Psych · Old age psychiatry — dementia neuropsychiatry
Behavioural and psychological symptoms of dementia
Also known as BPSD · Neuropsychiatric symptoms of dementia · NPS dementia · Dementia-related behavioural disturbance · Agitation in dementia · Psychosis of Alzheimer disease · Behavioural symptoms of dementia
Exam-exhaustive fellowship reference on behavioural and psychological symptoms of dementia (BPSD/NPS) — domains and NPI framing; multifactorial drivers including pain; DICE assessment; non-drug first-line care; antipsychotic mortality and stroke risk; CATIE-AD, DART-AD, CitAD, HTA-SADD; deprescribing; carer support. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Behavioural and psychological symptoms of dementia (BPSD), also called neuropsychiatric symptoms (NPS), drive carer distress, hospitalisation and residential care more often than pure memory loss. Fellowship exams test whether you default to a sedating tablet or whether you can formulate the behaviour, exclude delirium and pain, deploy non-pharmacological care, and use psychotropics with eyes open to black-box harms.[1][5]
Overview and definition
BPSD refers to the non-cognitive behavioural and psychological features that commonly accompany dementia syndromes: agitation and aggression, psychosis, depression and anxiety, apathy, sleep–wake disruption, disinhibition, aberrant motor behaviour, and appetite change. The IPA consensus framed these as behavioural and psychological signs and symptoms of dementia requiring systematic research and treatment approaches rather than informal dismissal as "just dementia."[1]
BPSD is not a single disease. Each domain can have different drivers (pain versus paranoid misinterpretation versus frontal disinhibition). ICD-11 and DSM-5-TR code the underlying major neurocognitive disorder and allow additional specification of behavioural disturbance; they do not replace a formulation of this person's agitation at 3 pm after personal care.[1][5]
Classification and symptom domains
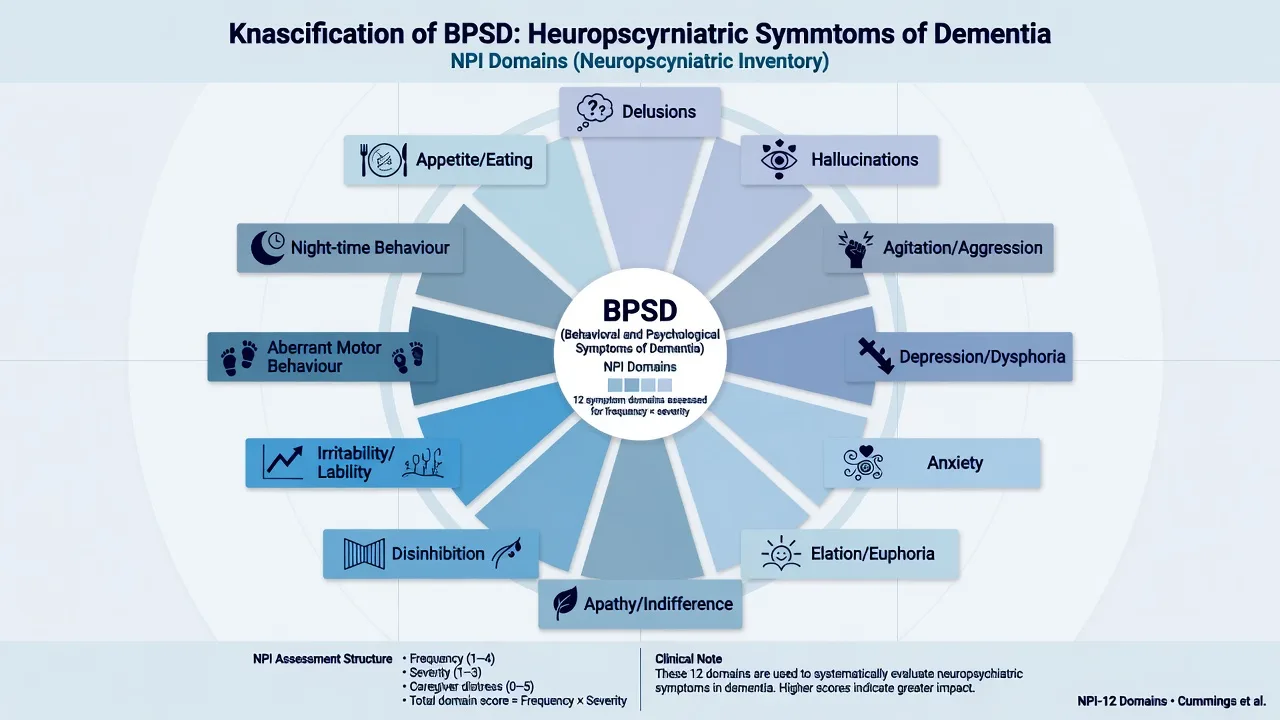
The Neuropsychiatric Inventory (NPI) is the classic multi-domain instrument: delusions, hallucinations, agitation/aggression, depression/dysphoria, anxiety, elation/euphoria, apathy/indifference, disinhibition, irritability/lability, aberrant motor behaviour, night-time behaviour, and appetite/eating change. Frequency and severity generate domain scores; carer distress is scored separately — a critical teaching point because distress, not only symptom intensity, drives institutionalisation.[2]
Agitation / aggression
- Verbal aggression, physical resistance, pacing, restlessness
- Often care-triggered (personal care, toileting)
- CMAI-style clusters useful for staff documentation
- High-risk for chemical restraint misuse
Psychosis
- Delusions of theft, abandonment, misidentification
- Visual hallucinations (think DLB differential)
- Phantom boarder / Capgras-like themes
- Not always distressing — treat distress and risk
Affective / apathy
- Depression: sadness, guilt, anhedonia, suicidal ideas
