Psych · Old age psychiatry — Alzheimer disease
Alzheimer disease
Also known as Alzheimer's disease · AD dementia · Major NCD due to Alzheimer disease · Dementia of Alzheimer type · Probable Alzheimer disease · Senile dementia of the Alzheimer type
Exam-exhaustive fellowship reference on Alzheimer disease — NIA-AA 2011 probable/possible clinical criteria; continuum from preclinical and MCI-due-to-AD to dementia; careful ATN biomarker research framing; amyloid/tau/cholinergic pathophysiology; assessment with collateral and cognitive screens; AChEI and memantine doses, titration, monitoring and DOMINO-AD; BPSD link with non-drug first line and antipsychotic mortality caution; capacity, care planning, and disposition. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Alzheimer disease (AD) is the core old-age psychiatry leaf under the broader dementia hub. FRANZCP MEQs demand NIA-AA language, a named cognitive enhancer with dose and monitoring, BPSD judgement, and capacity. MRCPsych tests continuum concepts, AChEI pharmacology, and carer communication. ABPN items stress criteria, biomarkers as research constructs, and antipsychotic black-box caution. Read this topic as a standalone exam resource; link to the dementia hub for multi-subtype comparison and to the BPSD topic for deep neuropsychiatric management.[1][7][20]
Overview and definition
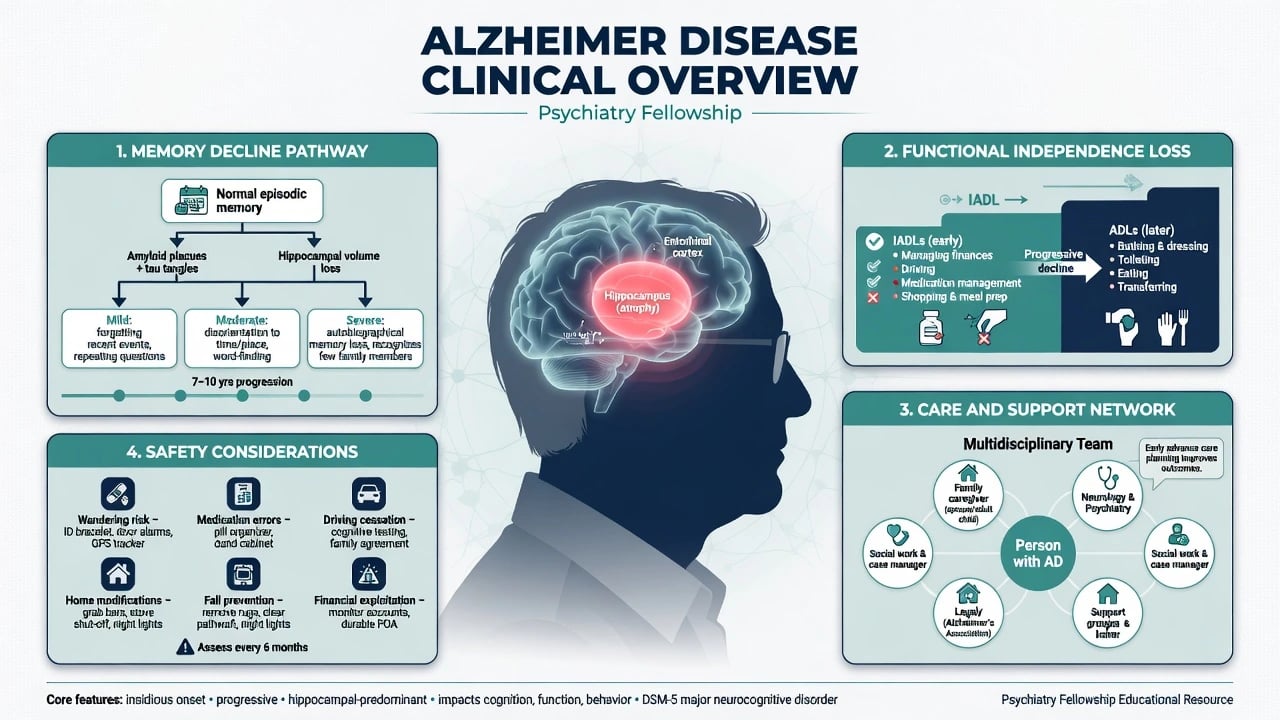
