Psych · Intellectual disability psychiatry
Epilepsy in intellectual disability
Also known as Epilepsy and learning disability · Epilepsy intellectual disability psychiatry · Seizures in ID · Refractory epilepsy ID · SUDEP intellectual disability · Postictal psychosis ID · AED psychiatric side effects ID
Exam-exhaustive fellowship reference on epilepsy in intellectual disability — prevalence and severity gradient (McGrother ~26%), treatment resistance, peri-ictal behaviour vs primary mental illness, postictal psychosis and forced normalisation, AED psychiatric adverse effects, psychotropics and seizure threshold, SUDEP and premature mortality, joint neurology–ID psychiatry care, capacity and safety. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Epilepsy is one of the highest-yield physical–psychiatric interfaces in intellectual disability (ID) psychiatry. Examiners test whether you can distinguish seizure-related behaviour from primary mental illness, choose psychotropics without wrecking seizure control, and address preventable harm (status, SUDEP, drowning) rather than only writing antipsychotics for “aggression.”[4][5][6]
Overview and definition
Epilepsy is a disease of the brain defined by an enduring predisposition to generate epileptic seizures and by the neurobiological, cognitive, psychological and social consequences of that condition. In people with ID, epilepsy is usually a comorbidity of shared developmental brain pathology, not a random second illness. Bowley and Kerr’s classic review framed the dual burden of higher prevalence, more complex seizure types, treatment resistance, and service gaps that still structure exam answers.[4][14]
Critical exam distinction. Behavioural change in a person with ID and epilepsy is not automatically “challenging behaviour” and not automatically “psychosis.” Time the change to seizures, AEDs, pain, communication barriers and environment before diagnosing a primary psychiatric disorder or escalating psychotropics.[5][6][15]
Classification: seizures, syndromes and peri-ictal psychiatry
ILAE operational seizure types
The 2017 ILAE operational classification organises seizures by onset (focal, generalised, unknown) with optional awareness and motor descriptors. In non-verbal people with ID, onset and awareness are often inferred from video and multi-informant description rather than self-report — examiners reward honest uncertainty plus good collateral, not forced certainty.[14]
Aetiology and syndrome teaching points
Shared causes include cortical malformations, genetic channelopathies and syndromic conditions (teaching examples: Lennox–Gastaut spectrum, Dravet, tuberous sclerosis complex, Angelman, Rett-spectrum phenotypes). Severity of ID and epilepsy often co-travel because both reflect the extent of early brain disruption.[2][4]
