Psych · Intellectual disability — neurodevelopmental
Foetal alcohol spectrum disorder
Also known as FASD · Fetal alcohol spectrum disorder · Fetal alcohol syndrome · Foetal alcohol syndrome · Partial fetal alcohol syndrome · Alcohol-related neurodevelopmental disorder · ARND · ND-PAE · Prenatal alcohol exposure
Exam-exhaustive fellowship reference on foetal alcohol spectrum disorder — diagnostic systems (Hoyme, Cook/Canadian, 4-digit code, DSM-5-TR ND-PAE), sentinel facial features, neurobehavioural profile, differentials (ADHD, ASD, ID, trauma), multidisciplinary assessment, comorbidity-focused management without a disease-modifying drug, secondary disability prevention, forensic interface, and primary prevention. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Foetal (fetal) alcohol spectrum disorder is a high-yield interface topic for intellectual disability, child and adolescent, addiction, forensic and perinatal psychiatry. Examiners test whether you can apply a named diagnostic framework, describe the neurobehavioural profile that drives most psychiatric referrals, separate FASD from ADHD/ASD/trauma without false mutual exclusivity, manage without inventing a core FASD tablet, and state the public-health prevention message with clinical humility rather than mother-blame.[1][2][12][18]
Overview and definition
FASD is the umbrella term for the range of physical, cognitive, behavioural and adaptive effects of prenatal alcohol exposure (PAE). Jones and Smith’s 1973 recognition of fetal alcohol syndrome (FAS) in early infancy established the classic dysmorphic–growth–CNS triad; the field has since expanded to a spectrum because many people with clinically important PAE-related brain injury lack the full facial phenotype.[6][15]
Core exam framing: alcohol is a teratogen; CNS vulnerability spans gestation; facial sentinel features largely reflect early first-trimester effects; neurobehavioural impairment can occur with or without classic face. There is no single laboratory or imaging test that confirms or excludes FASD in routine practice — diagnosis is clinical and multidisciplinary.[1][12][18]
Classification
Spectrum labels (historical and current)
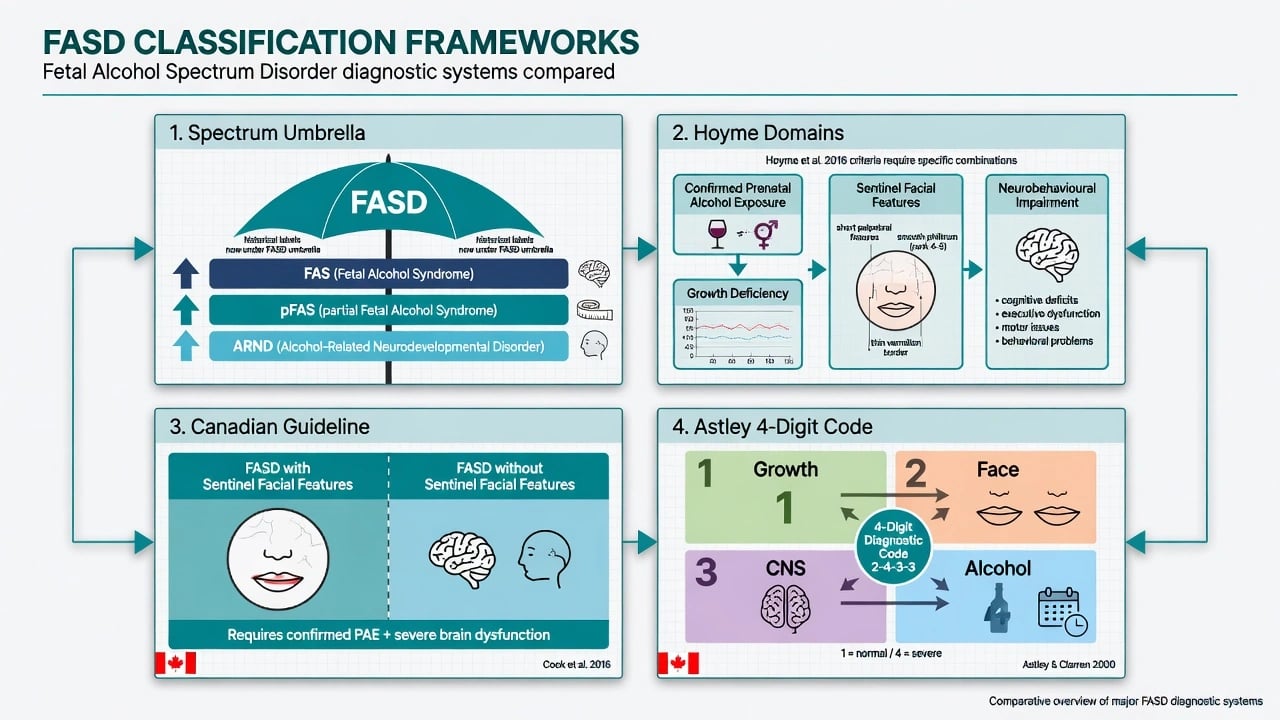