- Apathy: reduced initiative without sadness
- Anxiety and irritability common
- Apathy ≠ depression — treatment paths diverge
Sleep / motor / other
- Sundowning, reversed sleep–wake cycle
- Wandering, pacing, shadowing
- Disinhibition (esp. behavioural-variant FTD)
- Appetite change, hyperorality
Epidemiology and risk factors
Headline epidemiology for viva recall
Population studies show neuropsychiatric symptoms are highly prevalent in dementia and also appear in mild cognitive impairment at lower rates. The Cache County Study documented high point prevalence and near-universal period prevalence of NPS over five years among people with dementia — meaning a "behaviour-free" course is the exception, not the rule.[3][4]
Risk amplifiers. Greater dementia severity; specific aetiologies (visual hallucinations in DLB/PDD; disinhibition in bvFTD; mixed patterns in AD and vascular dementia); male sex for some aggression phenotypes; sensory impairment; pain; constipation and urinary retention; infection; dehydration; polypharmacy (especially anticholinergics and benzodiazepines); noisy or under-stimulating environments; disrupted routine; and high carer distress with skill–demand mismatch.[5]
Pathophysiology
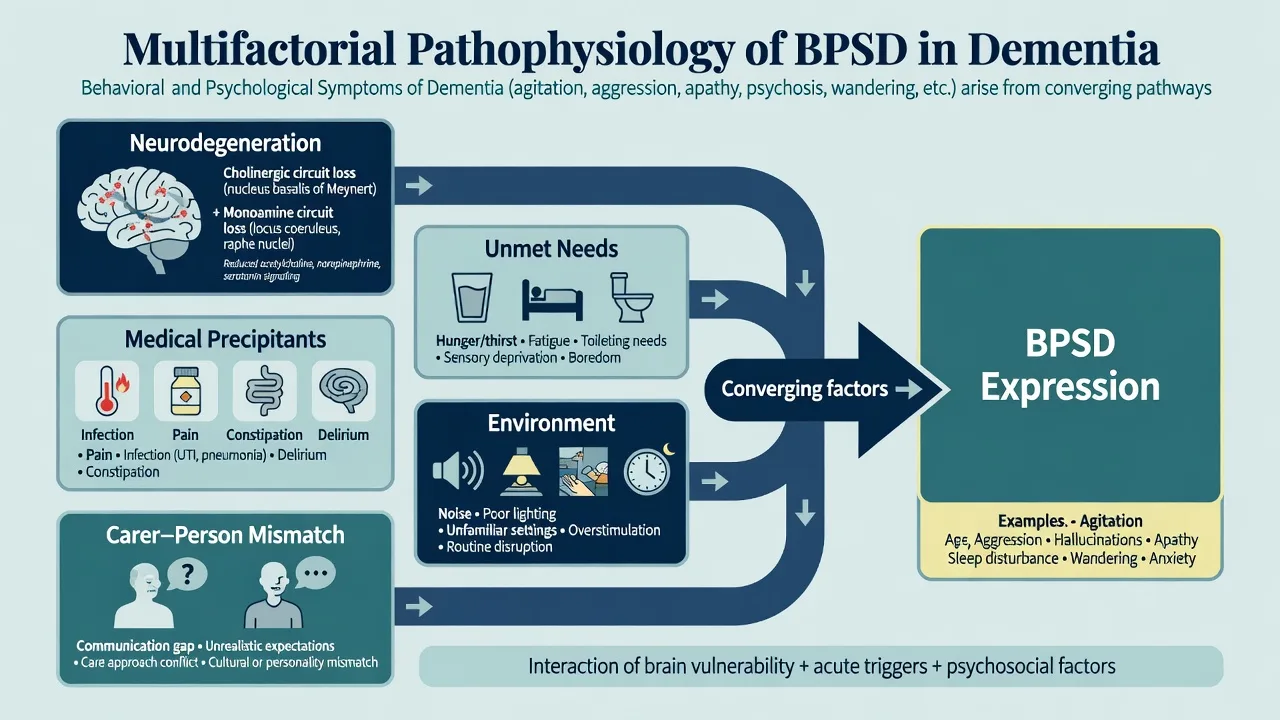
Examiners want a biopsychosocial cascade, not a single-neurotransmitter slogan.[5]
Neurobiology. Progressive loss of cholinergic, serotonergic, noradrenergic and dopaminergic innervation and frontotemporal–limbic circuit disruption alter stress reactivity, reward, sleep and reality testing. DLB pathology confers extreme neuroleptic sensitivity. Fronto-subcortical circuits in bvFTD explain disinhibition and loss of social cognition.[5]
Medical precipitants. Pain, delirium, infection (especially UTI and pneumonia), constipation, urinary retention, hypoxia, electrolyte disturbance, hypoglycaemia, and drug toxicity or withdrawal can convert a stable person into an agitated crisis overnight.[5][12]
Unmet needs and environment. Hunger, thirst, boredom, under- or over-stimulation, poor lighting, noise, and unfamiliar staff approaches produce behaviours that look "psychiatric" but are communications of need.[5][13]
Interpersonal cycle. Carer exhaustion and harsh or inconsistent approaches escalate resistance; skilled, calm, person-centred approaches de-escalate. This is formulation, not blame.[14]
Clinical presentation
Presentations cluster by domain and setting.[1][5]
Agitation. Calling out, pacing, resisting care, striking during personal care, exit-seeking. Often worse at transition times (sundowning). Document time, place, people present, and what immediately preceded the event (ABC chart).[5]
Psychosis. Delusions of theft are classic in Alzheimer disease; visual hallucinations of people or animals raise DLB suspicion when combined with REM sleep behaviour disorder, parkinsonism, and fluctuations. Misidentification (spouse is an impostor; house is not home) is common and highly distressing for families.[2][5]
