Psych · Intellectual disability psychiatry — neurodevelopmental dual diagnosis
Autism and intellectual disability comorbidity
Also known as ASD with intellectual disability · Autism and ID dual diagnosis · Autism with intellectual developmental disorder · Learning disability and autism · Neurodevelopmental dual diagnosis
Exam-exhaustive fellowship reference on autism spectrum disorder co-occurring with intellectual disability — dual-diagnosis assessment (social communication relative to developmental level), communication and AAC, epilepsy comorbidity, challenging behaviour with positive behaviour support, psychopharmacology for severe irritability with monitoring, capacity, safeguarding and transition. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Autism spectrum disorder (ASD) co-occurring with intellectual disability (ID / intellectual developmental disorder) is a high-yield intellectual disability psychiatry and child-and-adolescent interface topic. Fellowship examiners test whether you can apply the relative-to-developmental-level rule for dual diagnosis, run a multimodal assessment without diagnostic overshadowing, integrate communication/AAC, recognise the epilepsy gradient with cognitive impairment, formulate challenging behaviour before drugs, and prescribe for severe irritability only with named trial evidence and monitoring.[1][2][6][9][15]
Overview and definition
Dual diagnosis here means co-occurrence of ASD and ID — not the addiction dual-diagnosis sense. Both are neurodevelopmental, lifelong, and dimensional in support needs. ID requires deficits in intellectual functions and adaptive functioning (conceptual, social, practical domains) with onset during the developmental period; contemporary classification emphasises support needs rather than IQ number alone.[17]
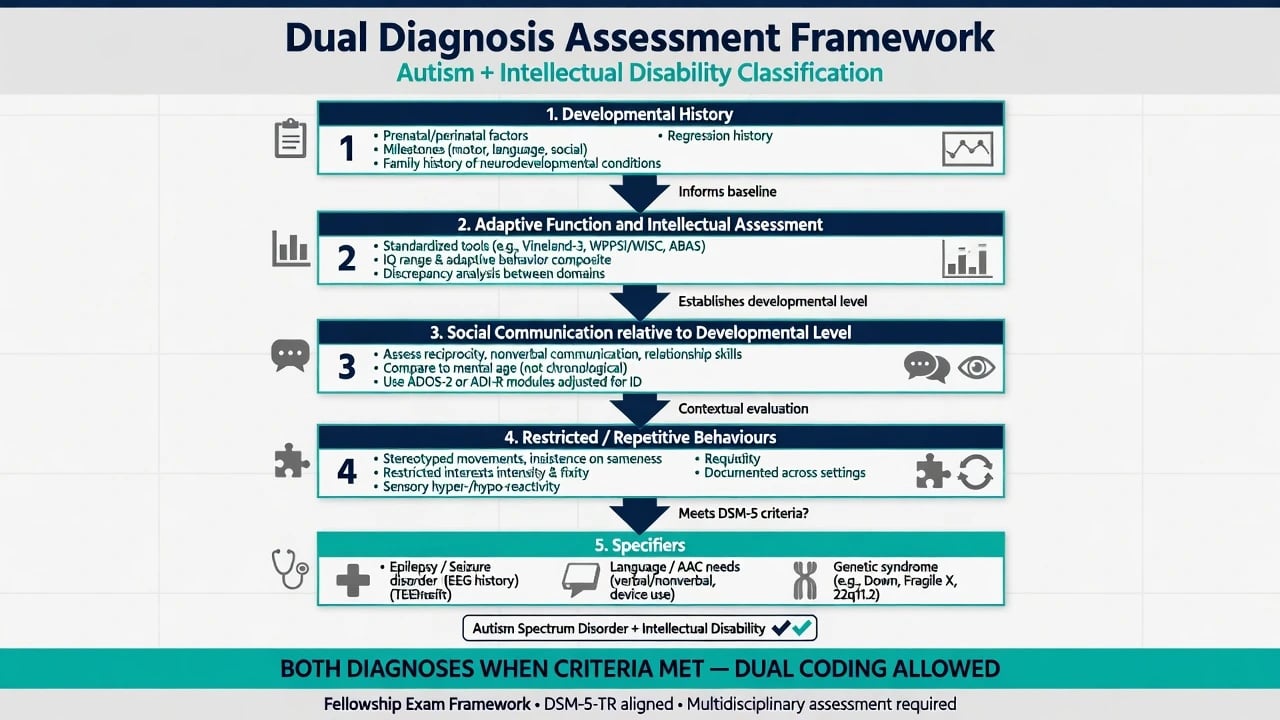
ASD requires persistent social-communication deficits across domains plus restricted/repetitive behaviours (RRBs), early developmental onset, and impairment. When ID is present, DSM-framed practice requires that social communication be below that expected for the general developmental level — otherwise you record ID alone without ASD.[1][2]
Classification
