Psych · intellectual-disability
Psychiatric disorders in intellectual disability
Also known as Dual diagnosis intellectual disability · Mental ill-health in learning disability · Psychiatric comorbidity in ID · DC-LD psychiatry · Learning disability mental illness
Exam-exhaustive fellowship reference on psychiatric disorders in intellectual disability — diagnostic overshadowing, modified/pathoplastic presentation, DC-LD and DM-ID frameworks, Cooper/Smiley epidemiology, differential of behaviour that challenges versus mental illness versus physical illness, adapted assessment, treatment adaptations, Tyrer/Sheehan/Deb psychotropic evidence, NICE and multiagency care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
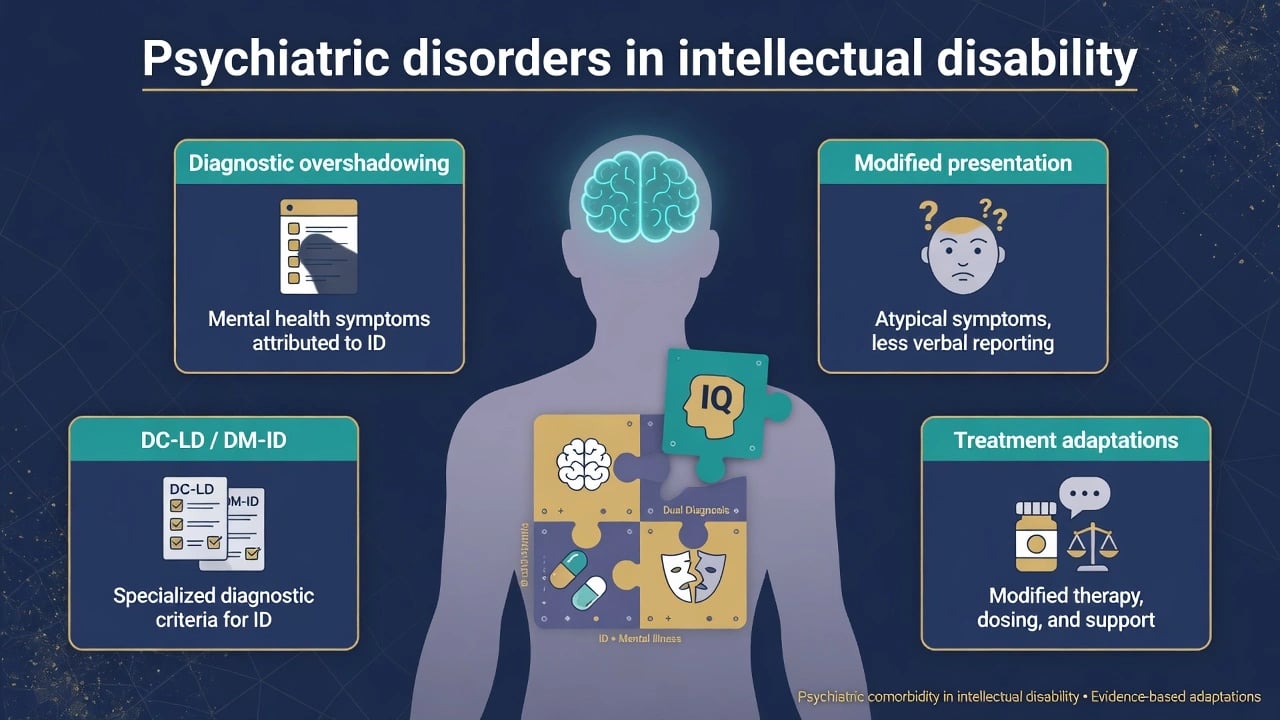
Psychiatric disorders in intellectual disability (ID) — often called dual diagnosis when mental illness co-occurs with ID — are a high-yield FRANZCP and MRCPsych topic. Examiners test whether you can name diagnostic overshadowing, describe pathoplastic / modified presentation by severity, use DC-LD (and DM-ID) as complementary systems, quote Cooper/Smiley epidemiology, and prescribe with Deb guide + Tyrer + Sheehan caution rather than reflex antipsychotics.[1][3][6][7][8]
Overview and definition
Intellectual disability (intellectual developmental disorder) is defined by deficits in intellectual and adaptive functioning with onset in the developmental period. Dual diagnosis means co-occurring mental illness / mental ill-health, not ID alone. Standard DSM-5-TR and ICD-11 criteria remain the diagnostic backbone, but communication limits and cognitive level can change how symptoms are expressed (pathoplasticity). Complementary systems such as DC-LD operationalise criteria for adults with moderate–profound ID and explicitly accommodate modified presentation.[1][3]
Mental ill-health in this population includes affective, psychotic, anxiety, autism-spectrum co-occurrence, dementia (especially in older people and Down syndrome), and problem behaviours classified within DC-LD hierarchies — problem behaviour is not automatically synonymous with a DSM major mental disorder, but it is clinically and epidemiologically central.[1][3][12]