Under the FASD umbrella, classical labels include FAS (sentinel facial features, growth deficiency and CNS involvement), partial FAS (pFAS), alcohol-related neurodevelopmental disorder (ARND) and alcohol-related birth defects (ARBD). Exact thresholds differ by system; the fellowship skill is naming the system and applying its combinations, not memorising every cut-point table under examination stress.[1][13][15]
Hoyme 2016 updated clinical guidelines
Hoyme and colleagues updated diagnostic guidelines emphasising documented combinations of confirmed PAE, growth deficiency, sentinel facial features (short palpebral fissures, smooth philtrum, thin upper vermilion) and neurobehavioural impairment (with cognitive and behavioural domains operationalised for clinical use). These guidelines remain a US/international exam landmark for structured diagnosis.[1]
Canadian lifespan guidelines (Chudley 2005 → Cook 2016)
Canadian guidance shifted practice toward diagnosing FASD with sentinel facial features versus FASD without sentinel facial features, both requiring severe brain dysfunction in specified domains plus PAE confirmation standards appropriate to age. Cook and colleagues provide a lifespan diagnostic pathway usable from childhood into adult services — highly relevant to dual-diagnosis and general adult interfaces.[2][13]
Astley 4-digit diagnostic code
The 4-digit code ranks growth, face, CNS and alcohol exposure each on a 1–4 severity scale, producing a compact diagnostic code that improves precision across the full PAE spectrum. Examiners may ask you to name the four ranks even if you do not score a case live.[9]
DSM-5-TR framing
DSM-5-TR includes neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE) as a condition that captures clinically significant neurobehavioural impairment after PAE. Use it as a communication bridge in US-style answers while still knowing that specialist FASD clinics often use Hoyme/Canadian/4-digit systems for full phenotype coding.[12][18]
Epidemiology and risk factors
Headline FASD numbers for exams
Global systematic synthesis estimated FASD prevalence among children and youth around 7.7 per 1000, with regional heterogeneity and under-ascertainment in many health systems.[4] Active case-ascertainment studies in US communities found substantially higher rates among first-graders — on the order of 1 to 5 percent depending on conservative versus less conservative estimation — implying clinical services systematically miss cases.[5]
