Psych · intellectual-disability
Capacity and supported decision-making in ID
Also known as Supported decision-making · Decision-making capacity intellectual disability · Legal capacity UNCRPD · Guardianship intellectual disability · Substitute decision-making ID · Mental capacity learning disability · Article 12 CRPD · Easy Read consent
Exam-exhaustive fellowship reference on decision-specific capacity and supported decision-making in intellectual disability — four functional abilities after accessible supports, UNCRPD Article 12 legal capacity vs mental capacity, guardianship least-restrictive principles, substitute pathways when supports fail, and CASC communication. Statutes are jurisdiction-specific; no invented section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
9 MCQs with explanations
Target exams
Red flags
Overview and definition
People with intellectual disability (ID) have historically been subject to status-based incapacity assumptions — as if diagnosis or IQ alone cancelled legal agency. Contemporary ethics and multi-board exam standards reject that model. Decision-making capacity is a clinical, functional judgment about whether this person can make this decision now, after material information has been disclosed in an accessible form and supports have been offered.[1][2][5]
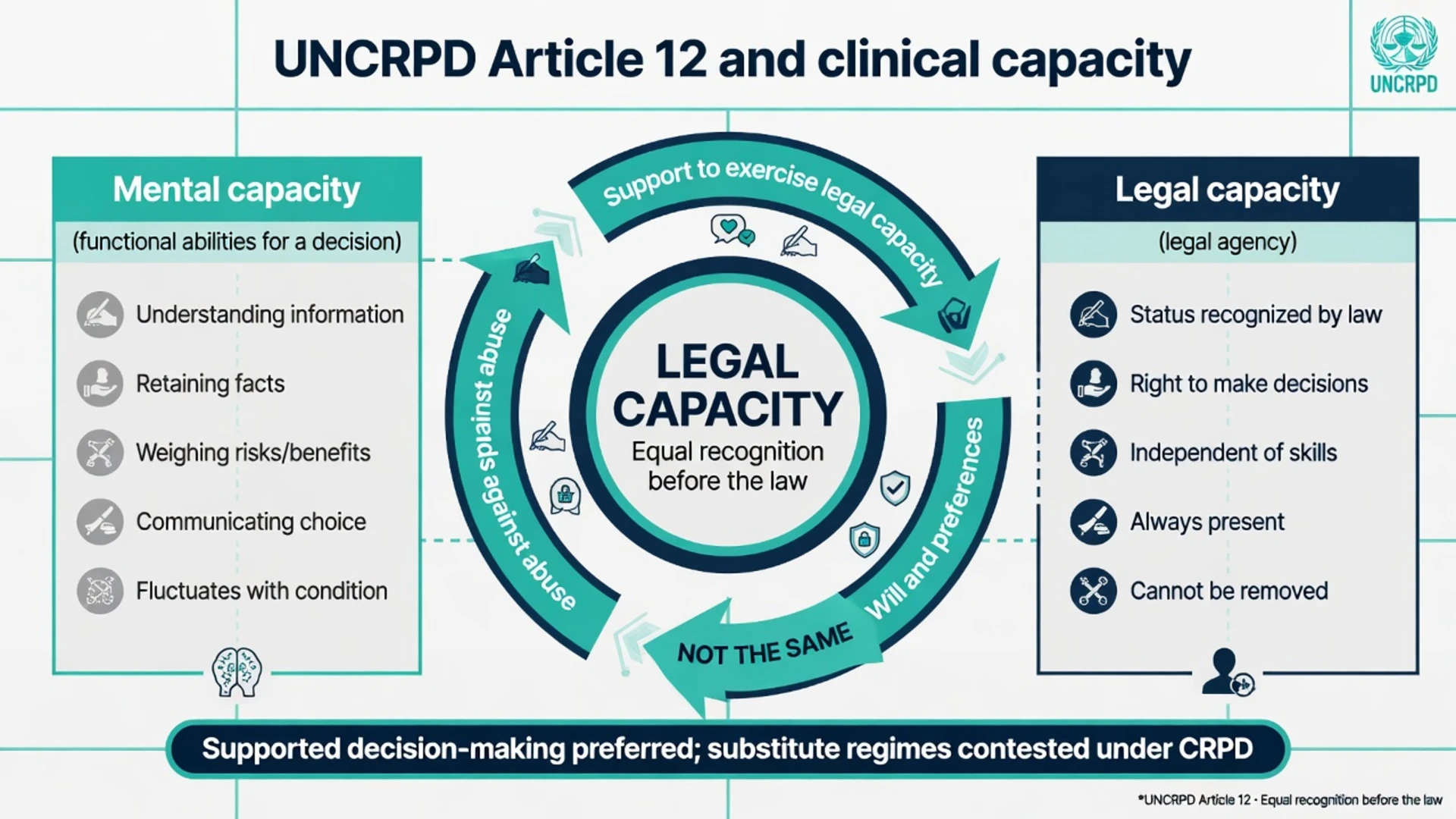
Legal capacity (UNCRPD Article 12 language) refers to recognition as a person before the law and the right to exercise legal agency on an equal basis with others, with access to support. Mental capacity (clinical functional abilities) is a different construct. Exams expect you to know both languages and the policy tension between them without inventing statute text.[10][12][17]
Informed consent (or informed refusal) still requires three pillars: capacity for that decision; adequate material information; and voluntariness free of coercion and undue influence.[2][5]
| Principle | Clinical meaning in ID practice |
|---|---|
| Presumption of capacity | Adults with ID are assumed capable until evidence shows otherwise for this decision |
| Decision-specific | Capacity for antibiotics is not capacity for complex surgery or financial instruments |
| Time-specific | Acute illness, post-ictal state, pain, or sedation can temporarily impair abilities |
| Unwise ≠ incapable | A capable person with ID may refuse recommended care |
| Supports first | Maximise demonstration of abilities before substituting |
