Psych · intellectual-disability
Offending and intellectual disability
Also known as Offenders with intellectual disability · Dual disability forensic · Learning disability and crime · Forensic intellectual disability · Intellectual disability criminal justice · ID and offending · Developmental disability justice pathway
Exam-exhaustive fellowship reference on offending and intellectual disability — prevalence method traps, offence patterns, victimisation overlap, suggestibility and fitness interfaces, dual diagnosis, adapted risk assessment, RNR-informed treatment, diversion and custody care. Statutes are jurisdiction-specific; no invented section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
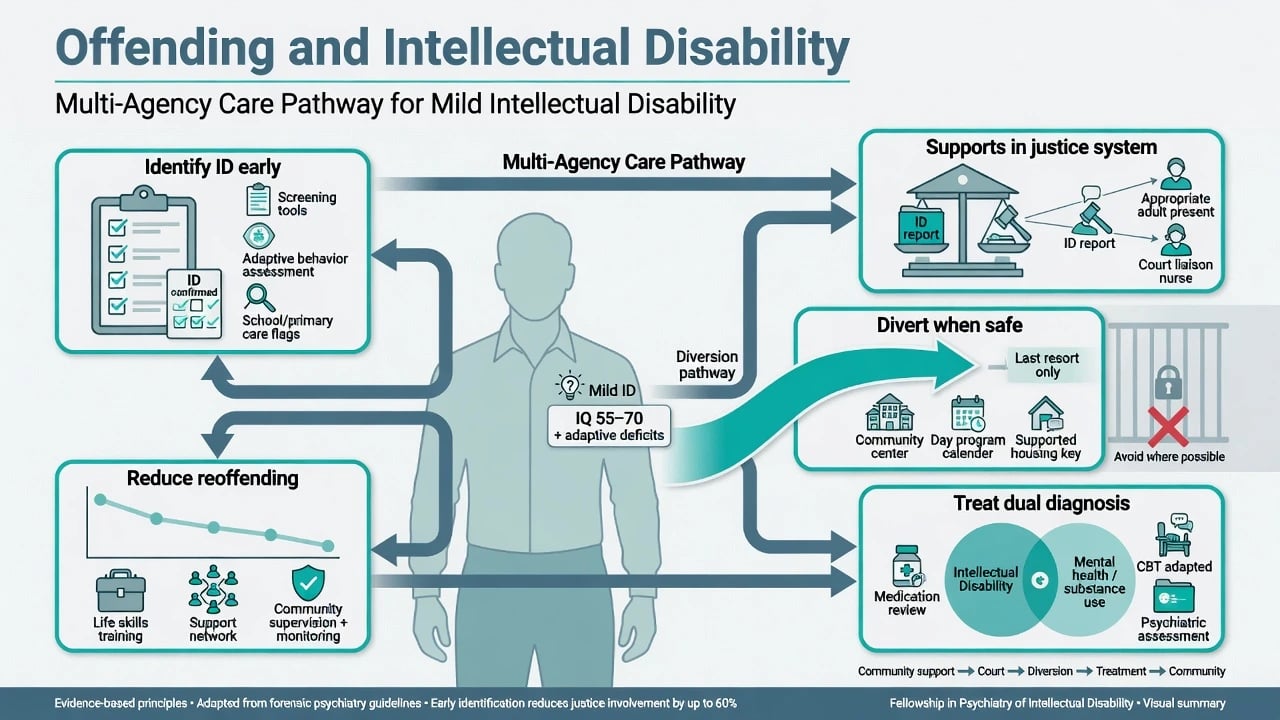
Offending and intellectual disability is a high-yield dual-disability interface for FRANZCP, MRCPsych and forensic stations. Examiners test whether you inflate prevalence from bad methods, whether you can separate challenging behaviour from crime, and whether you can run a rights-based pathway through police, court, diversion, community forensic care and custody without inventing statute numbers.[1][2][4]
Definition and classification
Intellectual disability (DSM-5-TR / ICD-11 intellectual developmental disorder concepts) requires deficits in intellectual and adaptive functioning with onset during the developmental period. Severity is guided more by adaptive needs than by a single IQ number. Borderline intellectual functioning and specific learning disorders are adjacent but not equivalent; justice settings often conflate all three under “slow” labels.[1][2]
“Offender with intellectual disability” and dual disability are service and research constructs, not freestanding diagnoses. They describe people who meet ID criteria (or closely related cognitive-adaptive impairment) and come into contact with the criminal justice system (CJS) as alleged or convicted offenders. Forensic intellectual disability psychiatry sits at the intersection of developmental disability, general adult psychiatry, and forensic risk work.[4][5]
Critical distinctions examiners expect — challenging behaviour is not a conviction; fitness is present-state trial participation; criminal responsibility is mental state at the alleged offence; none equals a global “ID means not guilty” label.[1][10]
| Construct | What it is | What it is not |
|---|---|---|
| Challenging behaviour | Service description of risk/impact | A criminal conviction |
| Alleged offence | Legal allegation under investigation | Proof of guilt or of mental disorder |
| Conviction / finding | Legal outcome under local process | A diagnosis of ID |
| Fitness / competence | Present-state ability to participate in trial | Retrospective criminal responsibility |
| Criminal responsibility | Mental state at time of alleged offence | Global “ID = not guilty” |
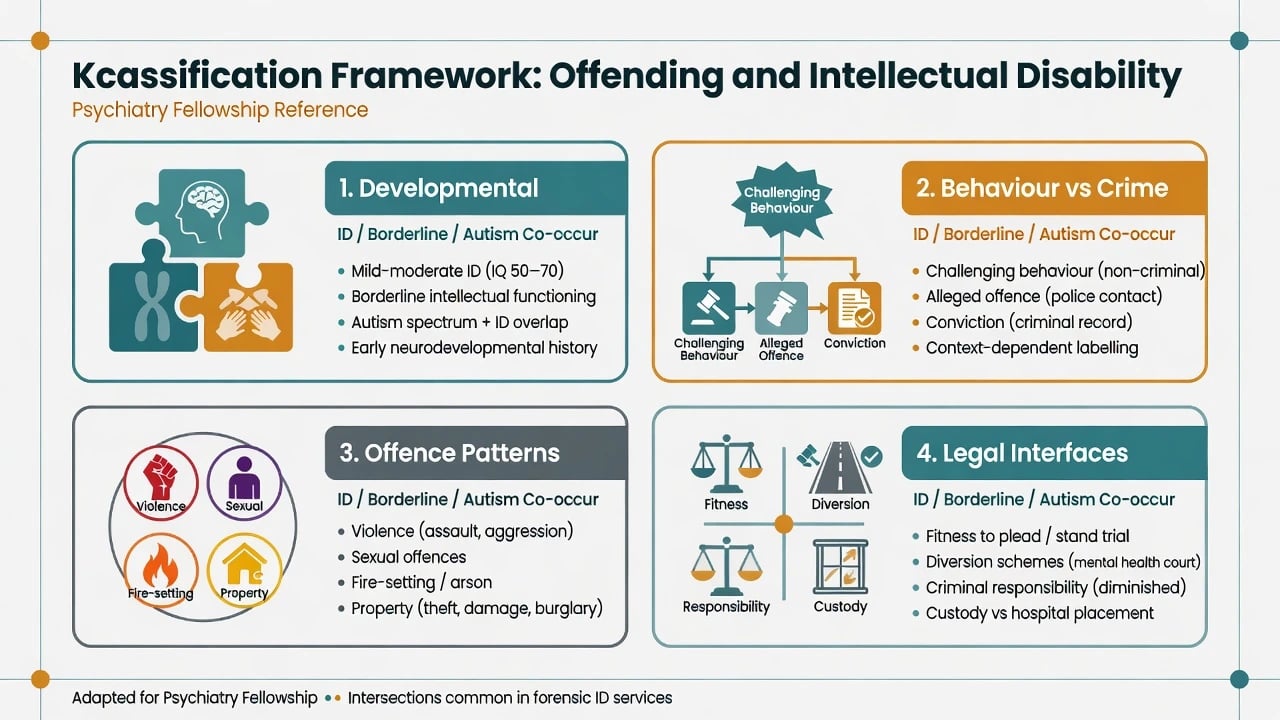
