Psych · Old age psychiatry — falls polypharmacy frailty
Falls, polypharmacy and frailty in old-age psychiatry
Also known as Falls in older adults psychiatry · Polypharmacy old-age psychiatry · Frailty and psychotropics · Fall-risk-increasing drugs FRIDs · Deprescribing frail elderly psychiatry · Geriatric falls medication review · Psychotropics and falls
Exam-exhaustive fellowship reference on falls, polypharmacy and frailty in old-age psychiatry — Fried vs Rockwood frailty, FRID psychotropics, Beers and STOPP/START, multifactorial falls prevention, deprescribing, safe late-life prescribing under frailty. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship viva language is concrete: name frailty frameworks, cite FRID meta-analyses, give illustrative deprescribing and safer start doses with monitoring, and refuse both sedative stacking and under-treatment of severe late-life depression.[3][5][13][16]
Definition and classification
A fall is an unintentional event in which a person comes to rest on the ground or another lower level. Exam discriminators separate mechanical trips, orthostatic or cardiac syncope, seizure, drop attacks, and drug-related ataxia or sedation — the chart phrase "mechanical fall" is not a diagnosis.[10]
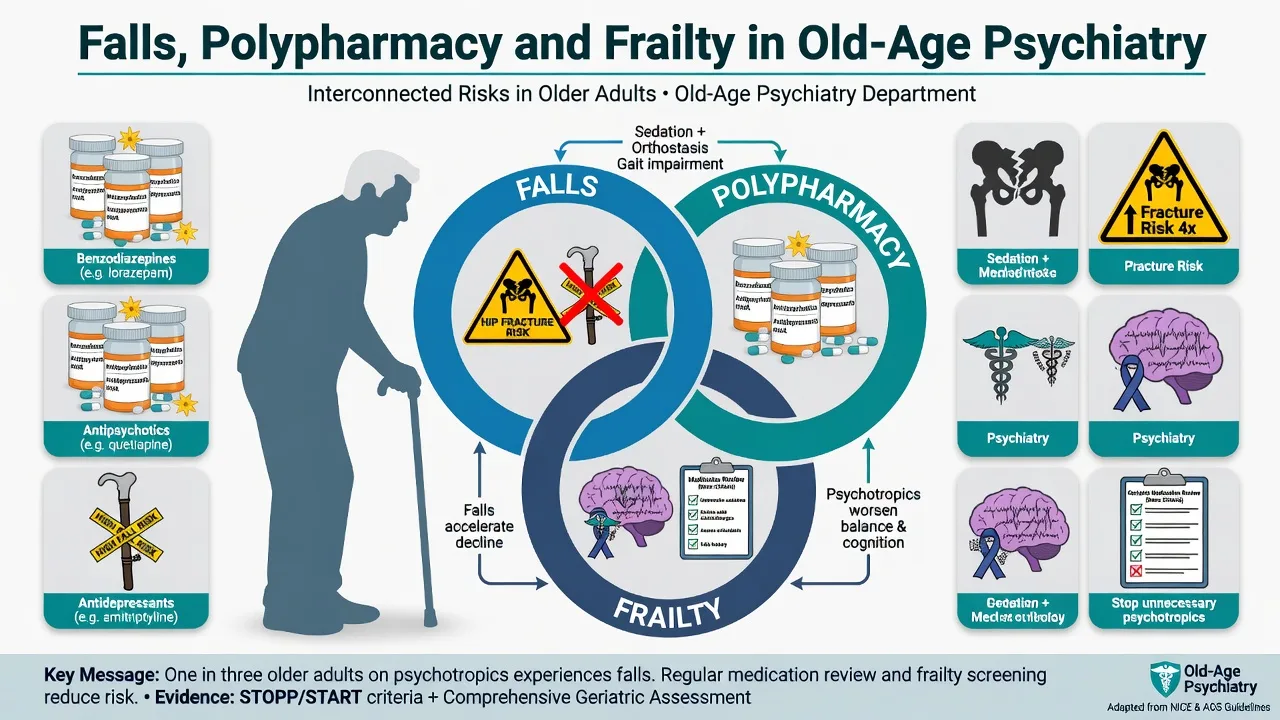
Polypharmacy is commonly operationalised as five or more regular medicines; hyperpolypharmacy is often ten or more. The clinically useful split is appropriate multimorbidity prescribing versus potentially inappropriate polypharmacy — including potentially inappropriate medications (PIMs) and fall-risk-increasing drugs (FRIDs).[7][8][13]
Frailty is a state of increased vulnerability to poor resolution of homeostasis after a stressor event — the most problematic expression of population ageing in geriatric medicine and highly relevant when any psychotropic is considered.[3]