AD is a progressive neurodegenerative disease characterised pathologically by amyloid-β plaques and hyperphosphorylated tau neurofibrillary tangles, and clinically most often by an insidious amnestic syndrome that expands multi-domain and eventually interferes with independence. For psychiatry exams, separate three layers: (1) clinical syndrome (what you diagnose at the bedside), (2) aetiological attribution to AD, and (3) biological AD defined by biomarkers or neuropathology in research frameworks.[1][4]
DSM-5-TR. Major neurocognitive disorder due to Alzheimer disease requires significant cognitive decline in one or more domains that interferes with independence, is not exclusively delirium, and is not better explained by another mental disorder, plus criteria pointing to AD (insidious onset and gradual progression; for typical AD, decline in memory and learning and at least one other domain). Specifiers include probable versus possible AD depending on evidence certainty and whether another aetiology is mixed in. Mild NCD due to AD uses the same aetiological logic without loss of independence (though compensation may be needed).[1][2]
ICD-11. Dementia due to Alzheimer disease is framed as progressive decline affecting multiple cognitive domains with interference in activities of daily living. State which manual you are using when nosology is examined.[1]
Classification and NIA-AA clinical criteria
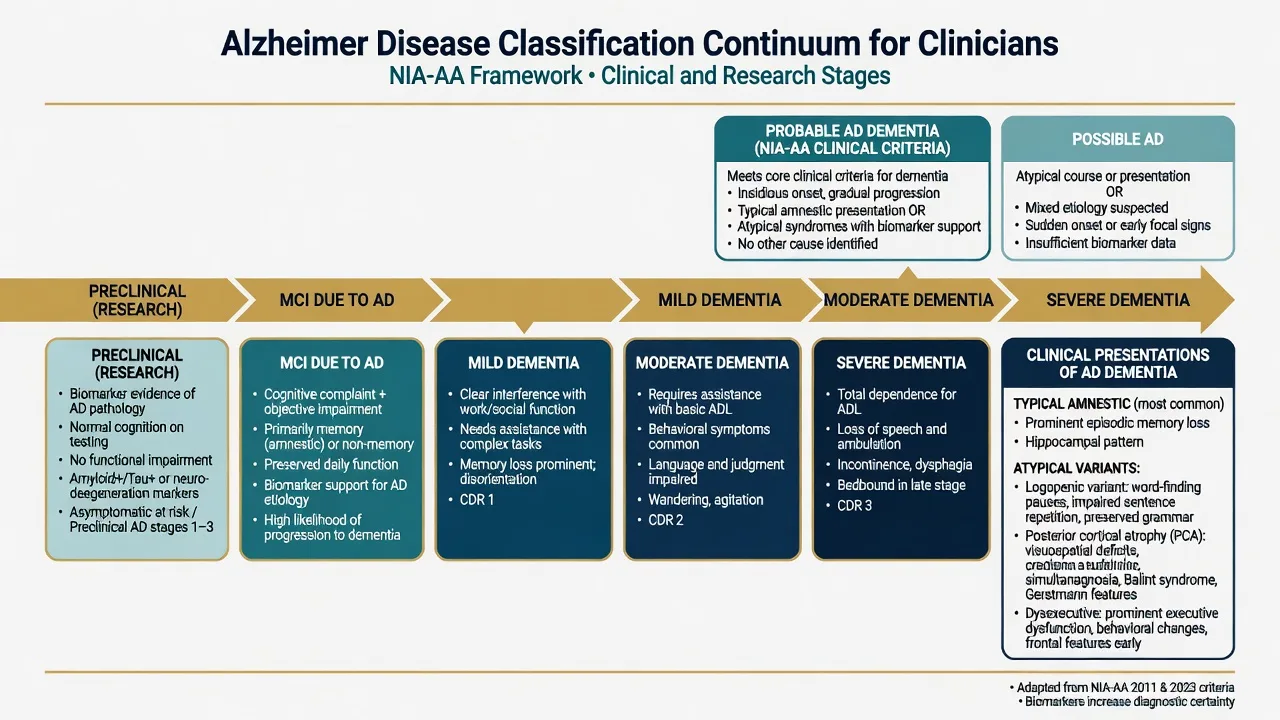
NIA-AA 2011 clinical dementia criteria (McKhann)
McKhann and colleagues provide the high-yield clinical standard still examined worldwide.[1]
- Meet all-cause dementia criteria (cognitive or behavioural symptoms interfering with function, representing decline, not explained by delirium or major psychiatric disorder alone, involving at least two domains or a combination of cognitive and behavioural change).