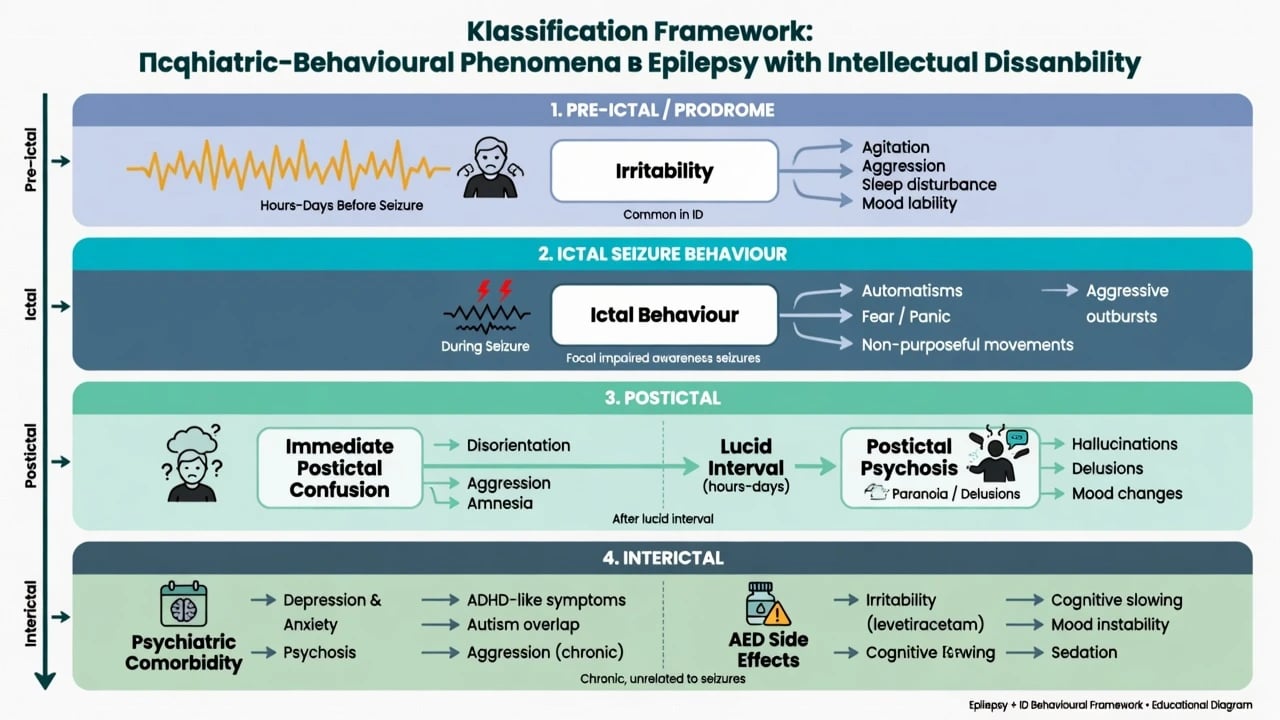
Psychiatric timing categories (must be exam-ready)
| Timing | Clinical pattern | Exam action |
|---|---|---|
| Pre-ictal / prodrome | Irritability, sleep change, mood lability hours–days before seizures | Diary correlation; do not only treat as primary mood disorder |
| Ictal | Automatisms, fear, impaired awareness, rare directed aggression | Protect airway/injury; video if recurrent |
| Immediate postictal | Confusion, aggression, amnesia | Safety; allow recovery; avoid punitive framing |
| Postictal psychosis | After cluster, often after a lucid interval, then psychosis | Safety, treat psychosis, neurology liaison — Logsdail/Toone pattern |
| Interictal | Depression, anxiety, psychosis, ADHD-like symptoms unrelated to single events | Standard psychiatric care, seizure-aware drugs |
| Iatrogenic | New irritability after AED change | Review AED first |
Epidemiology and risk
Headline epidemiology for viva recall
In a large adult ID service population, McGrother and colleagues reported epilepsy prevalence of approximately 26%, with about two-thirds of those with epilepsy still experiencing seizures despite anti-epileptic medication — the classic viva pair for prevalence plus treatment resistance.[1]
Robertson and colleagues’ systematic reviews confirm epilepsy is substantially more common than in the general population and increases with ID severity, and that epilepsy associates with increased mortality in people with ID, particularly where seizures are recent or ongoing.[2][3]
Population analyses of epilepsy generally also show elevated psychiatric comorbidity (mood, anxiety, psychosis pathways), a finding that compounds when ID limits symptom reporting.[9]
Pathophysiology and mechanisms
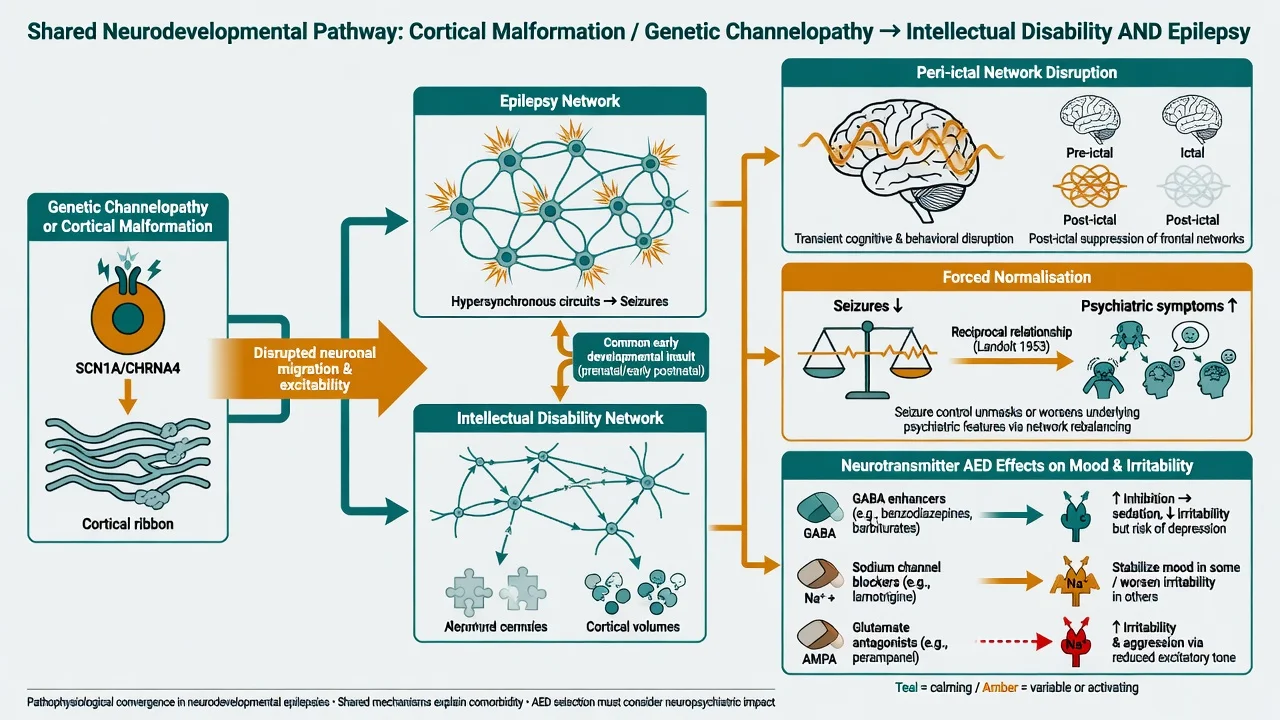
Examiners want a shared pathology model, not “epilepsy causes ID” as a single arrow.[4]
Shared developmental insult. Cortical malformation, channelopathy and genetic syndromes disrupt networks for cognition and for seizure generation simultaneously.[2][4]
Peri-ictal network disruption. Transient frontal and limbic network dysfunction produces confusion, aggression and cognitive slowing that recover with variable postictal duration — often longer and harder to judge against baseline in severe ID.[6][7]
Postictal psychosis. Classic descriptions emphasise psychosis emerging after seizures (often a cluster), frequently following a lucid interval of hours to days, with paranoid and affective features and substantial risk of harm — a CASC/viva red flag sequence.[7]
Forced normalisation (alternative psychosis). Psychiatric deterioration temporally linked to sudden improvement in seizures or EEG normalisation (Landolt concept; modern interface reviews) should be considered when aggressive AED escalation coincides with new psychosis or severe mood change — do not only add antipsychotics without reviewing the epilepsy trajectory.[8]