DSM-5-TR / ICD-11 dual coding
- ASD severity levels 1–3 rate support need for social communication and for RRBs separately from ID severity.[1]
- ID severity (mild–profound / mild–severe in adaptive terms) reflects intensity of supports required across adaptive domains.[17]
- ICD-11 maps autism spectrum disorder with co-occurring disorders of intellectual development and language impairment as clinically useful specifiers for service planning.[15]
- Historical labels (autistic disorder with mental retardation; PDD-NOS with cognitive impairment) collapse into dual ASD+ID coding when modern criteria are met.[1][2]
Why dual coding matters clinically
Dual diagnosis predicts higher rates of epilepsy, more intensive communication supports, higher challenging behaviour burden, and different educational/day-service trajectories than either diagnosis alone. Omitting either label risks wrong service pathways and diagnostic overshadowing of the other condition.[3][6][9]
Epidemiology and risk
Global ASD prevalence is on the order of about 1%, with surveillance estimates varying by method and region.[4] Recent US ADDM surveillance among 8-year-olds reported ASD prevalence near 1 in 36, with a substantial minority meeting criteria for co-occurring intellectual disability (examiners often expect roughly one-third order of magnitude in contemporary samples, recognising method-dependent ranges).[3]
Among people with ID, ASD rates are elevated relative to the general population. Psychiatric comorbidity (ADHD, anxiety, and other disorders) is common in ASD samples; dual diagnosis multiplies adaptive and behavioural complexity.[5] Male predominance remains, but girls with dual diagnosis may be under-recognised when assessment assumes a classic male social phenotype.[1][15]
Epilepsy co-occurs with ASD at rates far above population baseline; systematic reviews document bidirectional co-occurrence of epilepsy and autism, with cognitive impairment as a major risk stratifier.[6][7][8] Challenging behaviour is prevalent in ID populations in total-population studies and is a frequent presentation of dual-diagnosis services.[9]
Pathophysiology and mechanisms
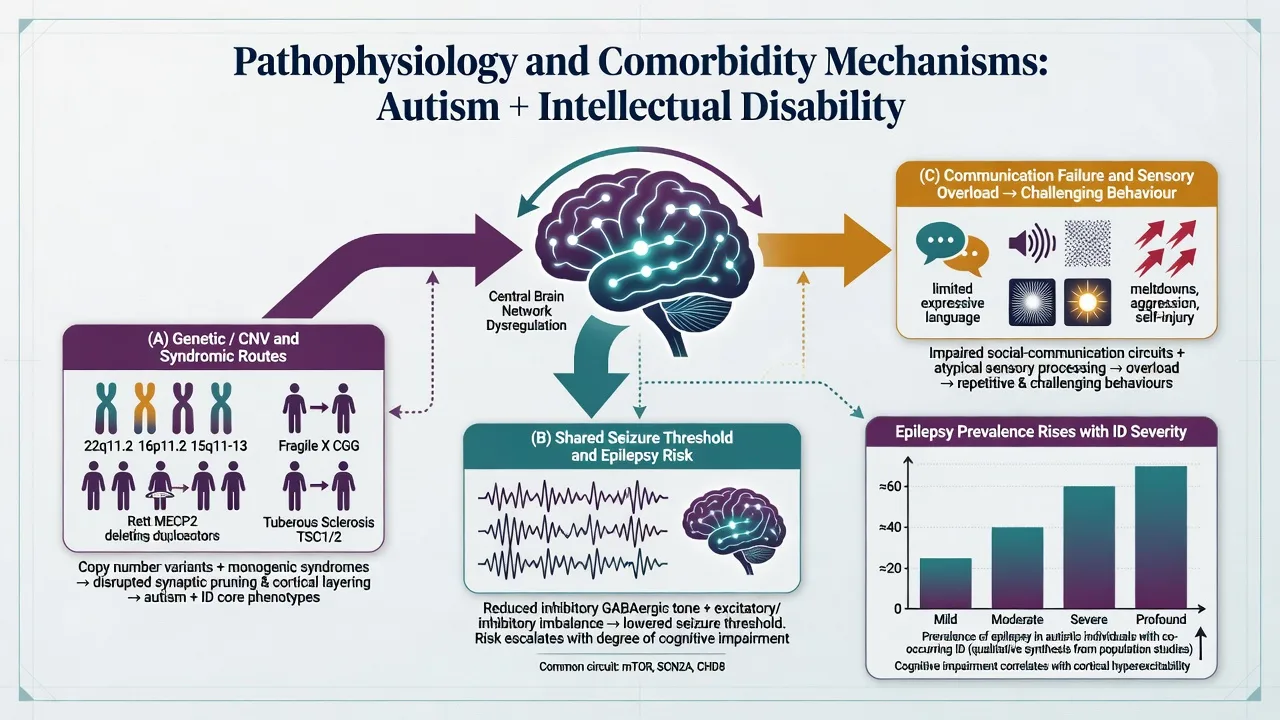
