Psych · Old age psychiatry — risk and safeguarding
Elder abuse and vulnerability
Also known as Elder mistreatment · Elder neglect · Abuse of older people · Financial exploitation of older adults · Self-neglect in older adults · Adult safeguarding older people
Exam-exhaustive fellowship reference on elder abuse and vulnerability — subtypes (physical, sexual, psychological, financial, neglect, self-neglect), epidemiology and mortality, risk ecology, assessment including private interview and capacity, multi-agency safeguarding and jurisdiction-aware reporting principles without invented statutes, psychiatry interface with dementia and late-life mental illness. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Elder abuse (elder mistreatment) is a high-yield old-age psychiatry and CASC topic because it sits at the intersection of risk, capacity, dementia care, carer stress, and adult safeguarding. Examiners test whether you can see the patient alone, name subtypes, formulate vulnerability, assess capacity without equating dementia with global incapacity, and escalate safely without fabricating legal sections.[1][6]
Overview and definition
Major clinical reviews frame elder abuse as a single or repeated act — or failure to act — occurring within a relationship where there is an expectation of trust, causing harm or distress to an older person.[1][2][16]
Vulnerability is not age alone. It is increased susceptibility to harm from cognitive impairment, functional dependency, multimorbidity, social isolation, sensory impairment, financial dependence of others on the older person, and power imbalance (including longstanding intimate partner violence grown old).[2][4]
DSM-5-TR and ICD-11 do not replace clinical recognition with a single "elder abuse disorder" diagnosis. The exam task is recognition, risk formulation, capacity analysis, and multi-agency response — while treating associated depression, trauma symptoms, substance use, and dementia-related needs.[1]
Classification — subtypes
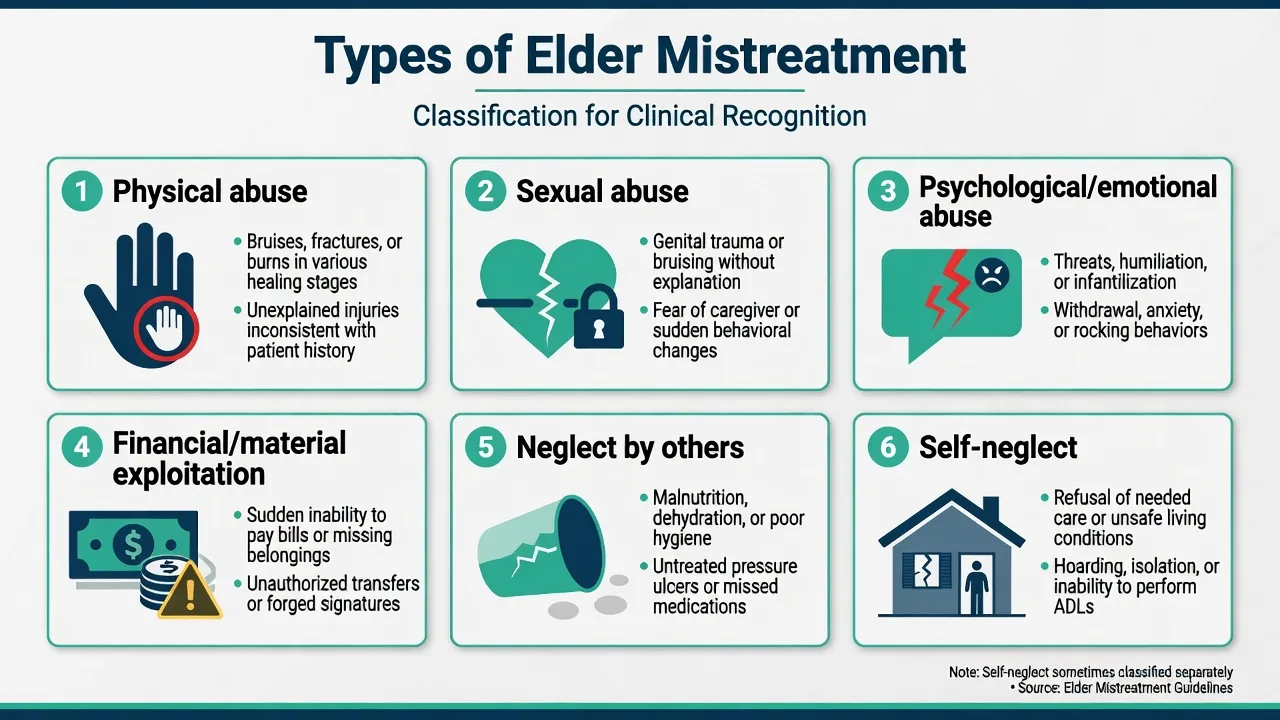
Physical
- Hitting, restraining, over-medication as control
- Patterned injuries; history inconsistent with findings
- Delayed presentation; multiple healing stages
Sexual
- Any non-consensual sexual contact
- May present as fear of care, genital injury, STI
- Forensic pathway when indicated
Psychological