AED mechanisms and mood. Agents with psychiatric adverse-effect signals (commonly taught: levetiracetam irritability/aggression; topiramate cognitive/mood effects; perampanel aggression risk; sometimes zonisamide) can mimic primary psychiatric illness; enzyme-inducing AEDs alter psychotropic levels.[6][12]
Clinical presentation
Seizure semiology in ID is frequently atypical or under-recognised: brief staring, atonic drops, myoclonus, nocturnal events, subtle focal automatisms, or behavioural arrest without clear self-report of aura. Carers may describe only “turns,” “absences,” or “meltdowns.” Video of events and structured diaries transform assessment quality.[1][5]
MSE adaptations. Baseline-relative change, multi-setting collateral, AAC, sleep and appetite trends, and a timeline tying symptoms to seizures and AED starts/dose changes. Capacity for each decision (investigations, AED change, psychotropic trial) is supported, not assumed absent because of ID or epilepsy.[5][16]
Differential diagnosis
Epileptic / peri-ictal
- Stereotyped events with postictal state
- Cluster then lucid interval then psychosis
- Nonconvulsive status with fluctuating awareness
- New events after AED non-adherence
Primary psychiatric
- Depression, psychosis, anxiety on own criteria
- Not time-locked to seizures
- Trauma-related escalation
- Still common — do not overshadow
Behavioural / autism
- Escape-maintained aggression
- Sensory meltdown
- Stereotypy mistaken for seizure
- Function analysis still required
Medical / drug
- AED psychiatric adverse effects
- Akathisia from antipsychotics
- Pain, constipation, infection
- Syncope, hypoglycaemia, movement disorder
Psychogenic non-epileptic seizures can coexist with epilepsy; video-EEG is definitive when available. Do not diagnose PNES from a single staff description of “dramatic” behaviour in someone with known epilepsy.[5][6]
Bedside assessment
History structure. Age at seizure onset; syndrome/aetiology if known; seizure types and frequency; last seizure; injuries; rescue medication; AED list with doses and adherence supports; prior status; sleep; water exposure; psychiatric history; psychotropics; carer goals.[5]
Functional and risk assessment. Map aggression or self-injury to peri-ictal windows versus operant functions (attention, escape, tangible, automatic). Risk domains: status epilepticus, injury, drowning, burns, SUDEP, aspiration, carer injury during seizures, sexual vulnerability during postictal states, and medication non-adherence.[3][13][15]
Investigations
Investigate to answer a clinical question, not as a generic “epilepsy bloods” ritual.[5]
- EEG / video-EEG when diagnosis of events is uncertain, nonconvulsive status is suspected, or syndrome classification would change management.
