Psych · intellectual-disability
Intellectual disability: assessment and classification
Also known as Intellectual developmental disorder · IDD · Learning disability UK · Mental retardation historical · Disorders of intellectual development · Global developmental delay · Adaptive functioning assessment
Exam-exhaustive fellowship reference on intellectual disability assessment and classification — DSM-5-TR intellectual developmental disorder and ICD-11 disorders of intellectual development; dual intellectual-plus-adaptive criteria with developmental onset; severity by adaptive function; standardised assessment; aetiological workup (CMA, fragile X, exome, metabolic, imaging red flags); differentials; multiagency services, supported decision-making and premature mortality. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Intellectual disability (ID), also termed intellectual developmental disorder (IDD) in DSM-5-TR and disorders of intellectual development in ICD-11, is a high-yield interface between child, adult, forensic and consultation-liaison psychiatry. Examiners test whether you can apply dual psychometric-adaptive criteria, avoid IQ-only diagnosis, run a rational aetiological workup, and organise multiagency supports while recognising elevated mental illness and premature mortality risk.[1][2][8][9][12][13]
Overview and definition
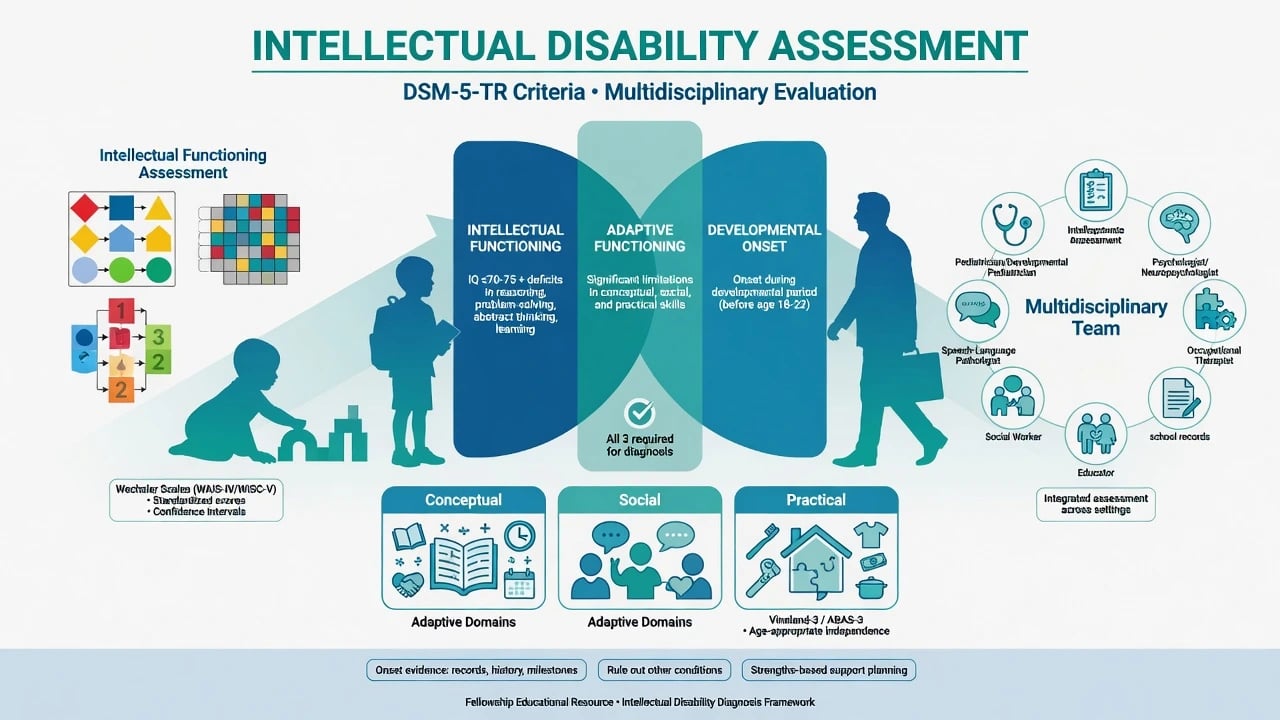
ID/IDD is a neurodevelopmental diagnosis, not a progressive dementia of later life and not a synonym for any behavioural disturbance in someone with low IQ. Core structure across modern manuals is: (1) intellectual functioning deficits (reasoning, problem-solving, planning, abstract thinking, judgment, academic learning, learning from experience) confirmed by clinical assessment and individually administered standardised intelligence testing when valid; (2) adaptive functioning deficits that limit independence and social responsibility in one or more activities of daily life across multiple environments (home, school, work, community); (3) onset during the developmental period (childhood or adolescence; DSM frames developmental period onset, commonly operationalised before adulthood).[2][6][7][8]
Terminology moved from mental retardation to intellectual disability / intellectual developmental disorders for clinical precision and rights-based language; WHO ICD-11 work explicitly reframed the construct as disorders of intellectual development.[9]
AAIDD systems-of-supports model emphasises definition, diagnosis, classification and intensity of supports — not labelling alone. Adaptive behaviour is a measurable construct with conceptual, social and practical domains, not a soft clinical impression.[6][8]
Classification
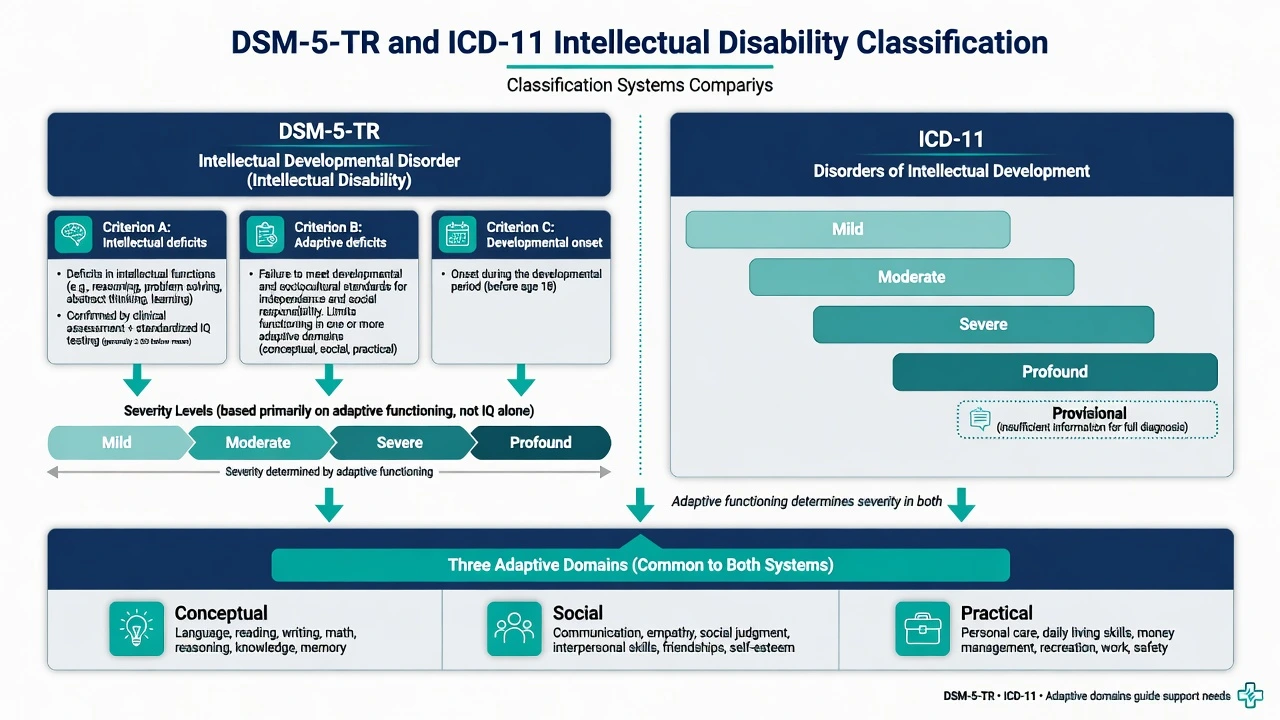
