Psych · Old age psychiatry — capacity, guardianship and end of life
Capacity, guardianship and end-of-life decisions
Also known as Decision-making capacity in older adults · Guardianship and substitute decision-making · Advance care planning psychiatry · End-of-life capacity assessment · Appelbaum capacity geriatric psychiatry · Palliative psychiatry end of life · Surrogate decision-making older adults
Exam-exhaustive fellowship reference on capacity, guardianship and end-of-life decisions in older adults — Appelbaum–Grisso four abilities, dementia and delirium capacity gradients, guardianship and surrogate frameworks without invented statutes, advance care planning and directives, goals-of-care discussions, and palliative psychiatric issues including depression and desire for hastened death. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Old-age psychiatry examiners test the full arc from bedside capacity through substitute decision-making to goals of care. Candidates fail when they globalise incapacity from a Mini-Mental score, confuse Mental Health Act powers with medical consent, invent guardianship sections, or treat a request for death as either pure “psychosis” or pure “autonomy” without assessment.[2][5][16]

Overview and definitions
Decision-making capacity is a clinical judgment about a specific decision at a specific time. Legal competence (terms vary by jurisdiction) often denotes a formal status determination by a court or tribunal (for example guardianship). Clinicians assess capacity at the bedside; tribunals resolve contested status and appoint decision-makers when required.[1][2][20]
Informed consent (or informed refusal) requires capacity for that decision, material information, and voluntariness free from coercion or undue influence.[2][5]
| Principle | Clinical meaning in old age |
|---|---|
| Presumption of capacity | Age and dementia diagnosis do not reverse the presumption |
| Decision-specific | Capacity for simple analgesia is not capacity for complex chemotherapy or residential placement |
| Time-specific | Delirium and settling depression create windows of recovery |
| Unwise ≠ incapable | A capable older person may refuse recommended care |
| Supports first | Hearing aids, interpreters, timing, simplified language before substitution |
Classification — Appelbaum four abilities and related constructs
The modern functional model derives from Appelbaum and Grisso: capacity rests on four abilities rather than diagnosis alone.[1][2]
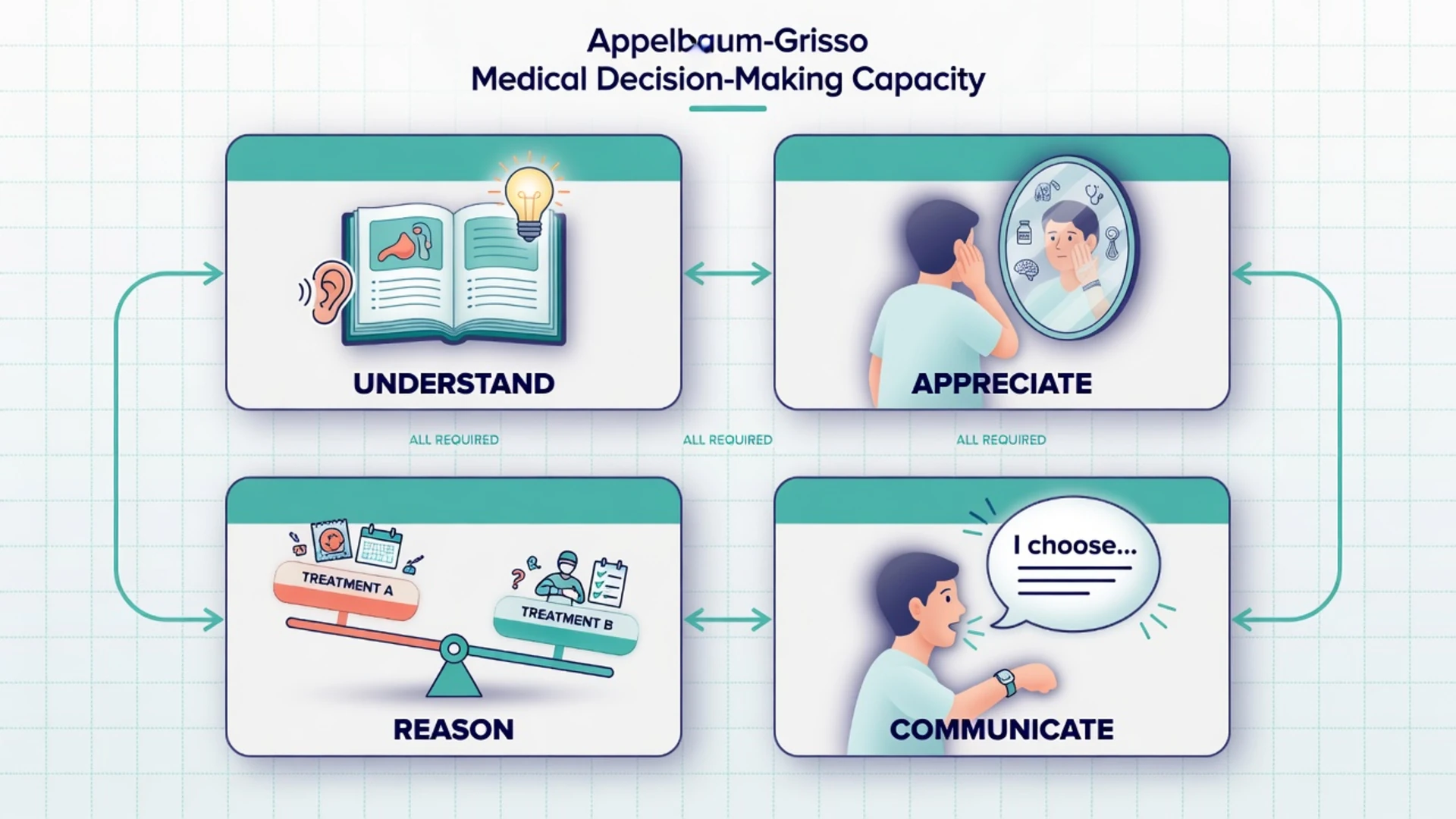
| Ability (Appelbaum/Grisso) | Exam-style wording | Bedside probe in older adults |
|---|---|---|
| Understand relevant information | Understand / retain | Teach-back of condition, proposed option, main risks and alternatives |