- Threats, humiliation, isolation, intimidation
- Threats of nursing-home placement as control
- Often co-occurs with other subtypes
Financial
- Theft, coercion over wills/POA, misuse of cards
- Sudden account changes; unpaid bills despite assets
- High yield with cognitive impairment
Neglect (by others)
- Failure to provide necessary care, food, meds, safety
- Pressure injuries, dehydration, missed appointments
- Active or passive omission
Self-neglect
- Often excluded from abuse-by-others definitions
- Squalor, refusal of services, hazardous living
- Capacity assessment is central
Institutional abuse includes facility-level neglect, staff-perpetrated abuse, and abusive practices such as unlawful restraint or chemical restraint used for convenience rather than assessed clinical need. Intimate partner violence (IPV) in later life may be continuous coercive control rather than a new late-onset phenomenon.[1][2]
Epidemiology and risk
A global systematic review and meta-analysis of community studies found that elder abuse is common, with substantial heterogeneity by region and method — the clinical takeaway is high prevalence plus under-detection, not a single universal percentage to memorise as dogma.[5]
The US National Elder Mistreatment Study mapped correlates of emotional, physical, sexual, and financial abuse and potential neglect in a large population sample.[4] Community population work further characterises prevalence and risk patterning.[14]
Outcome associations examiners expect: elder mistreatment has been associated with increased mortality in classic cohort work and with higher hospitalisation risk in later analyses.[3][11]
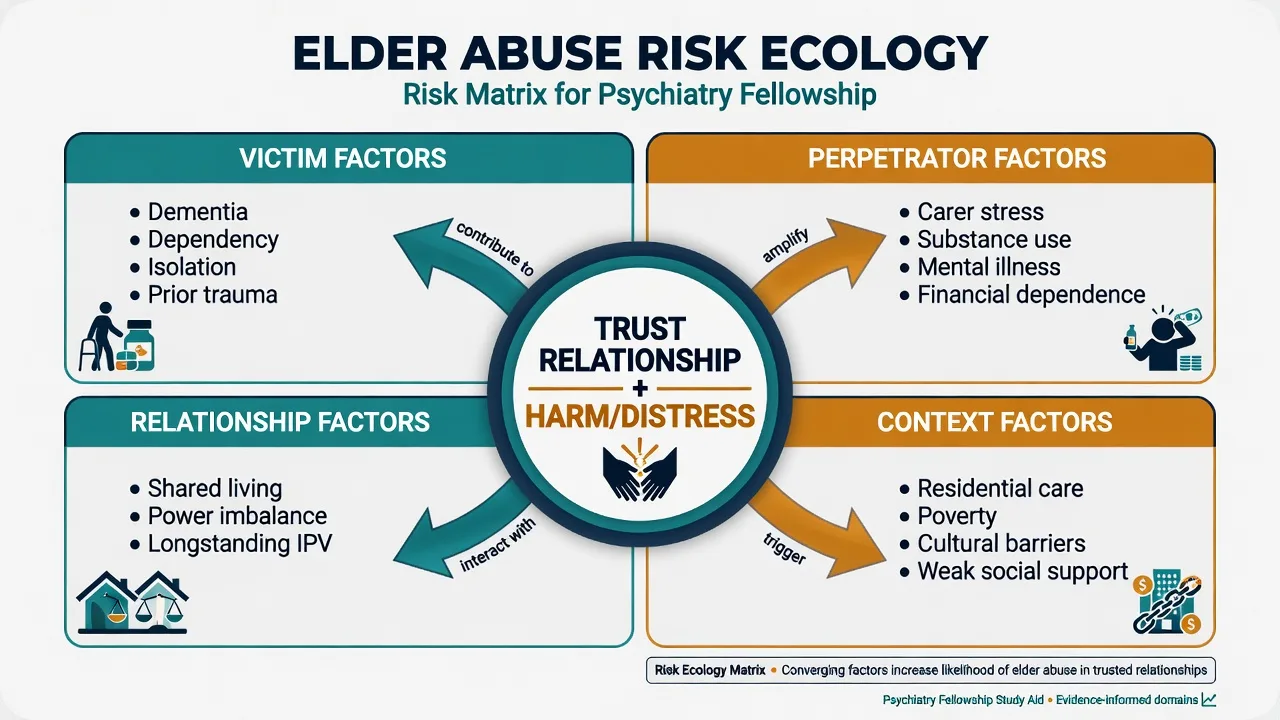
Victim-side risk: dementia and cognitive impairment, ADL/IADL dependency, isolation, prior trauma or IPV, mental illness, substance use, shared living with the abuser, and minority or migrant status when access to help is constrained.[2][4][14]
Perpetrator-side risk: carer burden and stress (especially with dementia), mental illness, alcohol/other substance use, financial dependence on the older person, and prior violence.[2][7]
The CARD study is high-yield for dementia carer contexts: family carers' abusive behaviour toward people with dementia relates to carer factors and the care situation — supporting prevention via carer support without excusing harm or replacing safeguarding when risk is present.[7]
