Psych · Intellectual disability psychiatry
Challenging behaviour and positive behaviour support
Also known as Behaviours that challenge · Behaviour of concern · Problem behaviour · Positive behavioural support · PBS · Functional behaviour assessment · Challenging behavior intellectual disability
Exam-exhaustive fellowship reference on challenging behaviour in intellectual disability — Emerson definition and epidemiology, functional analysis (attention, escape, tangible, automatic), positive behaviour support multicomponent framework, medical and psychiatric differentials, NICE NG11, limited antipsychotic role (Tyrer 2008), deprescribing and STOMP principles, capacity and restrictive practices. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
1 MCQ with explanations
Target exams
Red flags
Challenging behaviour (CB) is one of the highest-yield intellectual disability (ID) psychiatry interfaces in FRANZCP, MRCPsych and related boards. Examiners test whether you reflexively sedate, or whether you can formulate function, exclude medical and psychiatric drivers, implement positive behaviour support (PBS), and use medicines with eyes open to overprescribing data and deprescribing evidence.[1][4][5]
Overview and definition
Emerson’s widely taught definition frames challenging behaviour as culturally abnormal behaviour of such intensity, frequency or duration that the physical safety of the person or others is likely to be placed in serious jeopardy, or behaviour which is likely to seriously limit use of ordinary community facilities. CB is therefore defined by impact and context, not by a single topography.[2]
Critical exam distinction. Challenging behaviour is not a DSM-5-TR or ICD-11 diagnosis. It is a clinical and service description that may be maintained by environmental contingencies, driven by untreated pain or mental illness, amplified by autism or communication barriers, or some combination. Treating “behaviour” as if it were schizophrenia is the classic fellowship trap.[1][11]
Related language includes behaviours that challenge (UK), behaviours of concern, and problem behaviour. Modern practice emphasises rights, quality of life and reduction of restrictive practices, not suppression of the person.[1]
Classification: topography versus function
Common topographies
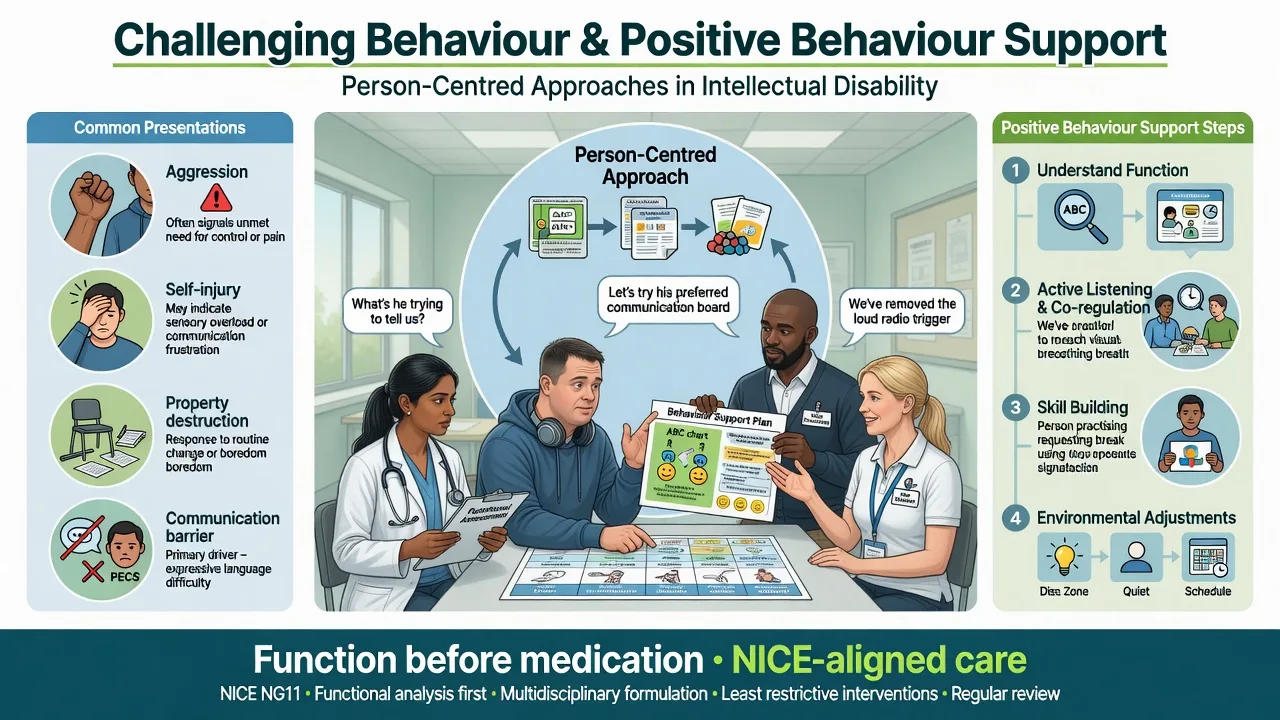
Common topographies include aggression toward people or property; self-injurious behaviour (SIB) such as head-banging, biting, hitting or eye-poking; severe stereotypy causing injury or exclusion; sexualised behaviour in public or non-consensual contexts; and high-risk subsets such as absconding, PICA, faecal smearing or fire-setting. Severity is rated by frequency, intensity, injury risk, and impact on placement, relationships and community access — not by moral judgment.[1][2]
