Psych · intellectual-disability
Down syndrome and mental health
Also known as Trisomy 21 psychiatry · Down syndrome depression · Down syndrome Alzheimer dementia · DS-AD · Down syndrome mental ill-health · Dementia in Down syndrome · CAMDEX-DS · DSQIID
Exam-exhaustive Down syndrome mental health for FRANZCP and global boards: behavioural phenotype, depression versus Alzheimer dementia, medical confounders, adapted assessment and dementia tools, start-low go-slow psychopharmacology, capacity and dementia-capable services.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
1. Definition and classification
Down syndrome is most often full trisomy 21; rarer mechanisms include Robertsonian translocation and mosaicism. Multi-system features (cardiac, thyroid, ENT/sleep, musculoskeletal, sensory) sit alongside a developmental cognitive profile usually in the mild–moderate intellectual disability range with individual variability.[1]
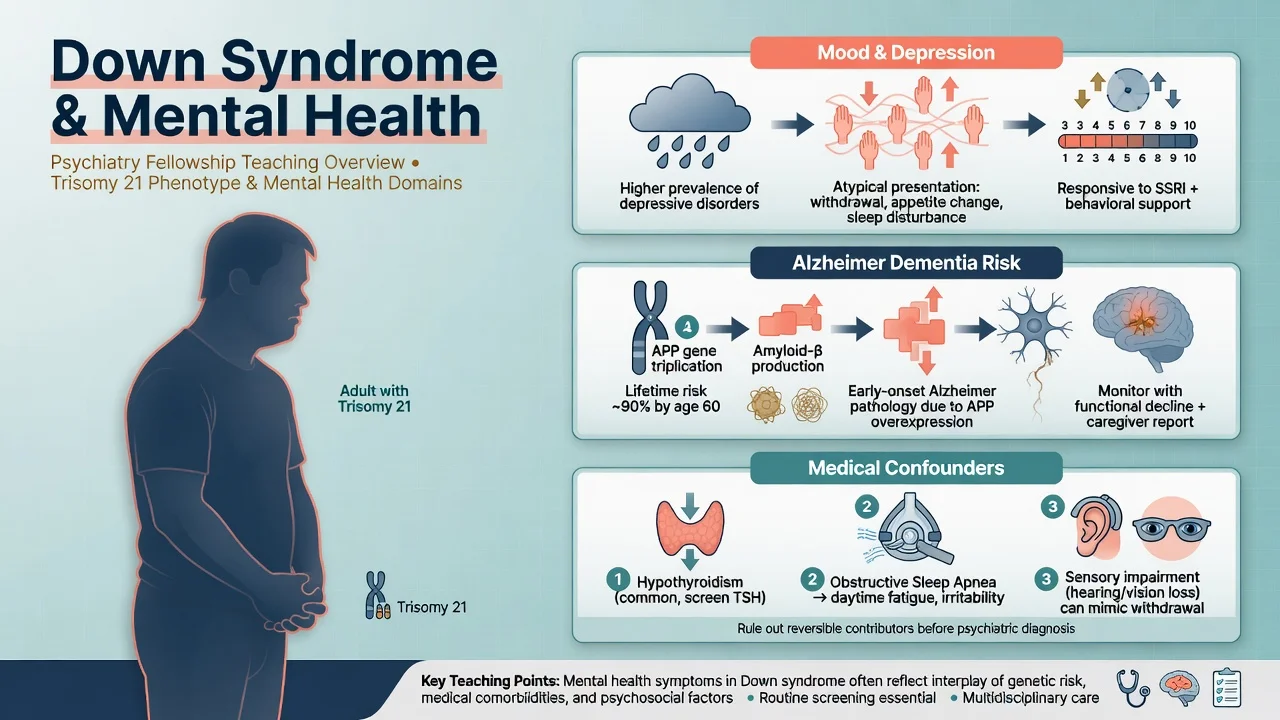
Behavioural phenotype (probabilistic). Dykens’ framework applies: DS confers a heightened probability of particular cognitive and behavioural patterns (often relative social engagement earlier in life; elevated later-life Alzheimer risk; depression and OCD-like behaviours commonly discussed) — not pathognomonic, exclusive, or a substitute for a DSM-5-TR/ICD-11 psychiatric diagnosis.[11][1]
What you still diagnose. Major depressive disorder (or equivalent), Alzheimer-type dementia, anxiety disorders, OCD-related presentations, ASD when criteria met, and delirium when present. The genetic diagnosis informs prior probability, medical surveillance and prognosis, not automatic attribution of every behaviour to “the syndrome”.[7][9]
Neuropathology versus clinical dementia. Almost all adults with DS develop Alzheimer-type neuropathology with age; clinical dementia is a clinical diagnosis based on progressive functional and cognitive decline from the individual’s baseline — not amyloid presence alone.[2][4]
2. Epidemiology and risk
Order-of-magnitude exam numbers
Mental ill-health in adults with DS. Mantry and colleagues showed that the pattern and standardised rates of mental ill-health in adults with DS differ from intellectual disability of all causes; depressive episode and dementia/delirium featured among higher-incidence categories in that population work — useful when examiners ask whether “all ID psychiatry is the same”.[7]