Depression versus apathy. Depression carries dysphoria, tearfulness, worthlessness and sometimes suicidal ideation. Apathy is reduced motivation and emotional reactivity without the affective pain of depression — common, disabling, and poorly responsive to antidepressants or antipsychotics.[5][16]
Sleep. Fragmented night sleep, daytime napping, nocturnal wandering, and reversed circadian rhythm amplify daytime aggression and carer burnout.[5]
MSE in moderate–severe dementia. Rely on observation and collateral: affect, spontaneous speech, agitation level, psychotic content if expressible, insight (usually limited), and risk behaviours. Do not expect a textbook subjective history.[5]
Differential diagnosis
Delirium
- Acute onset, fluctuating course
- Inattention is core
- Medical driver almost always present
- Never attribute pure delirium to 'BPSD' alone
Primary psychiatric illness
- Late-life depression, bipolar mania, late-onset psychosis
- History of primary psychiatric disorder helps
- Dementia may coexist (dual formulation)
- Avoid diagnostic overshadowing either way
Medication / substance
- Anticholinergics, opioids, benzos, steroids
- Alcohol withdrawal in hospitalised elders
- Akathisia from antipsychotics misread as agitation
- Review the entire chart, not just psychotropics
Medical pain drivers
- Arthritis, fracture, pressure injury
- Dental pain, urinary retention, constipation
- Otitis, headache, ischaemic pain
- Treat pain before escalating psychotropics
Also consider sensory deprivation, grief, major environmental change (new RACF), and elder abuse or neglect presenting as "behaviour."[5]
Clinical and bedside assessment — DICE and ABC
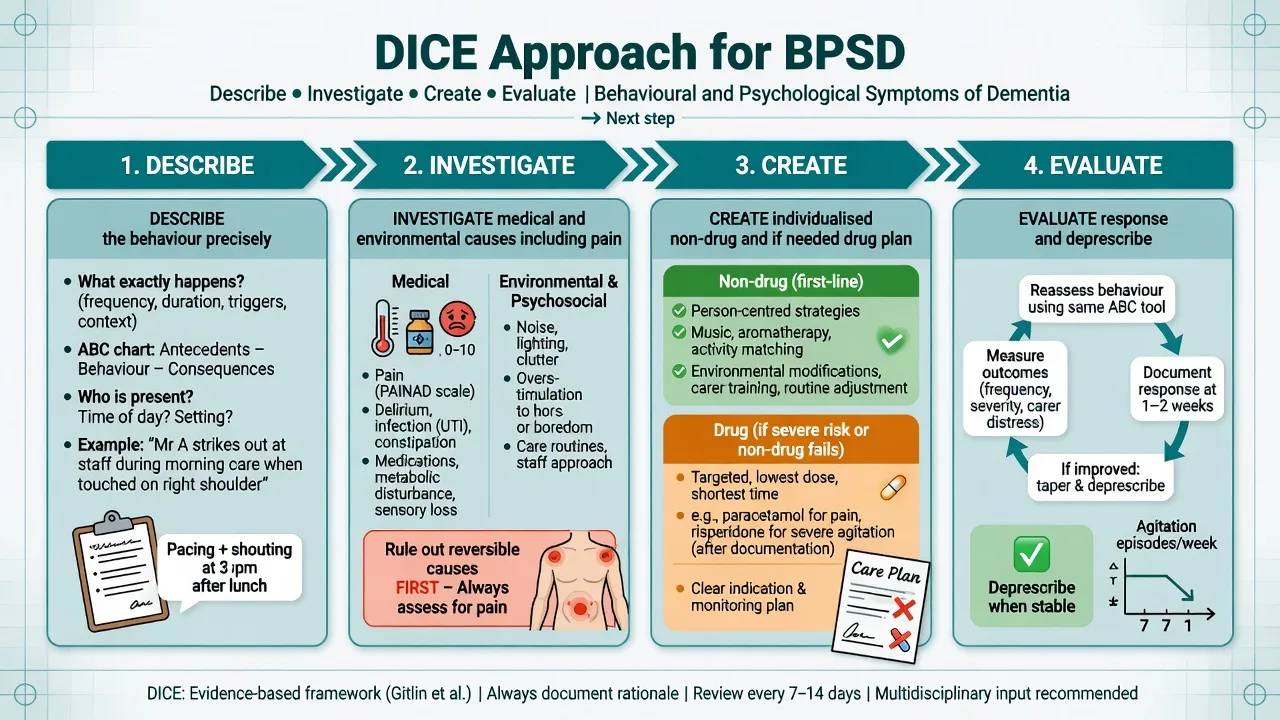
DICE (Describe–Investigate–Create–Evaluate) is the examiner-friendly scaffold from modern BPSD guidance: define the behaviour precisely; investigate person, carer and environmental contributors including medical causes; create a tailored plan prioritising non-drug strategies; evaluate response and modify, including deprescribing.[5]
ABC analysis. Antecedent → Behaviour → Consequence charts convert vague "aggressive all day" into measurable patterns staff can change (e.g. aggression only during showering with cold water and rushed approach).[5]
Always assess. Capacity for relevant decisions; vulnerability and elder-abuse risk; carer burden and safety; legal status principles under local Mental Health and Guardianship frameworks (jurisdiction-specific statutes — do not invent section numbers).[5]
Scales. NPI or NPI-Nursing Home versions track domains; Cohen-Mansfield Agitation Inventory (CMAI) is used for agitation research and facility audits. Scales guide measurement-based review; they do not replace diagnosis of delirium or pain.[2]
Investigations
Think delirium panel plus targeted extras, not endless imaging.[5]
Typical first-line when behaviour changes acutely: vital signs; fingerstick glucose; urinalysis/culture as indicated; FBC, CRP/ESR as available, U&E, calcium, LFTs; medication reconciliation; ECG before psychotropics (QTc, rate); consider chest imaging if infection suspected. TSH, B12 when not recently checked or presentation is subacute. Neuroimaging for new focal neurology, head injury, or rapid atypical decline — not for every chronic pacing resident.[5]