Functional classes (must be exam-ready)
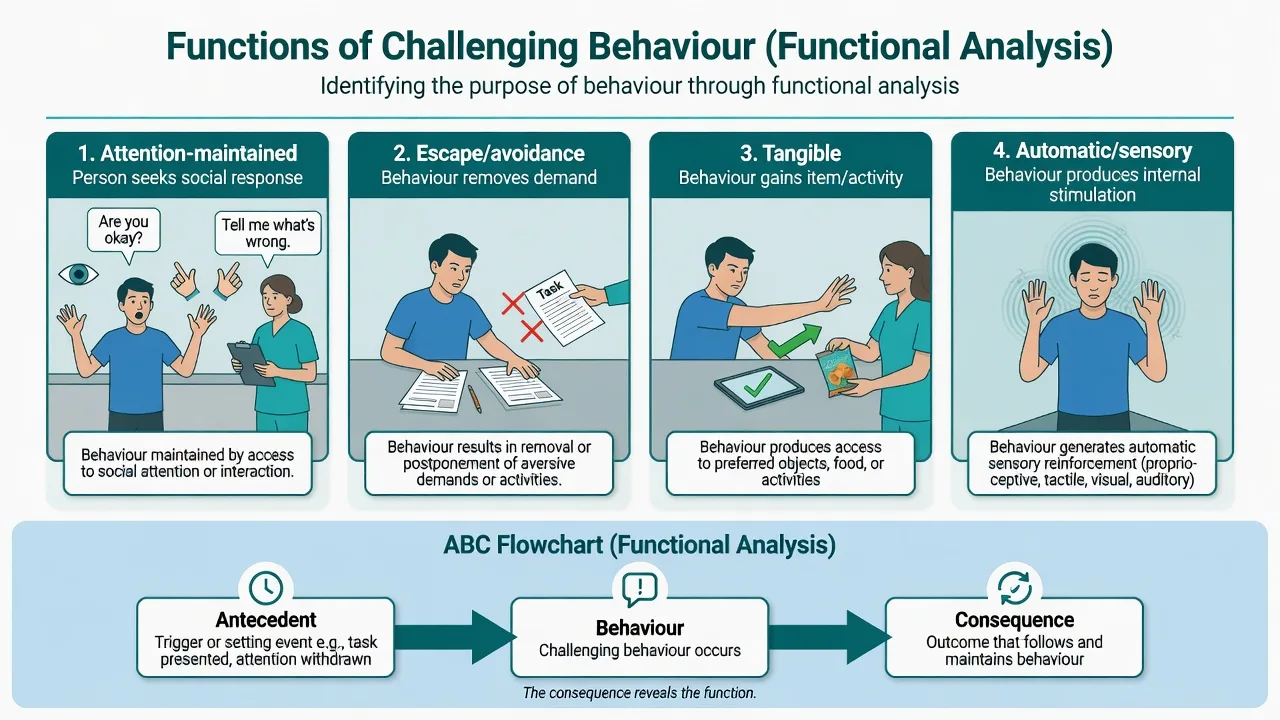
Classic experimental functional analysis (Iwata framework for self-injury, extended broadly) tests whether problem behaviour is more likely under conditions that deliver attention (social positive reinforcement), escape/avoidance of demand or aversive tasks (negative reinforcement), tangible access to preferred items or activities, or automatic/sensory reinforcement (behaviour persists when alone; not socially mediated). Descriptive tools use ABC charts (Antecedent–Behaviour–Consequence) across settings; interviews and rating tools (e.g. QABF-type approaches conceptually) generate hypotheses that PBS plans then test in real life.[6]
Epidemiology and risk
Headline epidemiology for viva recall
In a total-population study, Emerson and colleagues estimated that challenging behaviours were shown by roughly 10–15% of people with intellectual disability in contact with educational, health or social care services — a figure still used as the viva order-of-magnitude anchor, with higher rates in more severe disability and congregate settings.[2]
Risk markers. Severity of ID; limited expressive communication; autism spectrum co-occurrence; sensory impairment; epilepsy; certain genetic behavioural phenotypes; institutional or poorly matched environments; high staff turnover; and carer stress with skill–demand mismatch.[1][2]
Prescribing epidemiology. In UK primary care cohort data, recorded psychotropic prescribing substantially exceeded recorded mental illness among people with intellectual disability — a policy and exam pearl driving STOMP-style campaigns against overmedication for behaviour alone.[4]
Pathophysiology and maintaining mechanisms
Examiners want a biopsychosocial-operant model, not a single neurotransmitter slogan.[1][6]
Operant maintenance. Behaviour that is followed by attention, escape, or preferred items is strengthened. Automatic SIB may be maintained by sensory consequences. Intervention that ignores function (e.g. time-out for escape-maintained behaviour that actually removes the demand) can worsen the behaviour.[6]
Communication and unmet need. When speech or AAC is limited, aggression or SIB may be the most efficient way to refuse, request, or protest. Teaching a functionally equivalent communicative response is often more powerful than sedation.[1][15]
Medical drivers. Pain (dental, musculoskeletal, constipation, urinary retention, otitis, reflux), infection, peri-ictal states, sleep deprivation, and adverse drug effects (especially akathisia) convert a stable person into a crisis overnight.[1][11]