- MRI epilepsy protocol when aetiology is unclear, seizures newly worsen without explanation, or surgery is being considered — not endless re-imaging of a stable known syndrome without red flags.
- Bloods / drug levels as indicated by the AED regimen, toxicity concern, or systemic illness; metabolic and infection work-up for acute behavioural change.
- ECG when combining QTc-relevant psychotropics with polypharmacy.
- Genetics when an undiagnosed syndromic cause would alter counselling or targeted therapy.
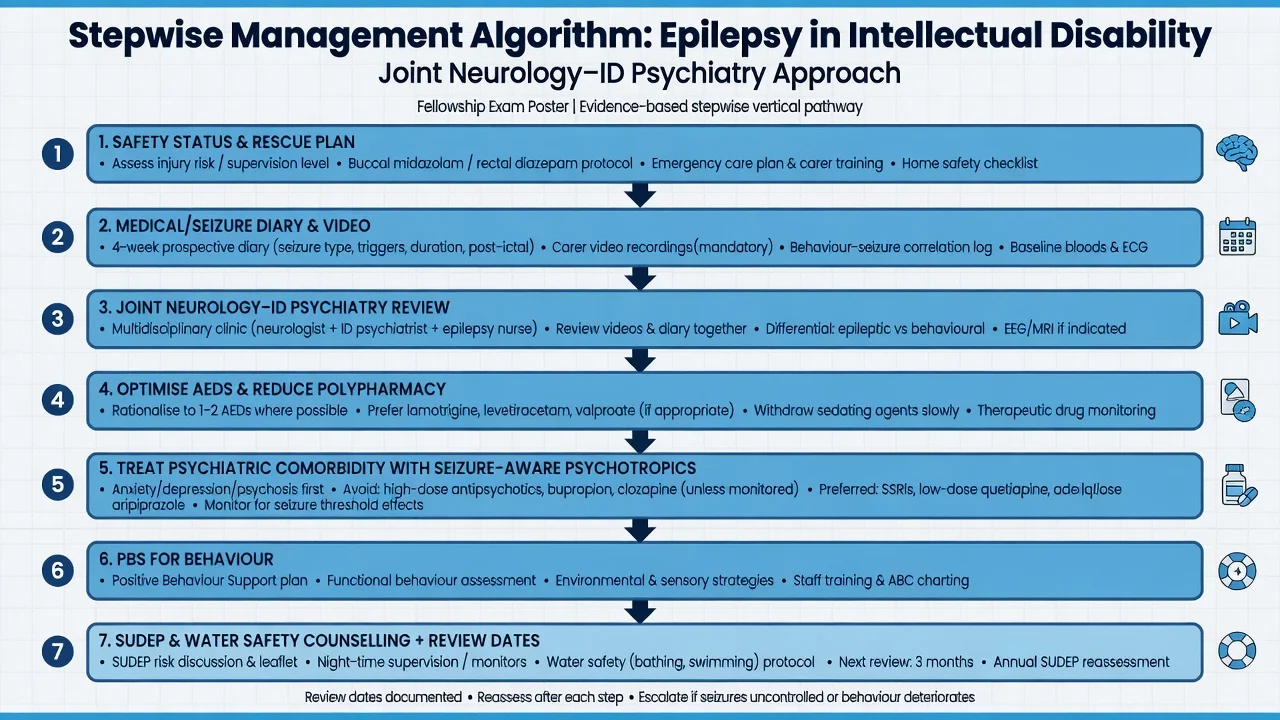
Acute management (safety)
Definitive management
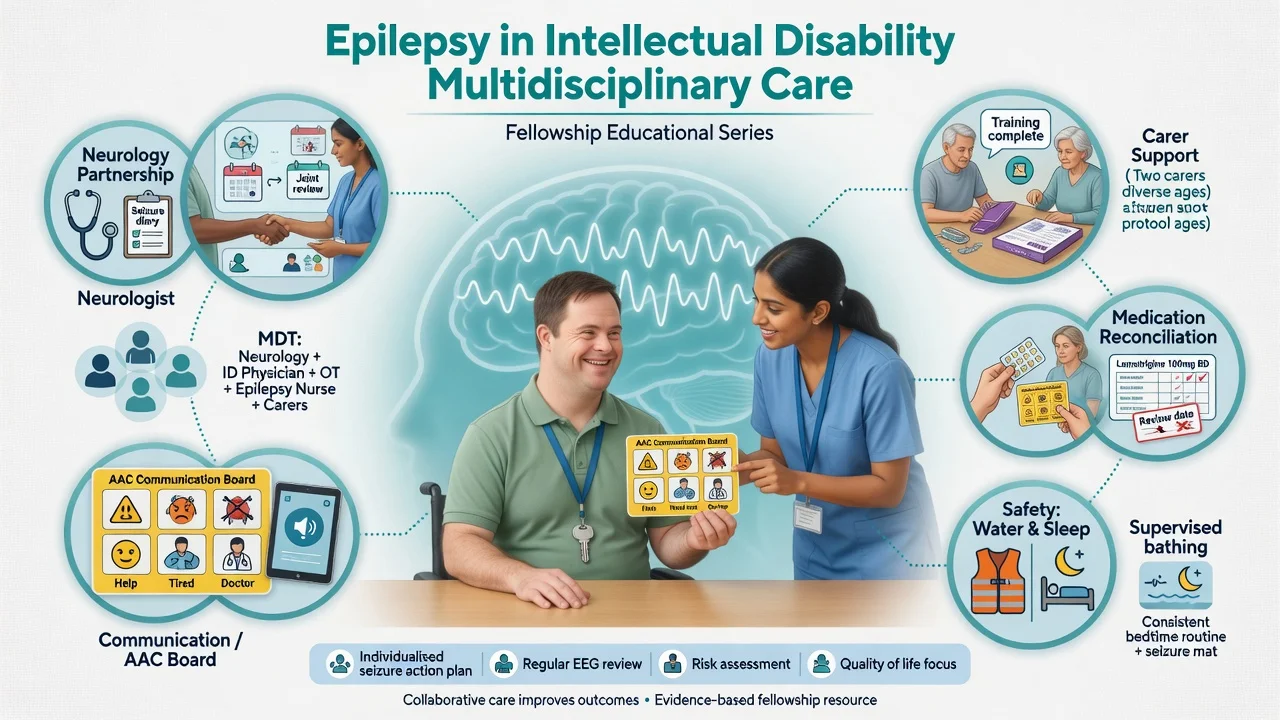
Joint epilepsy care (Kerr consensus principles)
Consensus guidance for epilepsy in adults with ID emphasises specialist epilepsy access, accurate diagnosis of events, individualised care plans, carer education, attention to psychiatric comorbidity, and avoidance of therapeutic nihilism. Quality of life, injury prevention and treatment of depression matter as much as raw seizure counts when epilepsy is refractory.[5][6]
Anti-epileptic drugs and psychiatric adverse effects
Optimise AEDs with neurology: simplify polypharmacy where possible; match agent to syndrome; monitor adherence using supports (blister packs, staff protocols). When new irritability, aggression, depression or psychosis appears after an AED start or dose rise, review that AED before diagnosing lifelong primary psychosis — high-yield agents in teaching include levetiracetam, perampanel, topiramate and zonisamide, while enzyme inducers complicate psychotropic levels.[6][12]
Valproate and reproductive risk. In women and people who can become pregnant, valproate carries major congenital malformation and neurodevelopmental risk; pregnancy prevention programmes and alternative AEDs are mandatory exam and practice points — capacity and supported decision-making shape how this is discussed in ID services.[5][12]
Psychiatric comorbidity treatment (seizure-aware)
Depression and anxiety are common in epilepsy populations and under-recognised when communication is limited; treat on clinical grounds with adapted assessment.[9][12]
Psychotropics and seizure threshold (exam ladder). Analyses of FDA trial data and clinical reviews show differential seizure risk: bupropion and clozapine are high-risk teaching examples; many SSRIs and several antipsychotics at usual doses have more modest signals, but any proconvulsant effect rises with dose, rapid titration, polypharmacy, alcohol withdrawal and poorly controlled epilepsy. Prefer agents with favourable epilepsy experience (commonly taught: sertraline/citalopram/escitalopram for depression/anxiety after individualisation; avoid casual bupropion). For psychosis, choose with neurology if epilepsy is active; use the lowest effective antipsychotic dose with metabolic and seizure monitoring — not open-ended chemical restraint for peri-ictal irritability.[10][11][12][16]