There is no single biomarker that diagnoses dual ASD–ID. Architecture includes high heritability for ASD, rare copy-number variants, and syndromic forms that concentrate dual phenotypes (fragile X, tuberous sclerosis complex, Angelman, and related genetic conditions — work up when indicated).[1][15]
Lower cognitive/adaptive level associates with higher epilepsy risk in ASD cohorts — a key viva fact linking the three domains examiners care about (ASD, ID, seizures).[6][7][8] Sensory hyper/hyporeactivity, executive limits, and communication failure provide mechanistic bridges to challenging behaviour without requiring a primary psychiatric drug target.[9][15]
Vaccines do not cause autism — a classic exam trap that still appears in parental counselling stations.[1]
Clinical presentation
Developmental and social-communication pattern
Early dual-diagnosis presentations combine delayed milestones with social-communication red flags beyond developmental expectation: limited joint attention, inconsistent response to name, reduced reciprocal play, restricted play repertoires, sensory aversions, and RRBs (stereotypies, sameness distress, intense interests scaled to developmental level).[1][2]
School-age dual diagnosis often shows limited peer engagement, need for visual structure, language delay or reliance on AAC, adaptive skill gaps, and behavioural escalation around transitions, noise, or demand. Adolescent and adult presentations include ongoing support needs, risk of behavioural crises at service transitions, and less camouflaging capacity when cognitive impairment is significant.[15][16]
Epilepsy interface
Suspect seizures with new staring spells, nocturnal events, unexplained falls, developmental regression, or abrupt post-event behavioural change. Do not assume all repetitive movements are non-epileptic stereotypy — and do not treat all stereotypy as seizure.[6][7][8]
Challenging behaviour phenotypes
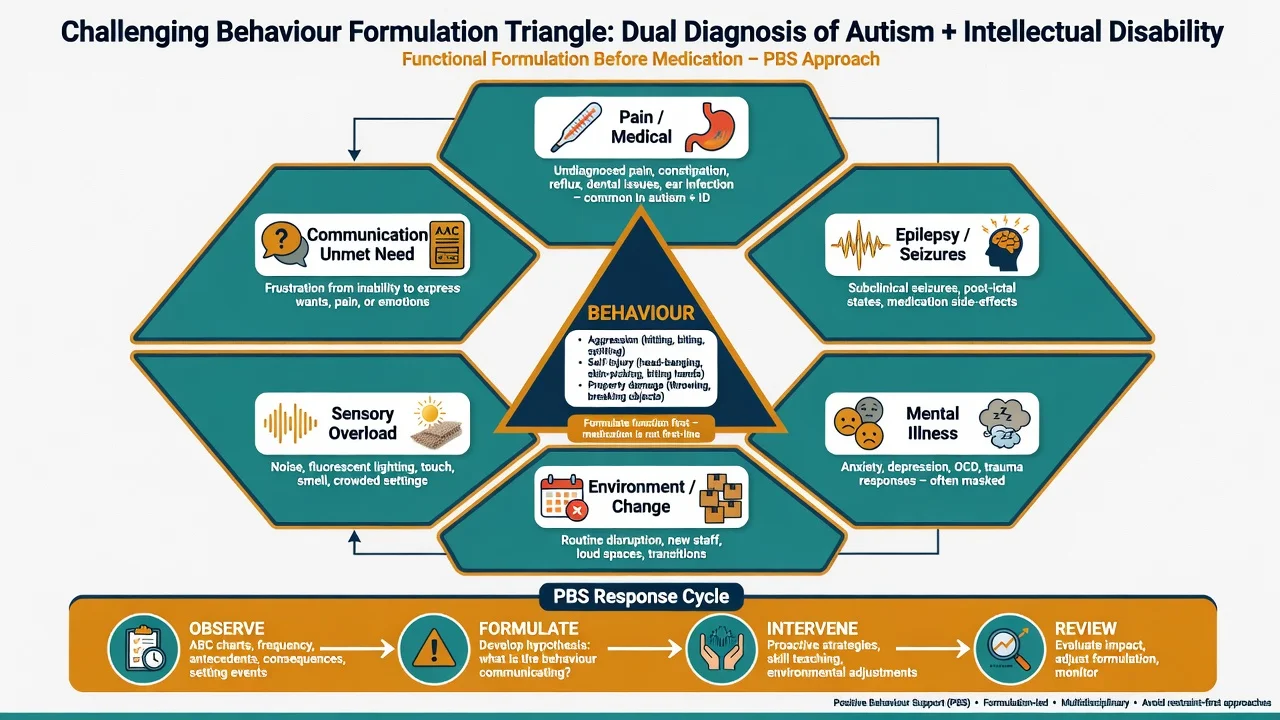
Common phenotypes: aggression toward others, self-injury, property destruction, severe disruption, and absconding. Until proven otherwise, treat behaviour as communication of unmet need (pain, overload, demand, change, illness, seizure-related state, or mental illness).[9]