- For probable AD dementia: insidious onset; clear-cut history of worsening; most prominent early deficits either amnestic (learning and recall of recently learned information) or non-amnestic (language, visuospatial, or executive); and no substantial evidence of another concurrent aetiology that better explains the deficits (for example, substantial cerebrovascular disease explaining the deficits, core features of DLB, or prominent behavioural variant FTD features).
- Possible AD dementia: atypical course (sudden onset or insufficient historical detail) or etiologically mixed presentation (for example, concomitant cerebrovascular disease or features of another dementia that could contribute).[1]
Continuum companions (2011)
- Preclinical AD (Sperling): research construct for cognitively unimpaired persons with biomarker evidence of AD pathophysiology — not a community diagnosis to hand patients casually without specialist framing.[3]
- MCI due to AD (Albert): symptomatic predementia with preserved independence; biomarker certainty tiers exist for research enrichment.[2]
- Historical Dubois 2007 research criteria emphasised earlier diagnosis with biomarkers — viva context for how the field moved beyond pure NINCDS-ADRDA exclusion diagnosis.[6]
Atypical clinical variants
Logopenic primary progressive aphasia, posterior cortical atrophy, and behavioural/dysexecutive presentations can be AD-spectrum phenotypes. Do not require early dense amnesia to consider AD when the phenotype fits an atypical AD syndrome and alternative frontotemporal or Lewy diagnoses are less likely.[1]
Epidemiology and risk
AD is the most common cause of dementia in older adults. Prevalence rises steeply with age. Women carry higher absolute case numbers (longevity and biological contributions). Age, APOE ε4 allele, and family history are major non-modifiable risks; rare autosomal-dominant mutations (PSEN1, PSEN2, APP) drive a minority of young-onset familial AD. Down syndrome markedly elevates AD risk because of APP dosage on chromosome 21.[1][7]
The Lancet Commission frames a substantial fraction of dementia cases as potentially attributable to modifiable mid- and late-life risks (education, hearing loss, hypertension, obesity, smoking, depression, physical inactivity, social isolation, diabetes, alcohol, TBI, air pollution, and related updates). Use this for prevention counselling and public-health viva, not as a claim that any single risk factor fully explains an individual patient's AD.[7]
Pathophysiology
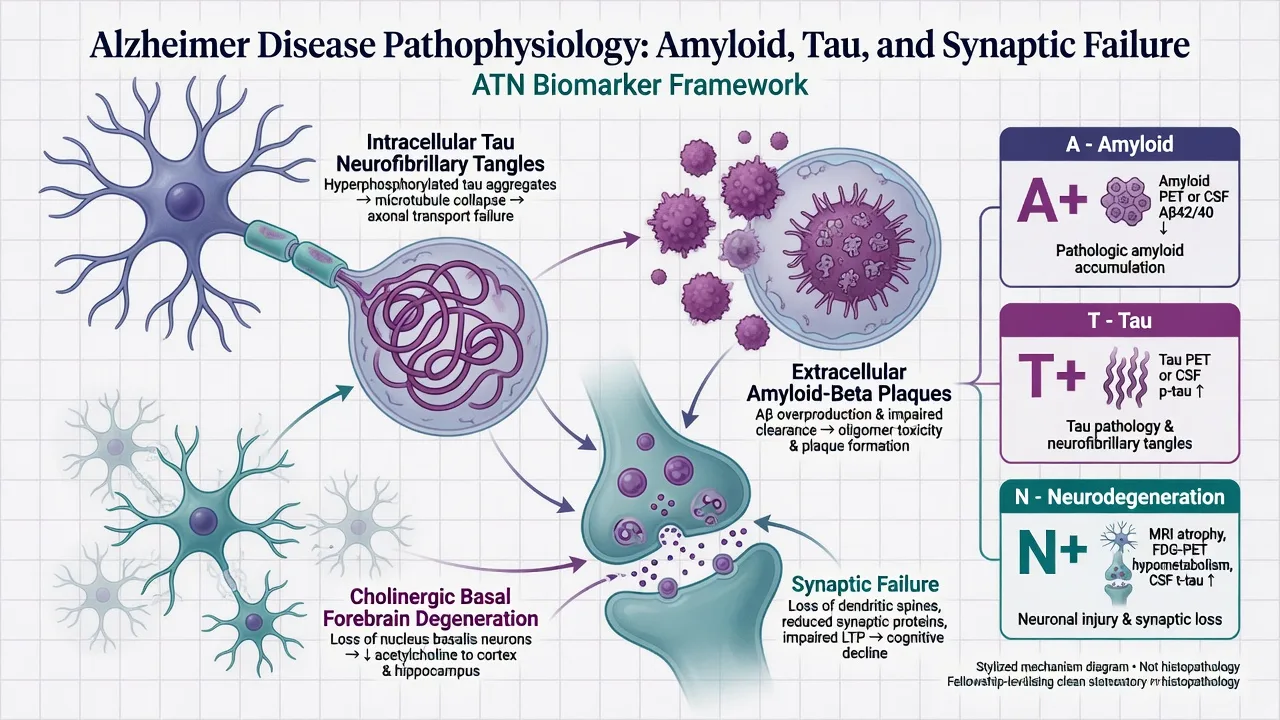
Core neuropathology: extracellular amyloid-β plaques and intracellular hyperphosphorylated tau neurofibrillary tangles, with early medial temporal and default-mode network vulnerability, progressive neocortical spread, synaptic failure, and neuroinflammation. Cholinergic basal forebrain degeneration supplies the symptomatic rationale for cholinesterase inhibitors. Glutamatergic NMDA pathway dysregulation supplies the symptomatic rationale for memantine. Mixed AD-vascular pathology is common in late life — pure single-etiology labels are often oversimplifications.[1][4][11]