Illustrative depression start in a medically monitored adult with ID and stable epilepsy (always individualise for interactions, renal/hepatic function and swallowing): sertraline 25–50 mg oral daily, titrate slowly to the lowest effective dose (often 50–100 mg daily), monitor mood, sleep, hyponatraemia risk, bleeding risk with NSAIDs, and seizure frequency with carers — cite epilepsy–depression treatment literature when justifying antidepressant use in active epilepsy.[12]
Behaviour support, not only tablets
When aggression is escape-maintained or sensory, positive behaviour support and environmental redesign remain first-line for non-psychotic challenging behaviour; epilepsy does not license lifelong antipsychotics without mental illness formulation. WPA ID prescribing guidance and ANZ framing still prioritise non-drug strategies for problem behaviour, with medicines time-limited and monitored when used.[15][16]
SUDEP and safety counselling
Sudden unexpected death in epilepsy is a major preventable-harm teaching domain: risk concentrates with uncontrolled generalised tonic–clonic seizures, nocturnal seizures, and non-adherence; mechanisms involve cardiorespiratory collapse in the postictal state. Counselling (proportionate, not terrifying), night-time supervision strategies where appropriate, adherence support, and water safety (bathing, swimming) are core ID psychiatry duties alongside neurology.[3][13]
Australia/NZ practice note. Shared care with neurology/epilepsy clinics, NDIS behaviour support where restrictive practices interface with seizure care, and Trollor-aligned caution with psychotropics for behaviour remain central. Document capacity, substitute decision-makers for AED/psychotropic changes, and SUDEP counselling in the care plan.[16]
Subtypes and scenarios
Severe/profound ID with refractory epilepsy. Prioritise safety, carer training, rescue plans, and quality-of-life goals; accept that seizure freedom may be unrealistic.[1][5]
Autism + ID + epilepsy. Sensory load and communication barriers amplify both meltdowns and seizure under-recognition; video and diary are essential.[4]
Postictal psychosis in mild–moderate ID. Classic lucid-interval story; high short-term risk; treat and reassess once seizures stabilise.[7]
New behaviour after levetiracetam. Dose reduction or switch often more rational than adding risperidone.[6][12]
Deprescribing redundant psychotropics. Safe if no mental illness indication and epilepsy plan is stable — coordinate so staff do not misread post-taper restlessness as “needs more AED.”[15][16]
Complications and pitfalls
- Diagnostic overshadowing (all behaviour = ID, or all behaviour = epilepsy)