Differential diagnosis
ID alone vs ASD+ID
- ID alone: social skills roughly match developmental level
- ASD+ID: social reciprocity and RRBs below developmental expectation
- Use multi-setting observation and developmental history, not IQ alone
- Dual coding when both thresholds met
Language / hearing / SCD
- Hearing impairment can mimic social disengagement
- Language disorder without RRB pattern is not ASD
- Social (pragmatic) communication disorder lacks RRBs
- Audiology is mandatory in language delay pathways
ADHD / anxiety / trauma
- ADHD co-occurs frequently — dual/triple diagnosis allowed
- Anxiety may drive avoidance; developmental RRB pattern still needed for ASD
- Trauma/attachment can alter social behaviour but need care history pattern
- Do not force either/or when criteria for multiple conditions are met
Psychosis / catatonia / epilepsy
- Autistic oddity is not psychosis without form change and functional break
- Catatonia: mutism, posturing, refusal to eat/drink — emergency pathway
- Nonconvulsive seizures and post-ictal states mimic behaviour change
- Atypical regression → epileptic encephalopathy differentials
Thurm and colleagues synthesise the field problem of differentiating ID from ASD and of identifying dual occurrence without circular reasoning — the practical answer is multi-method assessment anchored to developmental expectation.[2]
Dual-diagnosis assessment
Structure the history
- Developmental timeline — motor, speech, play, social milestones, regression windows.[1]
- Adaptive function — conceptual, social, practical skills across home, school, community.[17]
- Social communication relative to mental age — reciprocity, nonverbal communication, relationships.[2]
- RRBs and sensory profile — stereotypies, sameness, restricted interests, hyper/hyporeactivity.[1]
- Communication methods — speech, gesture, PECS/visual schedules, speech-generating devices.[15]
- Epilepsy and medical — seizure history, AEDs, pain sources, sleep, constipation, dental, reflux.[6][8]
- Behaviour formulation — antecedents, behaviour, consequences; carer response patterns; restrictive practices in use.[9]
- Risk and capacity — self-injury, aggression, exploitation, neglect, decision-specific capacity.