| Appreciate situation and consequences | Apply to self | Does the person accept that the illness and risks apply to them? |
| Reason about options | Use or weigh | Compare options with a consistent rationale linked to values |
| Express a choice | Communicate | Stable choice by speech, writing, or reliable alternative means |
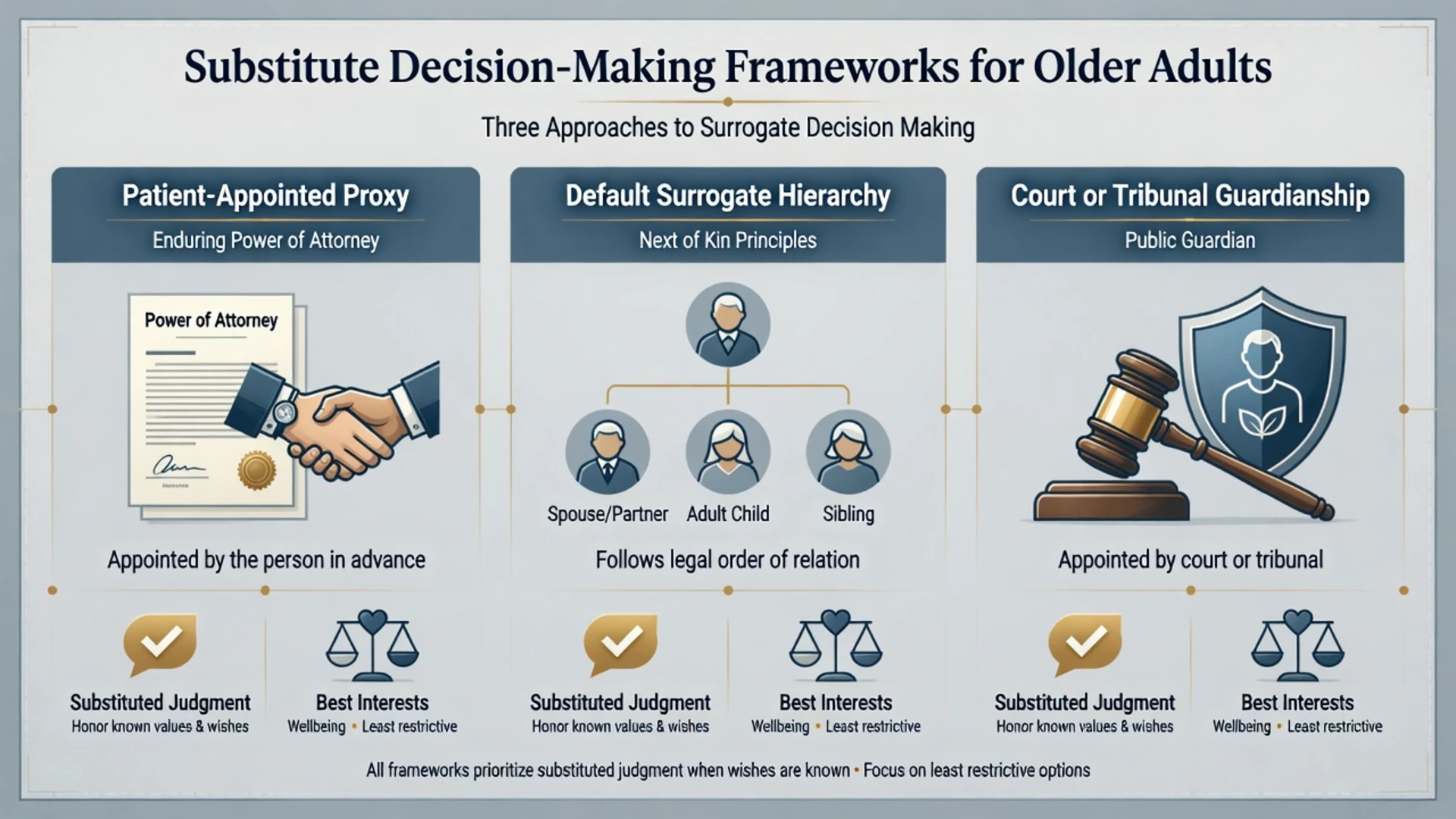
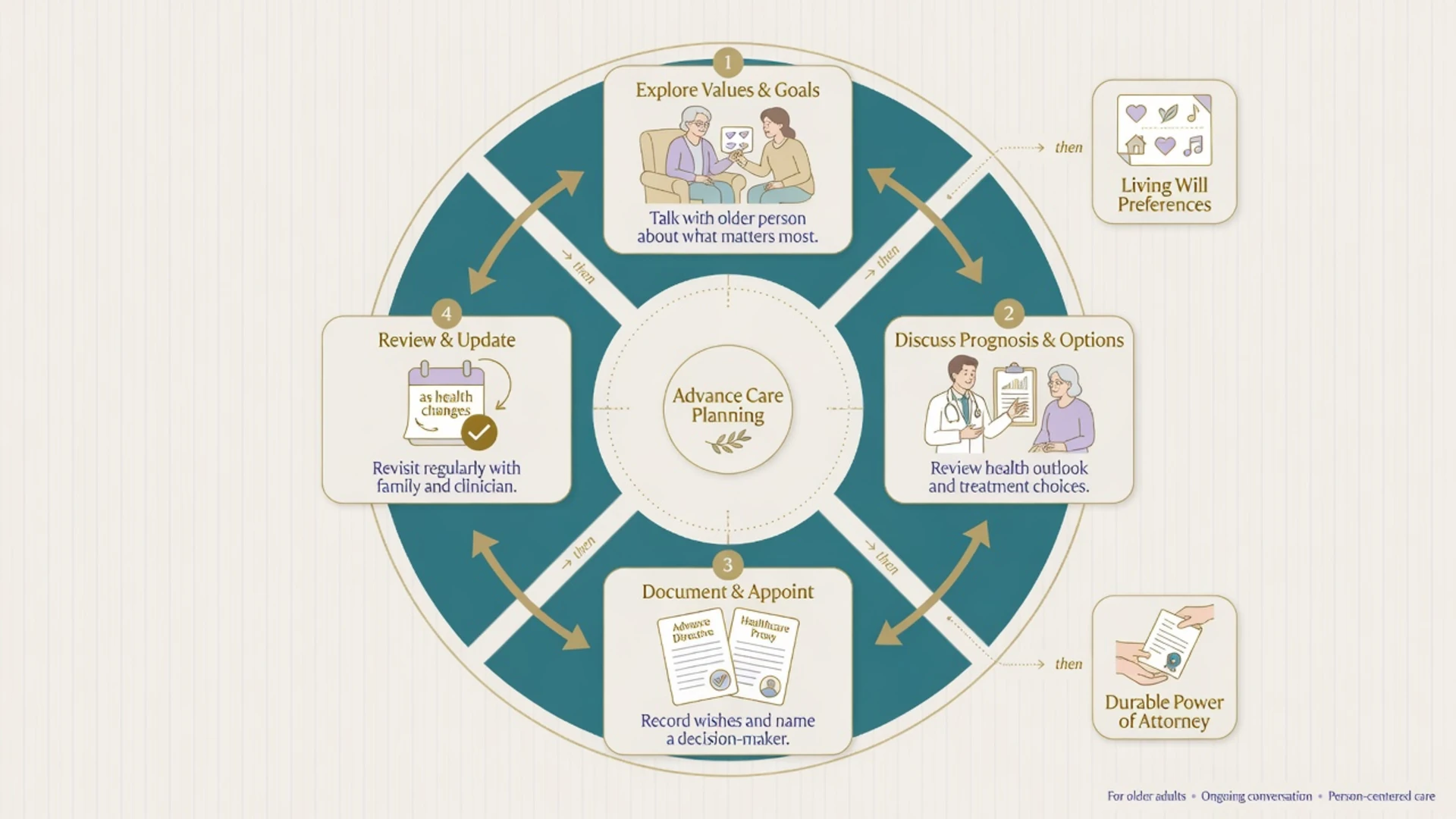
Related constructs (do not conflate): advance care planning (ACP) is an iterative communication process preparing patients and surrogates for future decisions; advance directives/living wills document treatment preferences; enduring/durable powers of attorney appoint a healthcare proxy while the person is still capacious; guardianship/administration is court or tribunal appointment when capacity is lacking for personal or financial domains (scope is jurisdiction-specific); substituted judgment decides as the person would have decided given their values; best interests promotes welfare with past and present wishes, beliefs, and least restriction when preferences are incomplete.[8][9][16]
Epidemiology and risk
Mental incapacity is common among medical inpatients; cognitive impairment and acute illness are major associated factors, and quiet incapacity is easy to miss if teams only seek signatures.[4]