Mechanisms and psychiatric interface
There is no single neurotransmitter model. Useful frameworks are ecological and interpersonal: dependency–stress, power and control, intergenerational transmission of violence, and institutional cultures that normalise poor care.[2]
Dementia interface. Cognitive impairment increases vulnerability (impaired reporting, financial naivety, dependency). BPSD can increase carer strain. Conversely, fear, bruises, or withdrawal may be mislabelled as "just dementia" or "just depression" — diagnostic overshadowing is a classic pitfall.[7][12]
Mental health sequelae. Depression, anxiety, PTSD-like symptoms, substance use, sleep disruption, worsening cognition under chronic stress, healthcare avoidance, and suicidal ideation. Treat these as real clinical problems, not expected "reactions" that justify inaction.[1][3]
Clinical presentation
Presentations span ED, primary care, old-age psychiatry clinics, residential aged care, and C-L wards.[13]
Interview red flags: alleged abuser insists on remaining present; patient looks to companion before answering; histories change; injuries explained as "she falls a lot" without matching pattern; patient minimises then discloses when alone; sudden transfer of assets to one relative; missed medications and weight loss despite "full-time care."[1][13]
MSE and risk. Note affect (fear, flatness, tearfulness), thought content (hopelessness, shame, threat beliefs that may be reality-based), cognition, insight into risk, and suicidality. Reality-based fear of a carer is not a delusion — do not antipsychotic-ise disclosure.[1]
Differential diagnosis
Accident / medical
- Falls, anticoagulants, senile purpura
- Still document and reassess if pattern evolves
- Inconsistency of history remains key
Self-neglect ± capacity
- May look like neglect by others
- Map who is responsible for care
- Capacity is decision-specific
Primary psychiatric
- Depression, psychosis, substance use
- Can coexist with true abuse
- Avoid overshadowing either way
Carer stress without abuse
- Exhaustion and poor skills
- Offer support early
- Escalate if acts/omissions cause harm
Assessment
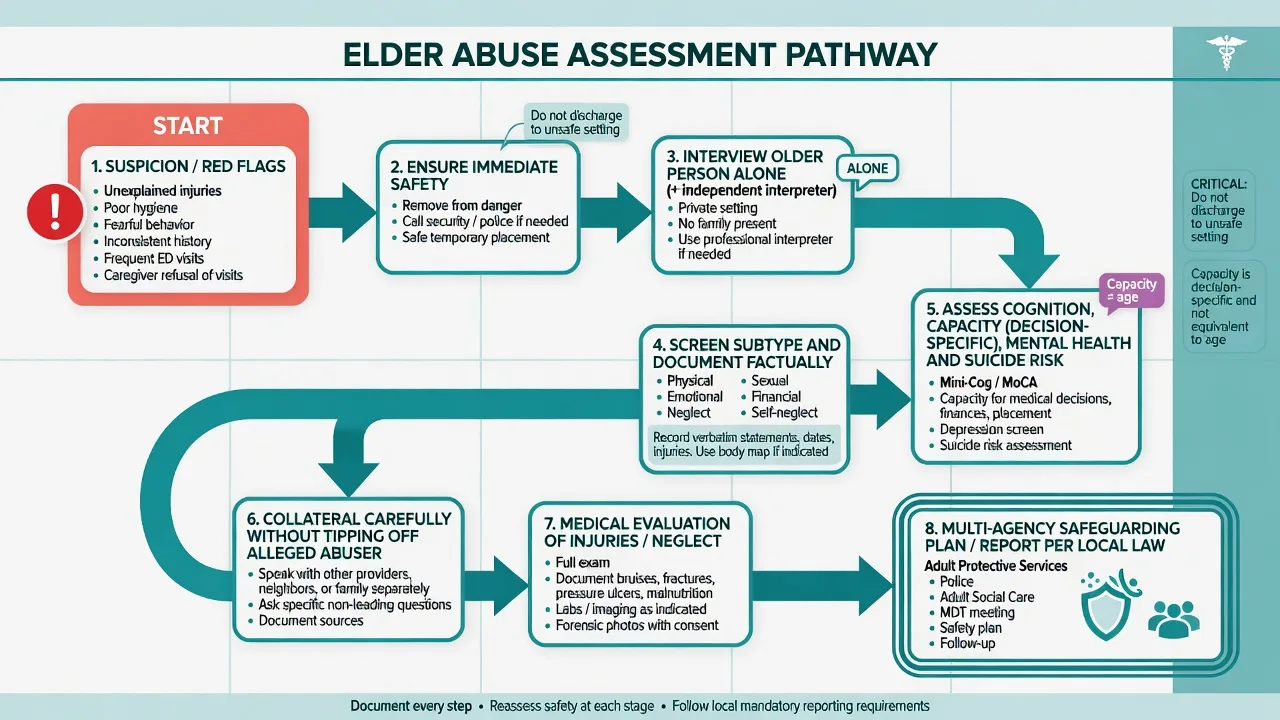
Core rules for bedside assessment when elder abuse is suspected.[1][13]
- Immediate safety — if danger is ongoing, separate, admit, or shelter before perfect paperwork.[1][13]