Classification and diagnostic frameworks
DSM-5-TR / ICD-11
Apply standard criteria when communication allows reliable symptom report. Specifiers for severity of ID matter because they predict how "classic" symptoms will appear. Co-occurring autism spectrum disorder, ADHD, epilepsy, and sensory impairment are coded separately when present.[3][13]
DC-LD (must name in exams)
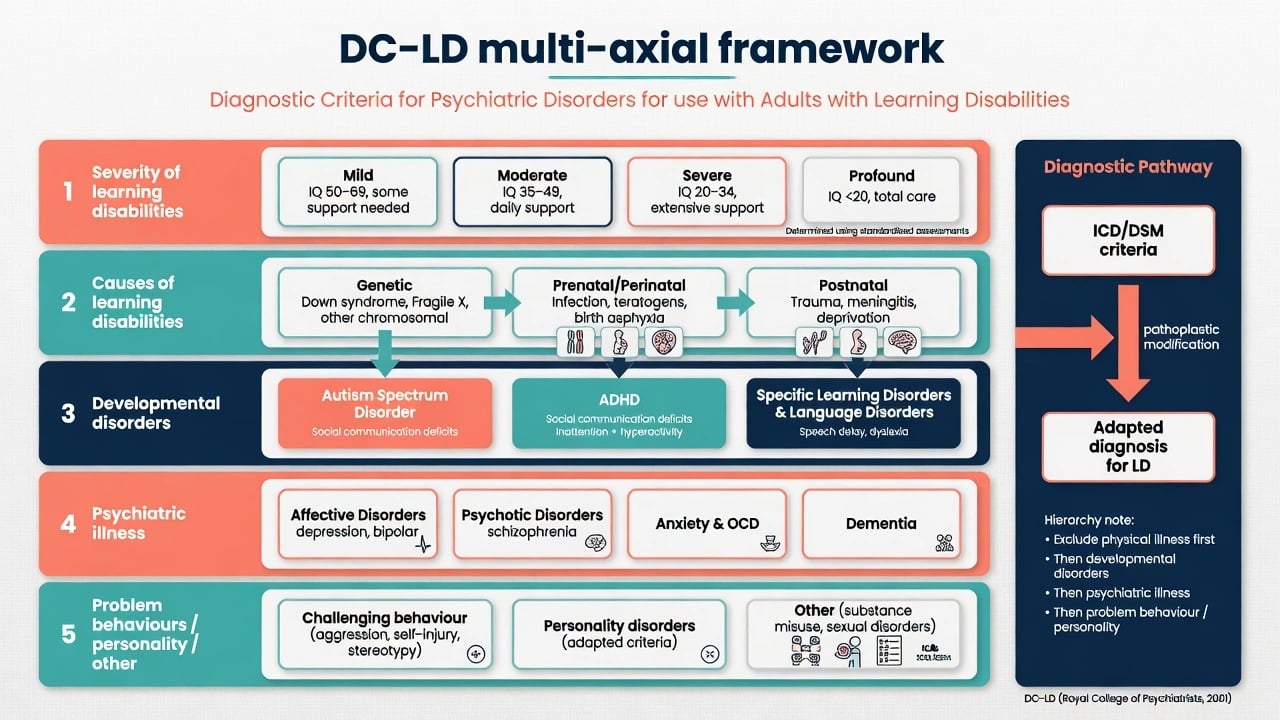
DC-LD (Diagnostic Criteria for Psychiatric Disorders for Use with Adults with Learning Disabilities/Mental Retardation, Royal College of Psychiatrists) is a multi-axial system complementary to ICD for adults with ID. It describes severity and causes of learning disability, developmental disorders, psychiatric illness, personality disorders, problem behaviours and other disorders, and uses a hierarchical approach that accommodates the pathoplastic effect of ID on psychopathology.[3]
Use DC-LD when standard ICD/DSM criteria under-detect illness because of limited verbal report, atypical behavioural equivalents, or when you need explicit structure for problem behaviours relative to psychiatric illness.[3]
DM-ID / DM-ID-2
The Diagnostic Manual–Intellectual Disability (DM-ID and DM-ID-2) provides adaptations of DSM criteria for people with ID — useful for ABPN-framed answers as the US counterpart conceptual toolkit to DC-LD.[3]
Epidemiology and risk
Headline dual-diagnosis numbers
In a population-based adult sample, Cooper and colleagues reported point prevalence of mental ill-health of 40.9% by clinical diagnosis, 35.2% by DC-LD, 16.6% by ICD-10-DCR, and 15.7% by DSM-IV-TR — examiners love this multi-system comparison because it proves classification choice changes apparent prevalence.[1] Problem behaviours were the most prevalent category under DC-LD thinking; affective, autistic, psychotic and anxiety disorders also contribute clinically important burden.[1][15]