Depression. Classic clinical series (Myers and Pueschel) and later reviews document depressive illness as a major treatable problem; presentation is often behavioural and functional rather than classic verbalised guilt. Prevalence estimates vary by sample and criteria — cite the range concept rather than inventing a single percentage.[8][9]
Dementia. Holland’s population-based study established rising prevalence and characteristic presentations of dementia in adults with DS. Zigman synthesised neurobiology and extreme AD risk. Contemporary multimorbidity data in older adults with DS reinforce high clinical dementia burden; Fortea’s biomarker work places DS on an Alzheimer continuum with ordered biomarker change.[2][3][4][12]
3. Pathophysiology
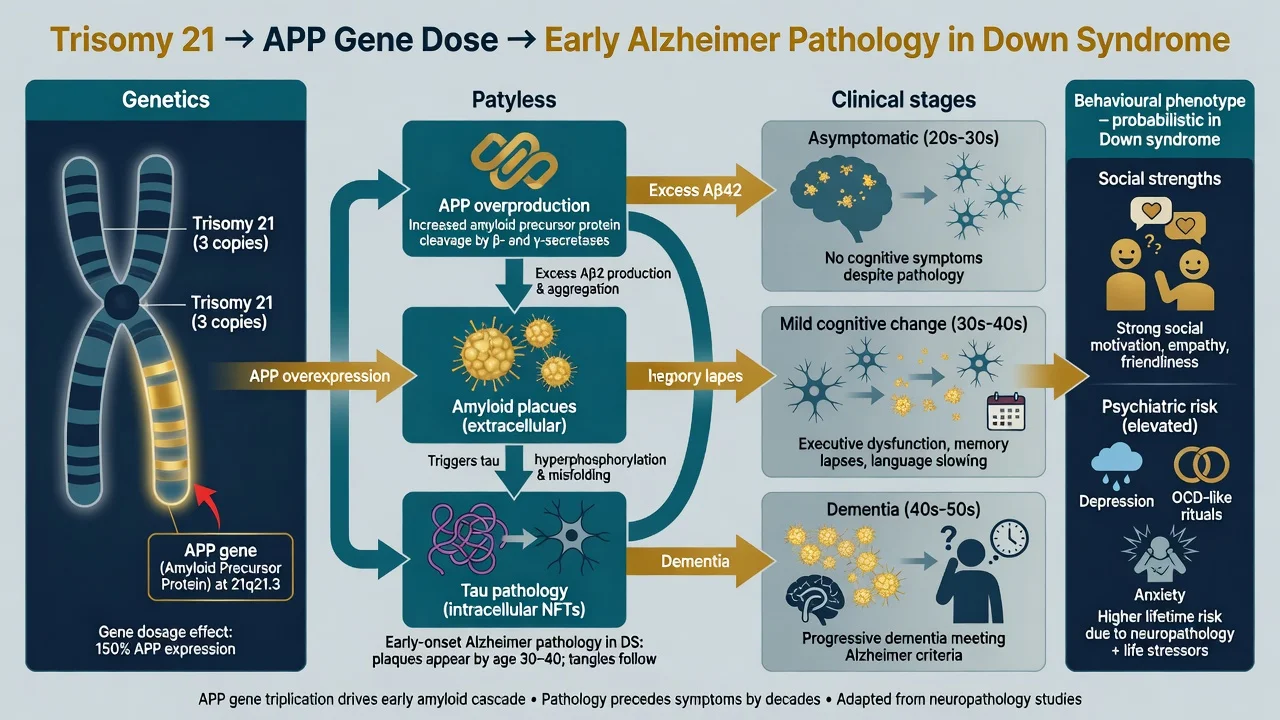
APP gene dose. Chromosome 21 includes the amyloid precursor protein gene. Extra copy number produces lifelong amyloid overproduction, early plaque pathology and subsequent tau-related neurodegeneration — the mechanistic backbone of DS-associated Alzheimer disease teaching.[2][1]
Biomarker cascade. Fortea and colleagues characterised ordered clinical and biomarker changes of Alzheimer disease in adults with DS, supporting the view of DS as a genetically determined Alzheimer model useful for both clinical staging language and research translation.[4]
Depression and behavioural change — multi-factor. Not reducible to amyloid alone: life events, sensory loss, pain, sleep disruption, hypothyroidism, early prodromal dementia, and social/environmental change all contribute. Treatable medical drivers are psychiatric interventions when they reverse functional decline.[8][1]
4. Clinical presentation
Across the lifespan
Childhood and adolescence. ADHD traits, anxiety, stubbornness/rigidity, OCD-like behaviours, sleep disturbance and, in a subset, autism spectrum features. Early developmental and educational supports dominate; psychiatric diagnosis still uses adapted criteria and collateral.[1][9]
Adulthood — depression. Withdrawal from previously enjoyed activities, irritability, tearfulness, sleep and appetite change, loss of skills, refusal of care, and reduced speech. Verbalised depressed mood and guilt may be limited — behavioural and functional change relative to baseline carries the diagnosis.[8][9]
Adulthood — Alzheimer dementia. Progressive decline in memory, executive function and adaptive skills; personality change; disorientation; late seizures, myoclonus and gait change in many. Early social strengths can make later apathy and skill loss particularly conspicuous to carers.[2][3][10]