Popova and colleagues estimated global alcohol use during pregnancy at about 9.8 percent and FAS (the severe facial–growth end) at about 14.6 per 10 000, with roughly one FAS birth per 67 women who drank during pregnancy in model estimates — order-of-magnitude exam figures, not local clinic prevalence.[10]
Risk framing. Dose, pattern (especially binge exposure), timing, maternal nutrition, genetic modifiers and postnatal environment all shape outcome. Public-health and clinical consensus: there is no known safe amount or safe time for alcohol in pregnancy.[12][10] Risk clusters with maternal alcohol use disorder, unplanned pregnancy, limited prenatal care and social adversity — address systems, not stereotypes.[12][16]
Pathophysiology
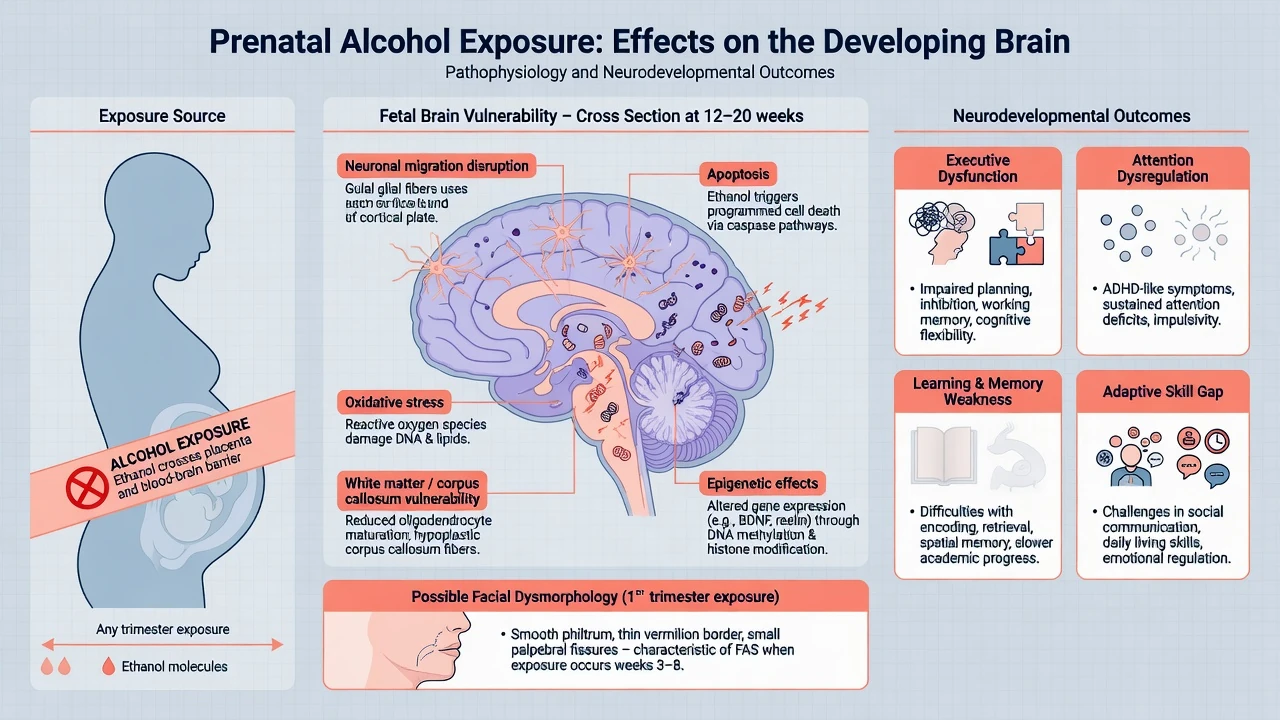
Ethanol crosses the placenta and disrupts neurodevelopment through apoptosis, oxidative injury, impaired neuronal migration and axon pathfinding, disrupted glial/oligodendrocyte maturation, and epigenetic modulation of gene expression.[15][18] Neuroimaging associations include reduced brain volume, corpus callosum anomalies and white-matter microstructural change, but imaging supports formulation; it does not replace clinical diagnosis.[18]
Clinical presentation and neurobehavioural profile
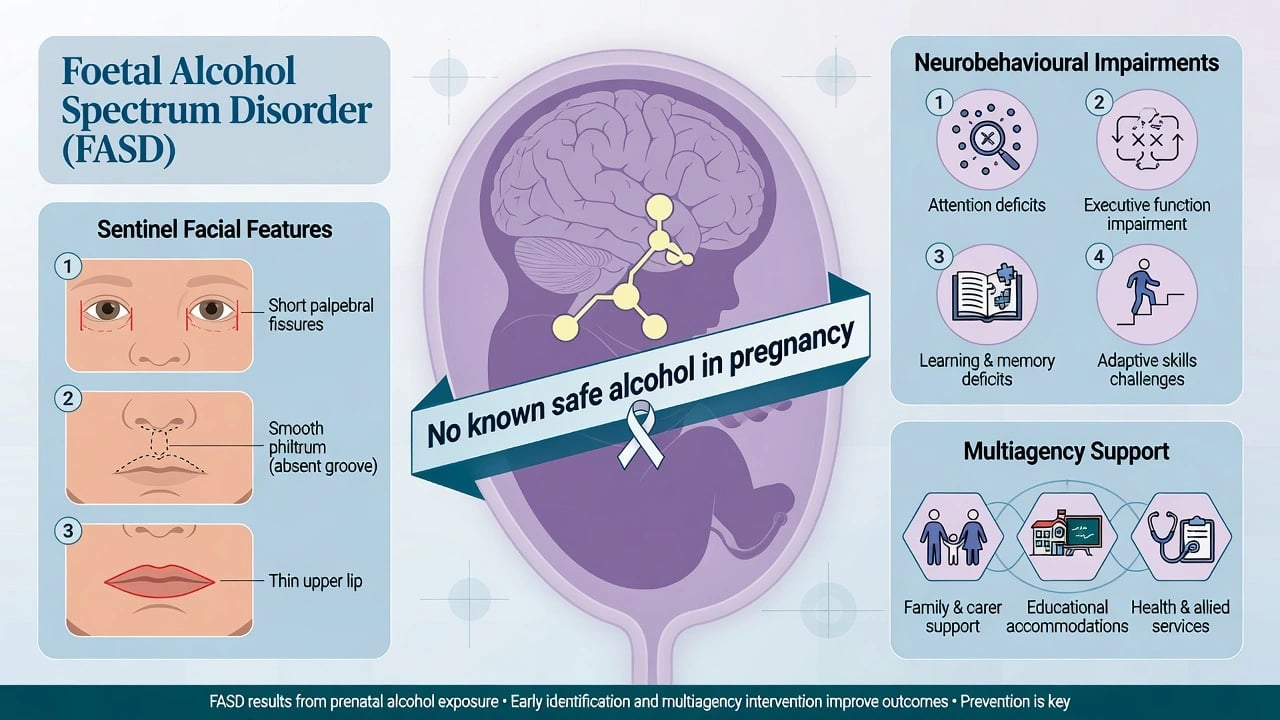
Sentinel facial triad (when present): short palpebral fissures, smooth philtrum, thin upper lip vermilion — measure with standardised tools when expertise is available.[1][9]
Growth: prenatal and/or postnatal deficiency of height, weight or head circumference may be present, especially toward the FAS end of the spectrum.[1]
Neurobehavioural profile (the psychiatry core). Collaborative work toward a FASD neurobehavioural signature emphasises difficulties in executive function, attention regulation, learning and memory, and adaptive behaviour that often outstrip what IQ alone predicts.[7][8] Comprehensive reviews document deficits across cognition, academic skill, attention, executive control, memory, motor and social domains after PAE.[8][15]