- Interview the older person alone (independent interpreter if needed — not a family member).[1][6]
- Ask directly but non-judgementally about hitting, shouting, control of money, being left without food/meds, forced sexual contact, and fear of someone at home.[1]
- Screening tools (EASI-style questions, H-S/EAST concepts, dementia-specific approaches) can structure enquiry; a systematic review shows multiple tools exist, but none replaces clinical judgement and a private conversation.[12][15]
- Document objectively: quotes, injury description, who was present, what was offered, what was refused, and the safety plan.[1][13]
- Capacity for relevant decisions using a functional, decision-specific approach (see next section).[8][10]
- Suicide and violence risk assessment as for any high-stress presentation.[1]
- Collateral carefully — do not tip off a suspected abuser in ways that increase retaliation risk before protections are in place.[6][13]
Professionals under-detect and under-report; knowledge gaps and uncertainty about process are recurrent themes in detection literature — have a local pathway memorised in principle form.[6]
Capacity and vulnerability decisions
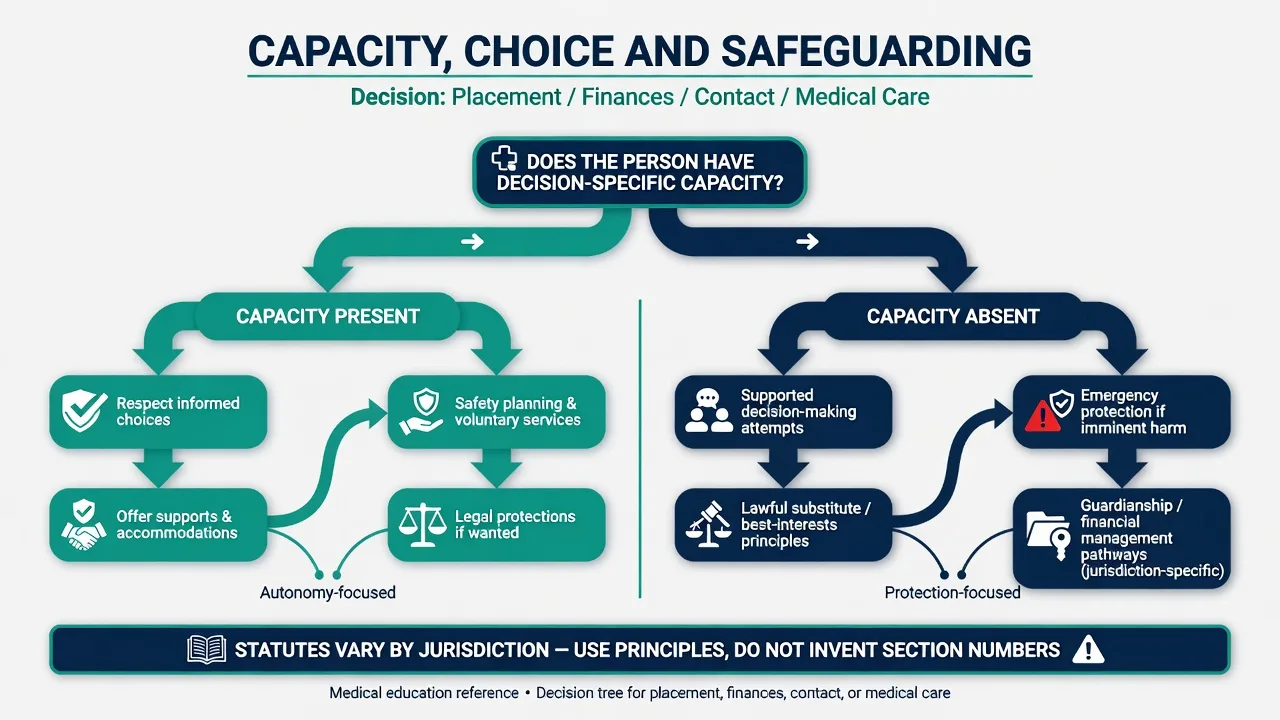
Capacity is decision- and time-specific, not a global label derived from age or dementia diagnosis. After disclosing material information, assess the abilities to understand, appreciate, reason/weigh, and communicate a choice (Appelbaum/Grisso framework; parallel language appears in many statutes).[8][9][10]
Exam-critical divergences: a person may retain capacity to decide who visits while lacking capacity for complex financial management; or retain capacity to refuse a particular service while needing protection from an imminent physical threat under emergency principles. Reassess when delirium, intoxication, fear, or untreated depression is optimised.[8][10]
Undue influence and coercion can undermine voluntary decision-making even when cognitive testing looks "not that bad." Document the process, free from pressure, and any controlling presence.[8][10]
Acute management and reporting principles
Medical priorities: treat injuries, dehydration, infection, pain, pressure injuries; consider forensic photography protocols with consent/capacity frameworks when relevant.[13]