DSM-5-TR: intellectual developmental disorder (intellectual disability)
Criterion A — Intellectual deficits. Confirmed by clinical assessment and standardised IQ testing (typically about 2 standard deviations or more below the population mean, often discussed as IQ approximately 70 plus or minus 5 to allow measurement error). Clinical judgment is required when testing is invalid (language barrier, sensory impairment, severe behaviour, cultural bias).[2][7]
Criterion B — Adaptive deficits. Failure to meet developmental and sociocultural standards for personal independence and social responsibility. Limitations appear in conceptual (language, reading, writing, maths, memory, knowledge), social (empathy, social judgment, communication, friendship), and/or practical (self-care, money, recreation, work, safety) domains.[6][7]
Criterion C — Developmental onset. Symptoms begin during the developmental period.[2][8]
Severity levels (mild, moderate, severe, profound) are defined primarily by adaptive functioning, not by IQ bands. This is a classic exam trap: quoting only IQ cut-offs for severity fails modern criteria.[7][8]
ICD-11: disorders of intellectual development
ICD-11 codes disorders of intellectual development with severity (mild, moderate, severe, profound) and allows a provisional designation when information is incomplete — useful in acute settings or when standardised testing cannot yet be completed. Adaptive behaviour again determines severity classification in practice.[9]
Related constructs examiners distinguish
| Construct | Key discriminator from ID |
|---|---|
| Global developmental delay (GDD) | Age typically under 5 years when reliable standardised testing of intelligence is not yet possible; reassess and convert diagnosis when testing becomes valid |
| Borderline intellectual functioning | Intellectual scores in the low-average/borderline range without meeting the adaptive-deficit threshold for ID |
| Specific learning disorder | Academic domain deficits with adaptive functioning otherwise generally age-appropriate outside literacy/numeracy demands |
| Acquired neurocognitive disorder | Onset after the developmental period (e.g. adult TBI, dementia) — not ID |
Epidemiology and risk factors
Headline ID numbers for exams
A meta-analysis of population-based studies estimated overall prevalence of intellectual disability on the order of about 1 percent, with variation by study design, age group and income setting; mild ID predominates numerically.[1] Rates are higher in socioeconomically disadvantaged populations, with complex contributions from perinatal care, nutrition, consanguinity patterns in some regions, ascertainment and educational systems.[1]