| Least restrictive | If substitute authority is needed, limit domain and duration |
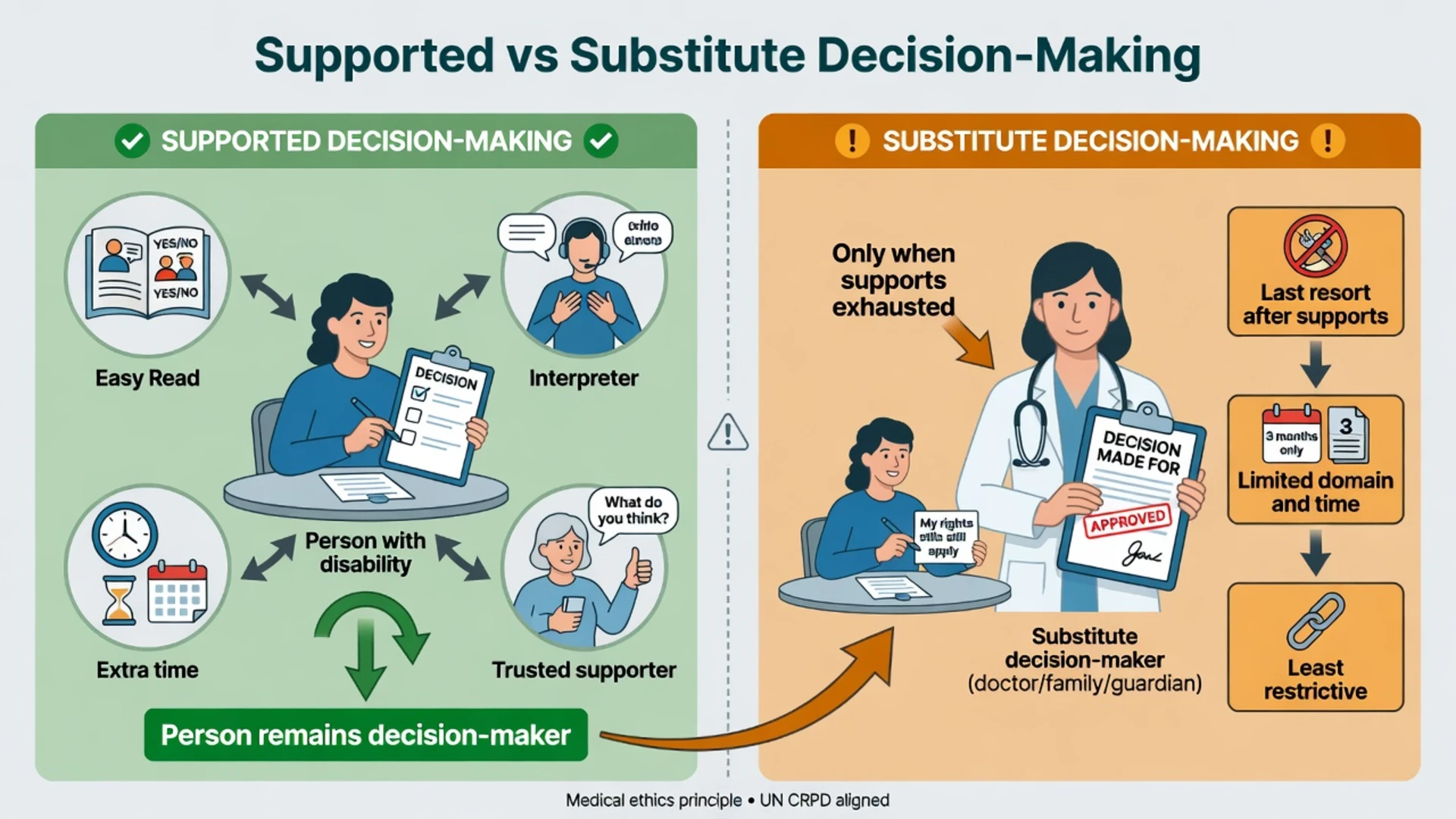
Supported decision-making vs substitute decision-making
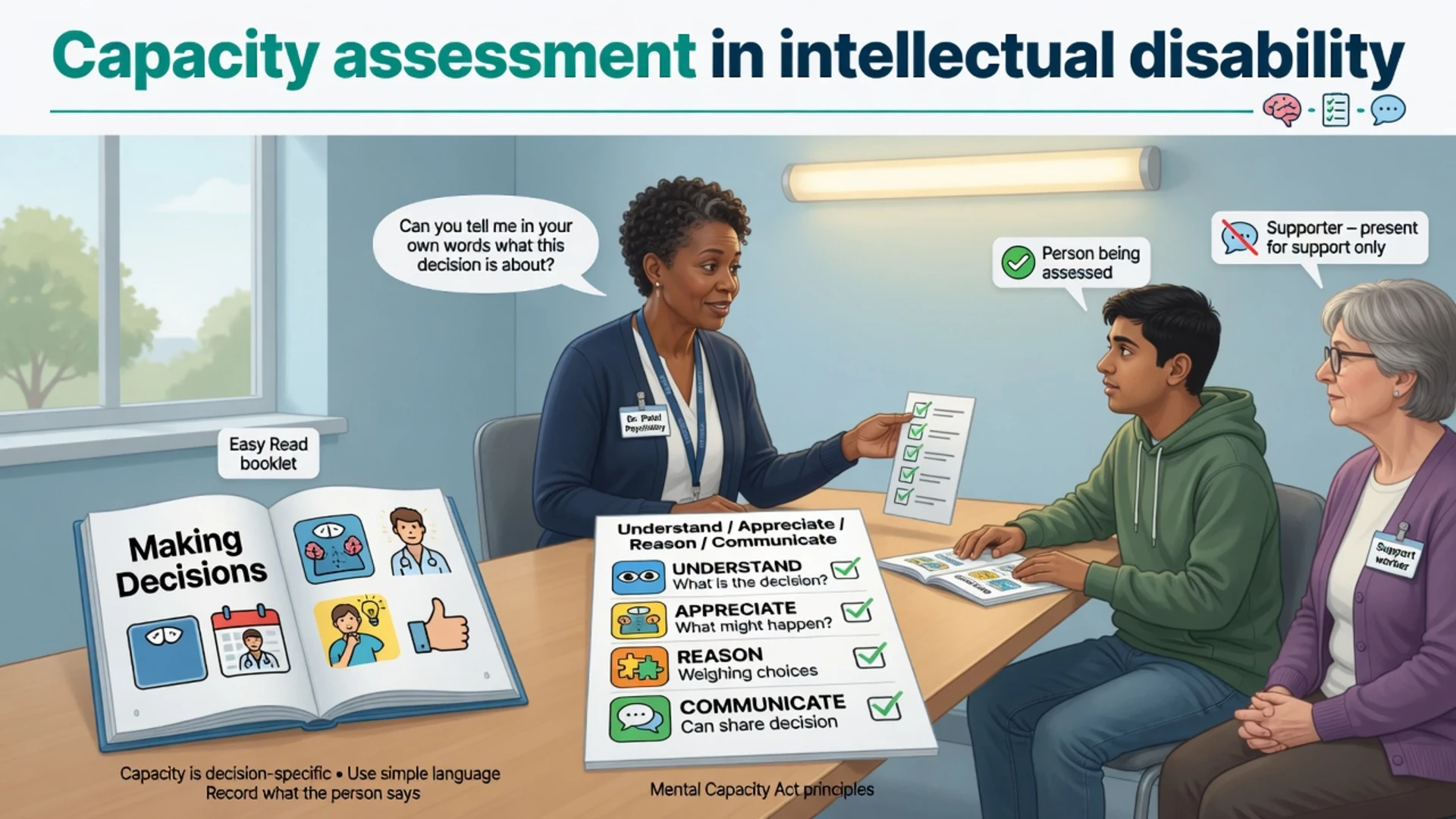
Supported decision-making (SDM) means the person remains the decision-maker while receiving tailored help to understand options, express will and preferences, and communicate a choice. Supports may include Easy Read materials, visual aids, chunking information, multiple shorter sessions, sensory adjustments, interpreters, AAC, and a trusted supporter who assists without taking over.[10][11][13][18]
Substitute decision-making means another person or body decides on the person's behalf under a lawful framework (guardian, attorney, proxy hierarchy, best-interests or equivalent process). SDM is ethically preferred and rights-aligned; substitute pathways are a last resort after reasonable supports, not the first move when ID is noted in the chart.[10][11][12]
Shared decision-making (clinician–patient partnership about options) is complementary but not identical to SDM as a disability-rights construct of legal agency support.[13]
Critical appraisal matters for exams: SDM is strongly promoted as an alternative to guardianship, yet implementation research warns that poorly designed "support" can become informal substitute control if safeguards against conflict of interest and undue influence are weak.[11][17]
The four abilities (adapted for ID)
The modern functional model (Appelbaum and Grisso) rests on four abilities rather than a diagnostic label.[1][2]
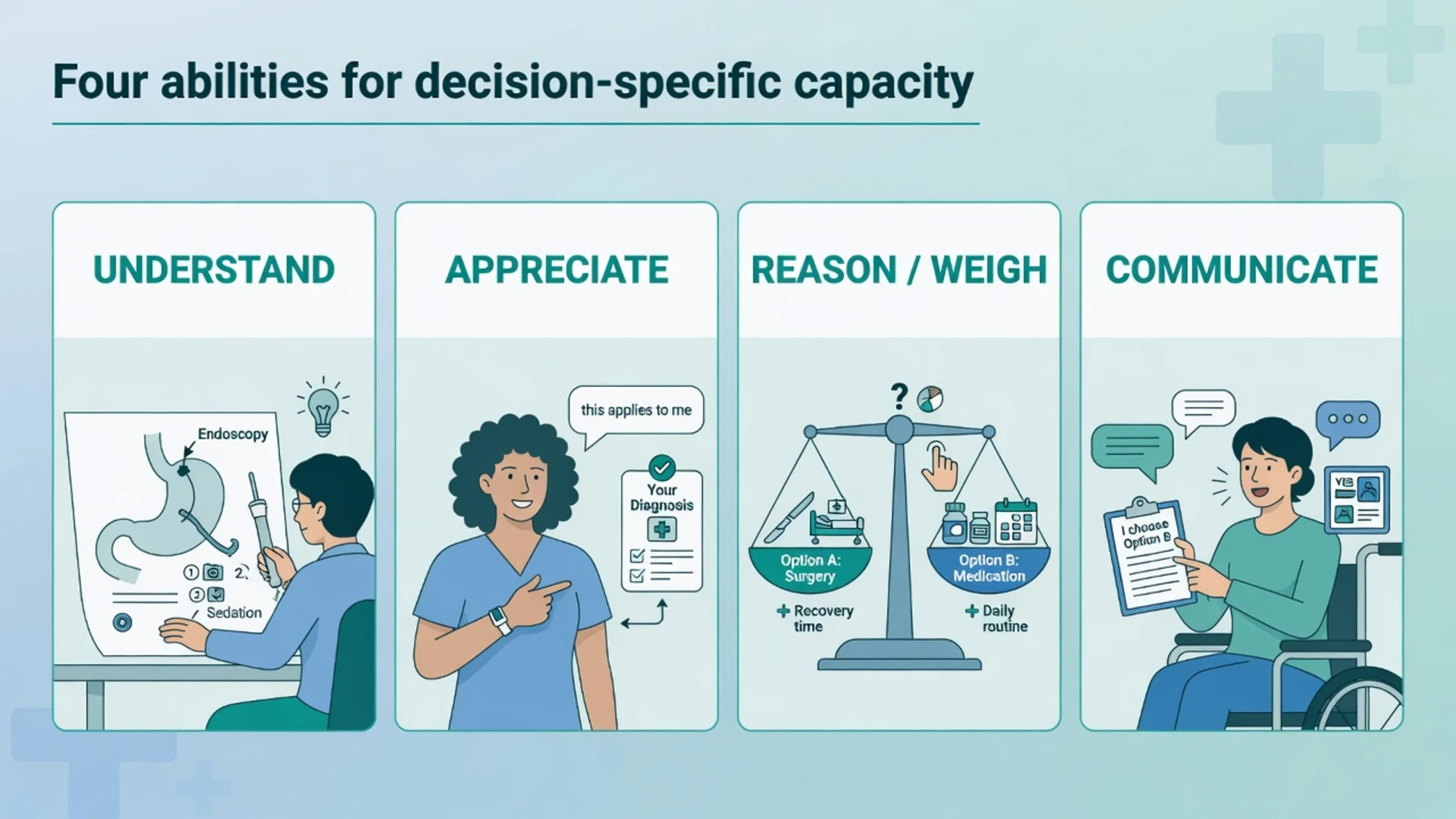
| Ability (Appelbaum/Grisso) | Statute-style wording | ID-adapted bedside probe |
|---|---|---|
| Understand relevant information | Understand / retain | Teach-back with pictures; chunk facts; re-check after a break |
| Appreciate situation and consequences | Apply information to self | "What will happen to you if we do this / do nothing?" |
| Reason about options | Use or weigh | Compare two concrete options with pros/cons cards |
| Express a choice | Communicate | Any reliable modality; check stability across time |
Empirical work shows many adults with mild or moderate ID can achieve health-care and research consent capacity scores comparable to comparison groups when information is accessible — group averages do not justify individual incapacity conclusions.[7][8]