Biomarkers — careful exam framing
Jack 2018 NIA-AA research framework (ATN). Biomarkers group into A (amyloid: CSF Aβ42 or Aβ42/Aβ40, amyloid PET), T (pathologic tau: CSF p-tau, tau PET), and N (neurodegeneration/injury: CSF t-tau, FDG-PET hypometabolism, structural MRI atrophy patterns). In research definitions, Alzheimer pathologic change is A+; Alzheimer disease biologically requires A+ and T+; N indicates severity/injury and is not disease-defining alone. The 2018 authors emphasised that applying the pure research framework as routine general medical practice was premature — examiners still reward this caution.[4]
2024 revised criteria (awareness level). Updated workgroup criteria further develop biological diagnosis and staging and respond to advances including blood-based biomarkers. For fellowship answers: know they exist, that access and funding differ by region, that counselling and false-positive/negative consequences matter, and that you must not invent local PBS/Medicare rules or claim universal primary-care blood tests as settled standard everywhere.[5]
Practical ordering rules for viva. Order structural imaging once in the diagnostic work-up. Reserve CSF/PET/blood biomarkers for memory-clinic or research contexts with pre-test counselling. Do not routine-test APOE as a diagnostic test without a clear purpose and counselling. Genetic testing for monogenic AD is a specialist genetics pathway for young-onset familial presentations.[1][4][5]
Clinical presentation
Typical amnestic AD. Insidious difficulty learning and recalling recent events, repeated questions, misplacing items, progressive word-finding, visuospatial and navigational difficulty, executive decline, then progressive loss of IADLs (finances, medications, cooking, transport) and later basic ADLs. Social facade may be relatively preserved early; insight often declines later (anosognosia).[1]
Neuropsychiatric symptoms. Apathy, depression, anxiety, irritability, sleep disturbance, and later psychosis and agitation are common across the course. Nearly all people with dementia experience behavioural and psychological symptoms (BPSD) at some point; quantify with NPI when management decisions are complex.[10][16]
Tempo. Years progressive. Weeks-to-months collapse forces a delirium and rapidly progressive dementia work-up, not an automatic "advanced AD" label.[1][7]
Differential diagnosis
| Discriminator | Typical AD | Vascular CI / mixed | DLB | bvFTD | Delirium |
|---|---|---|---|---|---|
| Onset | Insidious | Stepwise or subacute vascular events; or gradual small-vessel | Insidious with fluctuations | Insidious behavioural | Hours–days |
| Early lead | Episodic memory | Executive/processing speed, focal signs | Attention fluctuations, VH, RBD, parkinsonism | Disinhibition, apathy, empathy loss | Inattention |
| Course | Gradual years | Stepwise or fluctuating vascular | Fluctuating | Progressive behaviour/language | Tracks medical drivers |