Offence topographies discussed in ID samples include violence/aggression, sexual offences, fire-setting/arson, property, and public order. Referred forensic samples over-represent sexual and fire-setting pathways relative to general population crime mix; that is a referral and detection pattern, not proof that ID “causes” unique crimes.[2][5][15]
Epidemiology and risk
Prevalence claims are the classic exam trap. Systematic reviews show wide methodological scatter: definition of ID (IQ cut-off only vs adaptive criteria), sampling frame (community ID services vs police vs courts vs prisons), and definition of “offending” (allegation vs charge vs conviction) drive the numbers.[1][2]
Holland, Clare and Mukhopadhyay synthesised evidence that significantly below-average intellectual ability associates with some future offending risk when IQ is treated continuously, yet absolute rates of formal offending among people known to ID services remain relatively low, with annual CJS contact often discussed in a low single-digit percent range among service-known groups depending on study design. The clinical takeaway is dual: do not deny risk where it exists, and do not claim that “most people with ID offend.”[1]
Simpson and Hogg’s two-part systematic review mapped prevalence and predisposing factors across heterogeneous studies, reinforcing caution about pooling crude rates and highlighting social and developmental risk clustering rather than a simple ID-to-crime causal arrow.[2][3]
Prison prevalence. In a systematic review of approximately 12,000 prisoners, Fazel, Xenitidis and Powell found that typically about 0.5–1.5% of prisoners were diagnosed with intellectual disability (study range lower to a few percent). Screening tools and broader “learning difficulty” definitions yield higher rates of cognitive vulnerability without meeting full ID criteria. Under-ascertainment is common; over-claiming “30% of prisoners have ID” usually confuses screening positives with diagnosed ID.[6][8]
Australian prison data show that when ID is identified, co-occurring mental disorder is common, and international reviews highlight substantial physical and mental health comorbidity among prisoners with ID — dual diagnosis is the rule for service planning, not the exception.[7][8]
Clinical referred samples. Barron and colleagues found that offenders with ID often start problem behaviour early, accumulate multiple offence types, and show relatively high rates of sex offending and arson in specialist cohorts; therapeutic outcome literature remains limited and service-dependent.[4][5]
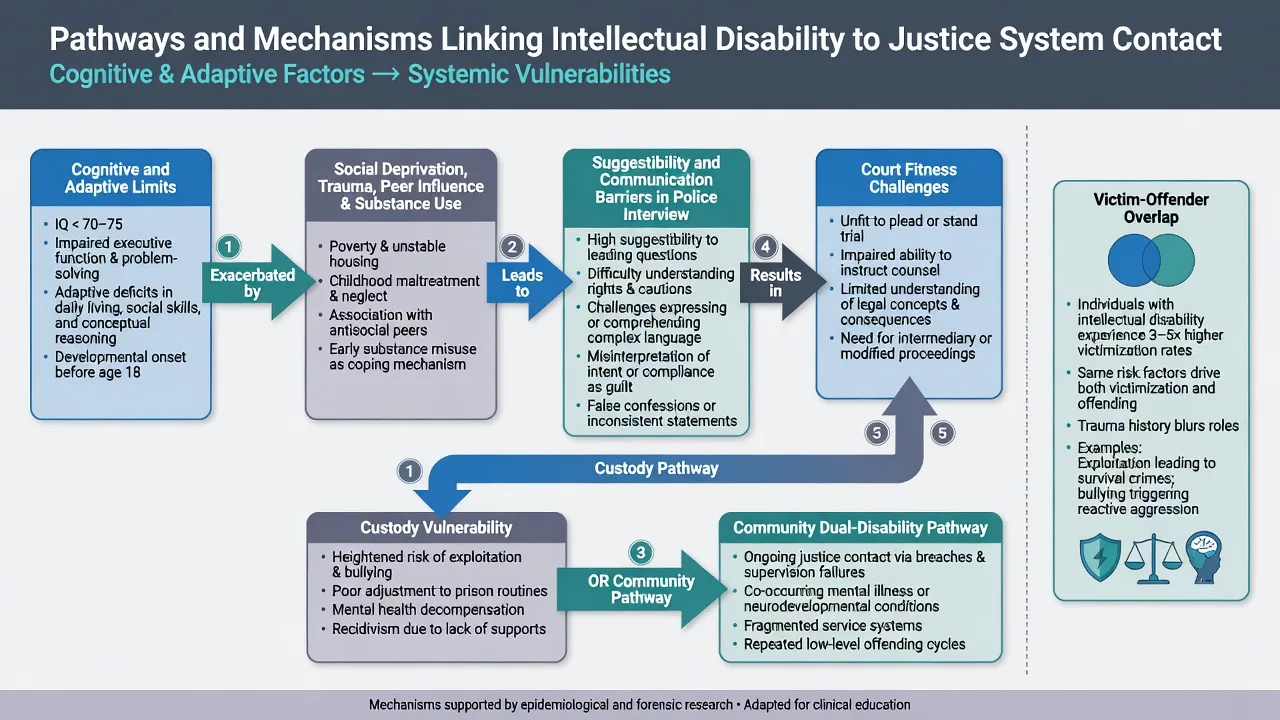
Population bidirectional risk. A large population study by Latvala and colleagues associated intellectual disability with elevated risk of violent and sexual crime and with elevated victimisation — the same person may be both offender and victim across the life course. Always assess both roles.[17]
Aggressive behaviour in community ID samples is common as a service concern (Crocker et al. prevalence work), but aggression is not synonymous with criminal prosecution; service response (police called vs PBS plan) shapes the “offender” label.[18]