Management — acute safety (resuscitation)
In dementia with Lewy bodies, avoid first-generation antipsychotics entirely when possible; even second-generation agents can precipitate severe rigidity, sedation and mortality. Prioritise cholinesterase inhibitors for some neuropsychiatric features in DLB pathways and specialist advice.[5]
Benzodiazepines may calm briefly but increase falls, confusion and paradoxical agitation in older adults; avoid as chronic BPSD therapy.[5]
Management — definitive and stepwise
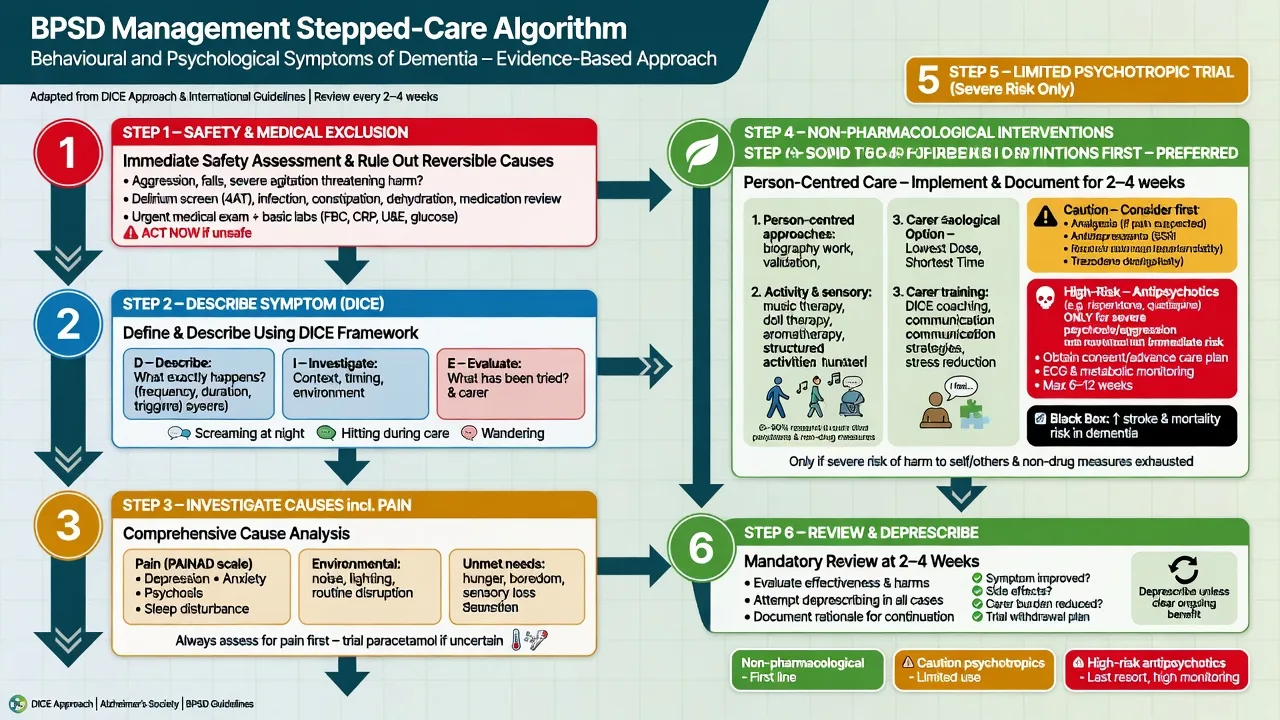
1. Non-pharmacological care first
Person-centred care, structured activities, music and sensory approaches, environmental modification (noise, lighting, wayfinding), consistent routines, and carer/staff training have the best risk–benefit profile. Meta-analysis of non-pharmacological interventions delivered to family carers shows meaningful reductions in NPS; systematic reviews of agitation interventions support multi-component, person-centred approaches over isolated gimmicks.[13][14]
2. Treat pain and medical drivers
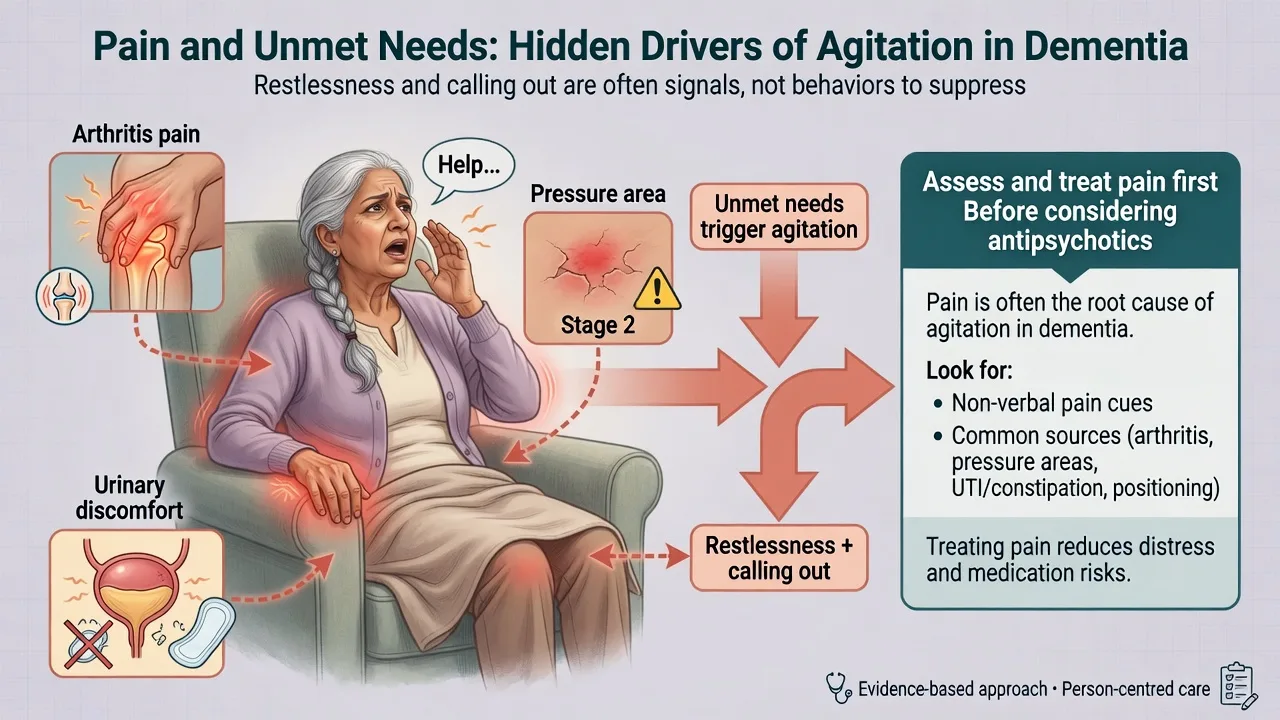
A cluster randomised trial of a stepwise pain protocol in nursing-home residents with dementia reduced behavioural disturbances — a high-yield exam pearl: analgesia before antipsychotic when pain is plausible. Regular paracetamol is commonly first-line for suspected musculoskeletal pain if no contraindication; escalate per geriatric pain pathways with attention to renal function and falls.[12]
3. When psychotropics are considered
Document: target symptom (e.g. physical aggression risking fracture, not "wandering"); severity and risk; non-drug measures already tried; discussion with substitute decision-maker; review date; monitoring plan.[5][6]
Antipsychotics — efficacy is modest. CATIE-AD found limited effectiveness of olanzapine, quetiapine and risperidone versus placebo for psychosis/aggression/agitation in outpatients with Alzheimer disease, with substantial discontinuation for intolerability or inefficacy. Cochrane review supports some benefit of atypicals for aggression and psychosis in AD but highlights adverse effects. Off-label use meta-analysis confirms small benefits and clear harms in elderly dementia populations.[7][8][17][18]
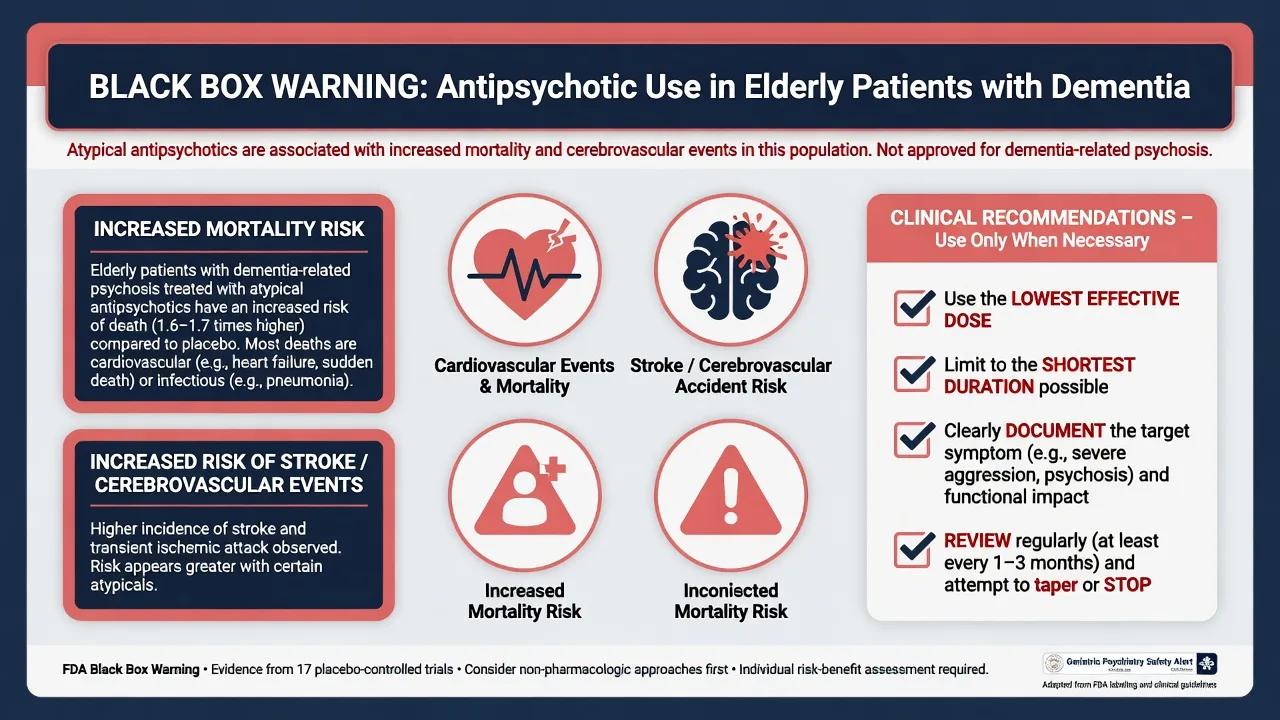
Antipsychotics — harms you must state. Schneider meta-analysis of RCTs: atypical antipsychotics increase risk of death versus placebo in dementia (order of magnitude ~1.5–1.7-fold in classic teaching of the black-box data). Observational work (Gill et al.) also links antipsychotic exposure to higher mortality. Cerebrovascular adverse events, including stroke, were signalled in risperidone dementia trials and regulatory warnings. Class effects include sedation, parkinsonism, falls, metabolic disturbance, QTc prolongation and pneumonia risk.[6][19][20]