Comorbidity burden is central to psychiatry practice: mental ill-health is substantially more common in adults with ID than in the general population, with associated factors including severity of disability, life events and physical health.[12] Children and adolescents with ID also show high rates of mental health problems in systematic reviews.[16] Epilepsy, sensory impairment, and multi-system genetic syndromes cluster especially with more severe ID.[2][5]
Premature mortality is a systems-level exam pearl. The UK Confidential Inquiry into premature deaths of people with intellectual disabilities (CIPOLD) demonstrated elevated premature death with a substantial proportion potentially avoidable — failures of health care access, delayed diagnosis, and diagnostic overshadowing of physical illness.[13]
Pathophysiology and aetiology
ID reflects heterogeneous disruption of early brain development. Genetic architecture includes chromosomal aneuploidy (e.g. Down syndrome), copy-number variants detectable by chromosomal microarray, X-linked disorders (fragile X), recessive metabolic and monogenic syndromes, and de novo sequence variants — a paradigm established in severe ID sequencing studies.[5][10][11] Environmental and acquired contributors include extreme prematurity, hypoxic-ischaemic injury, congenital infection, fetal alcohol exposure, postnatal meningitis/encephalitis and severe head injury during the developmental period.[2][14]
A larger identifiable genetic yield is expected in moderate-severe-profound ID and in those with congenital anomalies, epilepsy or dysmorphic features; mild ID more often remains without a single molecular diagnosis after first-line testing, though modern sequencing continues to expand yields.[5][10][18]
Clinical presentation
Early childhood. Delayed motor or language milestones, reduced learning from experience, limited play complexity, dependency beyond age expectations. GDD is often the working label before reliable IQ testing.[2][4]
School age (classic mild ID presentation). Academic failure despite opportunity, concrete thinking, difficulty with abstract curriculum, social naivety, practical skill gaps (money, time, organisation). May be missed if social strengths and family scaffolding mask adaptive deficits until demands rise.[6][8]
Moderate to profound. Earlier recognition; limited or non-verbal communication; high continuous support needs for personal care and safety; behaviour may communicate pain, unmet needs or psychiatric comorbidity rather than "personality."[2][12]
Adult presentation to general psychiatry. Longstanding undiagnosed mild ID may surface as repeated service contact, exploitation, forensic vulnerability, or treatment non-adherence misread as wilful. Always seek developmental and educational history.[8][12]
