Psych · old-age
Dementia with Lewy bodies and Parkinson disease dementia
Also known as DLB · Dementia with Lewy bodies · Parkinson disease dementia · PDD · Lewy body dementia · Lewy body disease · Cortical Lewy body disease
Exam-exhaustive fellowship reference on dementia with Lewy bodies (DLB) and Parkinson disease dementia (PDD) — McKeith 2017 core features and biomarkers; 1-year rule; RBD; neuroleptic sensitivity; cholinesterase inhibitors; avoidance of high-potency D2 blockade; DaT SPECT; RANZCP/NICE/APA-aligned management. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Why this topic matters in exams
Examiners use DLB/PDD to test whether you can: apply McKeith core features and the 1-year rule; recognise RBD as prodromal and supportive; refuse high-potency neuroleptics; start and monitor a cholinesterase inhibitor with a real dose; and sequence psychosis management without iatrogenic catastrophe.[1][4][15][16]
Definition and classification
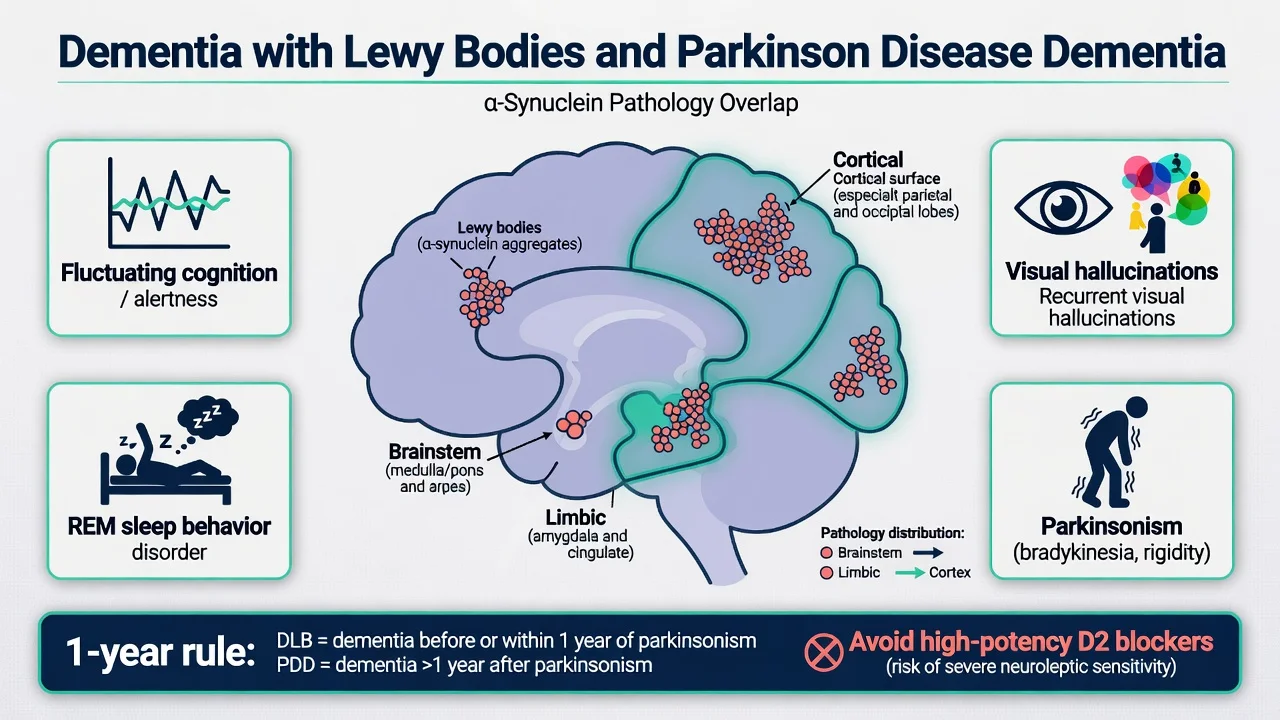
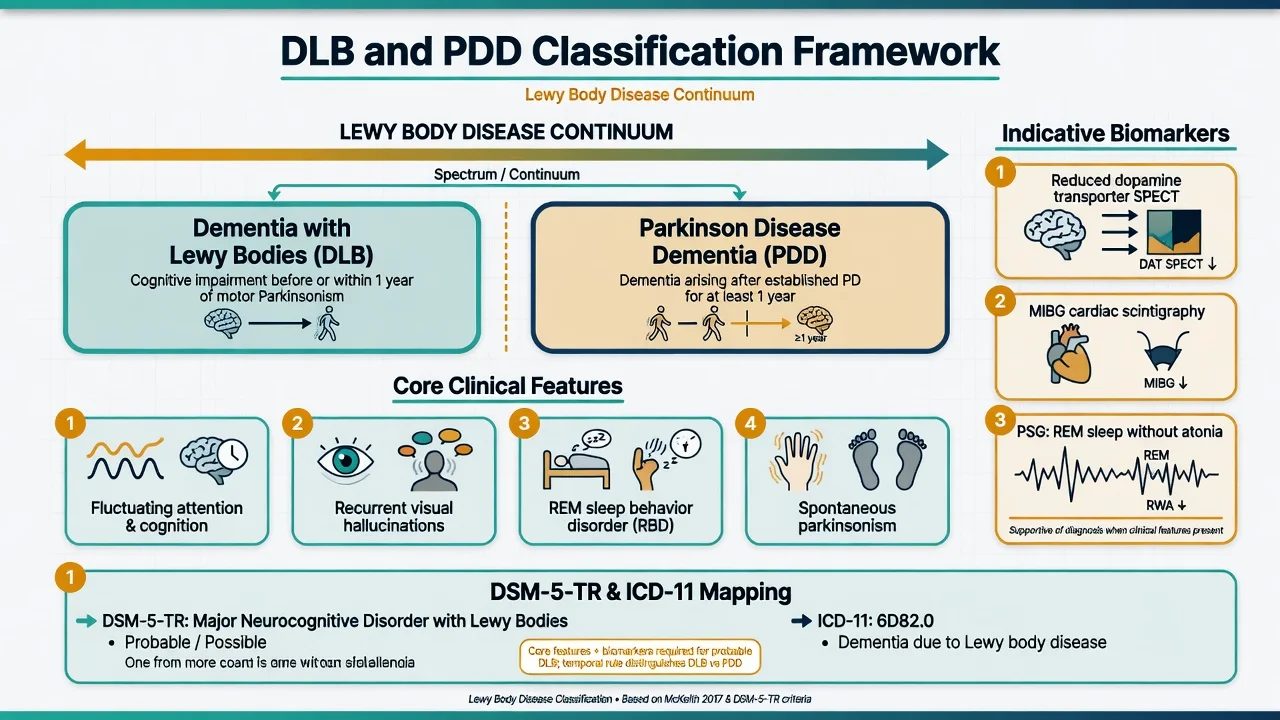
Dementia with Lewy bodies (DLB). Progressive dementia with characteristic clinical and biomarker features defined by the DLB Consortium fourth consensus report (McKeith 2017).[1] Dementia is essential: progressive cognitive decline of sufficient magnitude to interfere with normal social or occupational function, often with early attention, executive, and visuospatial deficits rather than pure amnestic Alzheimer patterning.[1][11]
Core clinical features (McKeith 2017):
- Fluctuating cognition with pronounced variations in attention and alertness
- Recurrent well-formed visual hallucinations
- REM sleep behaviour disorder (RBD), which may precede dementia by years
- One or more spontaneous cardinal features of parkinsonism (bradykinesia, rest tremor, or rigidity)
Probable vs possible DLB (operational teaching). Probable DLB: dementia plus two or more core clinical features, or one core feature plus one or more indicative biomarkers. Possible DLB: one core feature alone, or one or more indicative biomarkers without core features.[1] Supportive clinical features (e.g. severe neuroleptic sensitivity, falls, syncope, severe autonomic dysfunction, hypersomnia, hyposmia, systematised delusions, apathy/anxiety/depression) support the diagnosis but do not alone establish probable DLB.[1]
Indicative biomarkers (McKeith 2017): reduced dopamine transporter uptake in basal ganglia on SPECT/PET (e.g. 123I-FP-CIT); abnormal 123I-MIBG myocardial scintigraphy; polysomnographic confirmation of REM sleep without atonia.[1][10]