5. Differential diagnosis — the core fellowship skill
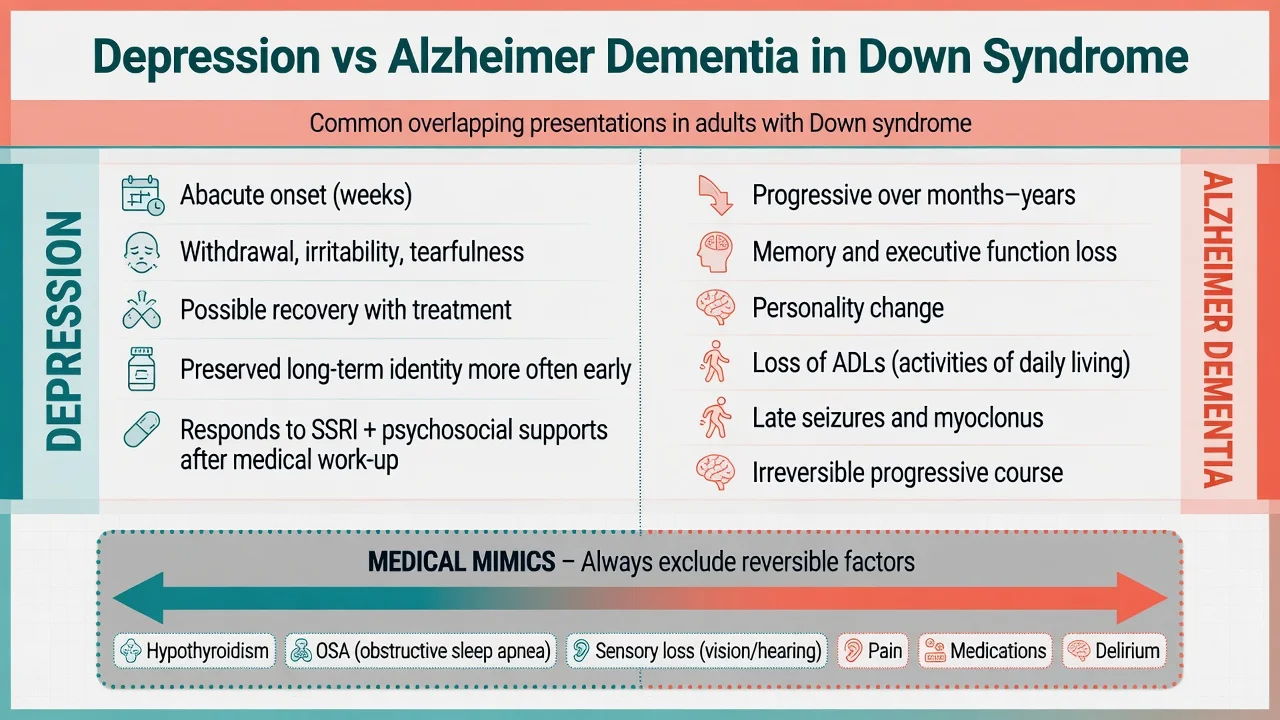
| Feature | Favours depression | Favours Alzheimer dementia |
|---|---|---|
| Onset | Weeks to few months | Months to years, progressive |
| Mood signs | Tearfulness, irritability, anhedonia | Apathy may dominate later |
| Cognition | May improve with mood recovery | Progressive multi-domain loss |
| Course | Potentially reversible with treatment | Progressive neurodegeneration |
| Late neurology | Uncommon if pure mood | Seizures, myoclonus more typical later |
| [3][8][2] |
Always also exclude: hypothyroidism, B12 deficiency, infection/delirium, obstructive sleep apnoea, hearing/vision loss, constipation/pain, anticholinergic or sedative load, grief and environmental change, and abuse/neglect.[1][8]
Diagnostic overshadowing is the named pitfall: attributing all new behaviour to DS and missing treatable depression, medical disease or dementia care needs.[7][11]
6. Assessment
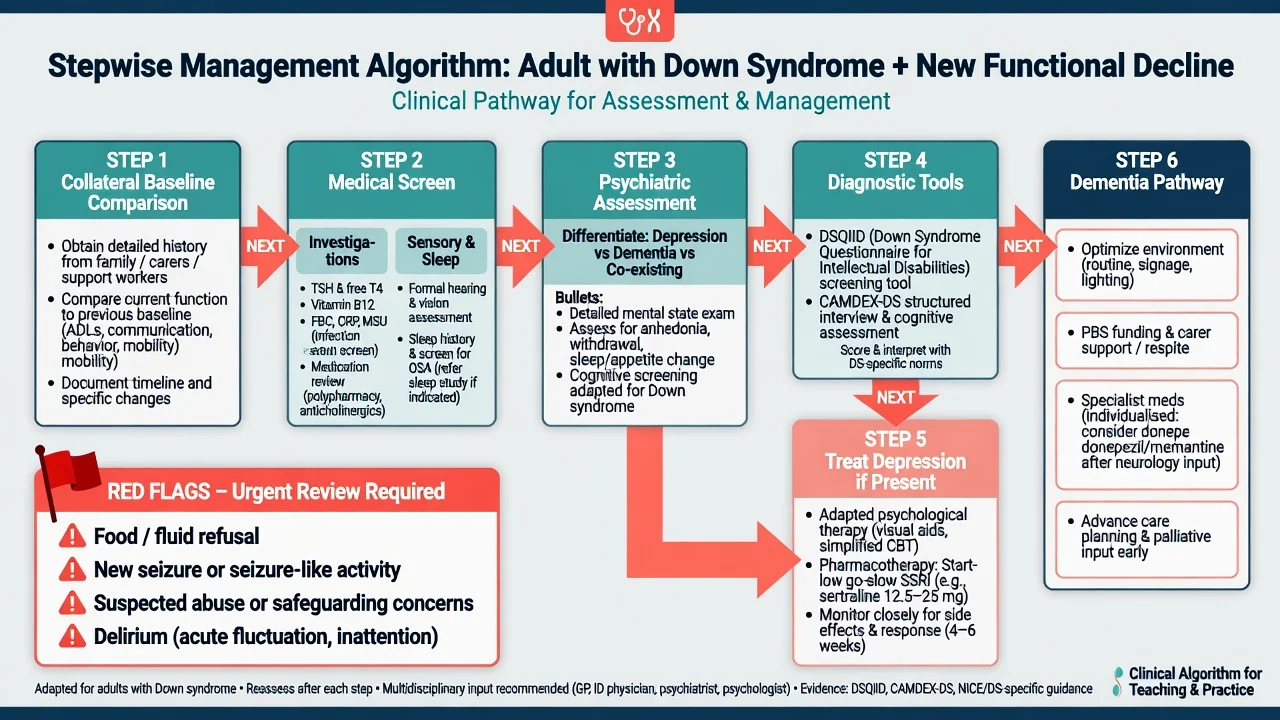
Structure. Developmental baseline (prior psychology/education reports); current adaptive function; onset timeline; medical systems review (thyroid, sleep, cardiac history, seizures); life events; safeguarding; carer capacity and burnout.[1][7]
MSE adapted for ID. Simple language, visual supports, adequate time, carer present for collateral. Assess affect, biological symptoms, psychosis carefully, cognition relative to known baseline, insight and risk (self-neglect, exploitation, suicide when mood disorder present).[8]
Capacity. Decision-specific. Use supported decision-making; least-restrictive legal framework under local statute — do not invent foreign section numbers in viva.[1]
7. Investigations and tools
Reversible work-up for new decline: TSH and free T4, B12/folate, FBC, electrolytes and glucose, infection screen as indicated, full medication review, hearing and vision assessment, and sleep evaluation when OSA is suspected (highly relevant medical comorbidity in DS).[1][8]
Dementia instruments combine carer screening with structured diagnostic interview when decline is suspected.[5][6]
- DSQIID (Deb et al.): observer-rated screening questionnaire for dementia in adults with intellectual disabilities — practical carer-facing tool.[6]
- Modified CAMDEX informant interview / CAMDEX-DS tradition (Ball et al.): structured, validated approach supporting diagnosis of dementia in adults with DS — exam answer for “how do you diagnose, not just screen?”.[5]