Tools and collateral
Use clinical judgment with structured aids (ADOS-2 adapted administration; ADI-R developmental interview) — tools support, they do not replace, dual diagnosis decisions in severe ID.[1][16] Adaptive scales (e.g. Vineland conceptual) and formal cognitive assessment by psychology complete the ID limb.[17] Always obtain collateral from parents/carers, school, day service, and prior speech/behaviour reports.[1]
Communication assessment
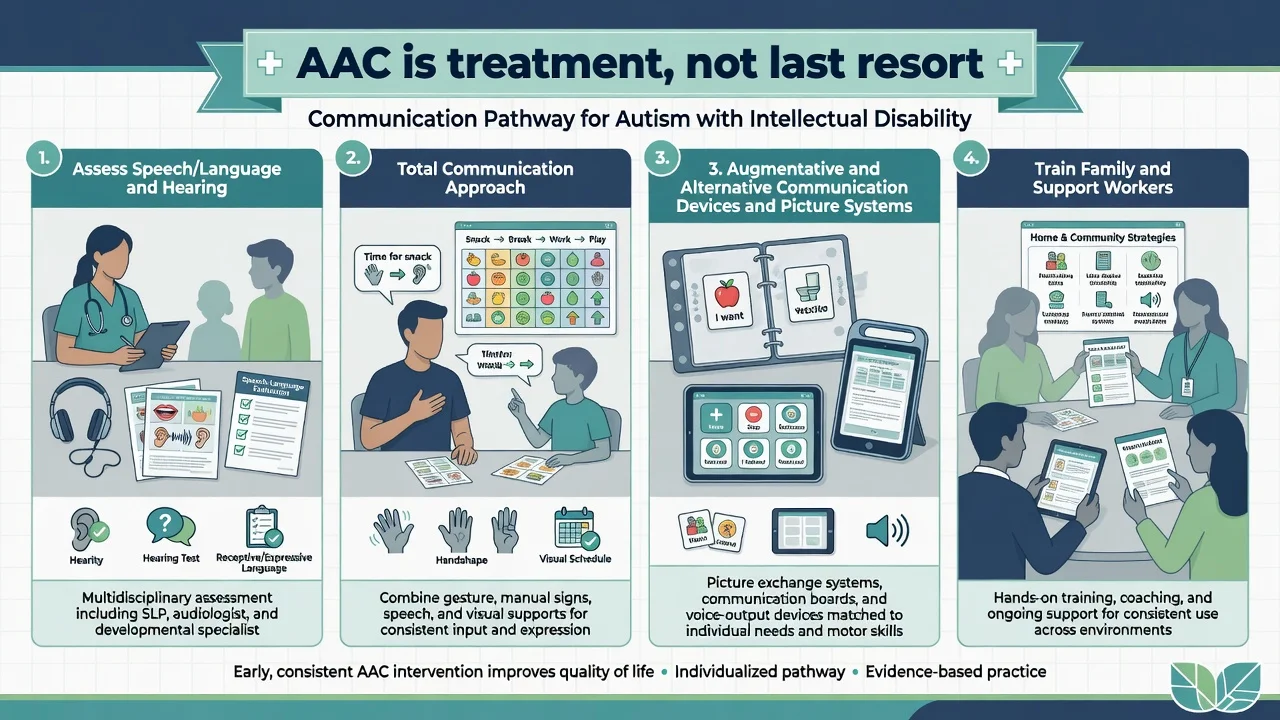
Assess hearing early. Involve speech-language pathology for total communication (speech, gesture, signs, visual supports) and AAC candidacy. Withholding AAC while waiting for speech to appear is a common service failure and prolongs challenging behaviour driven by communication frustration.[1][15]
Investigations
| Clinical question | Investigate | Do not routinely... |
|---|---|---|
| Language delay / first dual-diagnosis workup | Audiology; speech/language assessment | Assume hearing is normal without testing |
| Aetiology after dual diagnosis | Chromosomal microarray; fragile X; further genetics if indicated | Order endless panels without clinical indication |
| Seizure red flags / atypical regression | EEG ± neurology review; imaging if focal signs | Routine brain imaging for typical dual diagnosis without red flags |
| Behaviour change | Pain/medical screen (dental, constipation, infection, reflux, otitis, urinary) | Attribute solely to autism/ID |
| Before antipsychotic for irritability | Weight/BMI, BP, fasting glucose/lipids, ECG if indicated, EPS baseline | Start high-dose polypharmacy without baseline |
Genetic evaluation after ASD diagnosis is standard recommendation in major paediatric guidance; dual diagnosis strengthens the yield rationale for aetiology-seeking workup.[1][16]