Developmental course. Infancy may show poor suck, irritability and delayed milestones. School age classically presents as ADHD-like inattention/impulsivity, learning disability, classroom dysregulation and peer difficulty. Adolescence and adulthood bring high rates of mental illness, substance use, school disruption, justice contact and adaptive failure if supports are absent.[11][19][20]
MSE adaptations. Use concrete language, allow processing time, check understanding repeatedly, avoid multi-step verbal instructions, and do not confuse concrete or literal answers with oppositionality. Assess capacity decision-by-decision and screen suicide, substance use and exploitation risk explicitly.[11][18]
Differential diagnosis
Win differentials on PAE history quality, growth/face data, developmental timeline and adaptive–executive profile — not on a single behavioural label.[1][12]
ADHD
- Very high co-occurrence; dual diagnosis often correct
- PAE history and adaptive lag beyond pure ADHD tip to FASD framing
- Stimulants may help attention but do not treat FASD core injury
- School plan must address memory/executive load, not only inattention
ASD
- Social-communication overlap is real
- Restricted interests and sensory differences can co-occur
- Dysmorphology + PAE history and adaptive pattern help discrimination
- Dual diagnosis is allowed when both criteria are met
ID / other genetic syndromes
- Global ID may co-occur with FASD
- Dysmorphic differentials need genetics input
- Microarray/fragile X when phenotype suggests alternative
- Do not stop at 'ID unspecified' if PAE is documented
Trauma / attachment / neglect
- Common co-travellers in the same child
- Trauma does not erase teratogenic brain effects
- Formulation should include both PAE and adversity
- Safeguarding may be active alongside diagnosis
Other teratogens (e.g. valproate embryopathy) and genetic syndromes enter the dysmorphology differential — involve clinical genetics when facial or multi-system features are atypical for pure PAE.[1][18]
Clinical and bedside assessment
Structure fellowship assessments as follows:[1][2][12]
- PAE history — timing, quantity, binge pattern; use non-judgemental enquiry; seek collateral and prenatal records when available.