| Construct | Core idea | Exam use |
|---|---|---|
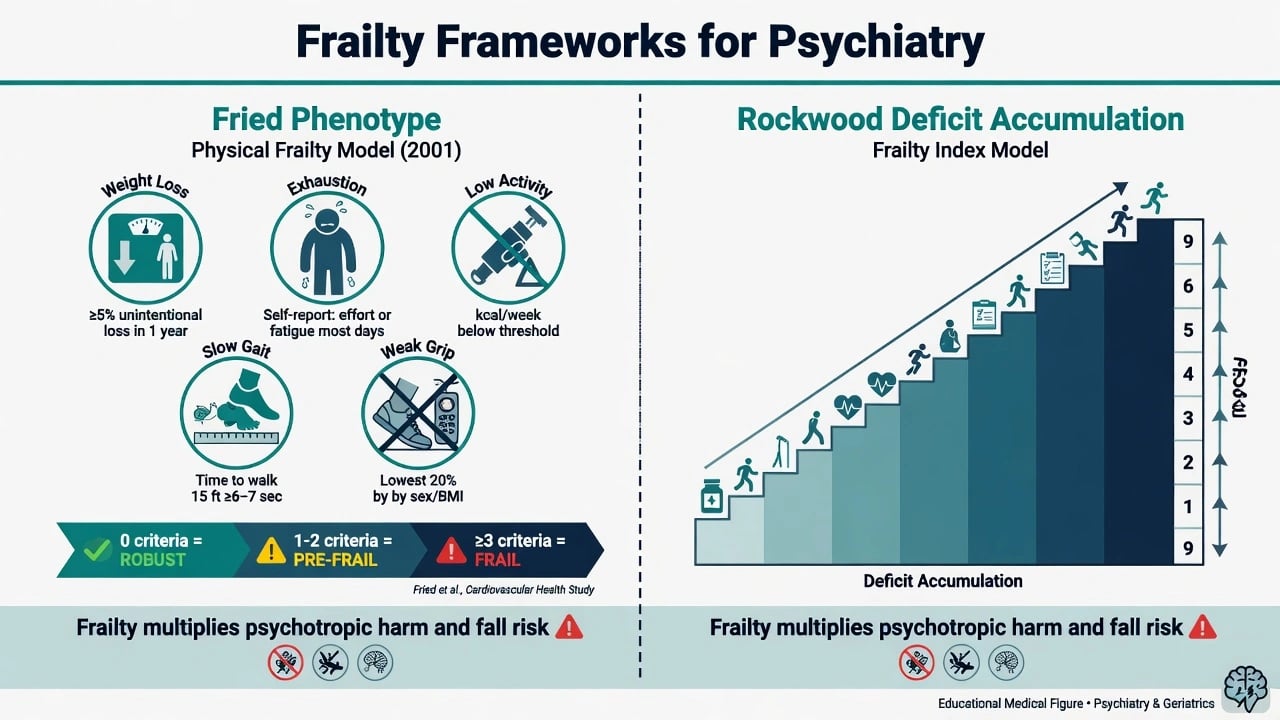
| Fried phenotype | Five criteria: weight loss, exhaustion, low activity, slow gait, weak grip | 0 robust; 1–2 pre-frail; ≥3 frail |
| Rockwood deficit accumulation | Frailty as cumulative health deficits → frailty index | Continuous risk; Clinical Frailty Scale (CFS) bedside grade |
| Polypharmacy / PIMs | Drug count plus appropriateness | Beers lists; STOPP stop rules; START missing treatments |
| FRIDs | Drug classes linked to falls | Psychotropics are high-yield for psychiatry exams |
Epidemiology and risk
Falls are common in community-dwelling older adults and more frequent in residential aged care and psychogeriatric settings. Prior falls strongly predict future falls; injurious falls drive fracture, hospitalisation, fear of falling, institutionalisation and mortality risk.[3][10]
Psychotropic exposure associates consistently with falls. Woolcott meta-analysis of nine medication classes links sedatives/hypnotics, antidepressants and benzodiazepines (among others) to falls in elderly persons; Seppala EuGMS FRID work shows antipsychotics, antidepressants and benzodiazepines are consistently associated with higher fall risk.[4][5] Glass meta-analysis finds unfavourable risk–benefit for sedative-hypnotics in older people with insomnia — a classic falls-related teaching point.[6]
Headline risk anchors for viva recall
Risk amplifiers. Frailty, prior falls, orthostatic hypotension, visual impairment, cognitive impairment and dementia, gait and balance disorder, environmental hazards, alcohol, nocturia, Parkinsonism or drug-induced EPS, and stacked CNS-active drugs.[3][4][5][10]
Pathophysiology and mechanisms
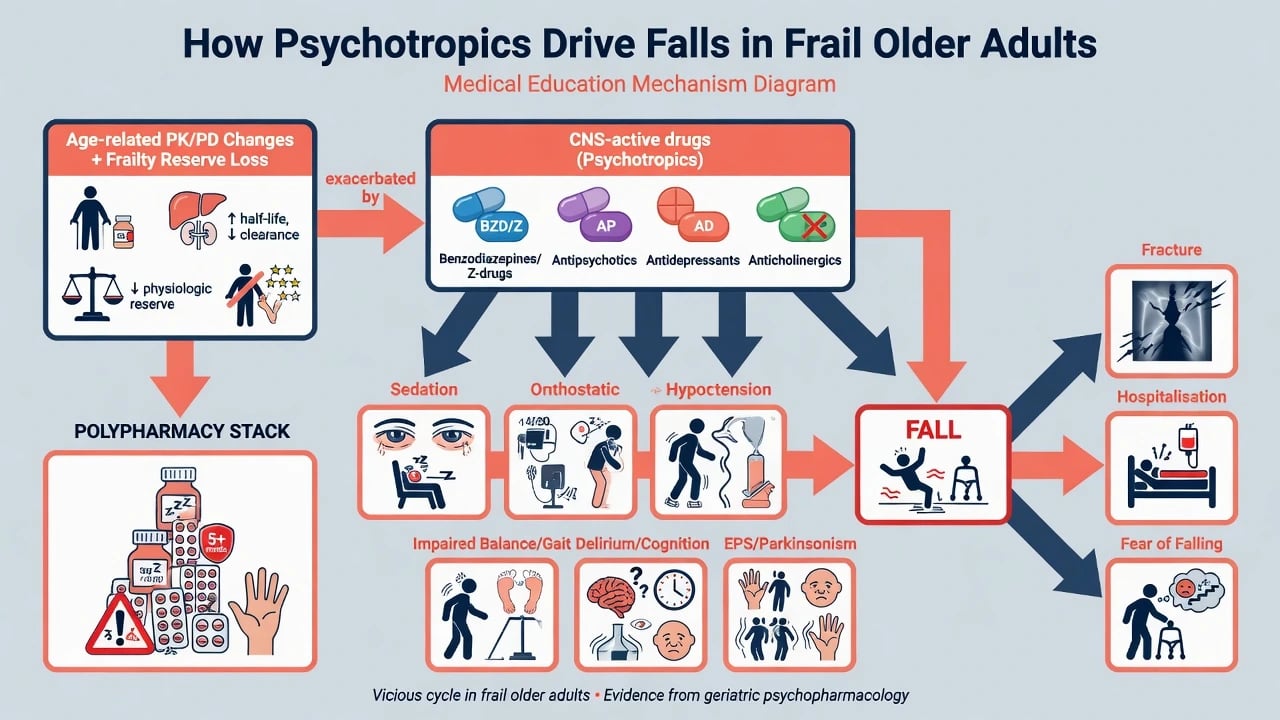
