatically prescribe adult NAC protocols to youth as if the adult RCT generalises.[2]
NAC literature reviews across BFRBs support cautious optimism with need for larger longer trials; it remains the best-supported oral pharmacologic option for many adult BFRB presentations when drug treatment is chosen.[14]
SSRIs, clomipramine, and olanzapine
SSRIs have inconsistent and generally modest effects on core hair-pulling relative to behaviour therapy; use them actively for comorbid depression, anxiety, or co-occurring OCD rather than as sole BFRB therapy.[4][5][12]
Clomipramine was superior to desipramine in a classic short-term double-blind comparison, supporting serotonergic selectivity historically — but anticholinergic and cardiac risks limit first-line modern use.[8]
Olanzapine showed efficacy versus placebo in a small RCT for TTM, yet metabolic burden (weight, glucose, lipids) means it is a specialist option for refractory severe disease after behavioural therapy and NAC discussion, not a casual first script.[10][12]
Specific subtypes and scenarios
Childhood and adolescent TTM. Family-delivered HRT, school camouflage distress, and paediatric NAC null data change the medication conversation; prioritise skills-based care.[2][5]
Automatic-dominant presentations. Heavy emphasis on awareness training, stimulus control (gloves, fidget alternatives, high-risk chair redesign), and environmental prompts.[9][11]
Focused/urge-dominant presentations. Add urge surfing, cognitive defusion, affect regulation, and ACT elements alongside competing response.[9]
Co-occurring TTM + SPD. Common; hierarchy by tissue risk and functional impact; skills generalise across BFRBs.[12][13]
Dermatology consultation-liaison. “Resistant acne scars” or non-healing facial lesions may be picking-driven; avoid endless procedures without BFRB treatment.[12]
Complications and pitfalls
- Missing trichophagia and trichobezoar.[12]
- Treating pure BFRB as OCD with high-dose SSRI alone and no HRT.[4][5]
- Extrapolating adult NAC success to children despite Bloch 2013.[2]
- Shaming patients so they conceal behaviour and drop out.[7]
- Misdiagnosing alopecia areata or tinea as TTM (or the reverse).[12]
- Starting olanzapine without metabolic monitoring or behavioural therapy attempt.[10]
Prognosis and disposition
Without treatment, course is often chronic. Behaviour therapy yields the most consistent short-term gains; relapse is common without maintenance practice. Poorer markers include untreated comorbidity, low homework engagement, and long untreated duration.[5][12]
Disposition is usually outpatient specialist psychology plus medical/psychiatric review; step up intensity for severe tissue damage, inability to function, or high suicide risk. Dermatology co-manages tissue recovery while psychiatry owns the BFRB pathway.[12]
Special populations
Children and adolescents. HRT with caregivers; school support; medication only after specialist consideration — remember paediatric NAC null findings.[2][5]
Pregnancy and lactation. Prefer behavioural therapies; any NAC or psychotropic decision is shared risk–benefit discussion with perinatal psychiatry when available.[12][14]
Intellectual disability and autism. Distinguish stereotypic movements from BFRB; adapt HRT with behavioural support plans and sensory strategies.[12]
Older adults. Late-onset picking needs medical itch and dermatosis work-up; avoid metabolic-heavy agents when possible.[12]
Evidence, guidelines and regional differences
Landmark pillars: Grant adult NAC TTM RCT;[1] Bloch paediatric NAC null;[2] Grant NAC SPD RCT;[3] McGuire meta-analysis of BT vs SRI;[4] Farhat updated meta-analysis favouring BT-HRT;[5] Christenson prevalence classic;[6] Grant population TTM and SPD surveys;[7][13] Swedo clomipramine vs desipramine;[8] Woods ACT/HRT;[9] Van Ameringen olanzapine;[10] Carlson ComB RCT;[11] Grant and Chamberlain clinical update;[12] Lee NAC BFRB review.[14]
In Australian and New Zealand practice, access to psychologists trained in HRT/ComB is often rate-limiting. Refer early to clinicians with BFRB competence; GPs and psychiatrists can start adult NAC discussion after medical review while therapy is arranged. TGA product information and compounding/quality issues matter for NAC. Mental Health Act frameworks are jurisdiction-specific and rarely first-line for pure BFRB without risk or incapacity.[12][14]
Exam pearls
BFRB exam anchors
References
- [1]Grant JE, Odlaug BL, Kim SW N-acetylcysteine, a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study Arch Gen Psychiatry, 2009.PMID 19581567
- [2]Bloch MH, Panza KE, Grant JE, et al. N-Acetylcysteine in the treatment of pediatric trichotillomania: a randomized, double-blind, placebo-controlled add-on trial J Am Acad Child Adolesc Psychiatry, 2013.PMID 23452680
- [3]Grant JE, Chamberlain SR, Redden SA, et al. N-Acetylcysteine in the Treatment of Excoriation Disorder: A Randomized Clinical Trial JAMA Psychiatry, 2016.PMID 27007062
- [4]McGuire JF, Ung D, Selles RR, et al. Treating trichotillomania: a meta-analysis of treatment effects and moderators for behavior therapy and serotonin reuptake inhibitors J Psychiatr Res, 2014.PMID 25108618
- [5]Farhat LC, Olfson E, Nasir M, et al. Pharmacological and behavioral treatment for trichotillomania: An updated systematic review with meta-analysis Depress Anxiety, 2020.PMID 32390221
- [6]Christenson GA, Pyle RL, Mitchell JE Estimated lifetime prevalence of trichotillomania in college students J Clin Psychiatry, 1991.PMID 1938977
- [7]Grant JE, Dougherty DD, Chamberlain SR Prevalence, gender correlates, and co-morbidity of trichotillomania Psychiatry Res, 2020.PMID 32334275
- [8]Swedo SE, Leonard HL, Rapoport JL, et al. A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (hair pulling) N Engl J Med, 1989.PMID 2761586
- [9]Woods DW, Wetterneck CT, Flessner CA A controlled evaluation of acceptance and commitment therapy plus habit reversal for trichotillomania Behav Res Ther, 2006.PMID 16039603
- [10]Van Ameringen M, Mancini C, Patterson B, et al. A randomized, double-blind, placebo-controlled trial of olanzapine in the treatment of trichotillomania J Clin Psychiatry, 2010.PMID 20441724
- [11]Carlson EJ, Malloy EJ, Brauer L, et al. Comprehensive Behavioral (ComB) Treatment of Trichotillomania: A Randomized Clinical Trial Behav Ther, 2021.PMID 34656205
- [12]Grant JE, Chamberlain SR Trichotillomania and Skin-Picking Disorder: An Update Focus (Am Psychiatr Publ), 2021.PMID 35747295
- [13]Grant JE, Chamberlain SR Prevalence of skin picking (excoriation) disorder J Psychiatr Res, 2020.PMID 32781374
- [14]Lee DK, Lipner SR The Potential of N-Acetylcysteine for Treatment of Trichotillomania, Excoriation Disorder, Onychophagia, and Onychotillomania: An Updated Literature Review Int J Environ Res Public Health, 2022.PMID 35681955