UNCRPD Article 12 and the capacity debate
Article 12 of the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) requires States to recognise that persons with disabilities enjoy legal capacity on an equal basis with others, to provide access to the support they may require in exercising legal capacity, and to implement safeguards against abuse that respect rights, will, and preferences.[10][12]
Exam-level points candidates must hold simultaneously:[10][12]
- Legal capacity is not a clinical score — it is legal agency and equal recognition before the law.[10][17]
- Clinical mental capacity assessment remains embedded in many domestic consent and guardianship systems; it is decision-specific and functional.[2][5]
- There is an ongoing scholarly and policy tension between abolitionist readings of Article 12 (replace all substitute regimes with SDM) and hybrid models that retain a carefully limited functional threshold while maximising supports and will-and-preferences guidance.[12][17]
- In clinical viva answers, state the tension honestly; describe what you do at the bedside (supports first, least restrictive lawful pathway); do not invent how your jurisdiction "implements Article 12 section X".[2][12]
Will and preferences language from CRPD debates reshapes how clinicians frame best interests: the goal is not clinician paternalism, but reconstructing what the person would want, including past expressions, relationships, and values — especially vital for people with severe or profound ID who communicate non-verbally.[12][15]
Epidemiology and clinical burden
People with ID remain over-represented in substitute decision systems historically, partly from status-based assumptions rather than careful functional assessment. Primary-care consensus guidance emphasises promoting participation in health decisions and supported approaches as routine, not exceptional.[13][14]
Research consent and healthcare decision studies show heterogeneity: many with mild ID retain capacity for concrete health decisions; deficits increase with complexity of information and with more severe cognitive impairment — still person-by-person, decision-by-decision.[7][8]
Mechanisms — why demonstration of capacity fails
Intellectual disability affects reasoning speed, working memory, abstract thinking, literacy, and sometimes social judgment — domains that map onto understanding, retention, and weighing. That mapping explains risk, not automatic failure.[6][7]