Mangoni and Jackson summarise age-related pharmacokinetic change (reduced hepatic blood flow and phase I capacity, declining GFR, increased fat:lean ratio prolonging lipophilic half-lives) and pharmacodynamic change (greater CNS sensitivity to GABA-A agonists and anticholinergics; impaired baroreflex and orthostatic tolerance).[16]
Frailty multiplies harm because physiological reserve is already reduced across neuromuscular, cardiovascular and cognitive systems — a minor sedative load or orthostatic dip becomes a hip fracture rather than a recoverable stumble.[3]
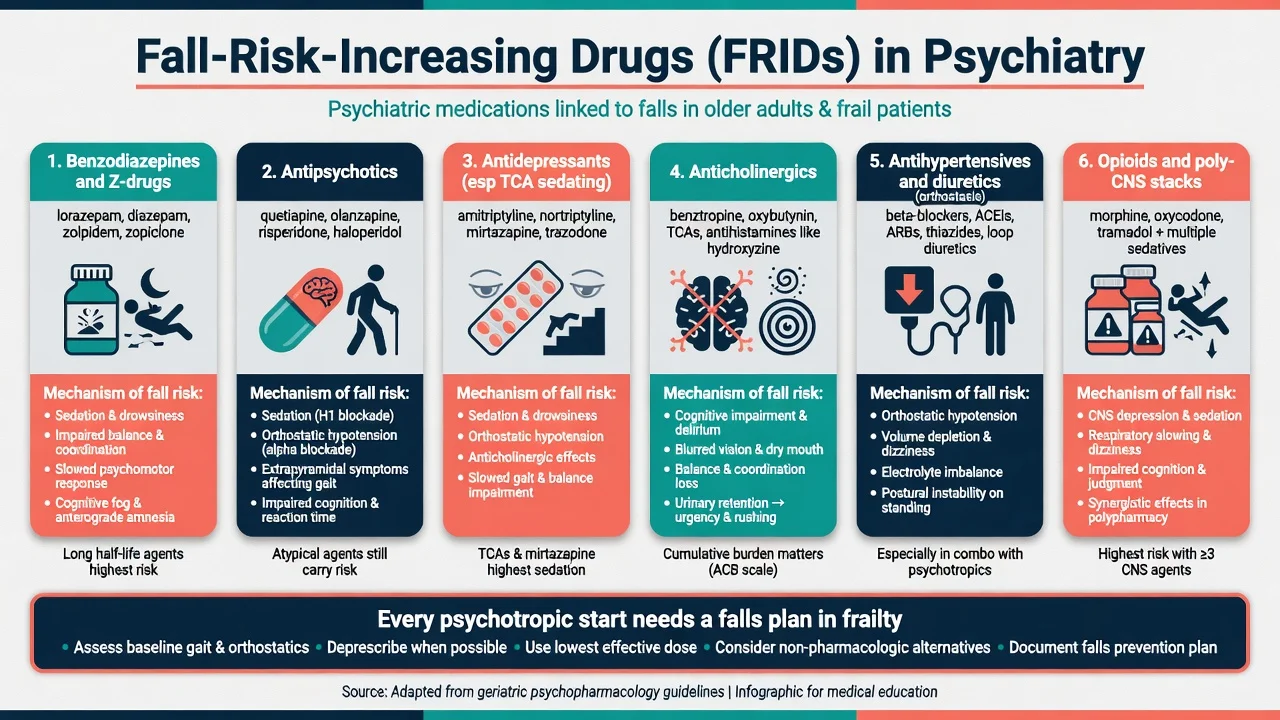
Drug → fall pathways examiners want — psychotropic FRIDs act via sedation, orthostasis, gait impairment, cognition and EPS, and stacked CNS load multiplies risk.[4][5][6]
- Benzodiazepines / Z-drugs: sedation, delayed reaction time, ataxia, night confusion.[4][5][6]
- Antipsychotics: sedation, orthostasis, EPS/parkinsonism, plus mortality/stroke signals in dementia.[5][15]
- Antidepressants: sedation (especially TCAs, mirtazapine, some older agents), orthostasis (TCAs), hyponatraemia (SSRI/SNRI) presenting as falls or confusion.[4][5]
- Anticholinergics: cognitive impairment, blurred vision, delirium — falls as a systems failure.[7]
- Stacked polypharmacy: multiplicative CNS load and drug–drug interactions.[4][5][16]
Post-fall cascade. Injury → fear of falling → activity restriction → deconditioning → worsening frailty → more falls and often institutional pressure for more sedation — a loop old-age psychiatrists must break.[3][10]
Clinical presentation
Structure the falls history: timing (relation to dose changes), location, witnesses, prodrome (dizziness, palpitations, blackout), injury, loss of consciousness, recovery, footwear and environment, and alcohol.[10]
Iatrogenic patterns are high yield: morning hangover sedation after night temazepam; orthostatic dizziness days after antipsychotic start; anticholinergic confusion; SSRI-associated hyponatraemia with falls and seizures; akathisia misread as agitation and treated with more antipsychotic.[5][7][16]