Imaging and biomarkers. Neuroimaging is case-by-case (e.g. atypical features, focal signs), not mandatory for every clinically typical progressive dementia in known DS. Research biomarker staging (Fortea) informs viva depth but does not replace clinical diagnosis in routine service exams.[4][10]
Before psychotropics: metabolic baseline and ECG as agent-appropriate.[8]
8. Acute and emergency management
Acute behavioural crisis: exclude pain, constipation, infection, seizure, sensory crisis, medication toxicity and abuse before “challenging behaviour” labelling. Severe depression with risk may require urgent psychiatric admission under local mental health law. New neurological events are medical until proven otherwise.[1][8]
9. Definitive management
Principles. Multidisciplinary care (ID psychiatry/psychology, speech and language, OT, audiology/ophthalmology, sleep/ENT, endocrinology, GP, day services). Non-pharmacological approaches first for behaviour driven by communication or environment (functional analysis, positive behaviour support).[1][7]
Depression. After medical work-up, combine developmentally adapted psychological support (simplified CBT elements, behavioural activation with carers, structured routine) with an SSRI when indicated. Start low, go slow in ID — for example sertraline oral 25 mg daily initially (some clinicians begin 12.5–25 mg in sensitive individuals), titrate slowly against effect and adverse effects, review at 2–4 weeks then 4–6 weeks, monitor activation, GI effects, hyponatraemia risk in older adults, and sexual side-effects as relevant. Continue an adequate trial duration once therapeutic; taper carefully after recovery period. Cite depression-in-DS evidence base for active treatment rather than nihilism.[8]
Dementia care. Environment simplification, consistent carers, visual supports, treat pain and sensory loss, carer education and respite, PBS for behavioural and psychological symptoms. Cholinesterase inhibitors or other dementia drugs are individualised/specialist decisions with realistic expectations — not a reflex script for every diagnosed case. Advance care planning and dementia-capable placement planning as disease progresses.[2][3][10]
Medical treatments that are psychiatric care. Correct hypothyroidism; treat OSA; optimise hearing aids/glasses; deprescribe anticholinergics where safe. These reverse “psychiatric” presentations more often than another antipsychotic.[1]