Viva numbers to keep honest
Risk markers (criminogenic and clinical). Male sex; young adulthood; childhood conduct problems; substance use; ADHD; autism co-occurrence; family disruption and trauma/abuse history; social deprivation and unemployment; antisocial peers; limited supervision; communication impairment; sexual knowledge gaps; and prior CJS contact. These are needs for intervention, not moral verdicts.[3][5][15]
Mechanisms and pathways
Examiners want a cognitive-social learning + vulnerability model, not a single gene or IQ slogan.[3]
Criminogenic needs (antisocial attitudes, associates, substance use, poor problem-solving, unstable housing/work patterns) operate in people with ID as in other populations. The responsivity difference is how interventions are delivered: concrete language, visual supports, longer programmes, behavioural rehearsal, and family/support-worker generalisation.[4][16]
Cognitive-adaptive mediators. Limited consequential thinking, executive dysfunction, concrete interpretation of rules, and social-cognitive difficulties can increase impulsive or poorly planned acts and reduce ability to exit peer-driven scenarios.[3]
Suggestibility, acquiescence and confabulation. Clare and Gudjonsson demonstrated elevated interrogative suggestibility, confabulation and acquiescence in people with mild learning disabilities — with direct implications for the reliability of police interviews and risk of false or contaminated statements. This is a core fellowship pearl for CASC and viva.[9]
System pathway. Unrecognised mild ID → complex interview → apparent “confession” → court without fitness supports → custody without dual-disability care. Parallel pathway: aggression maintained by escape/attention functions → police called repeatedly → criminalisation of service failure.[1][9][18]
Clinical presentation
Typical exam stems include mild ID with fluent short-phrase speech and unrecognised adaptive deficits under legal complexity; co-defendant pressure (“told me to say I did it”); sexualised behaviour framed only as staff management; fire interest with sensory or attention function versus planned arson; remand isolation after “behaviour” with medication stopped; and a parent demanding an “unfit” certificate based on IQ alone — each requires multi-source history and suggestibility-aware interview practice.[5][9][10]
MSE must be adapted: communication method, literacy, anxiety under authority figures, yes-saying, and capacity for each legal task. Collateral from disability support, family, school/work, and prior assessments is mandatory before final opinions.[9][10]
Differential diagnosis
Developmental
- ID with adaptive deficits and developmental onset
- Borderline intellectual functioning without full ID
- Autism with or without ID
- FASD cognitive-behavioural phenotype
Acquired / organic
- TBI after developmental period
- Epilepsy-related behavioural change