Psychiatric drivers. Depression, anxiety, PTSD, psychosis and ADHD can present as “behaviour” when history-taking is thin. Dual diagnosis is allowed when criteria are met; diagnostic overshadowing cuts both ways — do not miss mental illness, and do not invent psychosis to justify an antipsychotic for escape-maintained aggression.[1][4][11]
Clinical presentation
Presentations are setting-dependent. Aggression during personal care often signals pain, sensory aversion, or escape from demand. SIB that peaks when alone suggests automatic function. Property destruction when preferred items are denied suggests tangible maintenance. Document frequency, intensity, duration, injury, and staff response — the consequence side of ABC is where accidental reinforcement lives.[6]
MSE adaptations. Rely on observation relative to baseline, multi-setting collateral (family, day service, residential staff), and communication method (gesture, AAC, interpreter). Note affect change, sleep, appetite, new psychosis-like content, and trauma cues. Capacity is decision-specific with supported decision-making.[1][11]
Differential diagnosis
Medical / pain
- New change in behaviour is medical until proven otherwise
- Dental disease, constipation, UTI, fracture, reflux
- Epilepsy peri-ictal or post-ictal states
- Akathisia from antipsychotics misread as agitation
Mental illness
- Depression: withdrawal, tearfulness, self-harm change
- Psychosis: new fixed false beliefs, hallucinations
- PTSD / trauma-related escalation
- Treat when criteria met — do not overshadow
Neurodevelopmental
- Autism meltdown vs operant aggression (may coexist)
- ADHD impulsivity with ID
- Sensory overload in noisy settings
- Skill deficit not 'non-compliance'
Environmental / abuse
- Under/overstimulation, chaotic staffing
- Inconsistent boundaries and reinforcement
- Neglect, exploitation, sexual abuse
- Placement mismatch and boredom
Also consider substance intoxication/withdrawal in community adults, and intentionality carefully in forensic dual-disability settings without discarding functional analysis.[1]
Bedside assessment
History structure. Onset and course; topographies; high-risk times and places; communication level; sleep and pain clues; current and past psychotropics with indication; restrictive practices used; prior PBS or psychology input; carer goals and safety.[1]
Functional behaviour assessment (FBA) proceeds from indirect methods (structured interviews with multiple informants), to descriptive ABC recording across settings and staff, and when safe and specialist-supported to experimental functional analysis testing attention, demand, alone and play/control conditions (Iwata-type methodology).[6]