| Drug trap | AChEI usually considered | Limited pure-vascular AChEI role | Extreme neuroleptic sensitivity | AChEI often unhelpful | Fix cause first |
| Discriminators use tempo, lead domain, motor/sleep signs, and behavioural phenotype — not a single cognitive score.[1][16] |
Other differentials: late-life depression with cognitive impairment; medication effects (anticholinergics, benzodiazepines); alcohol-related brain damage; B12/thyroid/calcium disorders; OSA; NPH; subdural haematoma; HIV/syphilis when indicated; autoimmune encephalitis and CJD when rapid.[1][7]
Keep clinical and biological languages distinct in exams so you do not oversell biomarkers or underuse clinical criteria.[1][4]
Assessment
Collateral is mandatory. Structure: onset and tempo; cognitive domains; functional independence (IADLs then ADLs); BPSD; sleep (RBD raises DLB concern); vascular risks; alcohol and anticholinergic load; family history; driving, finances, weapons, fire safety; elder abuse and carer stress.[1][16]
Cognitive screens. MMSE remains a familiar bedside grader; MoCA is more sensitive for mild impairment and executive/visuospatial items. Neither replaces clinical judgement; both are affected by education, language, sensory impairment, and effort. Formal neuropsychology is valuable for atypical, young-onset, high-functioning, or high-stakes capacity questions.[8][9]
MSE. Orientation, attention (delirium screen), memory, language, praxis, visuospatial, insight, mood, psychosis, risk. Use NPI domains when neuropsychiatric burden drives care.[10]
Capacity. Appelbaum four abilities: understand relevant information, appreciate the situation and consequences, reason about options, and communicate a choice. Capacity is decision-specific and time-specific (treatment, finances, accommodation, research).[19]
Investigations
Baseline: FBC, U&E, LFT, B12, folate, TFT, glucose/HbA1c, calcium; consider HIV/syphilis if risk or atypical. Structural CT/MRI once to exclude treatable structural disease and support pattern recognition (educational AD-supportive pattern includes medial temporal/hippocampal atrophy — do not invent fake scan reports for a fictional patient). ECG before cholinesterase inhibitors when bradycardia, conduction disease, or interacting drugs are concerns.[1][14][20]
Acute behavioural crisis and medical safety
Acute change is delirium until proven otherwise. Hunt pain, infection (including UTI and pneumonia), constipation, urinary retention, hypoxia, electrolytes, new drugs, and sensory overload. De-escalate environment first. If imminent risk of harm after non-drug measures, any antipsychotic is a time-limited, lowest-effective-dose decision with documented risk-benefit and mortality counselling — not a standing residential order.[16][17]
Definitive management and care
Non-drug foundations
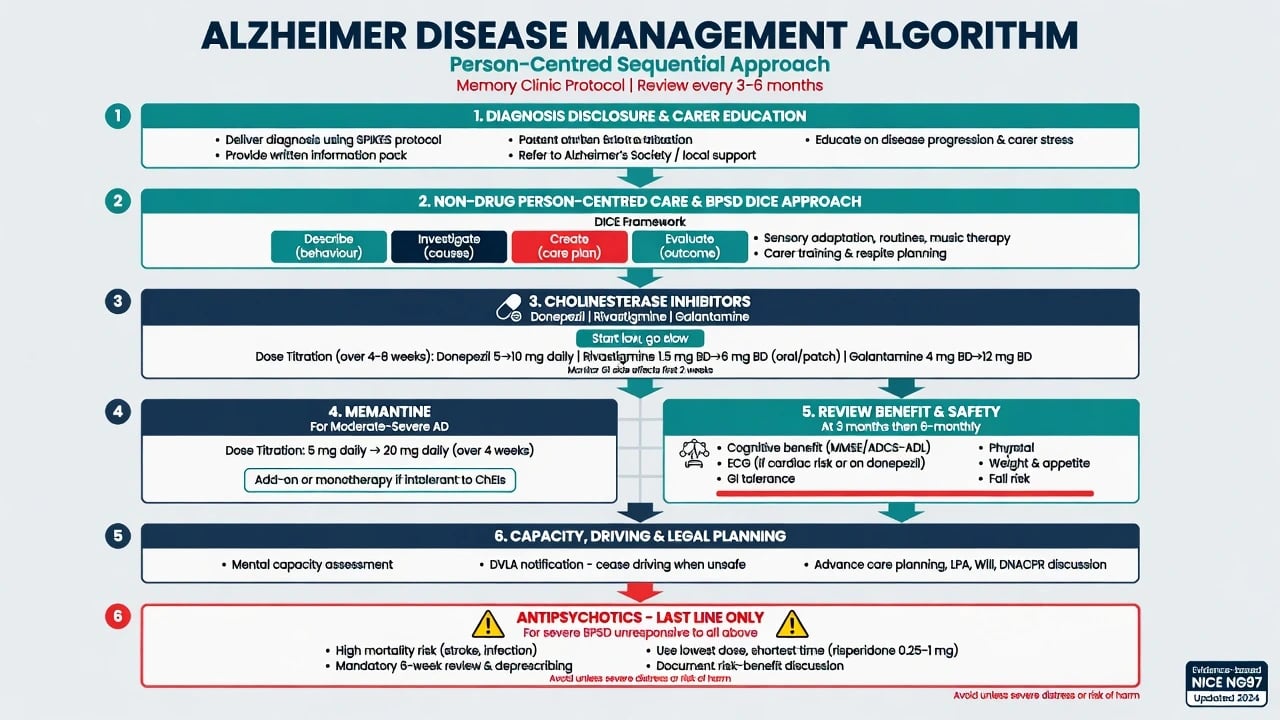
Diagnosis disclosure with hope and honesty; written information; carer education; occupational therapy and cognitive strategies; hearing and vision optimisation; exercise and social connection where feasible; community aged-care packages; advance care planning; driving advice per local licensing rules; financial and legal planning (enduring powers, guardianship pathways — jurisdiction-specific statutes, not invented section numbers).[7][20]