- Early dementia in older adults with ID
- Delirium / intoxication on presentation
Psychiatric dual diagnosis
- Psychosis or mania driving index offence
- Substance-induced aggression
- PTSD and trauma-related dysregulation
- ADHD impulsivity contributing to risk
Personality / social
- Antisocial traits vs ID-related impulsivity
- Peer exploitation and compliance
- Retaliatory violence after victimisation
- Malingering low effort vs true limitation
Assessment
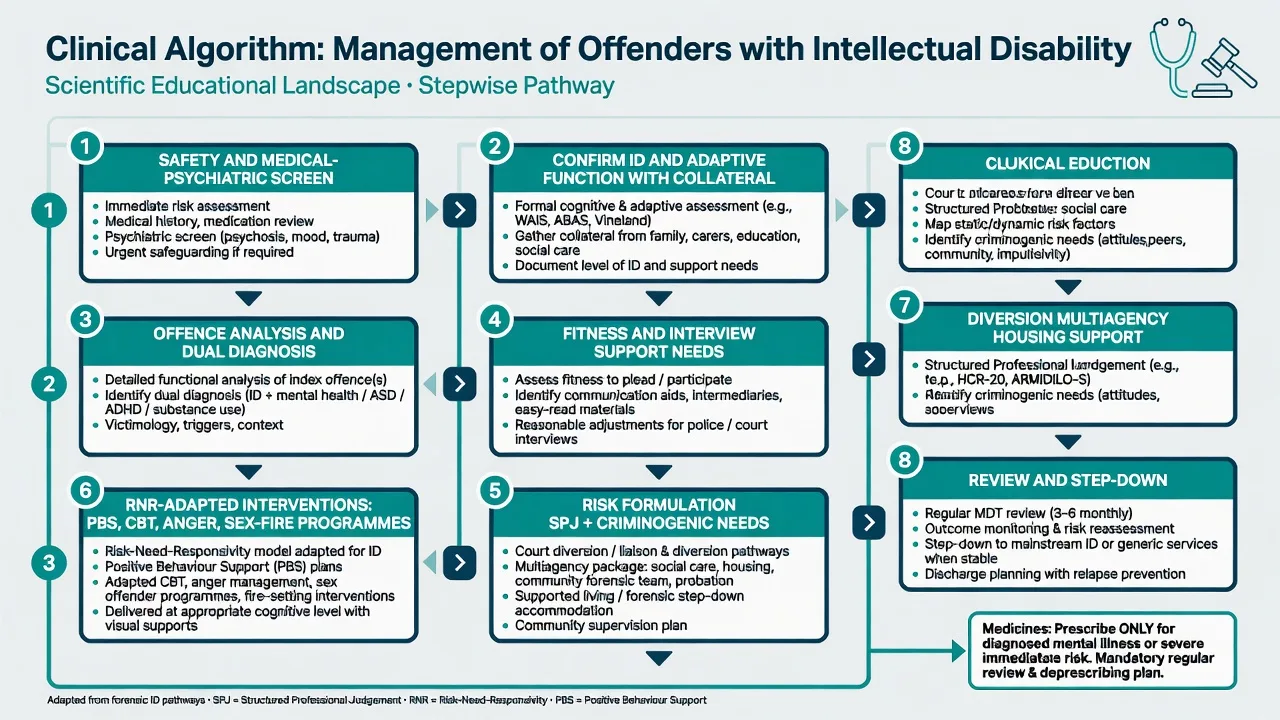
1. Confirm developmental disability properly. Developmental history; adaptive functioning (Vineland/ABAS-type concepts); cognitive testing when indicated; hearing/vision; communication profile. Do not diagnose ID from a single prison IQ screen alone.[1][6]
2. Offence analysis (multi-source). Index allegations, prior history, victim statements, CCTV, staff logs, substance use at the time, peer context, and offence-paralleling behaviour in the current environment. Self-report alone is insufficient, especially with suggestibility risk.[5][9][15]
3. Interview vulnerability. Screen for need for communication supports, intermediary/Appropriate Adult principles (local schemes vary — do not invent procedures), and risk of acquiescence. Document how information was explained and whether teach-back was possible.[9]
4. Fitness / competence to stand trial. Present-state functional abilities mapped to the local legal standard (Pritchard/Presser/Dusky-type principles): understand proceedings, instruct counsel, decide plea, follow evidence. IQ is not the test. AAPL competence guidance and restoration literature for persons with intellectual disability (Wall et al. training programme model) support structured, teachable knowledge deficits as potentially restorable.[10]
5. Criminal responsibility interface. Separate from fitness. Mental state at the time of the alleged offence under local insanity/mental impairment tests. ID alone rarely equates to legal insanity without additional severe impairment of understanding or control as defined locally. No invented section numbers.[10]
6. Risk formulation. Use structured professional judgment concepts (historical-clinical-risk frameworks) plus criminogenic needs. Meta-analytic evidence shows risk instruments have limited positive predictive value even in general forensic samples; high-risk bands still contain many non-recidivists. Apply tools with humility, ID-appropriate language, and protective factors — instruments inform, they do not decide liberty alone.[11][12][13][14]
7. Safeguarding dual role. Assess ongoing victimisation, sexual exploitation, financial abuse, and whether the person is safer as a “defendant” narrative that hides a victim pathway.[17]
Investigations
There is no “offending panel.” Investigate to answer clinical questions: substance screen when relevant; epilepsy evaluation if indicated; medical causes of behavioural change; neurodevelopmental assessment for autism/ADHD; baseline metabolic parameters and ECG before psychotropics if medicines are considered for a diagnosed mental illness. Neuropsychology is adjunctive for contested fitness when time and consent allow.[7][10]