Fear of falling and functional decline are clinical outcomes, not soft afterthoughts — they worsen depression, isolation and residential placement risk.[3]
Differential diagnosis
Syncope / cardiac
- Prodrome, exertional or postural clues
- QT-risk polypharmacy context
- ECG and electrolytes
- Not 'mechanical fall' by default
Drug / FRID effect
- Temporal link to start or dose-up
- Sedation, ataxia, orthostasis
- Polypharmacy stack present
- Fix list before adding more
Delirium / medical
- Acute fluctuating inattention
- Infection, pain, constipation, Na
- Falls as presenting feature
- Do not label pure delirium as BPSD
Neurodegenerative
- Gait failure in PD/DLB/PSP
- Drug-induced parkinsonism mimic
- Visual hallucinations in DLB
- Extreme AP caution
Bedside assessment
- Falls history and injury survey with collateral (family, RACF, ward staff).[10]
- Full medication reconciliation — prescribed, PRN residential stock, OTC anticholinergics, opioids, alcohol, herbals.[7][8]
- Frailty screen — Fried criteria where feasible, or Clinical Frailty Scale / deficit-accumulation thinking at the bedside.[1][2][3]
- Orthostatic BP, gait and balance, vision, footwear, home or ward environment hazards.[10]
- Cognition, mood, psychosis, capacity — capacity for deprescribing decisions and substitute decision-maker engagement when dementia is present.[13]
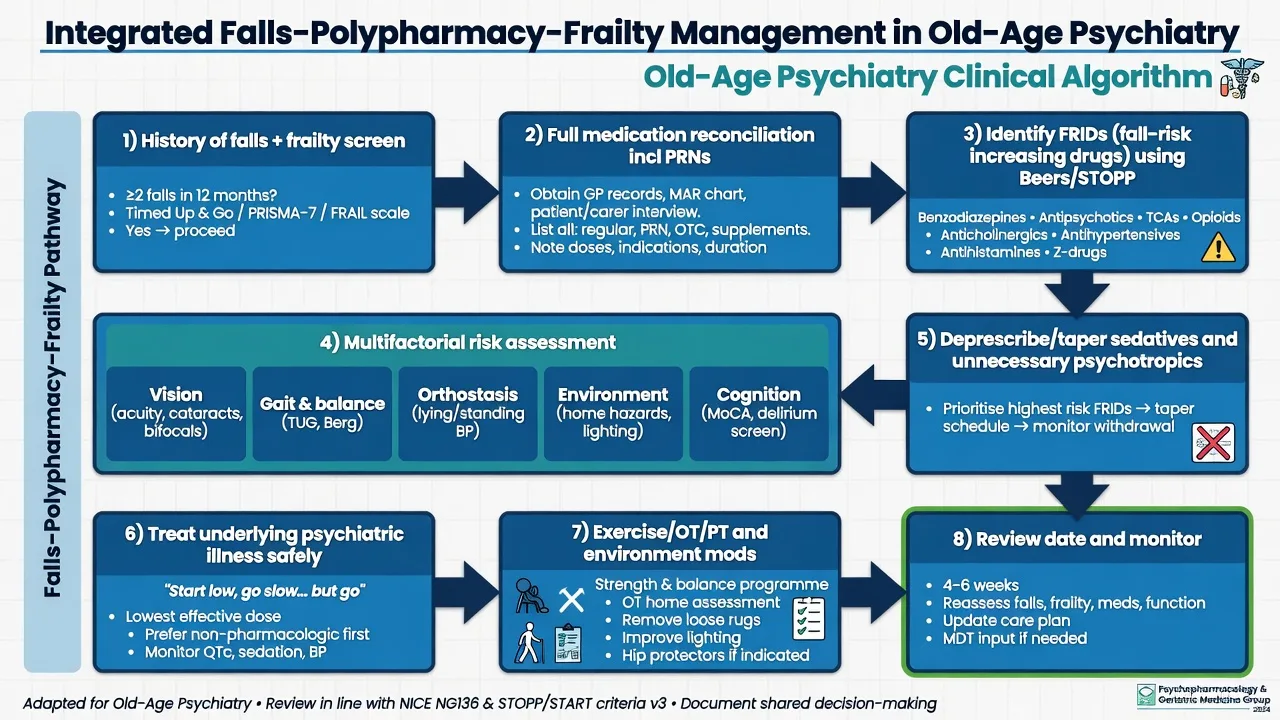
- Beers + STOPP/START lens — list PIMs and FRIDs; use START so under-treatment (e.g. untreated severe depression) is not missed.[7][8][9]
Investigations