BPSD link
Use the DICE approach (Describe the behaviour; Investigate contributors; Create and implement a plan; Evaluate): pain, environment, unmet needs, and carer communication often drive symptoms more than "need for antipsychotic." Non-pharmacological strategies are first line. See the dedicated BPSD topic for deep dosing of antipsychotics and deprescribing.[16]
Cholinesterase inhibitors (symptomatic)
AChEIs produce modest average benefits on cognition and global measures; they are not disease-modifying cures. Cochrane evidence supports small benefits of donepezil in mild, moderate, or severe AD dementia over 12–24 week trials.[14]
| Agent | Exam-ready dosing (oral/patch) | Notes |
|---|---|---|
| Donepezil | Start 5 mg PO once daily for at least 4 weeks, then 10 mg once daily if tolerated | Most common first-line; GI effects, vivid dreams (timing), bradycardia |
| Rivastigmine | Oral start 1.5 mg PO twice daily, titrate every 2 weeks toward 3–6 mg twice daily as tolerated; patch 4.6 mg/24 h → 9.5 mg/24 h (higher patch strengths per product info where indicated) | Patch may improve GI tolerability; also used in PDD |
| Galantamine | Start 8 mg/day, titrate every 4 weeks toward 16–24 mg/day (IR/ER formulations per product information) | Also dual AChE inhibition / nicotinic modulation framing in some texts |
| Monitor nausea, vomiting, diarrhoea, anorexia, weight loss, insomnia/vivid dreams, urinary urgency, bradycardia/syncope. Review benefit at about 3 months and at least every 6–12 months; deprescribe if no meaningful benefit or harm outweighs benefit. Local authority/PBS criteria may govern initiation and continuing supply in ANZ — follow current product information and local rules.[14][20] |
Memantine (symptomatic)
Memantine is an NMDA-receptor antagonist used primarily for moderate-to-severe AD. Landmark evidence: Reisberg showed benefit versus placebo in moderate-to-severe AD; Tariot showed benefit of memantine added to stable donepezil versus donepezil plus placebo; Cochrane supports small benefits in moderate-to-severe AD with less clear benefit in mild disease.[11][12][15]
Exam-ready titration: start memantine 5 mg PO once daily, increase by 5 mg weekly to target 10 mg twice daily (or extended-release 28 mg once daily where available and appropriate). Renal impairment: dose-adjust per current product information (accumulation risk). Adverse effects include dizziness, headache, and confusion; review interactions and renal function.[11][12][15]
DOMINO-AD pearl
In moderate-to-severe AD, continued donepezil was associated with cognitive and functional benefits compared with withdrawal; memantine effects were smaller or mixed depending on outcome. Exam translation: do not automatically stop donepezil solely because the patient has entered moderate–severe stages if it is tolerated and still offering benefit; individualise combination decisions.[13]