- Growth chart and OFC trajectory.
- Facial assessment — standardised when possible (palpebral fissure length, lip–philtrum guide).
- Neurodevelopmental domains — cognition, executive function, memory, attention, language, motor, adaptive, social, academic.
- Mental health and risk — ADHD, mood, anxiety, psychosis, substance use, suicide, exploitation, offending.
- Medical comorbidities — hearing, vision, sleep, seizures, congenital anomalies.
- Family system, custody, culture, carer burden, and child-protection status.
- Capacity for specific decisions; local guardianship/mental health law principles (least restrictive; do not invent foreign section numbers).[2][18]
Multidisciplinary diagnosis is the standard: paediatrics or developmental medicine, dysmorphology/genetics as needed, neuropsychology, psychiatry, speech/OT, and social work. Psychiatry often first meets the school-age behavioural phenotype — your job is to open the FASD differential, not to complete every growth measurement alone.[1][2][12]
Investigations
| Indication | Test / action | Note |
|---|---|---|
| Language delay / school failure | Hearing and vision | Do not skip basic sensory screens |
| Atypical dysmorphology or ID | Chromosomal microarray ± fragile X / panels | Rule out alternative or co-occurring genetic diagnoses |
| Seizures, focal neurology, atypical regression | EEG / neurology; MRI if indicated | Imaging does not diagnose typical FASD alone |
| Before psychotropics for aggression | Weight/BMI, metabolic panel, BP, ECG as indicated | Same safety culture as other neurodevelopmental care |
| Behavioural change | Dental pain, constipation, sleep apnoea, otitis | Medical drivers of behaviour are common |
| [1][12][18] |
Management — acute crisis
De-escalate with low sensory load, concrete single-step language, predictable choices and familiar carers. Exclude pain, delirium, seizure, intoxication and acute psychiatric emergency. Use least-restrictive safety measures. Safeguarding thresholds apply when the child or adult is at risk from carers or self.[16][18]
Management — definitive and stepwise
Core principle
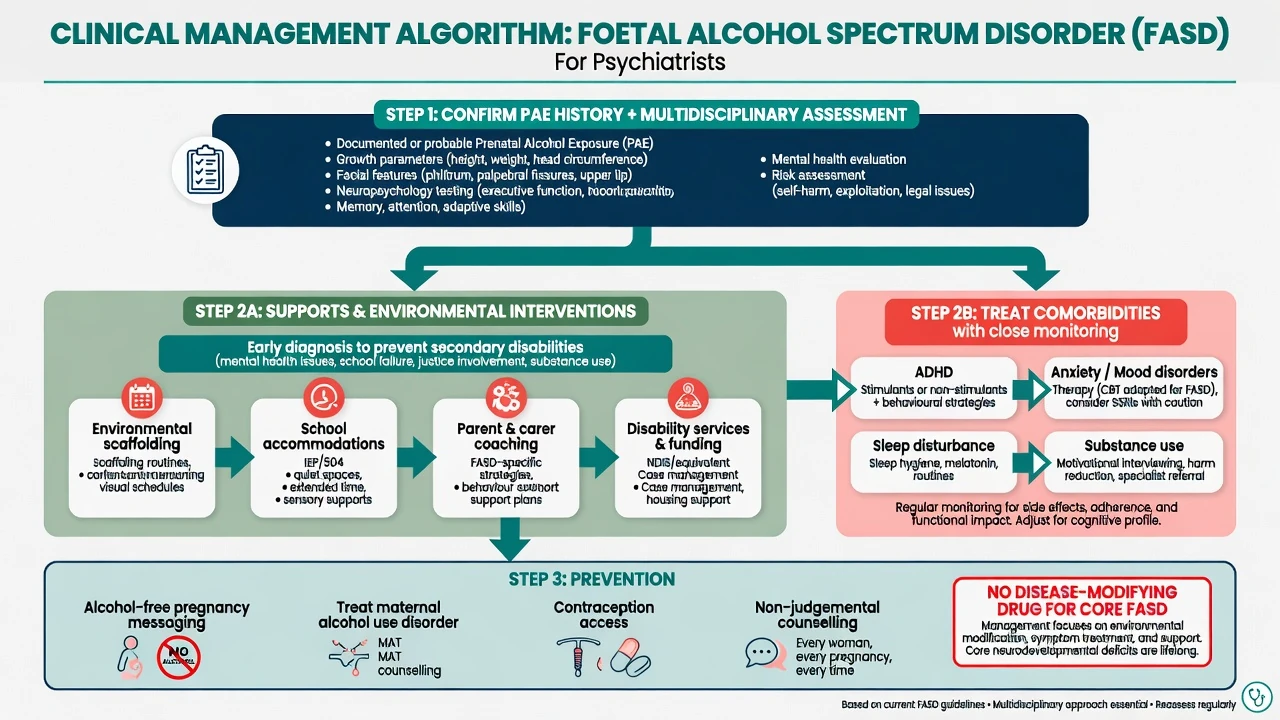
No medication reverses prenatal alcohol-related brain injury. Primary care is environmental scaffolding, education and disability supports, family coaching, and treatment of comorbidities. Early diagnosis and stable caregiving are protective against secondary disabilities.[12][19][16]
Environmental and educational scaffolding
Reduce cognitive load: visual schedules, chunked instructions, consistent routines, supervised transitions, and explicit teaching of social and daily living skills. Educational accommodations (extra time, reduced distraction, memory supports) are clinical interventions, not optional soft extras.[12][18] Parent and carer coaching plus positive behaviour support should precede long-term antipsychotic use for challenging behaviour.[17][16]
Comorbidity-targeted psychiatry
Meta-analytic and systematic reviews document a heavy burden of medical and mental health comorbidity in FASD.[3][14] Psychiatric conditions associated with PAE include ADHD-spectrum problems, mood and anxiety disorders, and later substance use and personality-related difficulties; adult series reported high rates of mental illness.[11][20][14]
Practical approach to comorbidity care follows the same principles as other neurodevelopmental disorders: treat threshold diagnoses, adapt for executive and language profile, and monitor physical health closely.[11][12][17]