Acute management and resuscitation
Acute behavioural crisis: low-stimulus environment, remove triggers, preferred communication method available, least-restrictive de-escalation, trained support staff, and medical triage. PRN psychotropics only within a documented plan with review — never as culture of care.[9][14]
Peri-ictal or post-ictal behaviour: stabilise seizure pathway with neurology; avoid mislabeling post-ictal confusion as primary psychosis or primary autism meltdown.[6][8]
Catatonia in ASD: mutism, posturing, immobility, food/fluid refusal — escalate on medical-psychiatric emergency pathways (lorazepam-challenge concept awareness for viva).[16]
Safeguarding applies: neglect, exploitation, inappropriate restrictive practices, and carer burnout are clinical issues, not pure social afterthoughts.[15]
Definitive management
Foundations (always)
- Educational and day-service adaptations, predictable routines, visual schedules.[1][15]
- Speech/AAC and occupational therapy sensory supports.[1]
- Parent/carer training — parent training improves disruptive behaviour more than education alone in ASD (Bearss RCT framing transferable to dual-diagnosis behavioural care).[13]
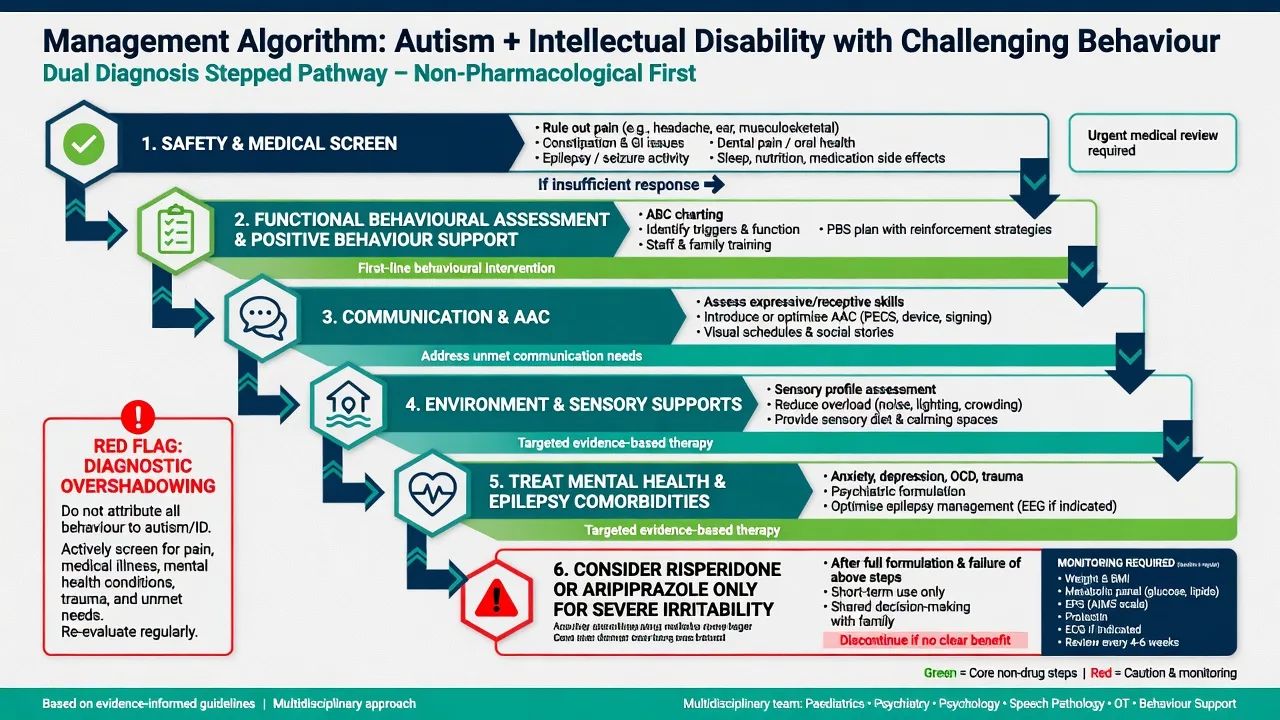
- Positive behaviour support (PBS) / functional behavioural assessment before psychotropics.[9]
Challenging behaviour
Emerson population work established that challenging behaviour is common enough in ID services to require system-level planning, not only individual crisis response.[9] First-line responses are environmental, communicative, skill-building, and medical — not lifelong antipsychotics for non-specific aggression.