Risk. Harm to self/others; sexual risk; fire and traffic; carer injury; placement breakdown; safeguarding (adults at risk / child protection as age-appropriate). Legal status uses least restrictive local Mental Health, Guardianship or disability frameworks — do not invent section numbers in exams; state principles.[1][11]
Investigations
There is no “challenging behaviour panel.” Investigate to answer a clinical question.[1]
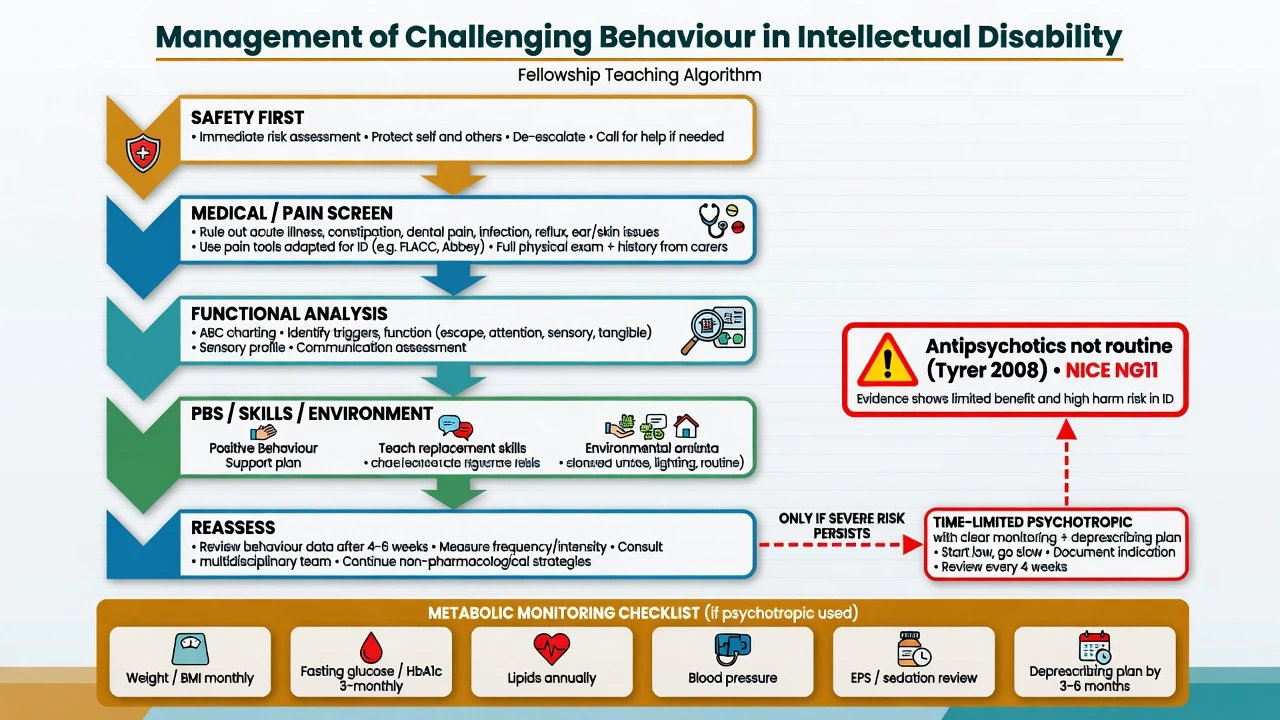
When behaviour is new or changed: vital signs; focused pain exam including dental and abdomen; constipation and urinary retention; urinalysis as indicated; basic bloods when systemic illness suspected; medication reconciliation. EEG or imaging only with neurological red flags (seizures, regression atypical for the person, focal signs) — not for chronic function-maintained CB.[1][11]
Before any antipsychotic trial: weight/BMI, blood pressure, fasting glucose and lipids as baseline, EPS examination, consider prolactin risk with risperidone, and ECG when cardiac risk or QTc-prolonging polypharmacy is present.[11]
Acute management (safety)
Definitive management — PBS first
Positive behaviour support
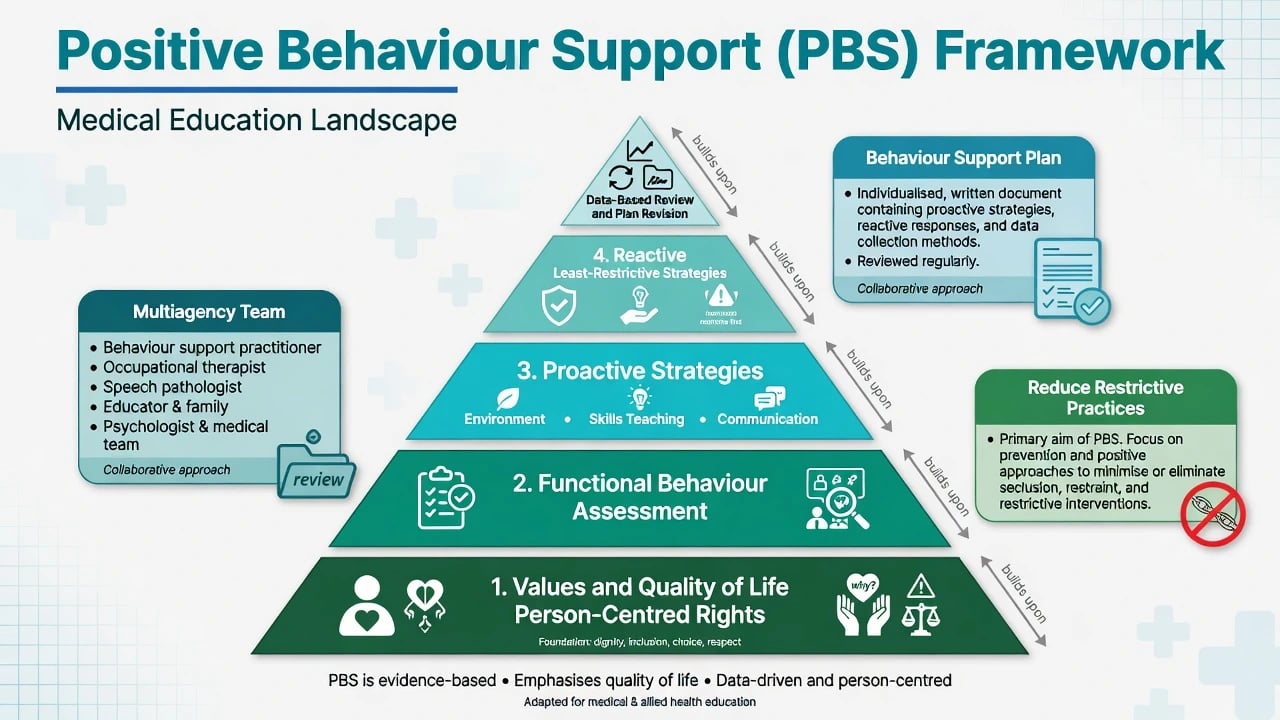
PBS is a multicomponent, values-based framework derived from applied behaviour analysis and disability rights principles. Core elements examiners expect are person-centred quality of life goals (not mere suppression); functional assessment driving the plan; proactive strategies (environmental redesign, predictable routines, skill teaching, functional communication training, active support); reactive strategies that are least restrictive and pre-planned; data-based review with multiagency ownership (health, disability support, education, family); and an explicit aim to reduce restrictive practices.[1][15]
PBS is not a single psychology session or a laminated poster. Fidelity of staff training and implementation determines outcome. A large cluster randomised trial of staff PBS training in adult services (Hassiotis et al.) did not show superiority on primary challenging-behaviour outcomes versus treatment as usual, with important caveats about implementation fidelity — cite this honestly rather than claiming universal trial superiority of generic training packages. Systematic reviews in education and disability settings still support PBS components when function-matched and well delivered.[9][10][15]
Adapted psychological therapies
For people with mild to moderate ID and anger-related aggression, group-based cognitive-behavioural anger management improved anger control in a cluster RCT (Willner et al.) — useful when cognitive access allows adapted CBT, not as a substitute for environmental PBS in profound ID.[12]
Guideline-aligned principles (NICE NG11 and international guides)