- ADHD symptoms: behavioural strategies plus stimulant or non-stimulant medication when criteria are met, starting low and monitoring appetite, sleep, growth and mood — expect partial responses and ongoing executive needs.[11][12]
- Anxiety and depression: adapted psychological therapies with concrete, structured methods; cautious SSRI use when indicated, with monitoring for activation and self-harm.[17]
- Sleep: sleep hygiene, rule out OSA and environmental chaos; consider melatonin pathways under local guidance when appropriate.[12]
- Substance use: motivational interviewing adapted for cognitive profile; integrated dual-diagnosis care.[17]
- Severe aggression: functional analysis and medical screen first; if antipsychotics are used after behavioural optimisation for safety, use the lowest effective dose, time-limited goals, and full metabolic monitoring — the indication is behaviour risk, not “treating FASD.”[18][17]
Systematic review evidence for mental health and substance-use interventions in PAE/FASD is growing but still limited; individualise and measure outcomes rather than assuming standard protocols transfer unchanged.[17]
Secondary disability prevention
Streissguth and colleagues documented high lifespan rates of disrupted school, trouble with the law, confinement, inappropriate sexual behaviours and alcohol/drug problems among people with FAS/FAE, with earlier diagnosis and stable nurturing environments increasing odds of escaping adverse outcomes.[19] Systems-level barriers (late diagnosis, fragmented services, stigma) perpetuate secondary conditions — advocacy is clinical work.[16]
Specific subtypes and scenarios
Toddler with PAE and delay. Parallel developmental assessment and early intervention; do not wait for “perfect face.”[12]
School-age ADHD + learning problems. Open FASD history; request multidisciplinary review; dual-label ADHD when criteria met.[11][7]
Adolescent forensic referral. Assess fitness, suggestibility, understanding of charges, and support needs; divert toward disability-informed justice pathways when appropriate.[19]
Adult first diagnosis. Addiction and mental health services often meet undiagnosed FASD — take developmental and PAE history; adapt therapy and housing supports.[20][2]
Pregnancy in a woman with FASD or AUD. Treat alcohol use disorder, offer contraception and preconception counselling, and support parenting capacity assessment without punitive framing that drives care avoidance.[12][10]
Capacity, safeguarding and multiagency care
Capacity is decision-specific. Support decision-making with plain language, visual aids and trusted supporters. Guardianship and mental health statutes are jurisdiction-specific — state principles (support first, least restrictive, best-interests only when capacity lacking for that decision).[2]
Safeguarding interfaces are frequent: parental AUD, neglect, domestic violence, sexual exploitation of vulnerable adolescents, and school exclusion. Report under local child protection / adult safeguarding duties when thresholds are met.[16][12]
Complications and pitfalls
- Missing FASD because the face is normal.[1][2]
- Diagnostic overshadowing: treating only ADHD or conduct problems and ignoring PAE brain injury.[11][14]
- Mother-blame that shuts down accurate history and engagement.[12]
- Inventing a disease-modifying pharmacotherapy for core FASD.[18]
