Psych · Old age psychiatry — anxiety disorders
Late-life anxiety disorders
Also known as Geriatric anxiety · Anxiety in older adults · Late-life GAD · Late-onset anxiety · Anxiety disorders in the elderly
Exam-exhaustive fellowship reference on late-life anxiety disorders — DSM-5-TR/ICD-11 framing, epidemiology (Beekman LASA, Byers NCS-R), GAD dominance, medical differentials, GAD-7, late-life CBT (Stanley, Brenes, Wetherell), SSRI/SNRI dosing with hyponatraemia vigilance (Lenze, Fabian), benzodiazepine harms (Beers, Billioti de Gage), fear of falling, suicide comorbidity, RANZCP/NICE/APA-aligned stepped care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Late-life anxiety is a high-yield FRANZCP old-age topic and a frequent MRCPsych/ABPN trap because examiners expect you to treat real disability without defaulting to long-term benzodiazepines or dismissing symptoms as normal ageing. A candidate who masters epidemiology, differentials, CBT and SSRI evidence, hyponatraemia, and Beers-criteria prescribing can answer most stems without another resource.[1][2][8]

Overview and definition
Late-life anxiety disorders describe clinically significant anxiety syndromes in older adults (commonly operationalised as age 60 or 65 years and older). The label is not a single DSM code: it groups DSM-5-TR anxiety disorders — especially generalised anxiety disorder (GAD), panic disorder, agoraphobia, social anxiety disorder, and specific phobia — plus anxiety due to another medical condition and substance/medication-induced anxiety when those apply.[2]
DSM-5-TR GAD requires excessive anxiety and worry more days than not for at least 6 months about a number of events or activities, difficulty controlling the worry, associated symptoms (restlessness, fatigue, concentration difficulty, irritability, muscle tension, sleep disturbance), and clinically significant distress or impairment, not better explained by substances, medical conditions, or another mental disorder.[2][15]
ICD-11 frames anxiety disorders with duration, severity, and functional descriptors that map closely enough for clinical work; when anxiety is fully explained by a medical condition or substance, classify as secondary rather than primary anxiety disorder.[2]
Two populations dominate exam thinking: (1) early-onset anxiety continuing into old age, often lifelong GAD with late medical amplification; and (2) late-onset first presentations, which force a higher yield organic and substance work-up.[1][2]