Common reversible barriers mistaken for incapacity include communication mismatch (complex medical jargon, no Easy Read), unaddressed sensory impairment, anxiety in unfamiliar settings, pain, delirium, post-ictal confusion, sedating medicines, psychiatric comorbidity impairing appreciation, and suggestibility or quiet assent after a lifetime of compliance training.[4][6][13]
Clinical presentation (ID psychiatry stems)
Typical referrals include elective surgery consent, psychotropic start/stop, residential placement or hospital discharge destination, dental general anaesthetic, contraception decisions (historically high abuse risk), research enrolment, family requests for a "global incapacity letter", and transition from paediatric services where parents still speak for an adult.[2][7][13]
Examiner stems commonly feature quiet assent without understanding, capable unwise refusal that must be respected after supports, capable agreement after teach-back, non-verbal persons communicating via AAC or consistent behavioural expression, and fluctuating capacity across acute illness.[2][13][15]
Differential and discriminators
- Understands with Easy Read
- Applies to self
- Weighs and chooses
- May still refuse unwisely
- Fails ability despite adapted disclosure
- Document supports tried
- Emergency / delay / limited substitute
- Need for AAC/interpreter
- Lack of education (teach first)
- Coercion by carer
- Disagreement with family
Capacity for treatment is not fitness to plead, not testamentary capacity, and not automatic co-extension across finance, sex, and housing domains.[5]
Bedside assessment method
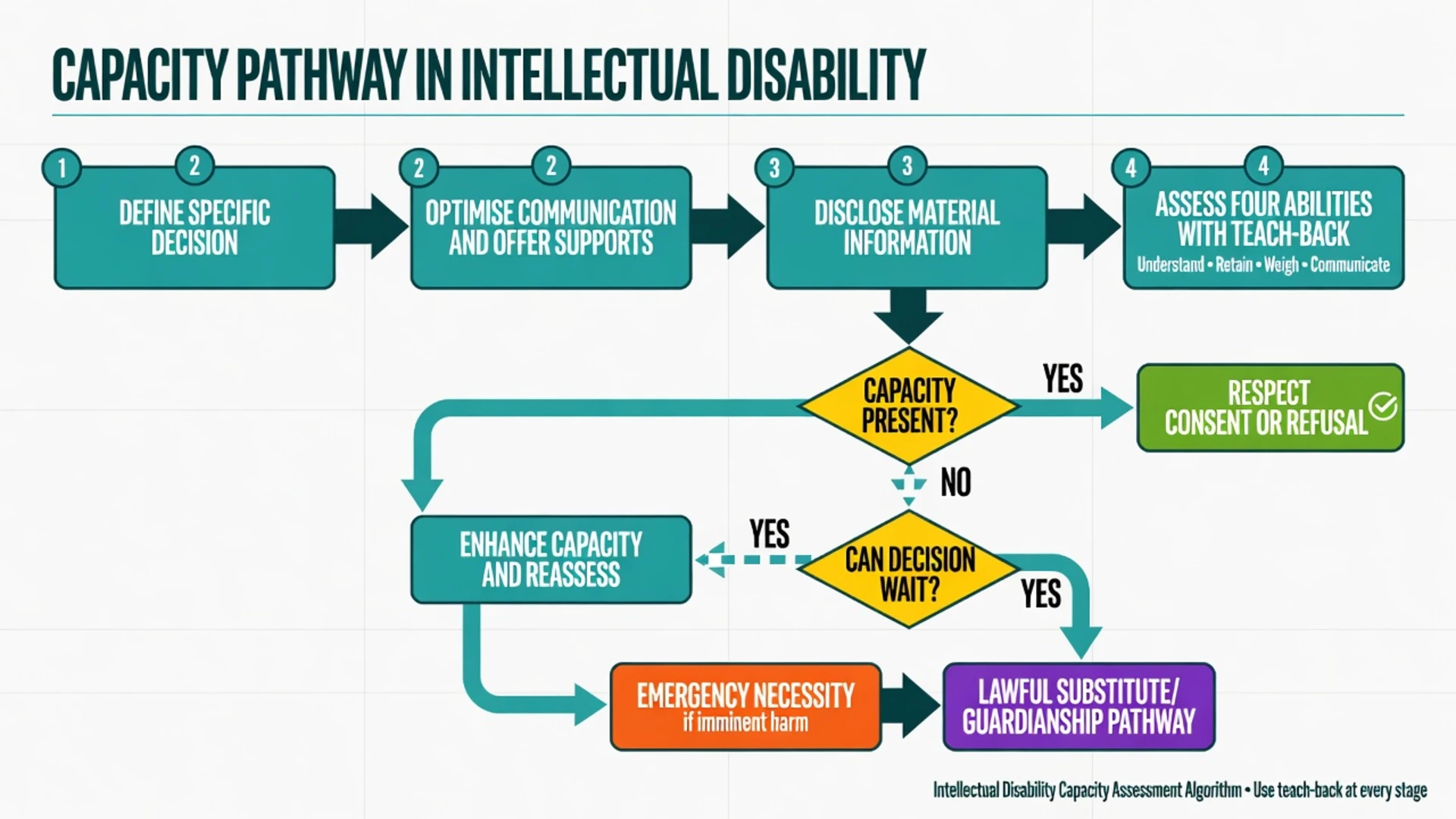
Practical sequence
- Name the decision precisely ("consent for laparoscopic cholecystectomy this admission", not "medical decisions").
- Talk to the person first — not only the carer. Seat supporters to the side; stop them answering for the person.
- Optimise communication — quiet room, glasses/hearing aids, Easy Read or pictorial aids, plain language, one idea at a time, extra time, return visit if needed.
- Disclose material information — condition, proposed intervention, benefits, material risks, alternatives including doing nothing.
- Probe each ability with teach-back and open questions; avoid yes/no-only formats that inflate apparent understanding.
- Assess voluntariness — pressure from family, service providers, or fear of losing support.