Parkinson disease dementia (PDD). Dementia arising in the context of established Parkinson disease, using MDS Task Force clinical diagnostic criteria (Emre 2007): PD diagnosis first; dementia by history/examination/cognitive testing with impairment in more than one cognitive domain and functional impact, not solely attributable to motor or autonomic disability.[3]
The 1-year rule (exam critical). If dementia begins before or within 1 year of parkinsonism, diagnose DLB. If dementia begins after Parkinson disease has been established for at least 1 year, diagnose PDD.[1][2][3] Pathologically both are Lewy body diseases; the rule is clinicopathologic convenience, not a claim of two unrelated diseases.[1][16]
DSM-5-TR / ICD-11. Map to major neurocognitive disorder with Lewy bodies (DSM-5-TR) or dementia due to Lewy body disease / Parkinson disease (ICD-11) as appropriate; still reason using McKeith/Emre clinical criteria in viva.[1][3]
Epidemiology and risk
DLB is among the most common neurodegenerative dementias after Alzheimer-type disease in older adults and is under-recognised in routine practice.[1][16] In Parkinson disease, cumulative dementia risk is high over long-term follow-up; Aarsland and colleagues documented substantial dementia prevalence in an 8-year prospective PD cohort, establishing PDD as an expected late complication rather than a rarity.[12]
Associations examiners expect: older age; male predominance in many DLB series; idiopathic RBD as a strong synucleinopathy risk marker; visual hallucinations and fluctuating cognition as clinical red flags; autonomic dysfunction and falls; frequent co-pathology with Alzheimer-type changes.[1][16] Outcomes include high rates of institutionalisation, carer burden, falls-related injury, and excess mortality relative to age-matched controls.[16]
Pathophysiology (exam-level)
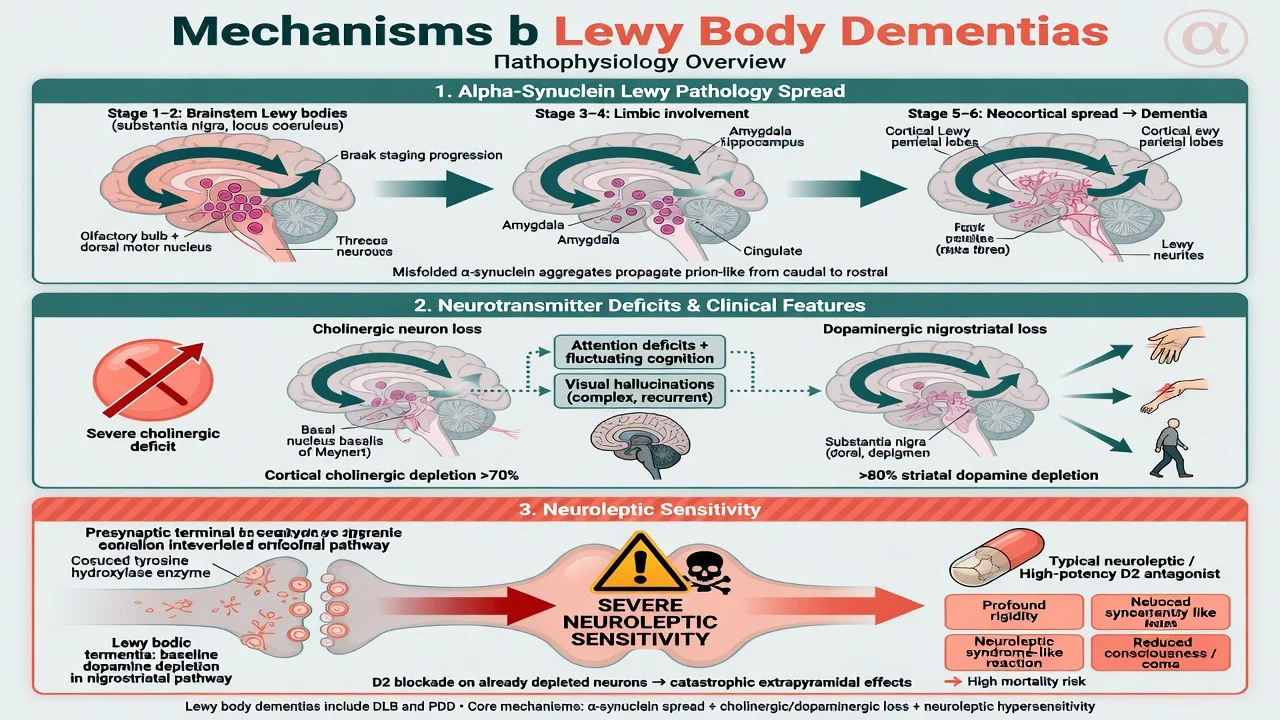
Lewy body dementias are alpha-synucleinopathies. Lewy bodies and Lewy neurites involve brainstem, limbic, and neocortical regions with variable Braak-type staging; Alzheimer co-pathology is common and modifies phenotype.[1][16]
Neurochemistry viva points:
- Marked cortical cholinergic deficit (often more severe than typical AD teaching comparisons) links to attentional failure, visual hallucinations, and responsiveness to cholinesterase inhibitors.[6][7][15]
- Nigrostriatal dopaminergic loss drives spontaneous parkinsonism and reduced dopamine transporter signal on SPECT.[10]
- Neuroleptic sensitivity reflects catastrophic extrapyramidal and autonomic responses when residual dopaminergic tone is blocked — historically documented as severe and sometimes fatal after conventional neuroleptics in Lewy body dementia.[4][5]