Acute management
Definitive management
Risk–Need–Responsivity adapted for ID
- Risk: intensity of service matches reoffending risk (higher risk gets more intensive multiagency intervention).
- Need: target criminogenic needs (substance use, antisocial peers/attitudes, problem-solving, sexual risk pathways, fire interest, instability of supports).
- Responsivity: this is the ID-specific lever — simplify language, use visual materials, shorter sessions with more repetition, behavioural practice, support-worker involvement, and longer programme duration.[4][15][16]
Psychological and behavioural interventions
For mild-to-moderate ID with anger-related aggression, group-based cognitive-behavioural anger management improved anger control in a cluster randomised trial (Willner et al.) — useful when cognitive access allows adapted CBT, not as a substitute for environmental redesign in profound ID.[16]
Specialist adapted sex-offender and fire-setting programmes (Lindsay and related dual-disability service literature) emphasise concrete sexual knowledge/consent education, offence chains in plain language, relapse prevention that support workers can implement, and long follow-up. Sexual and nonsexual offender pathways differ in referral pattern and treatment focus; do not run a generic “ID offender group” without offence-specific analysis.[15][4]
Where behaviour is primarily function-maintained and criminalised by repeated police callouts, positive behaviour support and placement redesign may reduce justice contact more than custody or open-ended medication.[18]
Pharmacotherapy principles
Medicines treat diagnosed mental illness (psychosis, mania, severe depression, ADHD when indicated) or, rarely, time-limited severe risk after non-drug optimisation — not “offending” itself. If an antipsychotic is used for residual severe aggression after PBS and medical exclusion, name the target risk, start low in sensitive adults with ID, monitor metabolic and EPS effects, set a review/stop date, and document consent/capacity process. Avoid open-ended chemical restraint for offence history alone.[7][16]
Diversion, community dual disability, and custody
Community forensic dual-disability teams, court liaison, probation partnerships, housing with skill-matched support, and day structure are recidivism-relevant. Diversion schemes are jurisdiction-specific — describe principles (identify ID early, divert from custody when risk allows, ensure treatment equivalence) without inventing local forms.[4][6]
In custody, apply equivalence of care: reception screening for cognitive vulnerability, continuity of psychotropics, protection from bullying, accessible communication, and planned release transition. Comorbidity data from Australian and international prison studies justify integrated mental health and disability support rather than behaviour-only management.[6][7][8]