Prospective work by Smiley and colleagues established incidence and predictors of new mental ill-health in adults with ID, reinforcing that this is not a static childhood-only problem.[2] Reviews of adult epidemiology continue to show elevated rates versus general population estimates, with methodological heterogeneity explaining wide historical ranges.[12]
In children and adolescents, systematic review data show comorbidity rates commonly in the 30–50% range with elevated relative risk of mental disorder compared with peers without ID.[9][13]
Associations in adult samples include more life events, female sex (in some analyses), type of support/residence, lower ability, higher consultation rates, smoking and incontinence; deprivation alone is not a simple universal predictor in all analyses.[1][2]
Mechanisms and vulnerability
Mental ill-health risk is multifactorial: shared genetic and neurodevelopmental aetiology, epilepsy and sensory impairment, limited coping and communication repertoire, dependency, trauma and abuse risk, social exclusion, and life events (bereavement, placement change, staff turnover).[1][5][12] The key clinical mechanism for examiners is pathoplasticity — the same underlying mood, anxiety or psychotic process may present as behavioural change rather than articulate phenomenology.[3]
Diagnostic overshadowing (core exam concept)
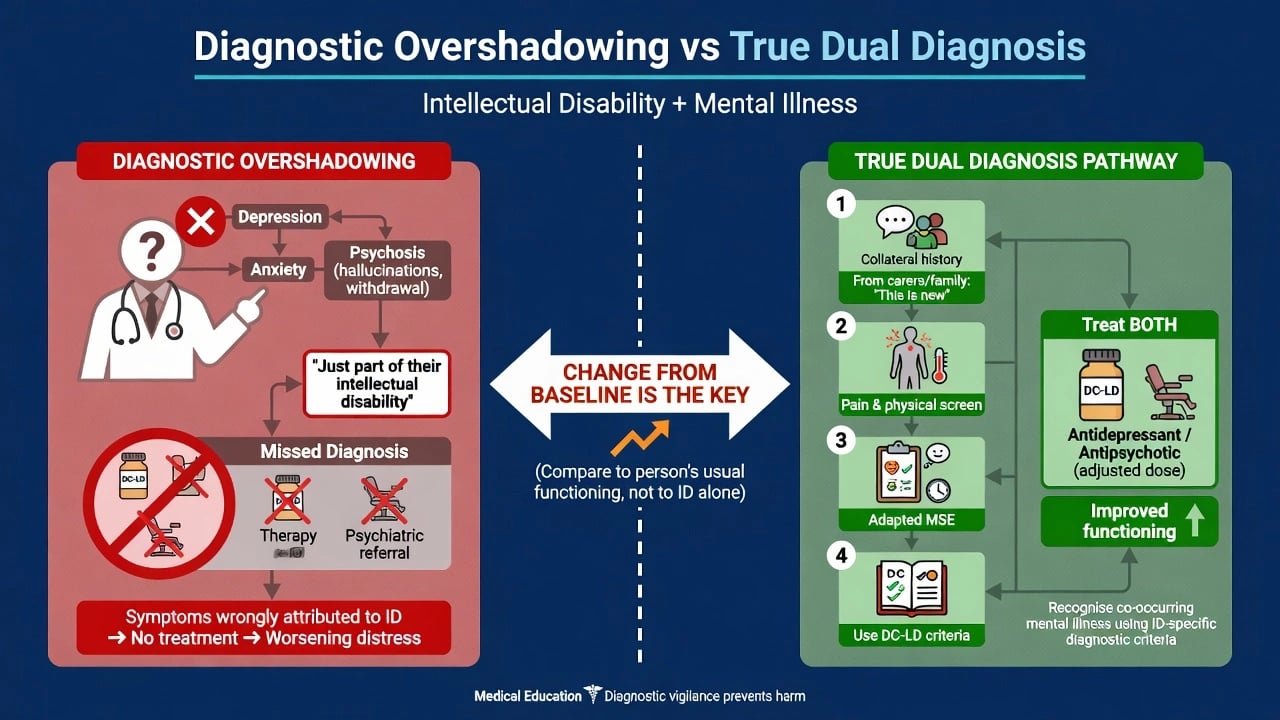
Diagnostic overshadowing is the cognitive bias in which a known ID diagnosis is so salient that clinicians falsely attribute symptoms of mental or physical illness to the disability itself, delaying recognition and treatment.[4][5] Classic experimental and clinical literature (Reiss and colleagues) established the concept; modern safety writing (Ali and Hassiotis) links overshadowing to suboptimal care and, in extreme cases, missed physical illness with fatal outcomes.[4][5]
Countermeasures: always ask "what has changed from this person's baseline?", obtain collateral, screen for pain and medical illness, use adapted MSE, and apply DC-LD/DM-ID when standard interview fails.[3][5]
Clinical presentation by severity