Classification pathways
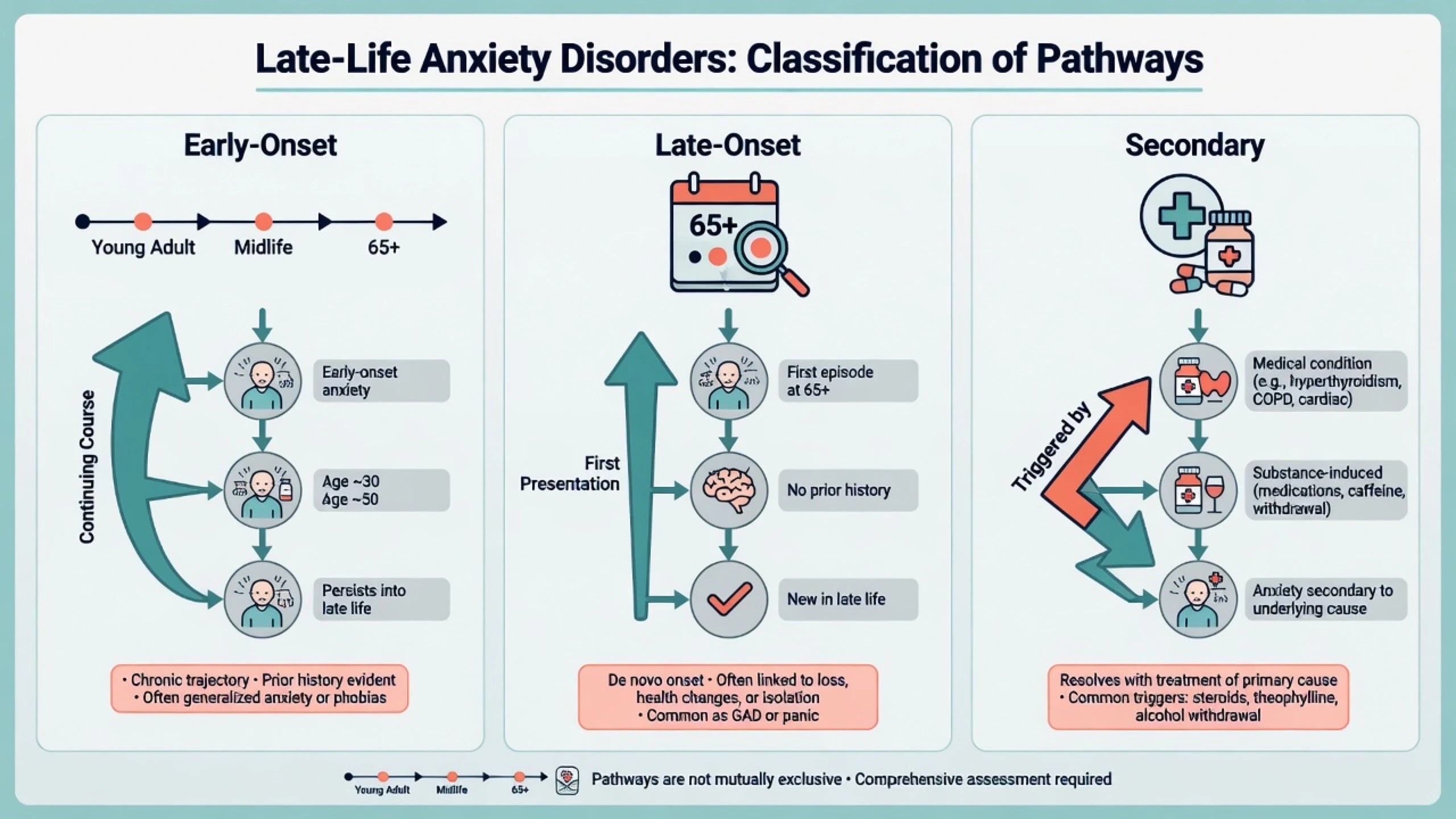
| Pathway | Typical clues | Exam priority |
|---|---|---|
| Early-onset into late life | Decades of worry, family history, prior treatment | Optimise CBT/SSRI; deprescribe BZD |
| Late-onset first episode | First florid anxiety after 60; medical change | Exclude organic/substance causes |
| Secondary anxiety | Temporal link to drug, thyroid, arrhythmia, withdrawal | Treat driver and syndrome |
| These are teaching constructs; individual patients may straddle columns.[1][2] |
Subthreshold worry and mixed anxiety–depression still impair function and drive primary-care visits; do not withhold stepped care because full syndromal criteria are narrowly missed when disability is clear.[3][4]
Epidemiology, burden, and risk
Community samples show anxiety disorders remain common and clinically important in later life. The Longitudinal Aging Study Amsterdam documented substantial anxiety morbidity in older adults, and National Comorbidity Survey Replication analyses highlight high occurrence of mood and anxiety disorders among older adults when lifetime and recent patterns are considered carefully.[1][3]
GAD is the anxiety syndrome most frequently encountered and studied in late life. Late-life GAD confers disability, poorer health-related quality of life, and increased healthcare utilisation beyond medical comorbidity alone.[4][2]
Risk factors include female sex for most anxiety disorders, chronic medical illness, pain, disability, sensory impairment, loneliness, bereavement, prior anxiety or depression, cognitive decline, polypharmacy, alcohol or sedative use, and elder abuse. Comorbidity with major depression is the rule in clinic samples, not the exception.[2][3][16]
Pathophysiology and mechanisms
Fear and worry circuitry involves amygdala–insula threat processing with prefrontal regulation; HPA-axis and autonomic arousal contribute to somatic symptoms without providing a diagnostic blood test.[2]
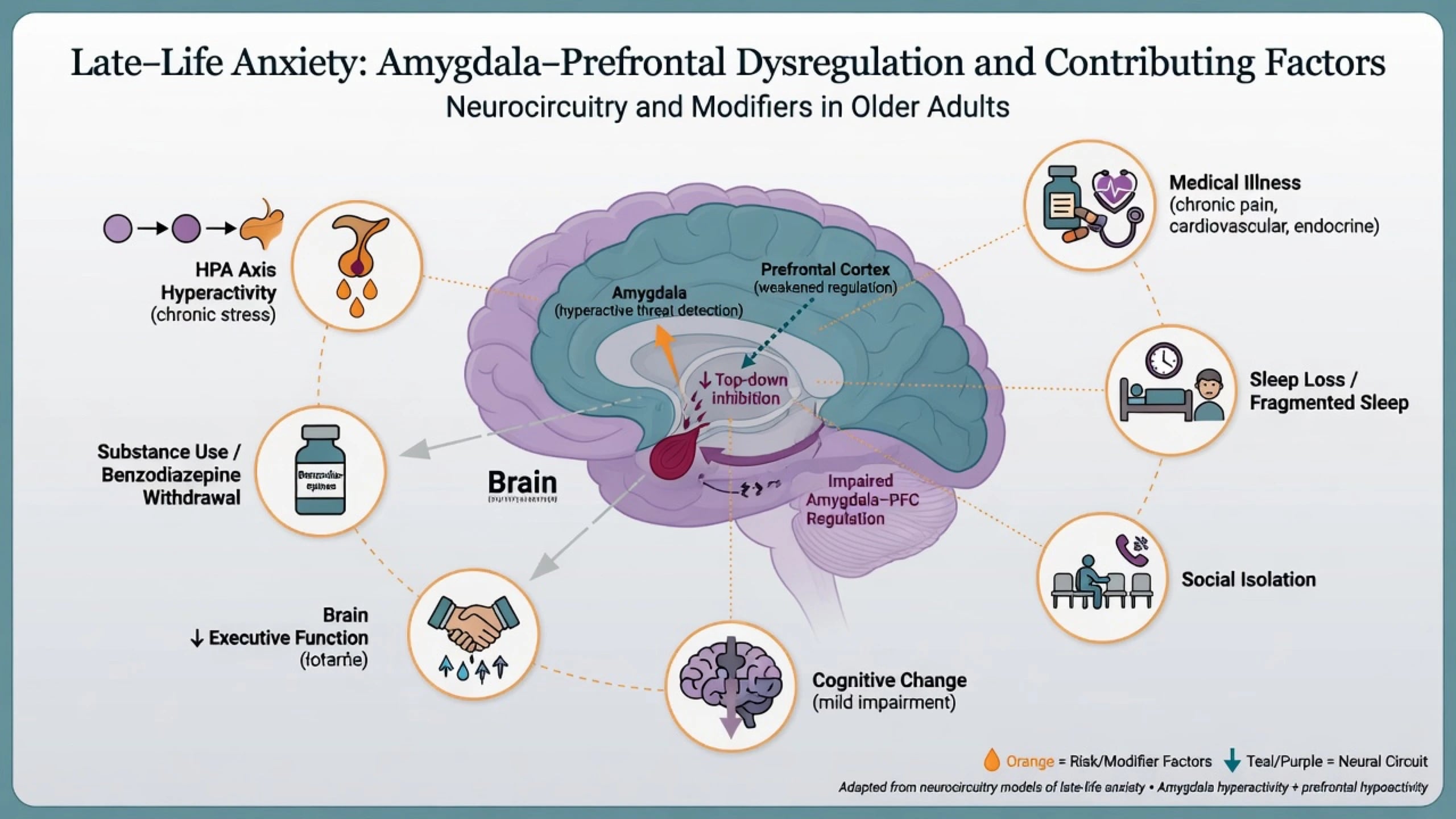
Psychological models remain viva gold: intolerance of uncertainty and worry as cognitive avoidance in GAD; catastrophic misinterpretation and safety behaviours in panic; behavioural restriction after falls creating fear-of-falling loops. Cerebrovascular and neurodegenerative burden can produce late-onset restlessness, irritability, and catastrophic reactions that look like primary anxiety but need cognitive evaluation.[2]