Fitness restoration
When unfitness is driven by lack of legal knowledge and skills rather than untreatable profound impairment, structured education programmes for persons with intellectual disability can restore trial competence in selected cases (Wall et al. model). Reassess functionally against the legal test after training.[10]
Australia/NZ practice note. Dual disability and justice pathways vary by state and territory. Emphasise early identification in police and court liaison services, NDIS behaviour support interfaces for community risk, prison reception screening for cognitive disability (Dias et al. Australian sample teaching point), and cultural safety for Aboriginal and Torres Strait Islander defendants. Fitness and mental impairment tests are jurisdiction-specific — use Presser-type principles language without invented sections.[7][10]
Subtypes and scenarios
Sexual offending with ID. Distinguish sexual knowledge/consent deficits and opportunity structures from deviant interest patterns and from peer-coerced participation. Use multi-source assessment and adapted treatment intensity matched to risk.[15]
Fire-setting. Assess function (attention, sensory, anger, instrumental), access to ignition materials, and prior fires. Combine offence-specific work with environmental control and support-worker plans.[5]
Violence with dual diagnosis. Treat active psychosis or mania first; do not attribute all violence to “ID.” Then address residual criminogenic needs.[7]
Victim–offender overlap. Person charged after retaliatory aggression may primarily be a victim of exploitation; safeguarding plan is part of risk management.[17]
Youth transition. Mild ID at school exit with peer-driven theft or sexual boundary problems needs education, family work, and early diversion — not automatic adult forensic trajectory.[3]
Complications and pitfalls
- Diagnostic overshadowing of mental illness, pain, or trauma as “just ID”
- Equating low IQ with unfitness or legal insanity
- Over-trusting risk tool labels while ignoring base rates and protective factors
- Open-ended antipsychotics for non-psychotic aggression linked to offences
- Ignoring suggestibility → unreliable statements and miscarriages of justice
- Failing to assess victimisation and co-defendant coercion
- Inventing statute section numbers in reports or exams
Prognosis and disposition
Recidivism is driven more by untreated criminogenic needs, substance use, antisocial associates, and unstable supports than by IQ band alone. Protective factors include stable supported housing, structured meaningful activity, prosocial relationships, effective communication supports, treated dual diagnosis, and consistent multiagency supervision with offence-paralleling monitoring.[3][4][15]