Reporting and multi-agency response — jurisdiction-aware principles (no invented sections): detection literature shows professionals often under-report; duties and pathways are local, so state principles rather than fabricated statutes.[1][6]
- Adult safeguarding / adult protective services / aged-care quality pathways exist in different forms across ANZ, UK, US, and other systems. Know your local escalation route as a clinician.[1][6]
- Mandatory reporting rules differ: some jurisdictions mandate reporting of certain residential aged care assaults or of abuse of adults with impaired capacity; others emphasise consent-based adult safeguarding with public-interest exceptions. Do not invent statute numbers in viva. State the principle: clarify local duty, document, escalate through designated channels, and prioritise safety.[1][6]
- Police when a crime is suspected and there is imminent danger, or when the person wants police involvement, or when local duty requires it.[1][13]
- Confidentiality has lawful limits when serious harm risk requires multi-agency sharing — still share the minimum necessary and record the basis.[1][6]
- Victim preference matters highly when capacity is present, but does not erase duties to others (e.g. other residents) or local mandatory duties.[1][8]
Frame answers around elder abuse prevention strategies, aged-care quality and reportable incident principles, state/territory guardianship and enduring power frameworks, and health-service safeguarding pathways. Residential care has additional institutional investigation routes. Avoid quoting fabricated section numbers; name the functional pathway (guardianship, public trustee, police, elder abuse helpline, facility serious incident processes).[1][6]
Definitive multi-agency management
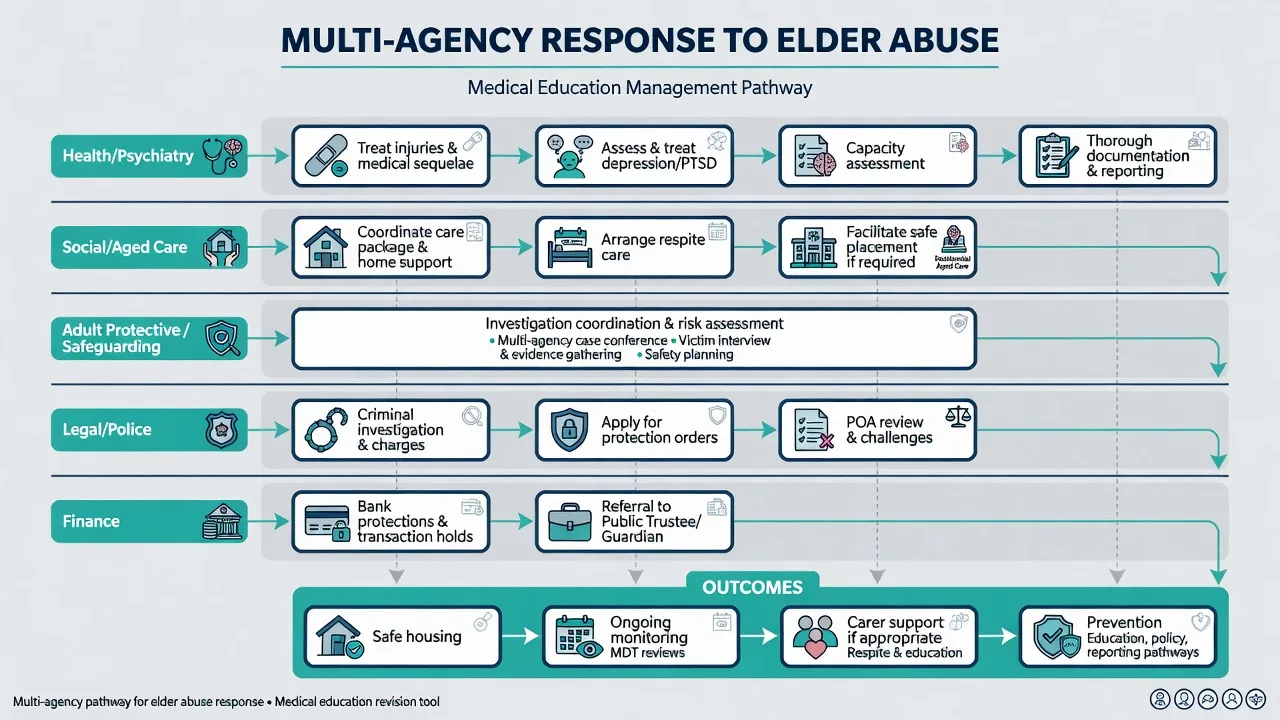
Health/psychiatry lane: treat medical sequelae; assess and treat depression, PTSD symptoms, anxiety, substance use; structured psychotherapy when appropriate; psychotropics only for clear psychiatric indications with geriatric caution; capacity opinions; clear documentation for partners.[1][8]
Social/aged care: packages, respite, alternative placement, carer education, BPSD support that reduces strain without chemical restraint abuse.[7]
Safeguarding/APS: coordinated enquiry, safety planning, case conference.[1][6]
Legal/police: protection/intervention orders principles, criminal investigation when indicated, challenge of improper powers of attorney via lawful process.[1][13]