Late-life anxiety associates with cognitive impairment in observational literature; treat anxiety and reassess cognition after improvement rather than prematurely locking in irreversible dementia labels, while still monitoring long-term cognitive trajectory.[2]
Clinical presentation
Late-life GAD. Pervasive worry about health, family safety, finances, and falls; restlessness or fatiguability; concentration difficulty often misattributed to dementia; muscle tension; insomnia; irritability; reassurance seeking from GP and relatives. Older adults may under-report emotion and lead with somatic complaints — chest tightness, GI upset, dizziness, urinary urgency, pain amplification.[2][4]
Panic and agoraphobia. Abrupt surges of fear with autonomic symptoms may be interpreted as cardiac or vestibular disease; housebound avoidance of public transport, shopping, or being alone is a classic late-life functional presentation.[2]
Fear of falling. Overlaps specific phobia, GAD health worry, and post-fall conditioning. It drives social isolation and deconditioning and needs physiotherapy/OT partnership alongside anxiety treatment.[2]
With cognitive impairment. Repetitive anxious questions, catastrophic reactions to minor change, and shadowing of carers may reflect anxiety–MCI/dementia interface rather than pure lifelong GAD alone.[2]
Differential diagnosis
| Discriminator | Primary late-life anxiety | Medical/substance anxiety | Anxious depression |
|---|---|---|---|
| Onset link | May be lifelong or gradual | Temporal to illness/drug/withdrawal | Mood episode package dominates |
| Core affect | Worry, fear, avoidance | Autonomic surge plus medical signs | Anhedonia, guilt, hopelessness |
| Cognition | Worry-related concentration loss | Delirium if fluctuating attention | Depressive cognitive impairment |
| Suicide risk | Elevated if depression comorbid | Variable | Often higher — ask and act |
| Time course, attention, and whether a full depressive syndrome is present remain the fastest bedside discriminators.[2][16] |
Other differentials. Thyrotoxicosis, arrhythmia, hypoxia, anaemia, hypoglycaemia, phaeochromocytoma (rare), alcohol or benzodiazepine withdrawal, stimulant or steroid effects, caffeine excess, illness anxiety disorder, OCD, PTSD, psychotic agitation, akathisia, restless legs, and BPSD-related anxiety.[2]