Contemporary UK and international guidance for people with learning disabilities whose behaviour challenges emphasises early identification of risk, personalised assessment including functional analysis, psychosocial and environmental interventions as first-line, parent/carer and staff training, and limited, carefully reviewed medication only when behaviour poses serious risk and non-drug approaches are insufficient or while behavioural programmes are being established. Regular review for reduction and discontinuation is expected — principles aligned with WPA Section on Psychiatry of Intellectual Disability prescribing guidance and UK NICE NG11 teaching for exams.[1][3][11]
Australia/NZ practice note. Behavioural approaches remain first-line. Trollor and colleagues emphasise that psychological and behavioural management is usually preferable to psychotropics for challenging behaviour, with medicines reserved for severe, persistent risk after non-drug optimisation, clear targets, and monitoring. NDIS Quality and Safeguards Commission rules on behaviour support and restrictive practices (chemical, mechanical, physical, seclusion, environmental) are high-yield for Australian practice stations — chemical restraint includes medicines used primarily to control behaviour, not treat a diagnosed condition.[11]
Limited role of antipsychotics
This is the highest-yield pharmacotherapy pearl on the topic: antipsychotics are not routine first-line treatment for non-psychotic challenging behaviour in adults with intellectual disability.[1][3]
Adults with ID and aggressive challenging behaviour without clear psychosis. The Tyrer et al. multicentre RCT compared risperidone, haloperidol and placebo: antipsychotics were not more effective than placebo for aggressive challenging behaviour, and the authors concluded they should no longer be regarded as acceptable routine treatment in this indication.[3]
Prescribing reality vs evidence. Despite weak indication for non-psychotic CB, antipsychotics are widely used; cohort data show psychotropic exposure far exceeding recorded mental illness, implying substantial off-label behavioural use.[4]
Deprescribing is feasible and recommended. Systematic review of reduction or discontinuation of antipsychotics for CB in adults with ID supports carefully supervised taper with multiagency behavioural support; many people can reduce or stop without catastrophic behavioural rebound when support is adequate. Barriers include staff anxiety about restlessness and autism-related concerns — address these with PBS, not automatic dose escalation.[5][13]
When paediatric/ASD trial data apply — and when they do not. Risperidone has RCT support for severe disruptive behaviour in children with subaverage IQ (Aman; Snyder) and for irritability in autistic children (RUPP/McCracken). Do not uncritically transplant those paediatric indications and dose schedules onto adults with non-psychotic CB and no autism-related irritability formulation. Population, indication and monitoring differ.[7][8][14]