RBD reflects brainstem synucleinopathy (sublaterodorsal tegmental region teaching) and may appear years before cognitive or motor disease.[1]
Clinical presentation and MSE
Fluctuation. Pronounced day-to-day or hour-to-hour changes in attention and alertness — from relatively lucid conversation to staring, somnolence, or disorganised speech — quantified in research with attention tasks and described by informants as "good days and bad days".[1][11]
Visual hallucinations. Recurrent, well-formed, often people or animals; insight may wax and wane; may be less distressing early than in primary psychosis, but still drive risk and carer distress.[1]
RBD. Dream enactment: punching, kicking, shouting, falling from bed; bed-partner injury is a classic history pearl; may precede dementia by years.[1]
Spontaneous parkinsonism. Bradykinesia, rigidity, and/or rest tremor not solely drug-induced; often axial and gait features with falls risk.[1]
Cognitive profile. Attention, executive function, and visuospatial construction often hit earlier and harder than free recall alone — contrast with typical amnestic-predominant AD at the bedside.[1][11]
PDD phenotype. Same cognitive and neuropsychiatric territory on a long-standing PD motor background, often after years of motor disease and dopaminergic therapy.[3][12]
MSE language (example). Alertness fluctuates during interview; orientation incomplete; attention impaired on serial tasks; describes seeing children in the room at night; no formal thought disorder; mood euthymic or anxious; insight partial; mild bilateral rigidity and reduced arm swing; orthostatic BP drop noted.[1][11]
Differential diagnosis (discriminators)
| Competing diagnosis | Fast discriminators |
|---|---|
| Alzheimer disease | Early progressive amnesia; VH and RBD less early; less spontaneous parkinsonism early |
| Delirium | Hours–days, clear medical driver; can coexist with DLB and amplify fluctuation |
| Vascular cognitive impairment | Stepwise course, focal signs, strategic infarcts/white-matter burden on imaging |
| Late-onset primary psychosis | Lack of RBD, fluctuation pattern, parkinsonism, and cognitive trajectory of LB disease |
| Charles Bonnet | Isolated visual phenomena with ocular disease, relatively preserved cognition/insight |
| Drug-induced parkinsonism / anticholinergic delirium | Temporal link to dopamine blockers or anticholinergics |
| PSP / MSA / CBD | Distinct motor, eye-movement, autonomic, or cortical sensory signatures |
ClinicalPearl: First late-life visual hallucinations with fluctuation and dream enactment is DLB until proven otherwise — not "late schizophrenia" by default.[1]