- Premature chronic antipsychotics without behavioural formulation.[17]
- Ignoring secondary disability risk and protective factors identified by Streissguth.[19]
- Forensic interviews without cognitive accommodations.[19]
Prognosis and disposition
FASD is lifelong. Adaptive outcomes vary widely. Protective factors include early diagnosis, stable caregiving free of violence, disability-informed education, and continuous supports into adulthood.[19][16] Disposition is multiagency: health, education, disability funding (e.g. NDIS interface in Australia), housing, and justice diversion when needed. Step intensity to risk and function.[12][18]
Special populations
Intellectual disability co-occurrence. Dual-diagnosis psychiatry skills apply: adapt communication, behaviour plans and capacity assessment; higher medical comorbidity load (Popova).[3][2]
Cultural and Indigenous contexts. Address alcohol-related harm disparities with equity-focused services and cultural safety. Avoid racial essentialism; FASD occurs in all communities where PAE occurs.[12][4]
Women of childbearing age with AUD. Every clinical contact is a prevention opportunity: alcohol treatment, contraception, folate and prenatal care access.[10][12]
Looked-after children. High PAE prevalence in some care populations — low threshold for developmental assessment.[12]
Evidence, guidelines and regional differences
No known safe alcohol level in pregnancy is standard public-health messaging. FRANZCP candidates should apply DSM-aware neurodevelopmental formulation, use multidisciplinary pathways, interface with NDIS/disability supports in Australia and local child protection frameworks, and manage comorbidities with physical-health monitoring. Maternal AUD care is both treatment and prevention.[12][2]
Landmark list to name in viva: Jones and Smith 1973; Astley 4-digit code; Chudley 2005 and Cook 2016 Canadian guidelines; Hoyme 2016; Williams AAP 2015; Lange 2017 global prevalence; May 2018 US communities; Popova 2016 comorbidity and 2017 pregnancy/FAS estimates; Mattson neurobehavioural profile work; Streissguth 2004 secondary disabilities; Famy 1998 adult mental illness; O’Connor and Paley psychiatric conditions; Weyrauch mental comorbidity; Wozniak Lancet Neurology 2019; Flannigan 2020 intervention review; Petrenko systems barriers.[1][2][4][5][18][19]
Prevention
Prevention is the only true disease-modifying strategy for the next generation of alcohol-related fetal brain injury.[10][12]
- Universal message: no known safe amount of alcohol in pregnancy; stop alcohol when planning pregnancy or as soon as pregnancy is recognised.[12][10]
- Targeted treatment of alcohol use disorder in women of reproductive age, with contraception access and non-punitive antenatal care.[10][12]
- Early identification of exposed infants and children to unlock supports that reduce secondary disabilities.[19][16]
- Stigma reduction so women disclose alcohol use and accept help.[12]
Exam pearls
[1] [4] [12] [19]ALCOHOL
Self-test: 9-year-old with ADHD labels, learning failure and possible maternal binge drinking
Take structured PAE history without blame. Plot growth/OFC; examine for sentinel facial features. Request multidisciplinary FASD assessment (neuropsychology, developmental paediatrics). Keep ADHD formulation if criteria met and treat with behavioural + pharmacological pathway carefully. Build school scaffolding and carer coaching. Screen hearing/vision, sleep, mood and safeguarding. Counsel family that early accurate diagnosis is protective. Do not promise a medicine that cures FASD.[1][7][12][19]