Mild ID
More "classical" presentations of depression, anxiety, OCD, psychosis and bipolar disorder are often detectable with simplified language, visual supports and collateral. Suicide risk is real in verbal people with depression — do not dismiss it.[1][9]
Moderate to profound ID
Expect behavioural equivalents when verbal report is limited — these are pathoplastic expressions of treatable mental illness, not inevitable features of ID alone.[2][3]
| Suspected illness | Possible equivalents in limited verbal ability |
|---|---|
| Depression | Irritability, withdrawal, loss of preferred activities, self-injury increase, sleep/appetite change, regression of skills, tearfulness |
| Anxiety | Avoidance, clinginess, autonomic arousal, new fears, sleep disturbance, aggression in demanding contexts |
| Psychosis | Unexplained fear, covering ears, responding to unseen stimuli, sudden functional collapse, bizarre new behaviours not explained by ASD baseline |
| Mania/hypomania | Reduced sleep need, increased energy, disinhibition, rapid/pressured speech if verbal, irritability |
These behavioural equivalents must be interpreted against developmental level and communication ability using DC-LD pathoplastic thinking rather than standard interview alone.[2][3]
Compare any change against known baseline (including ASD RRBs if dual neurodevelopmental diagnosis). New-onset symptoms matter more than lifelong mannerisms.[3][13]
Differential diagnosis
Win differentials on timeline, medical screen, environmental analysis, and form of symptoms — not shopping lists.[5][7]
- Physical illness / pain (constipation, dental, otitis, GORD, fracture, UTI, headache) — first exclusion in behavioural change.[5]
- Epilepsy and post-ictal states; AED side-effects.
- Medication toxicity / anticholinergic delirium and benzodiazepine paradoxical effects.
- Sensory overload, grief, abuse, placement change — functional analysis of behaviour.
- Autism baseline RRBs versus new OCD or psychosis.
- ADHD versus anxiety-driven restlessness.
- Substance use in mild ID adolescents and adults.