Assessment
History structure. Onset and sequence of cognitive vs motor symptoms (apply 1-year rule); detailed hallucination phenomenology; sleep/dream enactment (ask bed partner); falls, syncope, constipation, urinary symptoms, orthostatic dizziness; medication list (antipsychotics, anticholinergics, dopaminergic agents, opioids, benzos); driving, finances, fire/kitchen risk; carer burden and safeguarding.[1][16]
Examination. Cognitive testing with attention and visuospatial emphasis (MoCA often more sensitive than MMSE alone for non-amnestic profiles); full neurological exam for parkinsonism; orthostatic vital signs; swallow/aspiration risk as indicated.[1][11]
Scales (what they measure). MoCA — global screen; NPI — neuropsychiatric symptom domains; UPDRS motor items for parkinsonism severity in shared care with neurology. Scales support, not replace, consensus diagnosis.[1]
Risk and capacity. Falls, wandering, RBD injury, self-neglect, financial exploitation, medication non-adherence; assess decision-making capacity for treatment, residence, and finances with least-restrictive legal frameworks (jurisdiction-specific).[16][18]
Investigations
Standard dementia work-up. FBC, U&E, LFT, glucose, calcium, TSH, B12 (± folate), medication review; ECG before cholinesterase inhibitors or any antipsychotic; structural MRI preferred over CT when feasible (relative medial temporal preservation may favour DLB vs AD but is not pathognomonic).[1][18]
Indicative biomarkers when available and diagnostic uncertainty remains:
- 123I-FP-CIT (DaT) SPECT — reduced striatal uptake supports DLB vs non-DLB dementia with high sensitivity/specificity in multicentre study settings.[10]
- MIBG myocardial scintigraphy and PSG for REM without atonia where accessible.[1]
Do not delay supportive clinical diagnosis and ChEI trial solely because biomarker access is limited in ANZ public settings — clinical McKeith criteria remain primary.[1][16]
Acute / emergency management
- Safety of patient and others; exclude delirium, pain, constipation, infection, metabolic upset.
- De-escalate environment; avoid restraint where possible.
- Do not give high-potency typical antipsychotics for agitation in suspected DLB/PDD.[4][5]
- If life-threatening behavioural emergency after non-drug measures: seek senior old-age psychiatry/neurology input; any antipsychotic is a last resort with continuous monitoring for rigidity, consciousness, and autonomic change; prefer pathways that avoid high D2 affinity agents.[15][16]
- Suspected neuroleptic malignant syndrome-like reaction: stop agent, medical resuscitation pathway.