Near the end of life, a large proportion of older people who require treatment decisions lack capacity, which is why advance directives and appointed proxies matter for aligning care with prior wishes.[8]
Psychiatric populations also show substantial incapacity rates that vary by diagnosis and insight; depression alone does not equal incapacity but can impair appreciation and weighing when severe.[17][18]
Surrogates predict patient preferences imperfectly (about two-thirds accuracy in systematic review), and decision-making often burdens surrogates emotionally — support families as part of good care.[14][15]
Mechanisms — why capacity fails in later life
Attention, working memory, language, and executive function support understanding and reasoning. In dementia, progressive amnesia and executive failure erode understanding and weighing along a gradient; anosognosia selectively damages appreciation.[6][7]
Delirium produces fluctuating attentional failure — capacity can differ morning to evening. Late-life depression and hopelessness may collapse future-oriented weighing without abolishing factual teach-back.[18] Polypharmacy, infection, hypoxia, hyponatraemia, and pain create reversible incapacity windows that old-age psychiatrists must hunt for before declaring permanent incapacity.[4][5]
Clinical presentation — classic stems
Exam and ward stems cluster around: refuses hip fracture surgery or antibiotics; wants to leave hospital; refuses residential care; family demands full code against known values; contested enduring power of attorney; finances drained by a “helpful” relative; requests physician aid in dying or “just let me go”; quiet polite assent without understanding goals of care.[2][8]
Quiet incapacity (agreeable patient who cannot teach back) is as dangerous as loud refusal driven by delusion. Capable unwise refusal must be respected after full assessment and documentation.[2][5]
Differential and discriminators
Capable refusal
- Understands and appreciates
- Weighs options consistently
- May be unwise
- Respect and document
Incapacity
- Fails one or more abilities
- After adequate disclosure
- Supports tried
- Emergency / delay / surrogate
Not capacity problems
- Language or hearing barrier
- Coercion / undue influence
- Diagnosis or age alone
- Family disagreement
MHA vs guardianship
- MHA: psychiatric treatment + risk criteria
- Guardianship: substitute decisions
- Not interchangeable pathways
- Name local law in principle only
Capacity for treatment is not testamentary capacity, financial capacity, or forensic fitness to plead — map the correct legal test to the question asked.[20]
Bedside assessment
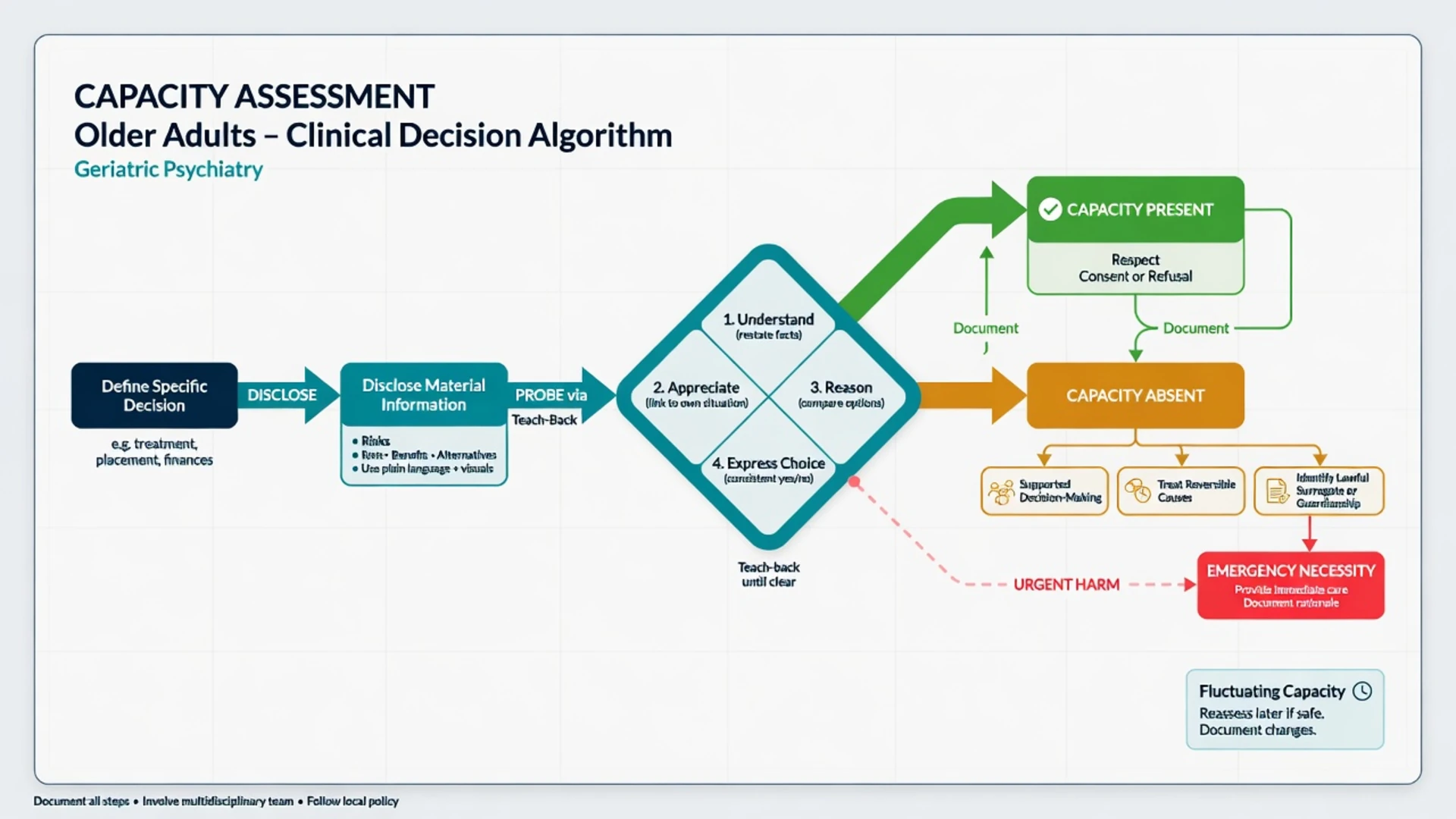
Practical sequence
- Name the decision precisely (e.g. “consent to above-knee amputation now,” not “capacity for medical care”).