MSE adaptations. Use plain concrete language; allow processing time; offer visual supports or AAC; obtain carer collateral; interpret "odd" answers against developmental level; do not equate limited verbal output with psychosis without careful form-versus-content analysis.[12][17]
Differential diagnosis
Win differentials on onset timing, adaptive breadth, academic specificity, and co-occurring social-communication pattern — not shopping lists.[2][8]
- ASD: dual diagnosis is allowed. ASD requires social-communication deficits and restricted/repetitive behaviours beyond what developmental level alone predicts; ID alone does not produce the RRB pattern of ASD.[2]
- Specific learning disorder: narrow academic impairment; adaptive function outside school often preserved relative to ID.
- Language disorder / hearing loss: can mimic intellectual limits — always check audiology.[2][4]
- Borderline intellectual functioning: supports may still be needed; diagnostic threshold for ID not met.
- Severe psychosocial deprivation: can suppress skills; reassess after environmental remediation.
- Adult-onset cognitive decline: dementia or ABI after developmental period is not ID.[8]
Bedside assessment
History structure. Pregnancy and birth; neonatal course; developmental milestones; regression; seizures; vision/hearing; education trajectory and statements of special need; adaptive skills by domain; family history of ID, epilepsy, consanguinity, recurrent miscarriage; trauma, abuse and exploitation risk; medication and substance exposure.[2][14]
Collateral. Parents/carers, school reports, previous psychology assessments, disability support plans — multi-informant history is essential because adaptive function must be sampled across settings.[2][6]
Intellectual testing. Individually administered, culturally and linguistically appropriate instruments (e.g. Wechsler scales) by a qualified psychologist. Report full-scale and index scores with confidence intervals; document threats to validity.[2][7]
Adaptive assessment. Standardised tools (e.g. Vineland Adaptive Behavior Scales, ABAS) sampling conceptual, social and practical domains across settings — essential for diagnosis and severity.[6][7]
Risk and capacity. Screen for abuse, neglect, financial and sexual exploitation, self-harm, aggression, and decision-specific capacity with supported decision-making preference. Do not declare global incapacity from the ID label alone.[8][13]
Psychiatric screen. Depression, anxiety, psychosis, ADHD, ASD and trauma presentations are common and often atypical — avoid diagnostic overshadowing.[12][16][17]
Investigations
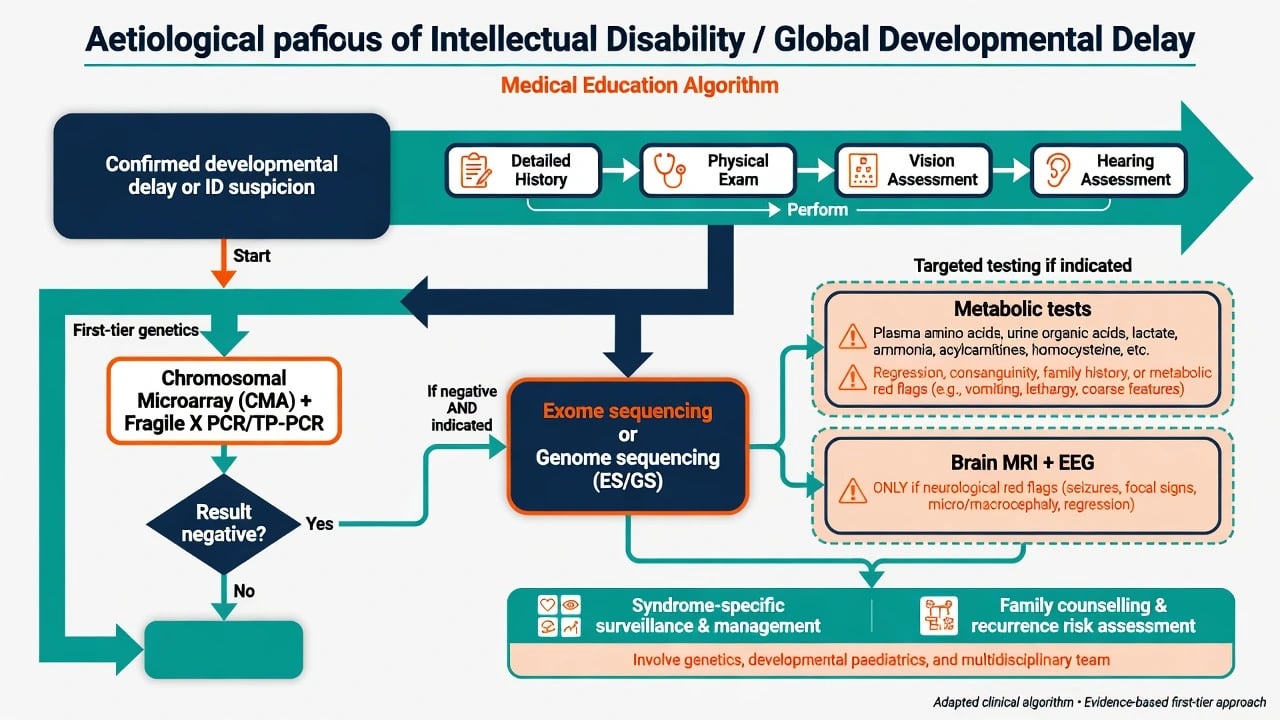
Aetiological evaluation follows clinical diagnosis of delay or ID, not the reverse.[2][4]