- Missing nonconvulsive status
- Abrupt AED cessation for behaviour
- Stacking antipsychotics for peri-ictal irritability
- Ignoring SUDEP, drowning and burns risk
- Valproate without reproductive risk management
- Forced normalisation missed after aggressive seizure control
- Enzyme-inducing AED–psychotropic interactions
Prognosis and disposition
Many people with ID and epilepsy remain treatment-resistant; outcomes improve when care plans integrate seizure first aid, medication supports, behavioural formulation, mental health treatment and carer training. Mortality risk tracks ongoing seizures — disposition needs shared neurology–ID psychiatry ownership, epilepsy nurse input where available, rescue protocols, medication reconciliation dates, and explicit safety education.[1][3][5]
Special populations
Transition from paediatric services. Loss of epilepsy follow-up at transition is a known harm pathway; ensure adult ID/epilepsy handover.[5]
Women and people who can become pregnant. Valproate risk, contraception, folic acid per neurology advice, and pregnancy planning with supported decision-making.[5][12]
Older adults with ID. Drug sensitivity, falls, aspiration, dementia interface, and polypharmacy reviews dominate.[16]
Forensic dual disability. Seizure-related aggression must be distinguished from offence-paralleling behaviour; capacity and intent analysis remain rigorous.[5]
Evidence and guidelines summary
McGrother 2006 supplies the ~26% prevalence and treatment-resistance teaching pair; Robertson 2015 reviews synthesise prevalence gradients and mortality excess with ongoing seizures; Bowley and Kerr 2000 and Kerr 2009 consensus guidelines structure adult ID epilepsy management; Kerr 2011 international statements address neuropsychiatric comorbidity treatment; ILAE 2017 supplies seizure classification language; Logsdail/Toone and Krishnamoorthy anchor postictal psychosis and forced normalisation; Alper, Pisani and Mula frame psychotropic seizure risk and drug selection; Devinsky 2016 reviews SUDEP epidemiology and prevention; Deb WPA and Trollor ANZ guides restrain casual psychotropic use for behaviour in ID.[1][2][3][4][5][6][7][8][10][11][12][13][14][15][16]
Exam pearls
- ~1 in 4 adults with ID (service contact) has epilepsy; higher in severe ID
- Expect ongoing seizures despite AEDs in a large fraction
- Always time-lock behaviour to the peri-ictal timeline
- Cluster → lucid interval → psychosis = postictal psychosis until proven otherwise
- Never stop AEDs abruptly for behaviour
- Review levetiracetam/perampanel/topiramate before stacking antipsychotics
- Avoid casual bupropion and high-risk proconvulsants
- Counsel SUDEP and water safety
- Valproate: teratogenicity and neurodevelopmental risk programmes