ANZ (RANZCP-aligned). Least-restrictive care, supported decision-making, ID mental health pathways where available; coordinate with NDIS/disability supports without inventing scheme rules in exam answers.[1][7]
UK (NICE-informed). Dementia diagnosis and post-diagnostic support principles apply with ID adaptation; challenging behaviour guidance prioritises functional analysis over routine antipsychotics.[3][8]
US (APA-informed). Dementia care and major depression guidelines adapted to developmental level; document capacity and surrogate decision-makers clearly.[2][8]
10. Subtypes and scenarios
Classic MEQ: 48-year-old with DS, three months of sitting alone, less speech, weight loss — depression work-up and treatment trial while tracking for dementia trajectory.[8][3]
Medical mimic: irritability and daytime sleepiness with snoring — OSA evaluation before antipsychotic.[1]
Transition: adolescent leaving school loses structure → mood and behaviour change; rebuild supports, do not leap to dementia language in a 19-year-old.[7]
End-stage DS-AD: seizures, dysphagia, full care needs — palliative psychiatry interface, carer support, avoid futile polypharmacy.[2][12]
11. Complications and pitfalls
- Missing treatable depression that looks like dementia (and vice versa).[8][3]
- Ignoring thyroid, OSA and sensory loss.[1]
- Antipsychotics for environmental behaviour without PBS thinking.[7]
- No personal baseline → false dementia diagnosis.[5][10]
- Therapeutic nihilism once “Alzheimer” is mentioned.[2]
- Failing capacity-supported decisions and advance planning.[1]
12. Prognosis and disposition
Life expectancy in DS has improved; dementia-capable adult services are therefore essential exam content. Depression is often treatment-responsive and can restore function. Clinical Alzheimer disease is progressive; multimorbidity is common in older adults with DS. Disposition usually shared between ID community teams, memory/dementia services and disability providers with a written multiagency plan and carer support.[1][12][3]
13. Special populations
Children: early intervention, school mental health, autism screen when indicated — do not over-pathologise developmental phenotype, but do not under-treat clear mood disorder.[1][9]
Adolescents: identity, sexuality education with capacity support, transition planning, mood disorders after life change.[7]
Older adults with DS: proactive surveillance for cognitive and functional decline from mid-adulthood; serial carer questionnaires help early detection.[3][6][12]