- Universal basics: vision and hearing assessment; growth parameters including head circumference; full physical and neurological examination for dysmorphism, neurocutaneous signs, organomegaly.[2][14]
- First-tier genetics: chromosomal microarray (CMA) is a first-tier diagnostic test for developmental disabilities/ID in consensus guidance, with substantially higher diagnostic yield than G-banded karyotype alone for unexplained ID.[3] Fragile X testing is recommended in the evaluation pathway, particularly given X-linked inheritance counselling implications.[2][14]
- Next-tier sequencing: diagnostic exome (and increasingly genome) sequencing has established yield in severe ID (de Ligt NEJM) and is integrated after or alongside first-tier tests depending on local pathways and phenotype urgency.[10][18]
- Metabolic testing: not shotgun in every mild ID; target when regression, episodic encephalopathy, consanguinity, suggestive family history, or other metabolic red flags — treatable intellectual developmental disorders must not be missed.[15]
- MRI / EEG: for neurological red flags (seizures, focal signs, progressive head-size change, regression, abnormal examination) — not routine fishing in uncomplicated mild ID.[2][4]
Acute management
Acute behavioural crisis is medical until proven otherwise: pain (including dental and constipation), infection, seizure, medication toxicity, delirium, environmental overload. De-escalate, reduce sensory load, use least restrictive safe setting, and involve familiar carers. Safeguarding if abuse/neglect is possible. Emergency treatment decisions use local capacity and mental health law with supported decision-making and least restrictive principles.[12][13][17]
Definitive management and services
There is no medication that treats core intellectual disability. Disease-modifying therapy applies only to rare treatable metabolic or other specific aetiologies once identified.[2][15]
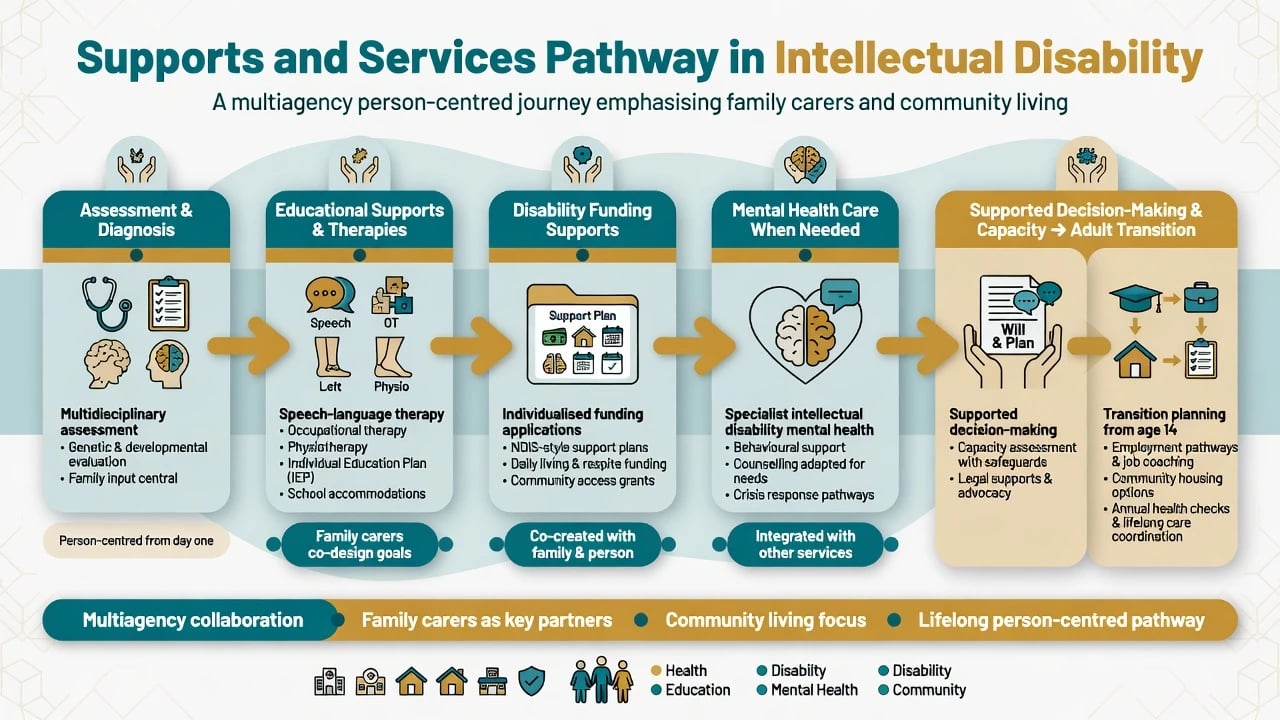
Foundational package. Educational supports and individual education planning; speech-language therapy; occupational therapy; physiotherapy as needed; alternative and augmentative communication; positive behaviour support and carer training; disability support funding and community living supports (in Australia, NDIS eligibility and planning; in the UK, learning disability services and annual health checks); vocational training, day activity, housing and transport matched to adaptive level; and family carer support and respite.[2][8]
Health action. Active physical health surveillance, vaccination, dental care, epilepsy management, and low threshold for investigating new symptoms — CIPOLD makes this an ethical and exam imperative.[13]