Targeted, not shotgun: U&E with sodium and eGFR (SIADH, dehydration, renal clearance), glucose, FBC, TSH/B12/folate as indicated, vitamin D when deficiency or bone health is relevant. ECG when QT-risk psychotropics, syncope, or electrolyte disturbance. Imaging follows head-injury and neurological red-flag rules — not every fall needs a CT. Bone-health pathway (fracture risk tools, DEXA referral framing) after recurrent falls or fragility fracture.[10][16]
Acute and emergency management
Definitive management — integrated algorithm
Multifactorial falls prevention
AGS/BGS guidance and Cochrane evidence support multifactorial assessment and intervention rather than a single silver bullet. Community evidence is strongest for exercise programmes (balance and strength), home safety interventions, and multifactorial packages that may reduce fall rates; Hopewell review supports multifactorial approaches for rate of falls with more uncertain effects on people sustaining one or more falls.[10][11][12]
Components examiners list: exercise (physio-led balance/strength), vision optimisation, footwear and environment, treat orthostasis and nocturia drivers, bone health, education, and medication review with FRID focus.[10][11]
Psychotropic FRID strategy and deprescribing
Deprescribing is the supervised process of dose reduction or stopping medicines that may be causing harm or are no longer beneficial — part of good prescribing, not therapeutic abandonment.[13][14]
High-yield deprescribing targets in psychiatry follow Beers/STOPP logic and FRID meta-analyses: taper unnecessary sedatives and open-ended dementia antipsychotics, reduce anticholinergic load, and avoid chaotic multi-drug stops.[5][6][7][8][13][15]
| Target | Approach | Safety notes |
|---|---|---|
| Benzodiazepines / Z-drugs | Gradual taper; non-drug sleep and anxiety strategies | Beers avoid; falls and cognition risk; Glass unfavourable R:B |
| Long-term antipsychotics in dementia without current severe target | Supervised taper with restart threshold | Mortality/stroke literacy; not chaotic stop |