Cultural and equity: access to genetics counselling, ID psychiatry and dementia services is uneven — name equity explicitly in formulation answers.[1][12]
14. Evidence and guidelines
Landmark teaching set for this topic: Antonarakis primer (multisystem DS); Zigman (AD neurobiology); Holland (population dementia); Fortea (biomarker cascade); Ball (CAMDEX informant validity); Deb (DSQIID); Mantry (mental ill-health epidemiology); Walker (depression review); Myers (classic psychiatric series); Krinsky-McHale (early outcome measures); Dykens (phenotype concept); Bayen (older adult multimorbidity).[1][2][3][4][5][6][7][8][9][10][11][12]
15. Exam pearls
References
- [1]Antonarakis SE, Skotko BG, Rafii MS, et al. Down syndrome Nat Rev Dis Primers, 2020.PMID 32029743
- [2]Zigman WB, Lott IT Alzheimer's disease in Down syndrome: neurobiology and risk Ment Retard Dev Disabil Res Rev, 2007.PMID 17910085
- [3]Holland AJ, Hon J, Huppert FA, Stevens F, Watson P Population-based study of the prevalence and presentation of dementia in adults with Down's syndrome Br J Psychiatry, 1998.PMID 9828989
- [4]Fortea J, Vilaplana E, Carmona-Iragui M, et al. Clinical and biomarker changes of Alzheimer's disease in adults with Down syndrome: a cross-sectional study Lancet, 2020.PMID 32593336
- [5]Ball SL, Holland AJ, Huppert FA, Treppner P, Watson P, Hon J The modified CAMDEX informant interview is a valid and reliable tool for use in the diagnosis of dementia in adults with Down's syndrome J Intellect Disabil Res, 2004.PMID 15312062
- [6]Deb S, Hare M, Prior L, Bhaumik S Dementia screening questionnaire for individuals with intellectual disabilities Br J Psychiatry, 2007.PMID 17470960
- [7]Mantry D, Cooper SA, Smiley E, et al. The prevalence and incidence of mental ill-health in adults with Down syndrome J Intellect Disabil Res, 2008.PMID 18197953
- [8]Walker JC, Dosen A, Buitelaar JK, Janzing JG Depression in Down syndrome: a review of the literature Res Dev Disabil, 2011.PMID 21392935
- [9]Myers BA, Pueschel SM Psychiatric disorders in persons with Down syndrome J Nerv Ment Dis, 1991.PMID 1833506
- [10]Krinsky-McHale SJ, Zigman WB, Lee JH, et al. Promising outcome measures of early Alzheimer's dementia in adults with Down syndrome Alzheimers Dement (Amst), 2020.PMID 32647741
- [11]Dykens EM Measuring behavioral phenotypes: provocations from the "new genetics" Am J Ment Retard, 1995.PMID 7779347
- [12]Bayen E, Possin KL, Chen Y, Cleret de Langavant L, Yaffe K Prevalence of Aging, Dementia, and Multimorbidity in Older Adults With Down Syndrome JAMA Neurol, 2018.PMID 30032260