- Conclude for this decision at this time; plan review; document supports offered and ability findings with quotes.[2][4][13]
Tools
The MacCAT-T operationalises understanding, appreciation, reasoning, and expressing a choice; it structures interviews but is not a legal verdict and may need adaptation for literacy and communication profile.[3][6] Cognitive screens and IQ scores correlate imperfectly with capacity — adjuncts at most.[4][6] Supported Decision Making inventory work operationalises support needs and environments for some service contexts but does not replace clinical judgment for a specific health decision.[18]
Canadian IDD primary-care consensus materials emphasise promoting decision-making capabilities and accommodating assessment so people can demonstrate residual capacity.[13][14]
SUPPORTS
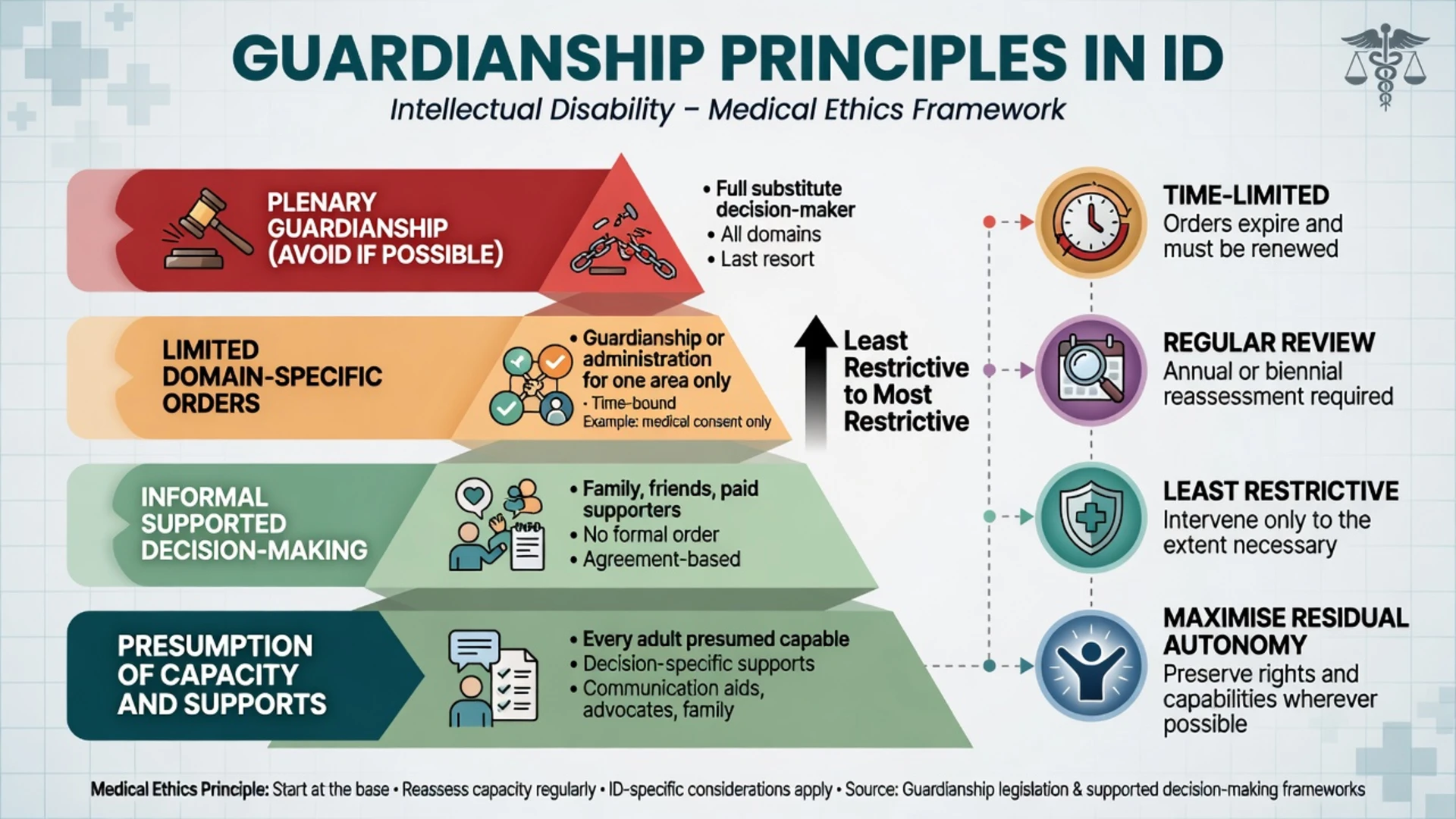
Guardianship principles (exam-level, jurisdiction-agnostic)
When substitute authority is required, contemporary principles (names of tribunals and Acts vary) converge on least-restrictive practice, limited domain, time-limited orders, residual autonomy, will-and-preferences guidance, and safeguards against conflict of interest.[10][11][12][17]
| Principle | Practical meaning |
|---|---|
| Least restrictive | Prefer informal supports and limited orders over plenary guardianship |
| Limited domain | Healthcare authority is not automatically financial or residential authority |
| Time-limited | Fixed review; restore rights when no longer needed |
| Residual autonomy | Maximise decisions the person can still make |
| Will and preferences | Guide substitute decisions by known wishes where possible |
| Safeguards | Conflict-of-interest checks; independent review pathways |
Do not invent section numbers. In exams, say: "under local guardianship / consent legislation" and describe principles. In clinical practice, name your local Act accurately after checking it.[5]
When capacity is absent after supports
Branching options
| Path | When | Principles |
|---|---|---|
| Emergency treatment | Immediate serious harm; cannot wait | Necessity / statutory emergency powers; document; least needed |
| Delay and enhance | Decision can wait | Treat reversible causes; educate; SDM training; reassess |
| Limited substitute / guardianship | Capacity absent; decision needed | Lawful process; limited domain; will and preferences; review |