Mental health care. Treat comorbid mental illness with adapted communication, formulation that includes developmental level, and careful psychotropic use only when indicated (companion psychiatric-disorders-in-ID topic). Diagnostic overshadowing is an explicit failure mode.[12][17]
ANZ: NDIS support planning; state disability and specialist ID mental health services; RANZCP interfaces with developmental disability psychiatry. Capacity law is jurisdiction-specific (e.g. guardianship and mental health acts) — speak in principles (decision-specific capacity, supported decision-making, least restrictive) rather than inventing section numbers. UK / MRCPsych: "Learning disability" terminology still used in services; NICE guidance on mental health problems in people with learning disabilities; annual health checks; CIPOLD and subsequent LeDeR programme as systems evidence. US / ABPN: IDEA educational supports; AAIDD definition widely cited; Medicaid waiver/support systems vary by state; DSM-5-TR severity language. India / MD-DNB: Resource-variable genetic testing access; emphasise clinical diagnosis, treatable causes, family counselling, and multi-tier service mapping.[8][13]
Subtypes and scenarios
- Preschool GDD: milestone lag; start sensory and first-tier workup; early intervention without waiting for a final IQ number.[2][4]
- School-age mild ID: dual IQ + adaptive testing; education plan; screen ASD/ADHD/anxiety.[2][8]
- Severe/profound ID: early genetics yield higher; communication and health surveillance dominate; behaviour as communication.[5][10]
- Adult first recognition: reconstruct developmental history; adaptive assessment; capacity and exploitation risk.[8][12]
- ID + epilepsy: coordinated neurology-psychiatry care; medication cognitive adverse effects matter.[2]
- ID + ASD: dual criteria; sensory and communication-first approaches.[2][16]
- Transition to adult services: plan from mid-adolescence — health, housing, work, decision-making supports, mental health handover.[8][13]
Complications and pitfalls
- IQ-only diagnosis without adaptive data.[7]
- Diagnostic overshadowing — classic Reiss construct: symptoms misattributed to ID, delaying mental or physical diagnosis.[17]
- Cultural and language bias on testing producing false-positive ID labels.
- Missing treatable metabolic disease by skipping red-flag metabolic evaluation.[15]
- Over-medication of behaviour without functional analysis or mental illness diagnosis.
- Normalising early death instead of fixing care pathways (CIPOLD).[13]
Prognosis and disposition
ID is lifelong, but adaptive outcomes are highly modifiable by education, communication supports, physical health care, mental health treatment and social inclusion.[8] Mild ID often permits semi-independent living with intermittent supports; severe and profound ID usually requires continuous support with quality-of-life and dignity goals. Disposition prefers community-based care; specialist intellectual disability psychiatry when mental illness, complex behaviour or forensic interface exceeds general service skill.[8][12]