Definitive management
Non-pharmacological (always first and continuous)
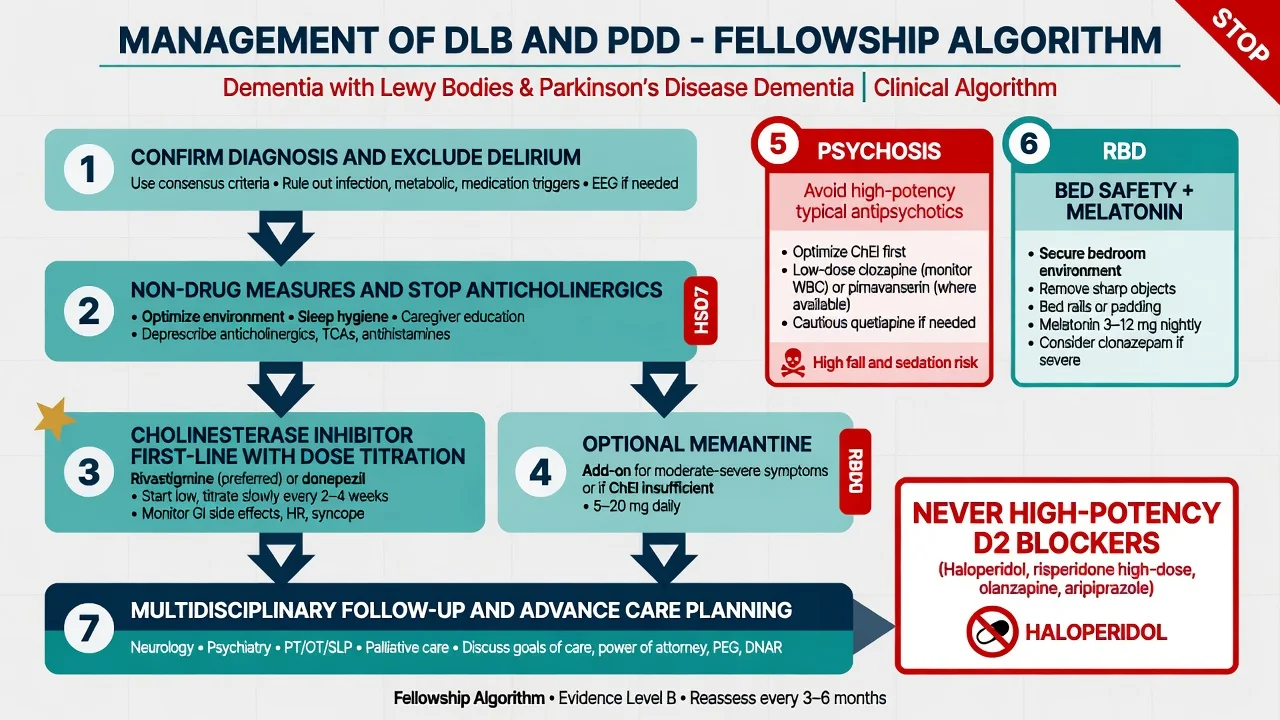
Person-centred care; optimise lighting and visual environment; reorientation without confrontation about hallucinations when insight is poor; structured routine; carer education that hallucinations are disease-related; falls prevention; RBD bedroom safety (pad corners, lower mattress, separate beds if partner injury risk); review sensory impairment.[16][18]
Deprescribe offending agents
Stop or minimise anticholinergics, sedating antihistamines, tricyclics with high anticholinergic load, and unnecessary benzodiazepines. In PDD/PD psychosis, carefully review dopaminergic load with neurology — reduce dopamine agonists and anticholinergics before escalating antipsychotics when motor status allows.[15][16]
Cholinesterase inhibitors (first-line pharmacotherapy)
ChEIs are the evidence anchor for cognitive and some neuropsychiatric symptoms in DLB and PDD.[6][7][8][15]
| Agent | Example start / titration (adult) | Key monitoring |
|---|---|---|
| Rivastigmine (oral) | Start 1.5 mg orally twice daily with food; increase by 1.5 mg twice daily every ≥2 weeks as tolerated toward 3–6 mg twice daily (total 6–12 mg/day) as used in PDD/DLB trials | Nausea, vomiting, anorexia, weight, diarrhoea, bradycardia/syncope, falls, vivid dreams, worsening tremor |
| Rivastigmine (patch) | Regional product info: often 4.6 mg/24 h then up-titrate to 9.5 mg/24 h (and higher strengths if licensed) | Skin reaction plus systemic ChEI effects |
| Donepezil | Start 3–5 mg orally once daily; increase to 10 mg daily after 4–6 weeks if tolerated (Mori DLB programme used 3, 5, and 10 mg arms) | GI effects, bradycardia, insomnia/nightmares, falls |
Landmark signals: rivastigmine improved cognition and neuropsychiatric outcomes vs placebo in DLB (McKeith 2000) and in PDD (Emre 2004 EXPRESS trial); donepezil improved cognitive outcomes in randomised DLB trials (Mori 2012).[6][7][8] Stinton systematic review/meta-analysis supports ChEIs as the best-evidenced class for Lewy body dementia symptoms overall.[15]
Memantine. May provide modest global benefit as adjunct or alternative when ChEI not tolerated; Emre 2010 RCT in PDD/DLB showed improvement on global impression measures with mixed domain effects — individualise, typical titration 5 mg orally daily toward 10 mg twice daily (20 mg/day) as tolerated with renal adjustment.[9][15]
Psychosis and agitation
Order of operations for fellowship answers: exclude delirium and pain; non-drug measures and environment; optimise or start cholinesterase inhibitor; review PD medications with neurology if PDD; only then consider specialist antipsychotic strategies.[8][15][16]