| Mental health pathway | Separate statutory criteria for compulsory psychiatric care | Does not auto-authorise all medical procedures |
For people with severe or profound ID, end-of-life and major treatment decisions often rely on relational knowledge of past preferences, behavioural cues, and close supporters — still person-centred, not clinician-only best interests by convenience.[15] Training carers and parents in decision-support skills can shift language from "non-decision-maker" to genuine support practice.[16]
Research consent deserves a goodness-of-fit ethic: adapt procedures to the person's communication and decision style rather than forcing a single consent script that only the least impaired can pass.[9]
Mental health law vs capacity / guardianship
Compulsory psychiatric treatment pathways (jurisdiction-specific mental health legislation) turn on mental disorder plus risk or equivalent criteria and least-restrictive principles. General medical consent usually follows capacity/guardianship frameworks. A person with ID under a mental health order may still have capacity for a medical procedure — or may lack it and need a separate substitute pathway. Never invent section numbers.[2][5]
Special populations and scenarios
Mild ID. Often retains capacity for concrete health decisions after accessible disclosure; risk is under-support and over-substitution by families.[7][8]
Moderate ID. Heterogeneous; invest in multi-session education and pictorial comparison of options.[7][13]
Severe/profound ID. High support needs; SDM becomes highly relational; document how will and preferences were reconstructed.[15]
Autism + ID. Literal language, concrete examples, and sensory environment control matter; do not equate flat affect or echolalia with incapacity.[2][13]
Transition to adult services. Parents may assume ongoing automatic authority. Adult law applies; parents may become supporters or lawful substitutes only under local rules.[13]
Ageing with ID / Down syndrome dementia. Capacity can decline domain-by-domain; reassess longitudinally; avoid global labels.[6][13]
Sexual relationships and sterilisation history. Decision-specific capacity with heightened ethical scrutiny given historical abuse; support autonomy and protection from exploitation simultaneously.[5][10]
Indigenous and CALD persons with ID. Use cultural safety, appropriate interpreters (not child family interpreters by default), and community supports rather than deficit framing.[2][13]