Practical dosing principles (illustrative adult older-person ranges — individualise, check local product information). Risperidone is often started at 0.25–0.5 mg orally once or twice daily (commonly staying at or under 1–2 mg total daily in dementia populations); olanzapine examples start around 2.5 mg orally at night; quetiapine examples start around 12.5–25 mg orally when EPS risk is high — always with review within 1–2 weeks and a plan to taper when stable.[5][7][18]
| Agent | Typical starting approach in frail older adult with severe BPSD | Monitoring notes |
|---|---|---|
| Risperidone | Low oral start; titrate slowly; keep total daily dose modest in dementia | EPS, prolactin, stroke risk, falls; region-specific limited licence for severe Alzheimer aggression/psychosis — know local PI wording |
| Olanzapine | Low night-time oral start; caution metabolic/sedation | Glucose, weight, sedation, anticholinergic load |
| Quetiapine | Low oral start; sometimes used when EPS risk high | Sedation, orthostasis, QTc; evidence of efficacy in CATIE-AD was weak |
| Avoid | Typical antipsychotics in DLB; high-dose polypharmacy "cocktails" | Neuroleptic sensitivity, oversedation |
Australia/NZ practice note. Risperidone historically has had more explicit product-information wording for certain severe behavioural disturbances in Alzheimer dementia than many other atypicals, but the black-box mortality and stroke concerns still apply. Prefer non-drug care; if used, lowest dose, shortest time, documented indication, and active deprescribing. Check current TGA/Medsafe product information and local health-service BPSD protocols rather than memorising obsolete package inserts.[5][6][20]
4. Antidepressants and other agents
CitAD: citalopram reduced agitation versus placebo in Alzheimer disease but with cognitive adverse effects and QTc concerns at the trial doses used — if an SSRI is considered for agitation, prefer cautious dosing, ECG awareness, and avoid high-dose citalopram in older adults.[15]
HTA-SADD: sertraline and mirtazapine were not clinically superior to placebo for depression in dementia and had more adverse events — do not assume "any low mood in dementia gets an antidepressant."[16]
Memantine is a cognition/stage drug; a dedicated agitation RCT (MAGD) did not support memantine as an effective anti-agitation treatment.[21]
Cholinesterase inhibitors may help some NPS in selected dementias (especially DLB pathways) as part of broader management, but they are not acute tranquillisers.[5]
5. Deprescribing
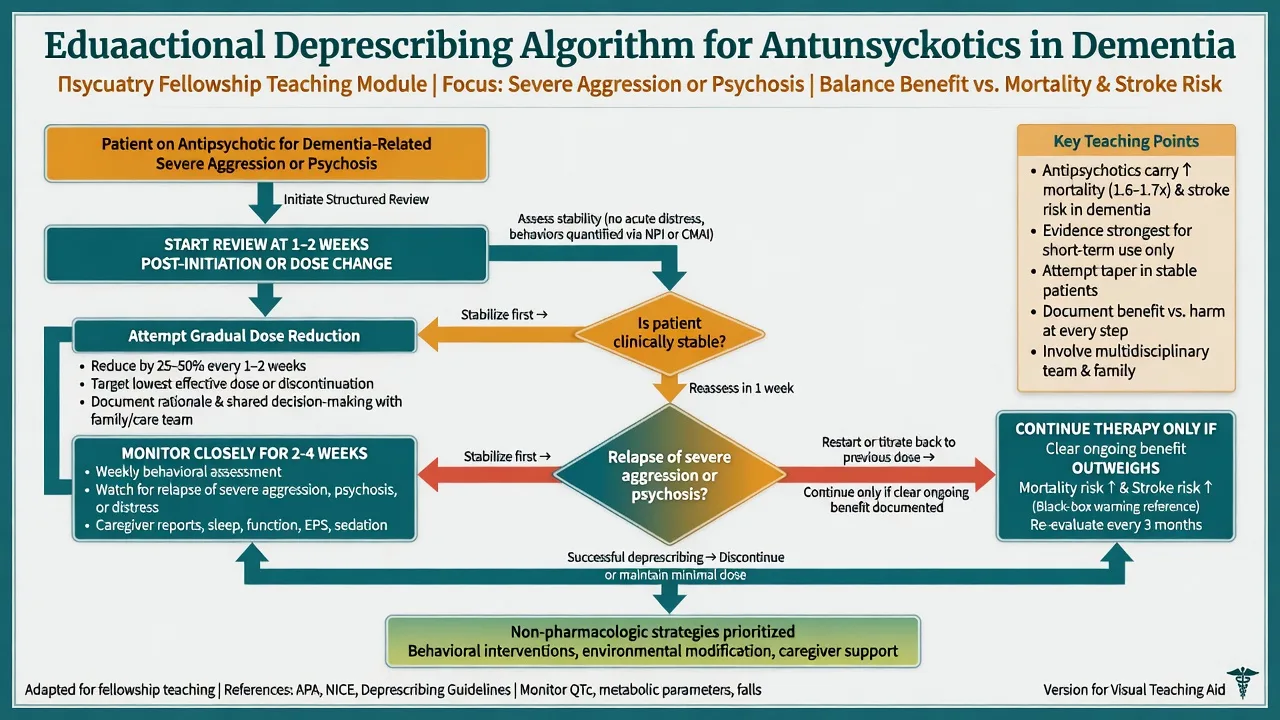
DART-AD showed that continuing neuroleptics offered little ongoing cognitive/functional advantage for many, and long-term follow-up raised serious mortality concerns with continued antipsychotic treatment. Devanand et al. showed that among responders to risperidone, discontinuation increased relapse risk of psychosis/agitation versus continuation — so deprescribing is not "always stop tomorrow," but "plan a supervised taper with a restart threshold."[9][10][11]