Special populations
- Children: GDD pathway, family-centred early intervention, education law interfaces.[2]
- Adults: undiagnosed mild ID, dual diagnosis services, employment and tenancy supports.[8][12]
- Ageing: earlier multimorbidity; Down syndrome dementia risk is a cross-link topic.[8][13]
- Women: reproductive health, parenting assessments, capacity for obstetric decisions.[8]
- Forensic: suggestibility, fitness, vulnerability — assessment of intellectual and adaptive function is pivotal.[8]
- Cultural diversity: interpreters, non-biased testing, Indigenous service models.[8][13]
Evidence and guidelines
Name these in viva without notes: Maulik 2011 prevalence meta-analysis (~1%); Moeschler and Shevell 2014 (AAP Pediatrics) comprehensive evaluation of ID/GDD; Miller 2010 AJHG CMA as first-tier test; Shevell 2003 Neurology practice parameter for GDD evaluation; Vissers genetic architecture and de novo paradigm; de Ligt 2012 NEJM diagnostic exome in severe ID; Tassé / Schalock / Luckasson adaptive behaviour and AAIDD definition-supports framework; Salvador-Carulla 2011 ICD-11 intellectual developmental disorders framing; Cooper 2007 adult mental ill-health prevalence; Heslop CIPOLD 2014 Lancet premature, often avoidable deaths.[1][2][3][4][5][6][7][8][9][10][11][12][13]
Exam pearls
ID triad
- Severity = adaptive support need, not IQ band alone.[7]
- Under 5 with broad delay = think GDD, then reclassify when testing valid.[2][4]
- Genetics phrase: CMA + fragile X first-tier; exome when indicated.[2][3][10]
- No tablet for core ID.[2]
- Overshadowing misses treatable illness — examine, investigate, formulate.[17]
- CIPOLD: premature avoidable death is a systems answer, not trivia.[13]
- Capacity is decision-specific; support decision-making.[8]
References
- [1]Maulik PK, Mascarenhas MN, Mathers CD, Dua T, Saxena S Prevalence of intellectual disability: a meta-analysis of population-based studies Res Dev Disabil, 2011.PMID 21236634
- [2]Moeschler JB, Shevell M; Committee on Genetics Comprehensive evaluation of the child with intellectual disability or global developmental delays Pediatrics, 2014.PMID 25157020
- [3]Miller DT, Adam MP, Aradhya S, et al. Consensus statement: chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies Am J Hum Genet, 2010.PMID 20466091
- [4]Shevell M, Ashwal S, Donley D, et al.; Quality Standards Subcommittee of the American Academy of Neurology; Practice Committee of the Child Neurology Society Practice parameter: evaluation of the child with global developmental delay Neurology, 2003.PMID 12578916