| TCAs and strong anticholinergics | Switch or stop when safer alternatives exist | Delirium, orthostasis, falls |
| Duplicative sedating stacks | Remove one CNS sedative at a time when frail | Monitor psychiatric relapse and withdrawal |
| Process | Scott deprescribing steps; written review date | Individualise goals of care |
When psychotropics remain necessary. Severe late-life major depression, mania, psychosis, or severe BPSD with risk of harm still need treatment. Core maxim: start low, go slow, but go to a therapeutic dose and duration — token micro-doses for months create pseudo-resistance and unfinished MEQs.[13][16]
Illustrative safer starts in frailty (individualise; check product information). Sertraline 25 mg orally daily for several days then 50 mg daily, with early sodium check especially if on diuretics, plus falls and bleeding vigilance on anticoagulation; mirtazapine 7.5–15 mg orally at night when sedation/appetite help is desired but with explicit falls counselling; if a time-limited antipsychotic is unavoidable for severe aggression after non-drug care, illustrative frail oral starts include risperidone 0.25–0.5 mg with documented target, consent discussion, falls precautions and a stop/review date — not open-ended use for wandering or calling out.[7][15][16]
Subtypes and high-yield scenarios
Community late-life depression + temazepam + two falls. Deprescribe temazepam with sleep hygiene and treat depression to efficacy; do not leave untreated severe MDD because of falls fear alone.[6][13]
RACF dementia on chronic risperidone + night Z-drug. Reconcile PRNs; non-drug ABC/pain review; supervised antipsychotic and hypnotic taper with staff education; black-box mortality framing for family discussion.[7][15]
Ward falls on psychogeriatric unit. Environment + observation level + FRID review + orthostasis + delirium screen — not only "increase specialling" while adding more sedation.[4][5][10]