If a time-limited antipsychotic is justified after PBS and medical optimisation (document residual severe risk of injury, failed or concurrent intensive behavioural plan, capacity/consent process), use a named target symptom and risk (not vague “behaviour”); start low if choosing risperidone in sensitive adults with ID (illustrative oral start 0.25–0.5 mg daily, individualise for frailty, epilepsy and interactions); titrate slowly to the lowest effective dose; avoid polypharmacy cocktails; monitor weight/BMI, glucose, lipids, EPS, sedation, prolactin symptoms, falls and ECG when indicated; set a time-limited trial with pre-agreed review and a deprescribing plan; stop if there is no meaningful risk reduction, intolerability, or once function-based PBS succeeds.[3][5][7][11]
Subtypes and scenarios
Severe SIB in profound ID. Prioritise medical pain screen, automatic versus social function, protective equipment only as least-restrictive interim, intensive PBS and communication systems; medicines alone rarely fix automatic SIB.[1][6]
Autism + ID. Sensory load, insistence on sameness, and communication barriers dominate. Irritability pharmacotherapy evidence is stronger in autistic children than in non-autistic adults with CB — still formulate first.[8]
Placement breakdown. Multiagency crisis plan, temporary increased support, urgent FBA, medication rationalisation rather than stacking doses.[1]
Long-term “behaviour antipsychotic”. Audit indication; if no mental illness and risk is controlled, plan gradual taper with enhanced PBS and staff education.[5][13]
Complications and pitfalls
- Diagnostic overshadowing of pain, depression, psychosis and abuse
- Chemical restraint without functional analysis or consent process
- Metabolic syndrome, tardive dyskinesia, prolactin effects, sedation and falls from chronic antipsychotics
- Function-mismatched interventions that reinforce CB
- High restrictive-practice culture without rights-based review
- Blaming the person rather than redesigning the environment and skill supports
Prognosis and disposition
CB can reduce substantially when function is correctly identified and PBS is implemented with environmental redesign and communication teaching. Persistence is more likely with profound communication barriers, untreated medical illness, chaotic staffing, and ongoing inadvertent reinforcement. Disposition needs a written behaviour support plan, crisis plan, medication review dates, and clear multiagency ownership — placement stability is a legitimate outcome metric.[1][15]
Special populations