- Disclose material information in accessible language; use teach-back.
- Probe each ability without leading only for agreement.
- Maximise capacity: hearing aids, glasses, interpreter, quieter room, family as support not substitute, reassess after treating delirium.
- Document: decision, information given, findings per ability, conclusion, supports, review timing.[2][3][5]
MacCAT-T operationalises the four abilities for research and teaching; clinical interview remains the gold standard for treatment decisions, and scores are not legal verdicts.[3][5] Cognitive screens (MoCA/MMSE) are adjuncts only — a “good” score does not prove capacity for a complex decision, and a low score does not prove incapacity for a simple one.[5][6]
Investigations
When incapacity is new or fluctuating, prioritise delirium work-up: infection, metabolic panel (including sodium, calcium, glucose), medication review (anticholinergics, opioids, benzodiazepines), oxygenation, and imaging when indicated by neurology or trauma. Neuropsychology helps for contested high-stakes decisions when time allows — not as a delay tactic when emergency treatment is required under necessity principles.[4][5]
Acute and emergency management
If incapacity is present and delay risks serious harm, provide emergency treatment under common-law necessity or statutory emergency provisions as applicable locally — document the risk, alternatives considered, and least restrictive option. Treat reversible causes immediately. Do not discharge an incapable patient into an unsafe destination.[2][5][16]
Mental Health Act pathways may authorise psychiatric treatment when statutory criteria are met; they are not automatic authority for all general medical interventions or residential placement. Using the wrong legal tool is a classic FRANZCP/MRCPsych trap.[17][20]
Definitive management — surrogates, guardianship, ACP
If capacity is present
Respect informed consent or refusal. Document risks, benefits, alternatives, and the person’s values. Offer ACP even when current decisions are clear.[2][9]
If capacity is absent
- Check for a valid advance directive and appointed healthcare attorney/proxy.
- Identify default surrogates under local hierarchy if no proxy (statutes vary widely).
- Escalate to guardianship / public guardian / tribunal when no lawful surrogate, conflict is irresolvable, or statutory thresholds for appointment are met.
- Apply substituted judgment when values are known; otherwise best interests with least restriction and consultation with relevant others.[8][14][16]
Do not invent section numbers, form codes, or “always next of kin” rules as universal law. DeMartino and colleagues illustrate how alternate decision-maker statutes differ even within one country — examiners reward principle-level answers with local humility.[16]
Advance care planning and directives
ACP should prepare patients and surrogates for future decisions, not merely tick living-will boxes.[9] In a national study of older decedents, advance directives were associated with care that matched preferences more often when end-of-life decisions arose in incapacity.[8] Encourage early ACP while residual capacity remains in progressive dementia.