Documentation standard
Write: decision defined; information disclosed (key points and format used); supports offered; findings for each ability with quotes or observed communication; voluntariness; conclusion (capacity present/absent for this decision at this time); pathway chosen; review plan; people present and their roles (supporter vs decision-maker).[2][4][13]
Pitfalls
- ID diagnosis or IQ as global incapacity
- Skipping supports then concluding incapacity
- Outcome bias (refusal = incapacity)
- Quiet assent without teach-back
- Family preference mistaken for the person's will
- Plenary guardianship for convenience
- Supporter with unexamined conflict of interest
- Conflating mental health compulsory powers with general medical authority
- Inventing statute sections in exam answers
- Diagnostic overshadowing of treatable mental illness impairing capacity
Prognosis and disposition
Capacity often improves with education, experience, recovery from acute illness, pain control, and carer training in decision support.[13][16] Plan reassessment windows and rights restoration. Disposition is an explicit formulation: respect autonomous decision; continue SDM; limited substitute order; emergency treatment; or separate mental health pathway when criteria are met for psychiatric care.[2][12]
CASC and communication skills
- Introduce yourself to the person first; ask how they communicate best.
- Use short sentences, one idea at a time, pictures if available.
- Teach-back without humiliation: "Can you tell me in your own words what the doctors want to do?"
- Invite the supporter to help after the person has tried, not instead of them.
- Explore refusal with curiosity; separate fear, past trauma in hospitals, and true weighing.
- Explain limited guardianship vs support to families in plain language without invented sections.
- Close with a clear plan and review time.
Exam pearls
References
- [1]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [2]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [3]Grisso T, Appelbaum PS, Hill-Fotouhi C The MacCAT-T: a clinical tool to assess patients' capacities to make treatment decisions Psychiatr Serv, 1997.PMID 9355168
- [4]Sessums LL, Zembrzuska H, Jackson JL Does this patient have medical decision-making capacity? JAMA, 2011.PMID 21791691
- [5]Buchanan A Mental capacity, legal competence and consent to treatment J R Soc Med, 2004.PMID 15340019