Practical approach: if stable for weeks without severe risk behaviours, reduce dose by roughly one-quarter to one-half every 1–2 weeks while reinforcing non-drug strategies; monitor NPI/CMAI-style targets, sleep, falls and EPS; restart or up-titrate only if severe aggression/psychosis returns with risk.[5][11]
6. Carer support
Psychoeducation, skills training, respite, and structured multi-component carer interventions reduce NPS and carer distress. Address sleep of the carer, financial strain, and abuse risk. Carer training is not optional soft care — it is evidence-based treatment.[14]
Specific subtypes and scenarios
Severe agitation/aggression. Safety → medical exclusion → pain protocol → environment/ABC → only then consider low-dose antipsychotic short course if risk remains high.[5][12]
Psychosis. Treat when distressing or dangerous. Visual hallucinations plus fluctuations/parkinsonism → DLB work-up and neuroleptic caution.[5]
Depression. Psychological and social activation approaches; antidepressants only with clear syndromal depression and monitoring — remember HTA-SADD.[16]
Apathy. Structured activity, stimulation, carer coaching; avoid antipsychotics as "activators."[5]
Sleep disturbance. Daytime light and activity, reduce caffeine/alcohol, treat pain and nocturia, limit night noise; avoid chronic benzodiazepines/Z-drugs as first-line.[5]
bvFTD disinhibition. Environmental controls, carer strategies, and specialist behavioural neurology/psychiatry input; antipsychotics have limited disease-modifying logic and high side-effect cost.[5]
Complications and pitfalls
- Using antipsychotics for wandering, calling out, or mild irritability (wrong targets).[5]
- Missing delirium, pain, constipation, retention, or akathisia.[5][12]
- Typical antipsychotics in DLB.[5]
- Chronic benzodiazepines for "settling."[5]
- No review date / never deprescribing despite stability.[9][10]
- Ignoring carer burnout and elder abuse.[5]
- Treating apathy as depression with escalating polypharmacy.[16]
Prognosis and disposition
Many BPSD episodes improve when precipitants are fixed and non-drug care is consistent; symptoms also fluctuate with dementia stage. Persistent high-risk aggression and psychosis increase residential-care placement. Disposition ladder: optimised home care with community aged-psychiatry support → respite → residential aged care with behaviour-support plans → inpatient psychogeriatric or medical admission for unsafe community management. Follow-up intensity tracks risk and recent medication changes.[3][4][5]
Special populations
DLB/PDD. Neuroleptic sensitivity is life-threatening; prefer non-drug care and cholinesterase inhibitors where indicated; specialist advice before any antipsychotic.[5]
Vascular dementia. Already elevated stroke risk — antipsychotic CVA harm is especially salient.[20]
Intellectual disability with acquired dementia. Dual disability services, sensory formulations, and careful capacity/guardianship pathways.[5]
Cultural and linguistic diversity / Indigenous older adults. Use interpreters, family decision structures, and culturally safe behavioural formulations; do not misread cultural expression as psychosis.[5]