Finance: bank freezes/alerts, public trustee/financial management orders when capacity for finances is absent and exploitation is active.[1][8]
Carer abuse that is stress-mediated and low-imminence may respond to respite, skills training, substance treatment, and dementia education — but safety overrides rehabilitation of the carer when harm is serious or escalating.[7]
Special scenarios
Dementia. Use dementia-sensitive screening concepts; believe patterns of injury and carer dynamics even when the person cannot give a linear narrative.[12]
Residential care. Facility investigation, alternative placement, and regulatory reporting principles; chemical restraint for staff convenience is an abusive practice frame.[1][2]
Self-neglect. Map capacity for specific decisions (accepting home care, hospitalisation). Capacious refusal of services is ethically hard; incapacitous self-neglect needs substitute pathways and least-restrictive support.[8][10]
Cultural safety. Independent interpreters; fear of authorities; sponsor-family dependence in migrant older adults; Indigenous older adults require culturally safe assessment and community-informed supports without minimising harm.[1][2]
Prognosis and disposition
Mistreatment-associated mortality and hospitalisation risk justify aggressive safety planning rather than passive observation.[3][11] Disposition requires a named safe destination, follow-up owner, multi-agency contacts, and review date. Prevention includes reducing isolation, supporting carers of people with dementia, financial safeguards, and staff training in detection.[2][6]
Exam pearls
SAFEGUARD (bedside prompt)
Pitfalls
- Equating dementia with incapacity for all decisions.[8]
- Inventing mandatory reporting sections in viva.[6]
- Accepting "she bruises easily" without pattern analysis.[1][13]
- Discharging home with the abuser as "carer" and no plan.[1][3]
- Antipsychotics for fear that is reality-based.[1]
- Ignoring financial exploitation because there are "no bruises."[1][4]
- Under-estimating psychological abuse and coercive control.[1][2]
Fellowship standard: recognise early, protect first, assess capacity properly, treat mental health sequelae, coordinate safeguarding — and speak about law as jurisdiction-specific principles, not improvised statutes.[1][2][8]
References