Possible DLB with hallucinations and falls. Extreme antipsychotic caution; rethink diagnosis if severe neuroleptic sensitivity appears.[15]
Lithium into frailty with falling GFR. Dose and level revision, renal/thyroid/calcium monitoring, toxicity literacy with dehydration and interacting drugs.[16]
Complications and pitfalls
- Physio-only falls plan while FRIDs continue unchanged.[4][5]
- Adding sedatives for pain-, constipation-, or delirium-driven "agitation."[7]
- Assuming Z-drugs are freeride hypnotics in frail adults.[6][7]
- Open-ended antipsychotics for mild BPSD.[15]
- Chaotic multi-drug stop without monitoring relapse or withdrawal.[13]
- Start-low-stay-low under-treatment of depression.[16]
- Missing orthostasis, hyponatraemia, and head injury red flags.[10]
Prognosis and disposition
Prior falls predict further falls; recurrent events raise fracture and institutionalisation risk. Community multifactorial and exercise interventions can reduce fall rates; residential care is harder and needs culture change as much as individual scripts.[11][12] Disposition spans GP collaborative care, pharmacy-led reviews, falls clinics, old-age CMHT, RACF medication advisory processes, and hospital consultation-liaison for complex polypharmacy. Follow-up intensity peaks after new psychotropic starts and after deprescribing steps.[13]
Special populations
Oldest-old / high CFS frailty — fewer concurrent drug changes, lower starts, goals-of-care honesty.[3] Dementia subtypes — DLB/PDD extreme neuroleptic caution.[15] Residential care — PRN culture and staff education are part of the prescription. Cultural diversity and Indigenous older adults — family decision styles, language access, and equitable review. Intellectual disability ageing — diagnostic overshadowing and high polypharmacy risk.