Children. Educational PBS and parent training are central; specialist CAMHS-ID pathways; paediatric risperidone evidence for severe disruptive behaviour exists but still requires behavioural formulation and metabolic monitoring.[7][14][15]
Older adults with ID. Premature ageing, sensory loss, pain, and dementia interfaces increase CB; lower medication thresholds for harm; deprescribe aggressively when possible.[11]
Forensic dual disability. Risk assessment, capacity, and offence-paralleling behaviour formulation sit alongside PBS; do not abandon functional analysis in secure settings.[1]
Cultural safety. Family explanatory models, language access, and Indigenous community supports must shape PBS goals — “compliance” without cultural fit is not success.[1]
Evidence and guidelines summary
Deb/WPA international prescribing guide and NICE NG11-style teaching share the exam take-home: psychosocial first, medication limited and reviewed. Emerson 2001 supplies the ~10–15% prevalence order of magnitude; Iwata 1994 anchors functional analysis; Tyrer 2008 shows risperidone/haloperidol not superior to placebo for aggressive CB in adult ID; Sheehan BMJ 2015 documents psychotropics exceeding recorded mental illness; Sheehan and Hassiotis 2017 support deprescribing; Aman/Snyder and RUPP address paediatric disruptive behaviour or autistic irritability rather than routine adult non-psychotic CB; Hassiotis 2018 cautions that staff PBS training fidelity matters; Willner 2013 supports adapted anger CBT in mild–moderate ID; Trollor 2016 frames ANZ behavioural-first prescribing.[1][2][3][4][5][6][7][8][9][11][12]
Exam pearls
- Challenging behaviour is a description, not a diagnosis
- Always name function (attention / escape / tangible / automatic) before a drug
- Pain and constipation before risperidone
- Tyrer 2008: antipsychotics not routine for aggressive CB in adults with ID
- Sheehan 2015: psychotropics exceed recorded mental illness — overmedication is real
- NICE NG11 / Deb guide: PBS/psychosocial first; medicine time-limited with review
- PBS without implementation fidelity is paperwork, not treatment
- Capacity is decision-specific; support decision-making; least restrictive care
- Document indication, monitoring, and deprescribing date whenever an antipsychotic is used for CB
References
- [1]Deb S, Kwok H, Bertelli M, et al.; Guideline Development Group of the WPA Section on Psychiatry of Intellectual Disability International guide to prescribing psychotropic medication for the management of problem behaviours in adults with intellectual disabilities World Psychiatry, 2009.PMID 19812757
- [2]Emerson E, Kiernan C, Alborz A, et al. The prevalence of challenging behaviors: a total population study Res Dev Disabil, 2001.PMID 11263632