Evidence, guidelines and regional differences
Landmark evidence set for exams: IPA consensus framing; NPI; CHS and Cache County epidemiology; Kales DICE/BMJ management review; Schneider mortality meta-analysis; CATIE-AD effectiveness; Ballard Cochrane; DART-AD withdrawal and mortality follow-up; Devanand discontinuation relapse; Husebo pain protocol; Brodaty and Livingston non-pharmacological evidence; CitAD; HTA-SADD; Gill mortality cohort; Wooltorton CVA signal; MAGD memantine; US brexpiprazole agitation RCT.[1][2][3][4][5][6][7][9][10][11][12][13][14][15][16][22]
Regional deltas centre on product licensing (risperidone wording), NICE versus APA versus local ANZ health-service pathways, and US-specific labelling for brexpiprazole agitation — principles of non-drug first and black-box harm are shared.[5][22]
Exam pearls
DICE
- CATIE-AD: modest benefit, high discontinuation — not a miracle class.[7][8]
- Schneider: atypical antipsychotics increase death risk in dementia RCTs.[6]
- DART-AD long-term: continuing neuroleptics linked to higher mortality signal — deprescribe thoughtfully.[10]
- Devanand: some risperidone responders relapse on stop — monitor during taper.[11]
- HTA-SADD: sertraline/mirtazapine not better than placebo for depression in dementia.[16]
- Apathy is not depression; wandering is not an antipsychotic indication.[5]
- DLB: never reach first for haloperidol.[5]
Self-test: 82-year-old with Alzheimer disease hitting staff at shower time
Best first moves? Describe ABC (shower, cold bathroom, rushed approach). Examine for pain and constipation. Trial warmer room, two-staff technique, music, and analgesia if indicated. Only if severe ongoing risk after medical and non-drug optimisation, consider risperidone 0.25–0.5 mg orally with stroke/death discussion, falls monitoring, and review in 1–2 weeks for taper. Check DLB features before any antipsychotic.[5][6][12]
References
- [1]Finkel SI, Costa e Silva J, Cohen G, Miller S, Sartorius N Behavioral and psychological signs and symptoms of dementia: a consensus statement on current knowledge and implications for research and treatment Int Psychogeriatr, 1996.PMID 9154615
- [2]Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia Neurology, 1994.PMID 7991117
- [3]Lyketsos CG, Lopez O, Jones B, Fitzpatrick AL, Breitner J, DeKosky S Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study JAMA, 2002.PMID 12243634
- [4]Steinberg M, Shao H, Zandi P, Lyketsos CG, Welsh-Bohmer KA, Norton MC, et al. Point and 5-year period prevalence of neuropsychiatric symptoms in dementia: the Cache County Study Int J Geriatr Psychiatry, 2008.PMID 17607801
- [5]Kales HC, Gitlin LN, Lyketsos CG Assessment and management of behavioral and psychological symptoms of dementia BMJ, 2015.PMID 25731881
- [6]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [7]Schneider LS, Tariot PN, Dagerman KS, Davis SM, Hsiao JK, Ismail MS, et al. Effectiveness of atypical antipsychotic drugs in patients with Alzheimer's disease N Engl J Med, 2006.PMID 17035647