Evidence and regional guidelines
Landmark anchors: Fried phenotype; Rockwood deficit accumulation; Clegg frailty review; Woolcott medications-and-falls meta-analysis; Seppala psychotropic FRIDs; Glass sedative-hypnotics; AGS Beers 2023; STOPP/START v2 and v3; AGS/BGS falls guideline summary; Gillespie and Hopewell Cochrane falls reviews; Scott and Reeve deprescribing; Schneider antipsychotic mortality meta-analysis; Mangoni age-related PK/PD.[1][3][4][5][7][10][13][15]
Australian and New Zealand practice integrates geriatric medicine falls pathways with old-age psychiatry medication review. Emphasise Beers/STOPP-style PIM thinking, non-drug BPSD care, and TGA/Medsafe product information for limited dementia behavioural wording. Shared care with GPs, pharmacists and RACF quality processes. Do not invent Mental Health Act section numbers across jurisdictions.[7][10][15]
Exam pearls
FALLS Rx safety
FALLS-RX
References
- [1]Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype J Gerontol A Biol Sci Med Sci, 2001.PMID 11253156
- [2]Rockwood K, Mitnitski A Frailty in relation to the accumulation of deficits J Gerontol A Biol Sci Med Sci, 2007.PMID 17634318
- [3]Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K Frailty in elderly people Lancet, 2013.PMID 23395245
- [4]Woolcott JC, Richardson KJ, Wiens MO, Patel B, Marin J, Khan KM, Marra CA Meta-analysis of the impact of 9 medication classes on falls in elderly persons Arch Intern Med, 2009.PMID 19933955
- [5]Seppala LJ, Wermelink AMAT, de Vries M, Ploegmakers KJ, van de Glind EMM, Daams JG, et al. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-Analysis: II. Psychotropics J Am Med Dir Assoc, 2018.PMID 29402652
- [6]Glass J, Lanctôt KL, Herrmann N, Sproule BA, Busto UE Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits BMJ, 2005.PMID 16284208
- [7]By the 2023 American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [8]O'Mahony D, O'Sullivan D, Byrne S, O'Connor MN, Ryan C, Gallagher P STOPP/START criteria for potentially inappropriate prescribing in older people: version 2 Age Ageing, 2015.PMID 25324330
- [9]O'Mahony D, Cherubini A, Guiteras AR, Denkinger M, Beuscart JB, Onder G, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3 Eur Geriatr Med, 2023.PMID 37256475
- [10]Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons J Am Geriatr Soc, 2011.PMID 21226685
- [11]Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, Lamb SE Interventions for preventing falls in older people living in the community Cochrane Database Syst Rev, 2012.PMID 22972103
- [12]Hopewell S, Adedire O, Copsey BJ, Boniface GJ, Sherrington C, Clemson L, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community Cochrane Database Syst Rev, 2018.PMID 30035305
- [13]Scott IA, Hilmer SN, Reeve E, Potter K, Le Couteur D, Rigby D, et al. Reducing inappropriate polypharmacy: the process of deprescribing JAMA Intern Med, 2015.PMID 25798731
- [14]Reeve E, Gnjidic D, Long J, Hilmer S A systematic review of the emerging definition of 'deprescribing' with network analysis: implications for future research and clinical practice Br J Clin Pharmacol, 2015.PMID 27006985
- [15]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [16]Mangoni AA, Jackson SHD Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications Br J Clin Pharmacol, 2004.PMID 14678335