- True mental illness meeting adapted criteria — do not under-diagnose because of overshadowing.[4][5]
Assessment
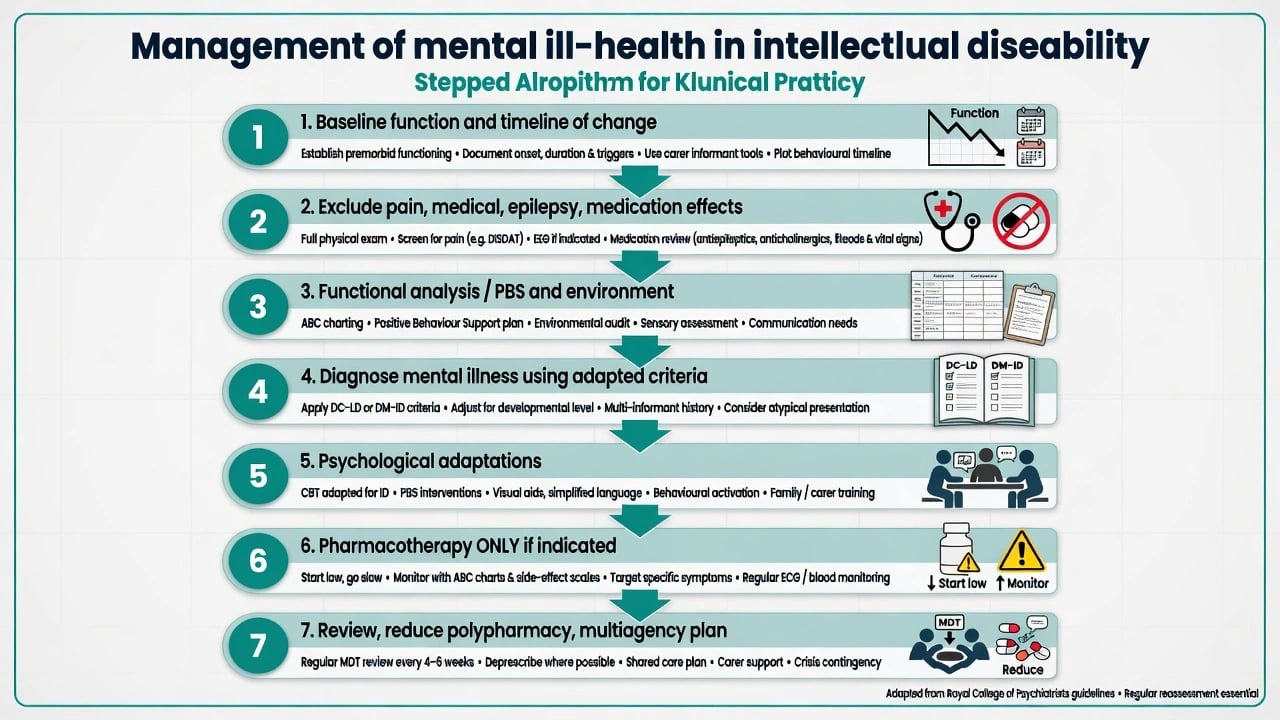
History structure. Developmental level and communication method (speech, AAC, signing); baseline adaptive function; timeline of change; life events; sleep, bowel, pain behaviours; epilepsy; full medication list; trauma and safeguarding; substance use if relevant.[3][5]
Collateral. Family, paid carers, school/day services, previous psychology reports, ABC charts, behaviour support plans, GP annual health check findings.[1][5]
Adapted MSE. Observation of affect, arousal, relatedness, response to environment and staff; allow processing time; reduce sensory load; do not equate limited eye contact or flat affect alone with psychosis if that is baseline ASD/ID style.[3]
Risk. Self-injury, aggression, absconding, exploitation, sexual vulnerability, neglect, suicide (especially mild ID with mood disorder), carer burnout and placement risk.[1][6]
Capacity. Decision-specific; maximise support (simple language, visual aids, time, trusted supporter); least restrictive legal pathway under local Mental Health / Guardianship / capacity legislation — do not invent foreign section numbers in exams.[5]
Tools (conceptual). PAS-ADD family instruments support case finding; DC-LD structures diagnosis — clinical judgment remains decisive.[3]
Investigations
Target the behavioural change: physical examination; FBC, U&E, LFT, glucose, TFT, B12/folate; infection screen as indicated; medication review. ECG and metabolic baseline before antipsychotics; QTc awareness with polypharmacy. EEG/imaging for seizure concern, atypical regression or focal neurology — not routine "ID work-up" for every behavioural presentation.[5][7]
Acute / emergency management
De-escalate: reduce noise and demand, offer familiar carer, sensory adaptations, least restrictive holding only if necessary. Exclude medical emergency and delirium. Rapid tranquillisation — if required — uses lowest effective doses with high vigilance for EPS, oversedation and respiratory depression in people with ID and physical comorbidity. Do not convert an ED visit into lifelong antipsychotic without formulation, consent/capacity process and review plan.[6][7][8]
Definitive management and treatment adaptations
Principles
- Treat identified mental illness with the same evidence-based classes as general adult psychiatry, adapted for cognition and communication.[7][10]
- For behaviours that challenge without mental illness, prioritise positive behaviour support, skills teaching, environmental redesign and carer training before long-term psychotropics.[7][14]
- Start low, go slow, define target symptoms and outcome measures, monitor adverse effects, and plan dose reduction when stable.[7][16]
Psychological adaptations
- Simplify language; use visual schedules, role-play and longer or more frequent shorter sessions.