End-of-life discussions associate with less aggressive near-death care and better caregiver bereavement outcomes in observational work; early integrated palliative care improves quality of life in advanced cancer trials — use these anchors when justifying timely goals-of-care conversations.[10][11]
Palliative psychiatric issues at end of life
Depression in terminal illness is under-recognised and treatable; distinguish from preparatory grief using persistent anhedonia, worthlessness, excessive guilt, and pervasive hopelessness rather than sadness alone.[12] Desire for hastened death associates strongly with depression and hopelessness in terminally ill cancer cohorts — treat depression, uncontrolled pain, and social isolation before concluding a purely values-based request.[12][13]
Delirium near death is common, impairs capacity, and is often multifactorial; non-pharmacological measures first; psychotropics only for severe distress with clear targets and review (dose and agent under local palliative protocols — cite clinical judgment and monitoring, avoid recipe-level invention).[5][12]
Requests for hastened death / PAD / VAD (where legal) require capacity assessment, exclusion of coercion, and screening for depression and anxiety; prevalence of psychiatric morbidity among requesters is not zero and assessment quality matters. Where PAD is illegal, the clinical task remains the same: relieve suffering, clarify values, treat reversible psychiatric drivers, and respect lawful refusal of life-prolonging treatment by a capacious person.[13][19]
Medications (exam-level principles only): for major depression in medically ill older adults, prefer agents with lower anticholinergic and fall risk when oral therapy is appropriate (e.g. sertraline or escitalopram oral at geriatric starting doses such as sertraline 25 mg orally daily, titrating cautiously with review of sodium, QTc risk factors, and interactions); psychostimulants are sometimes used short-term in palliative settings under specialist protocols — always document indication, dose, route, and monitoring, and do not use antidepressants as a delay tactic when emergency capacity issues require other pathways.[12]
Subtypes and high-yield scenarios
| Scenario | Capacity focus | Common pathway |
|---|---|---|
| Mild cognitive impairment | Often retains complex capacity | Support, early ACP |
| Moderate Alzheimer disease | Sliding-scale residual capacity | Decision-by-decision assessment |
| Severe dementia | Often lacks complex treatment capacity | Surrogate / guardianship |
| Hospital delirium | Fluctuating | Treat cause; reassess; delay non-urgent |
| Late-life depression with refusal | May impair weighing | Optimise mood treatment; reassess |
| Residential placement refusal | Residence decision distinct from medical | Local guardianship / aged-care law |
| Contested finances | Financial capacity separate | Administration / public trustee principles |
| Goals-of-care conflict | Values + capacity + directives | Ethics, lawful surrogate, palliative team |
Complications and pitfalls
- Status bias: “has dementia therefore no capacity.”
- Outcome bias: “refuses surgery therefore lacks capacity.”
- Skipping disclosure then diagnosing incapacity.
- Using family as automatic substitute without legal basis.
- Ignoring a valid advance directive or appointed proxy.
- Confusing MHA with medical best-interests authority.
- Missing treatable depression when the patient wants to die.
- Inventing statute section numbers under exam pressure.
- Failing to reassess fluctuating capacity.
Prognosis and disposition
Many incapacity states are temporary. Plan for recovery of capacity after delirium or acute medical treatment, and re-consent when possible. Document review intervals for borderline cases. Disposition must name whether care proceeds under emergency powers, delayed decision, lawful surrogate, formal guardianship process, or MHA pathway for psychiatric treatment.[2][4][16]
Support surrogates: a substantial minority experience lasting negative emotional effects from decision-making for others.[15]
Special populations
Indigenous and culturally diverse elders: use interpreters, allow culturally appropriate supporters, and avoid equating collective decision-making norms with incapacity — still protect the individual from coercion.[2]
Residential aged care: capacity for everyday choices often remains; chemical restraint for convenience is unethical and may be reportable under local frameworks (principles only).[6]
Severe mental illness at end of life: ensure equitable palliative access; capacity for medical decisions may be intact despite chronic psychosis — assess specifically.[17]