Tyrer 2008 (Lancet): in adults with intellectual disability and aggressive challenging behaviour, risperidone and haloperidol were not superior to placebo on the primary aggression outcome — a critical exam pearl against routine antipsychotic use for ID aggression without a clear psychiatric indication.[12]
Pharmacotherapy for severe irritability (ASD indication)
No medication treats core ASD social-communication deficits as a primary indication.[1][14][16]
When severe irritability (aggression, severe tantrums, self-injury) persists after behavioural optimisation and medical exclusion, selective pharmacotherapy may be considered with named trial evidence and monitoring.[10][11][14]
- Risperidone (oral): RUPP/McCracken RCT evidence in children with autism and serious behavioural problems. Start low and slow — commonly about 0.25–0.5 mg/day depending on weight, with gradual titration toward the lowest effective dose (trial mean effective totals often around 1–2 mg/day). Monitor weight, fasting glucose and lipids, EPS, and prolactin; review for dose reduction when stable.[10][14]
- Aripiprazole (oral): Owen RCT evidence for irritability in children/adolescents with autistic disorder. Often start 2 mg daily, then titrate (fixed-dose programmes commonly studied in the 5–15 mg/day range). Monitor metabolic effects and akathisia.[11][14]
Meta-analytic synthesis supports pharmacologic options for severe irritability in autism with attention to adverse effects — not carte blanche polypharmacy.[14]
Treat comorbidities as independent targets
Epilepsy control, sleep, ADHD, anxiety, and depression each deserve explicit formulation and adapted intervention — dual diagnosis is not a licence for diagnostic monism.[5][6][15]
Subtypes and clinical scenarios
| Scenario | Exam focus |
|---|---|
| Toddler dual diagnosis | Early identification, audiology, genetics pathway, early supports without waiting for perfect paperwork |
| Non-verbal school-age with self-injury | AAC urgency, pain screen, functional analysis, PBS, irritability meds only if severe and formulated |
| Adolescent with new seizures and behaviour change | Epilepsy workup, AED psychiatric effects, transition planning |
| Adult community dual diagnosis on long-term antipsychotic | Deprescribing review, Tyrer framing, metabolic harm, clear target symptom |
| Syndromic dual phenotype | Fragile X / TSC interfaces, family genetic counselling, epilepsy likelihood |
| Forensic vulnerability | Capacity, suggestibility, exploitation, adapted interview |
Complications and pitfalls
- Diagnostic overshadowing — missing pain, epilepsy, depression, abuse under an autism/ID label.[9][15]
- Misattributing all behaviour to autism or all to ID without dual formulation.[2]
- Premature antipsychotic without functional analysis; chronic metabolic harm and tardive risk.[12][14]
- Missing epilepsy or over-treating stereotypy as seizure.[6][8]
- Withholding AAC; over-focusing on spoken language only.[15]
- Vaccine myth and parental guilt in counselling stations.[1]
Prognosis and disposition
Outcomes are lifelong and highly variable. Better adaptive trajectories associate with communication access (including AAC), seizure control, support intensity, family resources, and treated mental health comorbidity — not with a single IQ point.[15][17] Autism literature documents premature mortality risk; epilepsy and associated medical/psychiatric burdens contribute to worse outcomes and demand active physical health partnership.[7][18]
Disposition planning: multiagency community supports (e.g. NDIS-type packages in ANZ), specialist dual-diagnosis/ID psychiatry input for complex behaviour, least-restrictive accommodation, education/employment pathways, and transition from child to adult services with a written care plan.[15]
Special populations
- Profound ID with minimal speech — observational assessment, AAC-centred care, high epilepsy vigilance.[2][6]
- Girls and women — under-recognition risk; do not require a male-typical social phenotype.[15]
- Indigenous and culturally diverse families — avoid biased under-diagnosis of autism in delayed development; use culturally safe collateral.[15]
- Forensic and secure settings — vulnerability, capacity, and adapted communication are mandatory.
Evidence and regional guidelines
RANZCP-informed dual-diagnosis and ID psychiatry practice emphasises least restrictive care, capacity and supported decision-making, PBS-informed behaviour support, and careful psychotropic stewardship. Australian disability systems (e.g. NDIS) interface with mental health — document support needs clearly without inventing statute section numbers.[15]
Landmark names to drop in viva: Hyman (AAP), Thurm (dual differentiation), Maenner (ADDM), Simonoff (comorbidity), Lukmanji / Woolfenden / Viscidi (epilepsy), Emerson (challenging behaviour epidemiology), Bearss (parent training), McCracken RUPP, Owen aripiprazole, Tyrer Lancet 2008, Lord Lancet Commission, Hirvikoski mortality.[1][2][3][5][6][7][9][10][11][12][13][15][18]
Exam pearls
Classic stem patterns
- Non-verbal child with ID — is this also autism? → relative social communication + RRBs.