- [6]Palmer BW, Harmell AL Assessment of Healthcare Decision-making Capacity Arch Clin Neuropsychol, 2016.PMID 27551024
- [7]Cea CD, Fisher CB Health care decision-making by adults with mental retardation Ment Retard, 2003.PMID 12622524
- [8]Fisher CB, Cea CD, Davidson PW, Fried AL Capacity of persons with mental retardation to consent to participate in randomized clinical trials Am J Psychiatry, 2006.PMID 17012694
- [9]Fisher CB Goodness-of-fit ethic for informed consent to research involving adults with mental retardation and developmental disabilities Ment Retard Dev Disabil Res Rev, 2003.PMID 12587135
- [10]Werner S Supported decision-making and personal autonomy for persons with intellectual disabilities: article 12 of the UN convention on the rights of persons with disabilities J Law Med Ethics, 2013.PMID 24446938
- [11]Kohn NA, Blumenthal JA A critical assessment of supported decision-making for persons aging with intellectual disabilities Disabil Health J, 2014.PMID 24456684
- [12]Szmukler G "Capacity", "best interests", "will and preferences" and the UN Convention on the Rights of Persons with Disabilities World Psychiatry, 2019.PMID 30600630
- [13]Sullivan WF, Heng J, Bach M, et al. Supporting adults with intellectual and developmental disabilities to participate in health care decision making Can Fam Physician, 2018.PMID 29650742
- [14]Sullivan WF, Diepstra H, Heng J, et al. Primary care of adults with intellectual and developmental disabilities: 2018 Canadian consensus guidelines Can Fam Physician, 2018.PMID 29650602
- [15]Watson J, Wilson E, Hagiliassis N Supporting end of life decision making: Case studies of relational closeness in supported decision making for people with severe or profound intellectual disability J Appl Res Intellect Disabil, 2017.PMID 28815814
- [16]Bigby C, Douglas J, Smith E, et al. "I used to call him a non-decision-maker - I never do that anymore": parental reflections about training to support decision-making of their adult offspring with intellectual disabilities Res Dev Disabil, 2022.PMID 34477481
- [17]Series L Getting the Balance Right: Conceptual Considerations Concerning Legal Capacity and Supported Decision-Making Int J Law Psychiatry, 2016.PMID 27329177
- [18]Shogren KA, Wehmeyer ML, Uyanik H, Heidrich M Development of the Supported Decision Making Inventory System Intellect Dev Disabil, 2017.PMID 29194029