Avoid high-potency D2 antagonists (haloperidol and other high-affinity D2 blockers) as first-line treatment of psychosis in DLB/PDD.[4][15][16] General dementia antipsychotic mortality and stroke risk still applies when any antipsychotic is used.[17]
When an antipsychotic is unavoidable:
- Clozapine (lowest effective dose, often starting around 6.25–12.5 mg orally at night, titrated carefully — many PD psychosis responders remain well below schizophrenia doses) has RCT support in PD drug-induced psychosis with mandatory haematological monitoring and specialist oversight.[14][15]
- Pimavanserin (selective 5-HT2A inverse agonist) reduced PD psychosis without worsening motor function in a phase 3 RCT (Cummings 2014); access and licensing vary by region (limited/not standard in many ANZ pathways at time of writing).[13][16]
- Quetiapine is widely used at low dose in practice for PD/DLB psychosis because of lower D2 affinity, but high-quality efficacy evidence is weaker than for clozapine — document uncertainty and review early.[15][16]
RBD
Prioritise environmental safety. Pharmacologically, melatonin is often preferred first in frail older adults when a drug is needed; low-dose clonazepam is classic but increases falls, sedation, and confusion risk — use sparingly with explicit risk discussion.[1][16]
Regional notes
NICE dementia guidance emphasises accurate subtype diagnosis, non-drug care, and cautious psychotropic use; offer ChEI for DLB (and PD dementia pathways align with rivastigmine evidence).[18] APA Alzheimer/other dementias principles and Lewy-body-specific reviews (Taylor 2020; Stinton 2015) converge on ChEI-first and antipsychotic restraint.[15][16] In Australia/New Zealand, confirm local PBS/Pharmac listings, DaTSCAN availability, clozapine monitoring logistics, and whether pimavanserin is accessible before viva promises.
Subtypes and scenarios
- De novo probable DLB cognitive presentation with VH and fluctuation
- PDD after long motor PD, often with dopaminergic polypharmacy
- Prodromal isolated RBD with emerging cognitive/autonomic soft signs
- Mislabelled late-onset psychosis actually prodromal DLB
- Nursing home BPSD with unrecognised DLB and prior typical antipsychotic exposure
- Mixed AD–LB pathology with blended amnestic and attentional features
Complications and pitfalls
Missing RBD history; treating VH as primary schizophrenia with high-dose risperidone/haloperidol; ignoring orthostatic hypotension and falls; adding anticholinergics for bladder or extrapyramidal symptoms; failing to coordinate with neurology on dopaminergic titration; continuing antipsychotics indefinitely without target review (general dementia mortality signal).[4][15][17]