Disease-modifying anti-amyloid therapies (awareness)
Monoclonal antibodies targeting amyloid are a rapidly evolving specialty pathway with eligibility constraints, ARIA risk, imaging surveillance, and highly variable regulatory and funding access by region and date. For psychiatry fellowship: state awareness, do not claim universal availability, and do not present them as a substitute for care planning, BPSD skill, or symptomatic pharmacology.[5][7]
Psychotropics for mood and psychosis
Treat major depression and anxiety thoughtfully (older-adult SSRI cautions including hyponatraemia and falls). Avoid chronic benzodiazepines and anticholinergic agents. Antipsychotics for severe psychosis or aggression only after non-drug approaches and medical exclusion: meta-analysis shows increased mortality with atypical antipsychotics in dementia; CATIE-AD demonstrated modest effectiveness with substantial discontinuation for intolerability or inefficacy. Counsel and document; time-limit and review.[17][18][20]
Special populations and scenarios
Young-onset AD (under 65). Broader differential, higher genetic yield, employment and dependent-children impact, and need for specialist memory and genetics pathways.[1]
Down syndrome. High lifetime AD risk; baseline cognitive disability complicates assessment — use longitudinal change and caregiver report.[7]
CALD and Indigenous peoples. Cognitive tools have validation limits; use interpreters, culturally safe assessment, and collateral who know premorbid function.[7]
Hospital CL. Delirium on AD background is the default for acute change; reinstate orientation aids, review high-risk meds, and plan safe discharge with carer capacity in mind.[16]
Prognosis and disposition
Course is progressive over years. Median survival after a dementia diagnosis is often roughly in a 4–8 year range depending on age, stage, comorbidity, and care setting — avoid false precision. Institutionalisation risk rises with BPSD, carer burnout, and loss of basic ADLs. Disposition ladder: home with supports → respite → residential aged care, with palliative care integration late. Memory clinic, old-age psychiatry, and geriatric medicine share care depending on neuropsychiatric complexity, medical multimorbidity, and local service design.[7][20]
Regional deltas
ANZ. Clinical diagnosis plus local authority/PBS criteria for AChEI and memantine initiation and continuation; state/territory Mental Health Act versus guardianship/administration for detention and substitute decision-making — quote principles (least restrictive, decision-specific capacity), not invented section numbers. UK. NICE dementia guidance emphasises non-drug care and structured AChEI/memantine pathways. US. APA Alzheimer guideline framework (note document age) plus FDA boxed warning on antipsychotic mortality in dementia-related psychosis.[17][20]
Exam pearls
- Probable AD (McKhann): insidious + progressive + amnestic or non-amnestic early lead + no better alternative explanation.[1]
- Mild vs major NCD: independence in everyday activities is the hinge, not a single MMSE cut-off.[1][2]