References
- [1]Hoyme HE, Kalberg WO, Elliott AJ, et al. Updated Clinical Guidelines for Diagnosing Fetal Alcohol Spectrum Disorders Pediatrics, 2016.PMID 27464676
- [2]Cook JL, Green CR, Lilley CM, et al. Fetal alcohol spectrum disorder: a guideline for diagnosis across the lifespan CMAJ, 2016.PMID 26668194
- [3]Popova S, Lange S, Shield K, et al. Comorbidity of fetal alcohol spectrum disorder: a systematic review and meta-analysis Lancet, 2016.PMID 26777270
- [4]Lange S, Probst C, Gmel G, Rehm J, Burd L, Popova S Global Prevalence of Fetal Alcohol Spectrum Disorder Among Children and Youth: A Systematic Review and Meta-analysis JAMA Pediatr, 2017.PMID 28828483
- [5]May PA, Chambers CD, Kalberg WO, et al. Prevalence of Fetal Alcohol Spectrum Disorders in 4 US Communities JAMA, 2018.PMID 29411031
- [6]Jones KL, Smith DW Recognition of the fetal alcohol syndrome in early infancy Lancet, 1973.PMID 4127281
- [7]Mattson SN, Roesch SC, Fagerlund A, et al.; Collaborative Initiative on Fetal Alcohol Spectrum Disorders (CIFASD) Toward a neurobehavioral profile of fetal alcohol spectrum disorders Alcohol Clin Exp Res, 2010.PMID 20569243
- [8]Mattson SN, Bernes GA, Doyle LR Fetal Alcohol Spectrum Disorders: A Review of the Neurobehavioral Deficits Associated With Prenatal Alcohol Exposure Alcohol Clin Exp Res, 2019.PMID 30964197
- [9]Astley SJ, Clarren SK Diagnosing the full spectrum of fetal alcohol-exposed individuals: introducing the 4-digit diagnostic code Alcohol Alcohol, 2000.PMID 10906009
- [10]Popova S, Lange S, Probst C, Gmel G, Rehm J Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: a systematic review and meta-analysis Lancet Glob Health, 2017.PMID 28089487
- [11]O'Connor MJ, Paley B Psychiatric conditions associated with prenatal alcohol exposure Dev Disabil Res Rev, 2009.PMID 19731386
- [12]Williams JF, Smith VC; Committee on Substance Abuse Fetal Alcohol Spectrum Disorders Pediatrics, 2015.PMID 26482673
- [13]Chudley AE, Conry J, Cook JL, Loock C, Rosales T, LeBlanc N Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis CMAJ, 2005.PMID 15738468
- [14]Weyrauch D, Schwartz M, Hart B, Klug MG, Burd L Comorbid Mental Disorders in Fetal Alcohol Spectrum Disorders: A Systematic Review J Dev Behav Pediatr, 2017.PMID 28460370
- [15]Riley EP, Infante MA, Warren KR Fetal alcohol spectrum disorders: an overview Neuropsychol Rev, 2011.PMID 21499711
- [16]Petrenko CL, Tahir N, Mahoney EC, Chin NP Prevention of secondary conditions in fetal alcohol spectrum disorders: identification of systems-level barriers Matern Child Health J, 2014.PMID 24178158
- [17]Flannigan K, Coons-Harding KD, Anderson T, et al. A Systematic Review of Interventions to Improve Mental Health and Substance Use Outcomes for Individuals with Prenatal Alcohol Exposure and Fetal Alcohol Spectrum Disorder Alcohol Clin Exp Res, 2020.PMID 33119894
- [18]Wozniak JR, Riley EP, Charness ME Clinical presentation, diagnosis, and management of fetal alcohol spectrum disorder Lancet Neurol, 2019.PMID 31160204
- [19]Streissguth AP, Bookstein FL, Barr HM, Sampson PD, O'Malley K, Young JK Risk factors for adverse life outcomes in fetal alcohol syndrome and fetal alcohol effects J Dev Behav Pediatr, 2004.PMID 15308923
- [20]Famy C, Streissguth AP, Unis AS Mental illness in adults with fetal alcohol syndrome or fetal alcohol effects Am J Psychiatry, 1998.PMID 9546004