Prognosis and disposition
Progressive neurodegenerative course with substantial morbidity; survival and institutionalisation risk are generally worse than uncomplicated late-onset AD teaching comparisons, but individual trajectories vary with co-pathology and complications.[16] Disposition spans home with packages of care, residential aged care, and hospital liaison. Plan advance care directives, driving assessment, financial enduring powers, and carer support early.[18]
Special populations
Residential aged care chemical-restraint risk is high — document non-drug trials and avoid "PRN haloperidol" culture.[17] Cultural formulation of visual experiences matters; use interpreters and family structure without dismissing core LB features as "culturally normal". Younger-onset and GBA-associated synucleinopathy awareness for selected cases, without over-testing every patient.[16]
Evidence and guidelines (named)
- McKeith 2017 fourth consensus diagnosis/management; McKeith 2005 third report historical scaffolding of 1-year rule teaching.[1][2]
- Emre 2007 PDD criteria; Aarsland 2003 PDD prevalence trajectory.[3][12]
- Trials: McKeith 2000 rivastigmine DLB; Emre 2004 rivastigmine PDD; Mori 2012 donepezil DLB; Emre 2010 memantine; Cummings 2014 pimavanserin; Pollak 2004 clozapine PD psychosis; McKeith 2007 DaT SPECT accuracy.[6][7][8][9][10][13][14]
- Syntheses: Stinton 2015; Taylor 2020; Schneider 2005 antipsychotic mortality in dementia; NICE dementia summary 2018.[15][16][17][18]
Exam pearls
- ChEI before antipsychotic for many LB neuropsychiatric symptoms.[6][7][15]
- Never high-potency D2 first-line — classic fail.[4]
- Name a dose: rivastigmine 1.5 mg twice daily starting, or donepezil 5 mg daily, with cardiac/GI monitoring.[7][8]
- Ask every older adult with new psychosis or dementia about dream enactment.[1]
- DaT SPECT supports, does not replace, clinical diagnosis.[10]
Self-check
Self-test against McKeith core features, the 1-year rule, cholinesterase inhibitor start doses with monitoring, neuroleptic sensitivity (why high-dose high-potency D2 blockade is first-line contraindicated), and the non-drug → ChEI → specialist psychosis sequence including clozapine haematological monitoring.[1][3][4][7][14]
References
- [1]McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium Neurology, 2017.PMID 28592453
- [2]McKeith IG, Dickson DW, Lowe J, et al. Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium Neurology, 2005.PMID 16237129