- Involve carers as co-therapists when appropriate and consented.
- Hassiotis pilot RCT supports feasibility of adapted CBT for anxiety/depression in mild ID.[10]
- Willner cluster RCT: group-based CBT anger management improved anger control in mild–moderate ID.[11]
- Do not exclude people from therapy solely because of ID label — match modality to ability.[10][11]
Pharmacotherapy — exam-critical evidence
Deb international guide (World Psychiatry 2009): assess behaviour thoroughly, formulate, consider non-drug interventions, initiate medicine only with clear targets, review efficacy and adverse effects, follow up systematically.[7]
Tyrer 2008 Lancet RCT: in aggressive challenging behaviour among adults with ID, risperidone and haloperidol were not superior to placebo on primary aggression outcomes at 4 weeks — aggression fell in all arms. Exam pearl: antipsychotics should not be regarded as acceptable routine treatment for aggressive challenging behaviour in this group.[8]
Sheehan 2015 BMJ cohort: proportion treated with psychotropics far exceeds proportion with recorded mental illness — population evidence of overprescribing relative to documented diagnosis.[6]
If an antipsychotic is used after medical exclusion, behavioural intervention and clear risk justification (or for a diagnosed psychotic/mood illness): start at the low end of the adult range (for example risperidone often 0.25–0.5 mg oral daily initially in sensitive adults with ID, titrating slowly), obtain baseline weight, waist, glucose/lipids, prolactin as indicated, and EPS/AIMS monitoring; set a time-limited trial with documented review for reduction.[7][8][16]
Antidepressants for diagnosed depression/anxiety (e.g. sertraline 25 mg oral daily start in sensitive adults, then titrate by response and tolerability) with monitoring for activation, sleep change and suicidality in verbal patients.[7][10]
Mood stabilisers / lithium / AEDs for bipolar or seizure comorbidity with full laboratory and clinical monitoring; avoid polypharmacy stacks without indication.[7][14]
Subtypes and common scenarios
- Mild ID + first-episode psychosis: standard early-intervention principles with simplified psychoeducation and capacity support.[1]
- Severe ID + self-injury increase: depression/pain/abuse screen before antipsychotic escalation.[5]
- ID + epilepsy: behavioural change may be seizure-related or AED-related — coordinate neurology.[12]
- ID + ASD: dual neurodevelopmental diagnosis common; irritability pathways differ from pure psychotic illness.[9][13]
- Placement breakdown: multiagency plan, least restrictive alternatives, avoid indefinite hospitalisation for social reasons alone.[6]
Complications and pitfalls
Diagnostic overshadowing; missing physical illness; antipsychotic overuse (Sheehan); metabolic syndrome, EPS, prolactin elevation, sedation and falls; polypharmacy; assuming global incapacity; excluding from psychological therapy; failing to plan transition from child to adult ID services.[4][5][6][8]
Prognosis and disposition
Course depends on aetiology of ID, type of mental illness, epilepsy burden, quality of support and access to specialist ID psychiatry. Multiagency care plans, annual health checks, carer support and skills maintenance improve outcomes. Step up to specialist or inpatient intellectual disability psychiatry when community risk is unmanageable; plan discharge to least restrictive living with skills preservation.[1][2][12]
Special populations
Children/adolescents: high comorbidity; school interface essential.[9][13] Older adults: dementia risk (especially Down syndrome), late-life depression, polypharmacy. Women: reproductive health, menopause, abuse vulnerability. Forensic: higher vulnerability as victims; capacity and fitness issues when offending. Cultural diversity: assessment bias and family structure — use interpreters and culturally safe formulation.[5][12]
Evidence and guidelines (regional deltas)
Landmark dual-diagnosis evidence and regional framing for exams are summarised below; quote named studies rather than vague "guidelines say".[1][3][6][7][8]
| Source | Exam takeaway |
|---|---|
| Cooper 2007 / Smiley 2007 | Prevalence ~40% clinical; multi-criteria comparison; incidence data |
| Cooper 2003 DC-LD | Pathoplastic criteria complementary to ICD |
| Deb 2009 World Psychiatry | International prescribing process standard |