Disposition ladder (least restrictive for risk): community dual-disability and PBS supports → conditional community supervision → specialist forensic ID services/secure beds → prison with in-reach. Review intensity as dynamic risk and protective factors change; structured tools may track change but clinical multiagency judgement remains central.[11][13]
Special populations
Women. Lower base rates of formal offending; higher relative contribution of trauma, coercive relationships, and victimisation contexts — formulation must not copy male pathways uncritically.[1][17]
Autism + ID. Sensory load, literal thinking, and social naivety alter both offence pathways and interview behaviour; adapt communication and avoid mistaking compliance for understanding.[3][9]
FASD. Executive and adaptive profiles with high justice contact in some jurisdictions require careful developmental diagnosis and strong responsivity adaptations rather than IQ-only labels.[3][1]
Cultural and Indigenous contexts. Test bias, language barriers, and systemic over-policing can distort both “ID” and “offender” labels; cultural safety is part of valid assessment and equitable pathway planning.[1][7]
Older adults with ID. New “offending” may signal dementia, delirium, or placement breakdown rather than a new antisocial career and needs medical-psychiatric re-evaluation first.[3][7]
Evidence and guidelines summary
Holland 2002 and Simpson and Hogg 2001 frame prevalence method hazards and predisposing factors. Barron 2002/2004 describe clinical IDO samples and limited outcome data. Fazel 2008 anchors prison diagnosed ID at roughly 0.5–1.5%; Dias 2013 and Hellenbach 2017 stress comorbidity. Clare and Gudjonsson 1993 make suggestibility non-negotiable for interview reliability. Wall 2003 models fitness restoration for intellectual disability. Fazel 2012 and Singh 2014 limit over-confidence in risk instruments; Buchanan and Large/Ryan support transparent, humble risk practice. Lindsay 2004 differentiates sexual and nonsexual pathways; Willner 2013 supports adapted anger CBT in mild–moderate ID. Latvala 2023 binds crime risk to victimisation risk at population level. Crocker 2006 contextualises aggression as common service concern without equating it to conviction rates.[1][2][3][4][5][6][7][8][9][10][11][12][15][16][17][18]
Exam pearls
- Most people with ID do not offend — method traps inflate headlines
- Prison diagnosed ID often ~0.5–1.5% (Fazel); screening ≠ diagnosis
- Suggestibility/acquiescence threaten confession reliability (Clare and Gudjonsson)
- Fitness ≠ IQ; responsibility ≠ fitness
- RNR responsivity is the ID treatment key
- Always assess victim–offender overlap
- No invented statute numbers — principles only unless you know local law
References
- [1]Holland T, Clare IC, Mukhopadhyay T Prevalence of criminal offending by men and women with intellectual disability and the characteristics of offenders: implications for research and service development J Intellect Disabil Res, 2002.PMID 12061335
- [2]Simpson MK, Hogg J Patterns of offending among people with intellectual disability: a systematic review. Part I: methodology and prevalence data J Intellect Disabil Res, 2001.PMID 11679044