- [3]Emre M, Aarsland D, Brown R, et al. Clinical diagnostic criteria for dementia associated with Parkinson's disease Mov Disord, 2007.PMID 17542011
- [4]McKeith I, Fairbairn A, Perry R, Thompson P, Perry E Neuroleptic sensitivity in patients with senile dementia of Lewy body type BMJ, 1992.PMID 1356550
- [5]McKeith IG, Ballard CG, Harrison RW Neuroleptic sensitivity to risperidone in Lewy body dementia Lancet, 1995.PMID 7544860
- [6]McKeith I, Del Ser T, Spano P, et al. Efficacy of rivastigmine in dementia with Lewy bodies: a randomised, double-blind, placebo-controlled international study Lancet, 2000.PMID 11145488
- [7]Emre M, Aarsland D, Albanese A, et al. Rivastigmine for dementia associated with Parkinson's disease N Engl J Med, 2004.PMID 15590953
- [8]Mori E, Ikeda M, Kosaka K; Donepezil-DLB Study Investigators Donepezil for dementia with Lewy bodies: a randomized, placebo-controlled trial Ann Neurol, 2012.PMID 22829268
- [9]Emre M, Tsolaki M, Bonuccelli U, et al. Memantine for patients with Parkinson's disease dementia or dementia with Lewy bodies: a randomised, double-blind, placebo-controlled trial Lancet Neurol, 2010.PMID 20729148
- [10]McKeith I, O'Brien J, Walker Z, et al. Sensitivity and specificity of dopamine transporter imaging with 123I-FP-CIT SPECT in dementia with Lewy bodies: a phase III, multicentre study Lancet Neurol, 2007.PMID 17362834
- [11]Walker MP, Ayre GA, Cummings JL, et al. Attention and fluctuating attention in patients with dementia with Lewy bodies and Alzheimer disease Arch Neurol, 2001.PMID 11405813
- [12]Aarsland D, Andersen K, Larsen JP, Lolk A, Kragh-Sørensen P Prevalence and characteristics of dementia in Parkinson disease: an 8-year prospective study Arch Neurol, 2003.PMID 12633150
- [13]Cummings J, Isaacson S, Mills R, et al. Pimavanserin for patients with Parkinson's disease psychosis: a randomised, placebo-controlled phase 3 trial Lancet, 2014.PMID 24183563
- [14]Pollak P, Tison F, Rascol O, et al. Clozapine in drug induced psychosis in Parkinson's disease: a randomised, placebo controlled study with open follow up J Neurol Neurosurg Psychiatry, 2004.PMID 15090561
- [15]Stinton C, McKeith I, Taylor JP, et al. Pharmacological Management of Lewy Body Dementia: A Systematic Review and Meta-Analysis Am J Psychiatry, 2015.PMID 26085043
- [16]Taylor JP, McKeith IG, Burn DJ, et al. New evidence on the management of Lewy body dementia Lancet Neurol, 2020.PMID 31519472
- [17]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [18]Pink J, O'Brien J, Robinson L, Longson D; Guideline Committee Dementia: assessment, management and support: summary of updated NICE guidance BMJ, 2018.PMID 29925626