- [1]Lachs MS, Pillemer KA Elder Abuse N Engl J Med, 2015.PMID 26559573
- [2]Pillemer K, Burnes D, Riffin C, Lachs MS Elder Abuse: Global Situation, Risk Factors, and Prevention Strategies Gerontologist, 2016.PMID 26994260
- [3]Lachs MS, Williams CS, O'Brien S, Pillemer KA, Charlson ME The mortality of elder mistreatment JAMA, 1998.PMID 9701077
- [4]Acierno R, Hernandez MA, Amstadter AB, Resnick HS, Steve K, et al. Prevalence and correlates of emotional, physical, sexual, and financial abuse and potential neglect in the United States: the National Elder Mistreatment Study Am J Public Health, 2010.PMID 20019303
- [5]Yon Y, Mikton CR, Gassoumis ZD, Wilber KH Elder abuse prevalence in community settings: a systematic review and meta-analysis Lancet Glob Health, 2017.PMID 28104184
- [6]Cooper C, Selwood A, Livingston G Knowledge, detection, and reporting of abuse by health and social care professionals: a systematic review Am J Geriatr Psychiatry, 2009.PMID 19916205
- [7]Cooper C, Selwood A, Blanchard M, Walker Z, Blizard R, et al. The determinants of family carers' abusive behaviour to people with dementia: results of the CARD study J Affect Disord, 2010.PMID 19446884
- [8]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [9]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [10]Sessums LL, Zembrzuska H, Jackson JL Does this patient have medical decision-making capacity? JAMA, 2011.PMID 21791691
- [11]Dong X, Simon MA Elder abuse as a risk factor for hospitalization in older persons JAMA Intern Med, 2013.PMID 23567991
- [12]Wiglesworth A, Mosqueda L, Mulnard R, Liao S, Gibbs L, et al. Screening for abuse and neglect of people with dementia J Am Geriatr Soc, 2010.PMID 20398118
- [13]Rosen T, Hargarten S, Flomenbaum NE, Platts-Mills TF Identifying Elder Abuse in the Emergency Department: Toward a Multidisciplinary Team-Based Approach Ann Emerg Med, 2016.PMID 27005448
- [14]Burnes D, Pillemer K, Caccamise PL, Mason A, Henderson CR Jr, et al. Prevalence of and Risk Factors for Elder Abuse and Neglect in the Community: A Population-Based Study J Am Geriatr Soc, 2015.PMID 26312573
- [15]Gallione C, Dal Molin A, Cristina FVB, Ferns H, Mattioli M, et al. Screening tools for identification of elder abuse: a systematic review J Clin Nurs, 2017.PMID 28042891
- [16]Lachs MS, Pillemer K Abuse and neglect of elderly persons N Engl J Med, 1995.PMID 7632211