| Tyrer 2008 Lancet | Antipsychotics not routine for aggression alone |
| Sheehan 2015 BMJ | Psychotropics exceed recorded mental illness |
| Hassiotis / Willner | Adapted CBT is feasible and can help |
| NICE NG11 (UK) | Challenging behaviour: psychosocial first; antipsychotics only under strict conditions |
| RANZCP / ANZ practice | Specialist ID psychiatry pathways; capacity and NDIS/disability interfaces |
| APA / DM-ID framing (US) | Adapted DSM criteria language for ABPN answers |
State which framework you are using and name regional service pathways rather than inventing legal section numbers.[1][2][3][6][7][8][10][11]
Exam pearls
ANZ answers emphasise specialist intellectual disability psychiatry, capacity/guardianship interfaces and disability supports. UK answers often cite DC-LD heritage, NICE challenging-behaviour guidance and STOMP-style deprescribing culture. US answers may name DM-ID adaptations of DSM. Core clinical science is shared: overshadowing, modified presentation, hierarchical assessment, cautious psychotropics.[3][6][7]
References
- [1]Cooper SA, Smiley E, Morrison J, Williamson A, Allan L Mental ill-health in adults with intellectual disabilities: prevalence and associated factors Br J Psychiatry, 2007.PMID 17197653
- [2]Smiley E, Cooper SA, Finlayson J, et al. Incidence and predictors of mental ill-health in adults with intellectual disabilities: prospective study Br J Psychiatry, 2007.PMID 17906241
- [3]Cooper SA, Melville CA, Einfeld SL Psychiatric diagnosis, intellectual disabilities and Diagnostic Criteria for Psychiatric Disorders for Use with Adults with Learning Disabilities/Mental Retardation (DC-LD) J Intellect Disabil Res, 2003.PMID 14516368
- [4]Reiss S, Szyszko J Diagnostic overshadowing and professional experience with mentally retarded persons Am J Ment Defic, 1983.PMID 6829617
- [5]Ali A, Hassiotis A Illness in people with intellectual disabilities BMJ, 2008.PMID 18340045
- [6]Sheehan R, Hassiotis A, Walters K, Osborn D, Strydom A, Horsfall L Mental illness, challenging behaviour, and psychotropic drug prescribing in people with intellectual disability: UK population based cohort study BMJ, 2015.PMID 26330451
- [7]Deb S, Kwok H, Bertelli M, et al.; Guideline Development Group of the WPA Section on Psychiatry of Intellectual Disability International guide to prescribing psychotropic medication for the management of problem behaviours in adults with intellectual disabilities World Psychiatry, 2009.PMID 19812757
- [8]Tyrer P, Oliver-Africano PC, Ahmed Z, et al. Risperidone, haloperidol, and placebo in the treatment of aggressive challenging behaviour in patients with intellectual disability: a randomised controlled trial Lancet, 2008.PMID 18177776
- [9]Einfeld SL, Ellis LA, Emerson E Comorbidity of intellectual disability and mental disorder in children and adolescents: a systematic review J Intellect Dev Disabil, 2011.PMID 21609299
- [10]Hassiotis A, Serfaty M, Azam K, et al. Cognitive behaviour therapy (CBT) for anxiety and depression in adults with mild intellectual disabilities (ID): a pilot randomised controlled trial J Intellect Disabil Res, 2011.PMID 21492437
- [11]Willner P, Rose J, Jahoda A, et al. Group-based cognitive-behavioural anger management for people with mild to moderate intellectual disabilities: cluster randomised controlled trial Br J Psychiatry, 2013.PMID 23520220
- [12]Cooper SA, van der Speck R Epidemiology of mental ill health in adults with intellectual disabilities Curr Opin Psychiatry, 2009.PMID 19535982
- [13]Munir KM The co-occurrence of mental disorders in children and adolescents with intellectual disability/intellectual developmental disorder Curr Opin Psychiatry, 2016.PMID 26779862
- [14]Deb S, Unwin GL Psychotropic medication for behaviour problems in people with intellectual disability: a review of the current literature Curr Opin Psychiatry, 2007.PMID 17762588
- [15]Cooper SA, Smiley E, Morrison J, Williamson A, Allan L Mental ill-health in adults with intellectual disabilities: prevalence and associated factors (DC-LD subtype rates) Br J Psychiatry, 2007.PMID 17197653
- [16]Deb S, Kwok H, Bertelli M, et al. International guide to prescribing psychotropic medication for the management of problem behaviours in adults with intellectual disabilities (monitoring principles) World Psychiatry, 2009.PMID 19812757