- Behaviour escalation — pain? epilepsy? communication? environment? mental illness?
- Start risperidone? → only after formulation; dose low; monitor metabolic panel.
- Adult on long-term risperidone for years for "aggression" → review indication (Tyrer), metabolic harm, PBS plan.
- New staring spells in dual diagnosis → epilepsy pathway, not only stereotypy.
Capacity maxim
Capacity is decision-specific and enhanced by supported decision-making and accessible communication — dual diagnosis does not equal global incapacity.[15][17]
References
- [1]Hyman SL, Levy SE, Myers SM; Council on Children with Disabilities, Section on Developmental and Behavioral Pediatrics Identification, Evaluation, and Management of Children With Autism Spectrum Disorder Pediatrics, 2020.PMID 31843864
- [2]Thurm A, Farmer C, Salzman E, Lord C, Bishop S State of the Field: Differentiating Intellectual Disability From Autism Spectrum Disorder Front Psychiatry, 2019.PMID 31417436
- [3]Maenner MJ, Warren Z, Williams AR, et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020 MMWR Surveill Summ, 2023.PMID 36952288
- [4]Zeidan J, Fombonne E, Scorah J, et al. Global prevalence of autism: A systematic review update Autism Res, 2022.PMID 35238171
- [5]Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, Baird G Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample J Am Acad Child Adolesc Psychiatry, 2008.PMID 18645422
- [6]Lukmanji S, Manji SA, Kadhim S, et al. The co-occurrence of epilepsy and autism: A systematic review Epilepsy Behav, 2019.PMID 31398688
- [7]Woolfenden S, Sarkozy V, Ridley G, Coory M, Williams K A systematic review of two outcomes in autism spectrum disorder - epilepsy and mortality Dev Med Child Neurol, 2012.PMID 22348343
- [8]Viscidi EW, Johnson AL, Spence SJ, Buka SL, Morrow EM, Triche EW The association between epilepsy and autism symptoms and maladaptive behaviors in children with autism spectrum disorder: a population-based study Autism, 2014.PMID 24165273
- [9]Emerson E, Kiernan C, Alborz A, et al. The prevalence of challenging behaviors: a total population study Res Dev Disabil, 2001.PMID 11263632
- [10]McCracken JT, McGough J, Shah B, et al.; Research Units on Pediatric Psychopharmacology Autism Network Risperidone in children with autism and serious behavioral problems N Engl J Med, 2002.PMID 12151468
- [11]Owen R, Sikich L, Marcus RN, et al. Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder Pediatrics, 2009.PMID 19948625
- [12]Tyrer P, Oliver-Africano PC, Ahmed Z, et al. Risperidone, haloperidol, and placebo in the treatment of aggressive challenging behaviour in patients with intellectual disability: a randomised controlled trial Lancet, 2008.PMID 18177776
- [13]Bearss K, Johnson C, Smith T, et al. Effect of parent training vs parent education on behavioral problems in children with autism spectrum disorder: a randomized clinical trial JAMA, 2015.PMID 25898050
- [14]Fung LK, Mahajan R, Nozzolillo A, et al. Pharmacologic Treatment of Severe Irritability and Problem Behaviors in Autism: A Systematic Review and Meta-analysis Pediatrics, 2016.PMID 26908468
- [15]Lord C, Charman T, Havdahl A, et al. The Lancet Commission on the future of care and clinical research in autism Lancet, 2022.PMID 34883054
- [16]Volkmar F, Siegel M, Woodbury-Smith M, King B, McCracken J, State M; AACAP Committee on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder J Am Acad Child Adolesc Psychiatry, 2014.PMID 24472258
- [17]Schalock RL, Luckasson R, Tassé MJ An Overview of Intellectual Disability: Definition, Diagnosis, Classification, and Systems of Supports (12th ed.) Am J Intellect Dev Disabil, 2021.PMID 34700345
- [18]Hirvikoski T, Mittendorfer-Rutz E, Boman M, Larsson H, Lichtenstein P, Bölte S Premature mortality in autism spectrum disorder Br J Psychiatry, 2016.PMID 26541693