- [5]Vissers LE, Gilissen C, Veltman JA Genetic studies in intellectual disability and related disorders Nat Rev Genet, 2016.PMID 26503795
- [6]Tassé MJ, Schalock RL, Balboni G, et al. The construct of adaptive behavior: its conceptualization, measurement, and use in the field of intellectual disability Am J Intellect Dev Disabil, 2012.PMID 22809075
- [7]Tassé MJ, Luckasson R, Schalock RL The Relation Between Intellectual Functioning and Adaptive Behavior in the Diagnosis of Intellectual Disability Intellect Dev Disabil, 2016.PMID 27893317
- [8]Schalock RL, Luckasson R, Tassé MJ An Overview of Intellectual Disability: Definition, Diagnosis, Classification, and Systems of Supports (12th ed.) Am J Intellect Dev Disabil, 2021.PMID 34700345
- [9]Salvador-Carulla L, Reed GM, Vaez-Azizi LM, et al. Intellectual developmental disorders: towards a new name, definition and framework for "mental retardation/intellectual disability" in ICD-11 World Psychiatry, 2011.PMID 21991267
- [10]de Ligt J, Willemsen MH, van Bon BW, et al. Diagnostic exome sequencing in persons with severe intellectual disability N Engl J Med, 2012.PMID 23033978
- [11]Vissers LE, de Ligt J, Gilissen C, et al. A de novo paradigm for mental retardation Nat Genet, 2010.PMID 21076407
- [12]Cooper SA, Smiley E, Morrison J, Williamson A, Allan L Mental ill-health in adults with intellectual disabilities: prevalence and associated factors Br J Psychiatry, 2007.PMID 17197653
- [13]Heslop P, Blair PS, Fleming P, Hoghton M, Marriott A, Russ L The Confidential Inquiry into premature deaths of people with intellectual disabilities in the UK: a population-based study Lancet, 2014.PMID 24332307
- [14]Moeschler JB; American Academy of Pediatrics Committee on Genetics Clinical genetic evaluation of the child with mental retardation or developmental delays Pediatrics, 2006.PMID 16740881
- [15]van Karnebeek CD, Shevell M, Zschocke J, Moeschler JB, Stockler S The metabolic evaluation of the child with an intellectual developmental disorder: diagnostic algorithm for identification of treatable causes and new digital resource Mol Genet Metab, 2014.PMID 24518794
- [16]Totsika V, Liew A, Absoud M, Adnams C, Emerson E Mental health problems in children with intellectual disability Lancet Child Adolesc Health, 2022.PMID 35421380
- [17]Reiss S, Szyszko J Diagnostic overshadowing and professional experience with mentally retarded persons Am J Ment Defic, 1983.PMID 6829617
- [18]Waggoner D, Wain KE, Dubuc AM, et al. Yield of additional genetic testing after chromosomal microarray for diagnosis of neurodevelopmental disability and congenital anomalies: a clinical practice resource of the American College of Medical Genetics and Genomics (ACMG) Genet Med, 2018.PMID 29915380