- ATN: A+T+ = biological AD in 2018 research terms; A+ alone = Alzheimer pathologic change; N is not disease-defining alone.[4]
- Donepezil 5 mg → 10 mg after at least 4 weeks; memantine titrate to 10 mg twice daily for moderate–severe disease; renal adjust memantine.[11][14]
- DOMINO-AD: continued donepezil still matters in moderate–severe AD.[13]
- BPSD: DICE first; antipsychotics increase mortality — last line, short course, counsel.[16][17]
- Capacity: understand, appreciate, reason, communicate choice.[19]
- Always exclude delirium and reversible factors before attributing decline solely to AD progression.[1][16]
AD exam spine
References
- [1]McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514250
- [2]Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514249
- [3]Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514248
- [4]Jack CR Jr, Bennett DA, Blennow K, et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer's disease Alzheimers Dement, 2018.PMID 29653606
- [5]Jack CR Jr, Andrews JS, Beach TG, et al. Revised criteria for diagnosis and staging of Alzheimer's disease: Alzheimer's Association Workgroup Alzheimers Dement, 2024.PMID 38934362
- [6]Dubois B, Feldman HH, Jacova C, et al. Research criteria for the diagnosis of Alzheimer's disease: revising the NINCDS-ADRDA criteria Lancet Neurol, 2007.PMID 17616482
- [7]Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission Lancet, 2020.PMID 32738937
- [8]Folstein MF, Folstein SE, McHugh PR "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician J Psychiatr Res, 1975.PMID 1202204
- [9]Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [10]Cummings JL, Mega M, Gray K, et al. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia Neurology, 1994.PMID 7991117
- [11]Reisberg B, Doody R, Stöffler A, et al. Memantine in moderate-to-severe Alzheimer's disease N Engl J Med, 2003.PMID 12672860
- [12]Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial JAMA, 2004.PMID 14734594
- [13]Howard R, McShane R, Lindesay J, et al. Donepezil and memantine for moderate-to-severe Alzheimer's disease N Engl J Med, 2012.PMID 22397651
- [14]Birks JS, Harvey RJ Donepezil for dementia due to Alzheimer's disease Cochrane Database Syst Rev, 2018.PMID 29923184
- [15]McShane R, Westby MJ, Roberts E, et al. Memantine for dementia Cochrane Database Syst Rev, 2019.PMID 30891742
- [16]Kales HC, Gitlin LN, Lyketsos CG Assessment and management of behavioral and psychological symptoms of dementia BMJ, 2015.PMID 25731881
- [17]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [18]Schneider LS, Tariot PN, Dagerman KS, et al. Effectiveness of atypical antipsychotic drugs in patients with Alzheimer's disease N Engl J Med, 2006.PMID 17035647
- [19]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [20]APA Work Group on Alzheimer's Disease and other Dementias, Rabins PV, Blacker D, et al. American Psychiatric Association practice guideline for the treatment of patients with Alzheimer's disease and other dementias. Second edition Am J Psychiatry, 2007.PMID 18340692