- [8]Sultzer DL, Davis SM, Tariot PN, Dagerman KS, Lebowitz BD, Lyketsos CG, et al. Clinical symptom responses to atypical antipsychotic medications in Alzheimer's disease: phase 1 outcomes from the CATIE-AD effectiveness trial Am J Psychiatry, 2008.PMID 18519523
- [9]Ballard C, Lana MM, Theodoulou M, Douglas S, McShane R, Jacoby R, et al. A randomised, blinded, placebo-controlled trial in dementia patients continuing or stopping neuroleptics (the DART-AD trial) PLoS Med, 2008.PMID 18384230
- [10]Ballard C, Hanney ML, Theodoulou M, Douglas S, McShane R, Kossakowski K, et al. The dementia antipsychotic withdrawal trial (DART-AD): long-term follow-up of a randomised placebo-controlled trial Lancet Neurol, 2009.PMID 19138567
- [11]Devanand DP, Mintzer J, Schultz SK, Andrews HF, Sultzer DL, de la Pena D, et al. Relapse risk after discontinuation of risperidone in Alzheimer's disease N Engl J Med, 2012.PMID 23075176
- [12]Husebo BS, Ballard C, Sandvik R, Nilsen OB, Aarsland D Efficacy of treating pain to reduce behavioural disturbances in residents of nursing homes with dementia: cluster randomised clinical trial BMJ, 2011.PMID 21765198
- [13]Livingston G, Kelly L, Lewis-Holmes E, Baio G, Morris S, Patel N, et al. Non-pharmacological interventions for agitation in dementia: systematic review of randomised controlled trials Br J Psychiatry, 2014.PMID 25452601
- [14]Brodaty H, Arasaratnam C Meta-analysis of nonpharmacological interventions for neuropsychiatric symptoms of dementia Am J Psychiatry, 2012.PMID 22952073
- [15]Porsteinsson AP, Drye LT, Pollock BG, Devanand DP, Frangakis C, Ismail Z, et al. Effect of citalopram on agitation in Alzheimer disease: the CitAD randomized clinical trial JAMA, 2014.PMID 24549548
- [16]Banerjee S, Hellier J, Dewey M, Romeo R, Ballard C, Baldwin R, et al. Sertraline or mirtazapine for depression in dementia (HTA-SADD): a randomised, multicentre, double-blind, placebo-controlled trial Lancet, 2011.PMID 21764118
- [17]Maher AR, Maglione M, Bagley S, Suttorp M, Hu JH, Ewing B, et al. Efficacy and comparative effectiveness of atypical antipsychotic medications for off-label uses in adults: a systematic review and meta-analysis JAMA, 2011.PMID 21954480
- [18]Ballard C, Waite J The effectiveness of atypical antipsychotics for the treatment of aggression and psychosis in Alzheimer's disease Cochrane Database Syst Rev, 2006.PMID 16437455
- [19]Gill SS, Bronskill SE, Normand SL, Anderson GM, Sykora K, Lam K, et al. Antipsychotic drug use and mortality in older adults with dementia Ann Intern Med, 2007.PMID 17548409
- [20]Wooltorton E Risperidone (Risperdal): increased rate of cerebrovascular events in dementia trials CMAJ, 2002.PMID 12451085
- [21]Fox C, Crugel M, Maidment I, Auestad BH, Coulton S, Treloar A, et al. Efficacy of memantine for agitation in Alzheimer's dementia: a randomised double-blind placebo controlled trial PLoS One, 2012.PMID 22567095
- [22]Lee D, Slomkowski M, Hefting N, Chen D, Larsen KG, Kohegyi E, et al. Brexpiprazole for the Treatment of Agitation in Alzheimer Dementia: A Randomized Clinical Trial JAMA Neurol, 2023.PMID 37930669