- Challenging behaviour still needs function — epilepsy is not a free pass for lifelong antipsychotics
References
- [1]McGrother CW, Bhaumik S, Thorp CF, Hauck A, Branford D, Watson JM Epilepsy in adults with intellectual disabilities: prevalence, associations and service implications Seizure, 2006.PMID 16782360
- [2]Robertson J, Hatton C, Emerson E, Baines S Prevalence of epilepsy among people with intellectual disabilities: A systematic review Seizure, 2015.PMID 26076844
- [3]Robertson J, Hatton C, Emerson E, Baines S Mortality in people with intellectual disabilities and epilepsy: A systematic review Seizure, 2015.PMID 26076855
- [4]Bowley C, Kerr M Epilepsy and intellectual disability J Intellect Disabil Res, 2000.PMID 11079350
- [5]Kerr M, Scheepers M, Arvio M, et al. Consensus guidelines into the management of epilepsy in adults with an intellectual disability J Intellect Disabil Res, 2009.PMID 19527434
- [6]Kerr MP, Mensah S, Besag F, et al. International consensus clinical practice statements for the treatment of neuropsychiatric conditions associated with epilepsy Epilepsia, 2011.PMID 21955156
- [7]Logsdail SJ, Toone BK Post-ictal psychoses. A clinical and phenomenological description Br J Psychiatry, 1988.PMID 3167343
- [8]Krishnamoorthy ES, Trimble MR, Sander JW, Kanner AM Forced normalization at the interface between epilepsy and psychiatry Epilepsy Behav, 2002.PMID 12609326
- [9]Tellez-Zenteno JF, Patten SB, Jetté N, Williams J, Wiebe S Psychiatric comorbidity in epilepsy: a population-based analysis Epilepsia, 2007.PMID 17662062
- [10]Alper K, Schwartz KA, Kolts RL, Khan A Seizure incidence in psychopharmacological clinical trials: an analysis of Food and Drug Administration (FDA) summary basis of approval reports Biol Psychiatry, 2007.PMID 17223086
- [11]Pisani F, Oteri G, Costa C, Di Raimondo G, Di Perri R Effects of psychotropic drugs on seizure threshold Drug Saf, 2002.PMID 11888352
- [12]Mula M Epilepsy and Psychiatric Comorbidities: Drug Selection Curr Treat Options Neurol, 2017.PMID 29046989
- [13]Devinsky O, Hesdorffer DC, Thurman DJ, Lhatoo S, Richerson G Sudden unexpected death in epilepsy: epidemiology, mechanisms, and prevention Lancet Neurol, 2016.PMID 27571159
- [14]Fisher RS, Cross JH, French JA, et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology Epilepsia, 2017.PMID 28276060
- [15]Deb S, Kwok H, Bertelli M, et al.; Guideline Development Group of the WPA Section on Psychiatry of Intellectual Disability International guide to prescribing psychotropic medication for the management of problem behaviours in adults with intellectual disabilities World Psychiatry, 2009.PMID 19812757
- [16]Trollor JN, Salomon C, Franklin C Prescribing psychotropic drugs to adults with an intellectual disability Aust Prescr, 2016.PMID 27756975