Ageing with intellectual disability: supported decision-making first; guardianship is last resort (see dedicated ID capacity topic for depth).[2][16]
Evidence and regional deltas
Landmark anchors: Appelbaum/Grisso abilities and 2007 clinical practice review; MacCAT-T; Sessums Rational Clinical Examination; Raymont medical inpatients; Kim/Karlawish dementia capacity literature; Silveira advance directives; Sudore/Fried ACP as preparation; Shalowitz and Wendler/Rid on surrogates; Wright and Temel on end-of-life communication and early palliative care; Block and Breitbart on depression and desire for death; Ganzini on mental health among PAD requesters; DeMartino on statutory heterogeneity.[1][2][5][8][11][16]
ANZ (FRANZCP primary): State/territory consent, guardianship, and enduring power schemes differ; Mental Health Acts differ. VAD/PAD laws exist in some jurisdictions with strict safeguards — state principles and local statute names you know, never invent sections for another state. RANZCP ethics and local health service ACP policies guide practice.[2][16]
UK/Ireland (MRCPsych): Mental Capacity Act principles (England and Wales) are often taught internationally as a scaffold (presumption, support, unwise decisions, best interests) but are not universal law. Scotland and Northern Ireland differ.[2][20]
USA (ABPN): State surrogate hierarchies and advance directive statutes vary widely; POLST/MOLST paradigms are state-dependent.[8][16]
India / MD-DNB: Mental Healthcare Act 2017 capacity and advance directive principles at high level; guardianship interfaces with other civil law — keep answers principle-based.[16][20]
Exam pearls
CAPACITY checklist
If you can only carry five anchors into the viva: Appelbaum four abilities; presumption and decision-specificity; Raymont/Silveira epidemiology of incapacity; surrogate accuracy limits plus ACP value; Block/Breitbart approach to depression and desire for death at end of life.[1][4][8][12][13]
References
- [1]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [2]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [3]Grisso T, Appelbaum PS, Hill-Fotouhi C The MacCAT-T: a clinical tool to assess patients' capacities to make treatment decisions Psychiatr Serv, 1997.PMID 9355168
- [4]Raymont V, Bingley W, Buchanan A, et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross-sectional study Lancet, 2004.PMID 15488217
- [5]Sessums LL, Zembrzuska H, Jackson JL Does this patient have medical decision-making capacity? JAMA, 2011.PMID 21791691
- [6]Kim SY, Karlawish JH, Caine ED Current state of research on decision-making competence of cognitively impaired elderly persons Am J Geriatr Psychiatry, 2002.PMID 11925276
- [7]Karlawish JH, Casarett DJ, James BD, et al. The ability of persons with Alzheimer disease (AD) to make a decision about taking an AD treatment Neurology, 2005.PMID 15883310
- [8]Silveira MJ, Kim SY, Langa KM Advance directives and outcomes of surrogate decision making before death N Engl J Med, 2010.PMID 20357283
- [9]Sudore RL, Fried TR Redefining the "planning" in advance care planning: preparing for end-of-life decision making Ann Intern Med, 2010.PMID 20713793
- [10]Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment JAMA, 2008.PMID 18840840
- [11]Temel JS, Greer JA, Muzikansky A, et al. Early palliative care for patients with metastatic non-small-cell lung cancer N Engl J Med, 2010.PMID 20818875
- [12]Block SD Assessing and managing depression in the terminally ill patient Ann Intern Med, 2000.PMID 10651602
- [13]Breitbart W, Rosenfeld B, Pessin H, et al. Depression, hopelessness, and desire for hastened death in terminally ill patients with cancer JAMA, 2000.PMID 11147988
- [14]Shalowitz DI, Garrett-Mayer E, Wendler D The accuracy of surrogate decision makers: a systematic review Arch Intern Med, 2006.PMID 16534034
- [15]Wendler D, Rid A Systematic review: the effect on surrogates of making treatment decisions for others Ann Intern Med, 2011.PMID 21357911
- [16]DeMartino ES, Dudzinski DM, Doyle CK, et al. Who decides when a patient can't? Statutes on alternate decision makers N Engl J Med, 2017.PMID 28402767
- [17]Okai D, Owen G, McGuire H, et al. Mental capacity in psychiatric patients: Systematic review Br J Psychiatry, 2007.PMID 17906238
- [18]Hindmarch T, Hotopf M, Owen GS Depression and decision-making capacity for treatment or research: a systematic review BMC Med Ethics, 2013.PMID 24330745
- [19]Ganzini L, Goy ER, Dobscha SK Prevalence of depression and anxiety in patients requesting physicians' aid in dying BMJ, 2008.PMID 18842645
- [20]Buchanan A Mental capacity, legal competence and consent to treatment J R Soc Med, 2004.PMID 15340019