- [3]Simpson MK, Hogg J Patterns of offending among people with intellectual disability: a systematic review. Part II: predisposing factors J Intellect Disabil Res, 2001.PMID 11679045
- [4]Barron P, Hassiotis A, Banes J Offenders with intellectual disability: the size of the problem and therapeutic outcomes J Intellect Disabil Res, 2002.PMID 12354316
- [5]Barron P, Hassiotis A, Banes J Offenders with intellectual disability: a prospective comparative study J Intellect Disabil Res, 2004.PMID 14675234
- [6]Fazel S, Xenitidis K, Powell J The prevalence of intellectual disabilities among 12,000 prisoners - a systematic review Int J Law Psychiatry, 2008.PMID 18644624
- [7]Dias S, Ware RS, Kinner SA, Lennox NG Co-occurring mental disorder and intellectual disability in a large sample of Australian prisoners Aust N Z J Psychiatry, 2013.PMID 23723292
- [8]Hellenbach M, Karatzias T, Brown M Intellectual Disabilities Among Prisoners: Prevalence and Mental and Physical Health Comorbidities J Appl Res Intellect Disabil, 2017.PMID 26775928
- [9]Clare IC, Gudjonsson GH Interrogative suggestibility, confabulation, and acquiescence in people with mild learning disabilities (mental handicap): implications for reliability during police interrogations Br J Clin Psychol, 1993.PMID 8251959
- [10]Wall BW, Krupp BH, Guilmette T Restoration of competency to stand trial: a training program for persons with mental retardation J Am Acad Psychiatry Law, 2003.PMID 12875497
- [11]Fazel S, Singh JP, Doll H, Grann M Use of risk assessment instruments to predict violence and antisocial behaviour in 73 samples involving 24 827 people: systematic review and meta-analysis BMJ, 2012.PMID 22833604
- [12]Singh JP, Fazel S, Gueorguieva R, Buchanan A Rates of violence in patients classified as high risk by structured risk assessment instruments Br J Psychiatry, 2014.PMID 24590974
- [13]Buchanan A Risk of violence by psychiatric patients: beyond the "actuarial versus clinical" assessment debate Psychiatr Serv, 2008.PMID 18245161
- [14]Large MM, Ryan CJ, Nielssen OB Helpful and unhelpful risk assessment practices Psychiatr Serv, 2010.PMID 20439381
- [15]Lindsay WR, Smith AH, Law J, et al. Sexual and nonsexual offenders with intellectual and learning disabilities: a comparison of characteristics, referral patterns, and outcome J Interpers Violence, 2004.PMID 15231027
- [16]Willner P, Rose J, Jahoda A, et al. Group-based cognitive-behavioural anger management for people with mild to moderate intellectual disabilities: cluster randomised controlled trial Br J Psychiatry, 2013.PMID 23520220
- [17]Latvala A, Tideman M, Søndenaa E, et al. Association of intellectual disability with violent and sexual crime and victimization: a population-based study Psychol Med, 2023.PMID 35238292
- [18]Crocker AG, Mercier C, Lachapelle Y, et al. Prevalence and types of aggressive behaviour among adults with intellectual disabilities J Intellect Disabil Res, 2006.PMID 16901292