- [3]Tyrer P, Oliver-Africano PC, Ahmed Z, et al. Risperidone, haloperidol, and placebo in the treatment of aggressive challenging behaviour in patients with intellectual disability: a randomised controlled trial Lancet, 2008.PMID 18177776
- [4]Sheehan R, Hassiotis A, Walters K, et al. Mental illness, challenging behaviour, and psychotropic drug prescribing in people with intellectual disability: UK population based cohort study BMJ, 2015.PMID 26330451
- [5]Sheehan R, Hassiotis A Reduction or discontinuation of antipsychotics for challenging behaviour in adults with intellectual disability: a systematic review Lancet Psychiatry, 2017.PMID 27838214
- [6]Iwata BA, Dorsey MF, Slifer KJ, Bauman KE, Richman GS Toward a functional analysis of self-injury J Appl Behav Anal, 1994.PMID 8063622
- [7]Aman MG, De Smedt G, Derivan A, Lyons B, Findling RL; Risperidone Disruptive Behavior Study Group Double-blind, placebo-controlled study of risperidone for the treatment of disruptive behaviors in children with subaverage intelligence Am J Psychiatry, 2002.PMID 12153826
- [8]McCracken JT, McGough J, Shah B, et al.; Research Units on Pediatric Psychopharmacology Autism Network Risperidone in children with autism and serious behavioral problems N Engl J Med, 2002.PMID 12151468
- [9]Hassiotis A, Poppe M, Strydom A, et al. Clinical outcomes of staff training in positive behaviour support to reduce challenging behaviour in adults with intellectual disability: cluster randomised controlled trial Lancet Psychiatry, 2018.PMID 29436314
- [10]Hassiotis A, Poppe M, Strydom A, et al. Positive behaviour support training for staff for treating challenging behaviour in people with intellectual disabilities: a cluster RCT Health Technol Assess, 2018.PMID 29596045
- [11]Trollor JN, Salomon C, Franklin C Prescribing psychotropic drugs to adults with an intellectual disability Aust Prescr, 2016.PMID 27756975
- [12]Willner P, Rose J, Jahoda A, et al. Group-based cognitive-behavioural anger management for people with mild to moderate intellectual disabilities: cluster randomised controlled trial Br J Psychiatry, 2013.PMID 23520220
- [13]de Kuijper GM, Hoekstra PJ Physicians' reasons not to discontinue long-term used off-label antipsychotic drugs in people with intellectual disability J Intellect Disabil Res, 2017.PMID 28560761
- [14]Snyder R, Turgay A, Aman M, Binder C, Fisman S, Carroll A; Risperidone Conduct Study Group Effects of risperidone on conduct and disruptive behavior disorders in children with subaverage IQs J Am Acad Child Adolesc Psychiatry, 2002.PMID 12218423
- [15]Beqiraj L, Denne LD, Hastings RP, Paris A Positive behavioural support for children and young people with developmental disabilities in special education settings: A systematic review J Appl Res Intellect Disabil, 2022.PMID 35199433