Primary anxiety and medical disease frequently coexist; treat both rather than forcing a false dichotomy.[2]
Assessment
History structure. Age at onset; lifetime course; prior CBT and medication trials; medical multimorbidity; polypharmacy; alcohol and benzodiazepines; falls and fear of falling; cognitive trajectory; bereavement; isolation; elder abuse screen; living situation and carers; driving and functional status.[2][3]
MSE and risk. Document worry domains, panic symptoms, avoidance, insight, and a direct suicide assessment — especially when depression coexists. Older adults complete suicide with high lethality; ask about ideation, plan, means (medications, firearms), and protective factors.[16]
Scales. GAD-7 is a brief screen and severity tracker; cut-points guide probability of GAD but do not replace structured clinical diagnosis, and somatic multimorbidity or cognitive impairment can inflate or obscure scores.[15] Collateral from family, GP, or aged-care staff is mandatory when under-reporting or cognitive impairment is suspected.[2]
Investigations
Baseline for new, late-onset, or atypical anxiety: FBC, U&E with sodium, LFT, TSH, glucose; B12/folate when cognitive change present; ECG if cardiac symptoms or before QT-risk agents; toxicology when indicated.[2][12]
Imaging is not routine for classic lifelong GAD. Consider neuroimaging for late first onset with atypical features, focal neurology, or rapid cognitive decline.[2]
Monitoring after treatment start: serial GAD-7/CGI; early sodium check after SSRI/SNRI initiation in frail older adults, especially with diuretics — prospective data show clinically important hyponatraemia risk with serotonergic agents such as paroxetine in older adults.[12][15]
Acute and emergency management
Stabilise medical status, restrict lethal means when suicidal ideation is present, determine intensity of care, and apply least-restrictive legal frameworks when capacity and risk demand involuntary care (jurisdiction-specific statutes — state principles, not invented section numbers).[16]
Iatrogenic emergencies. SSRI/SNRI hyponatraemia (confusion, falls, seizures): hold the agent, correct sodium under medical protocols, choose an alternative regimen. Serotonin syndrome and severe activation/akathisia require immediate regimen review.[12]
Definitive management
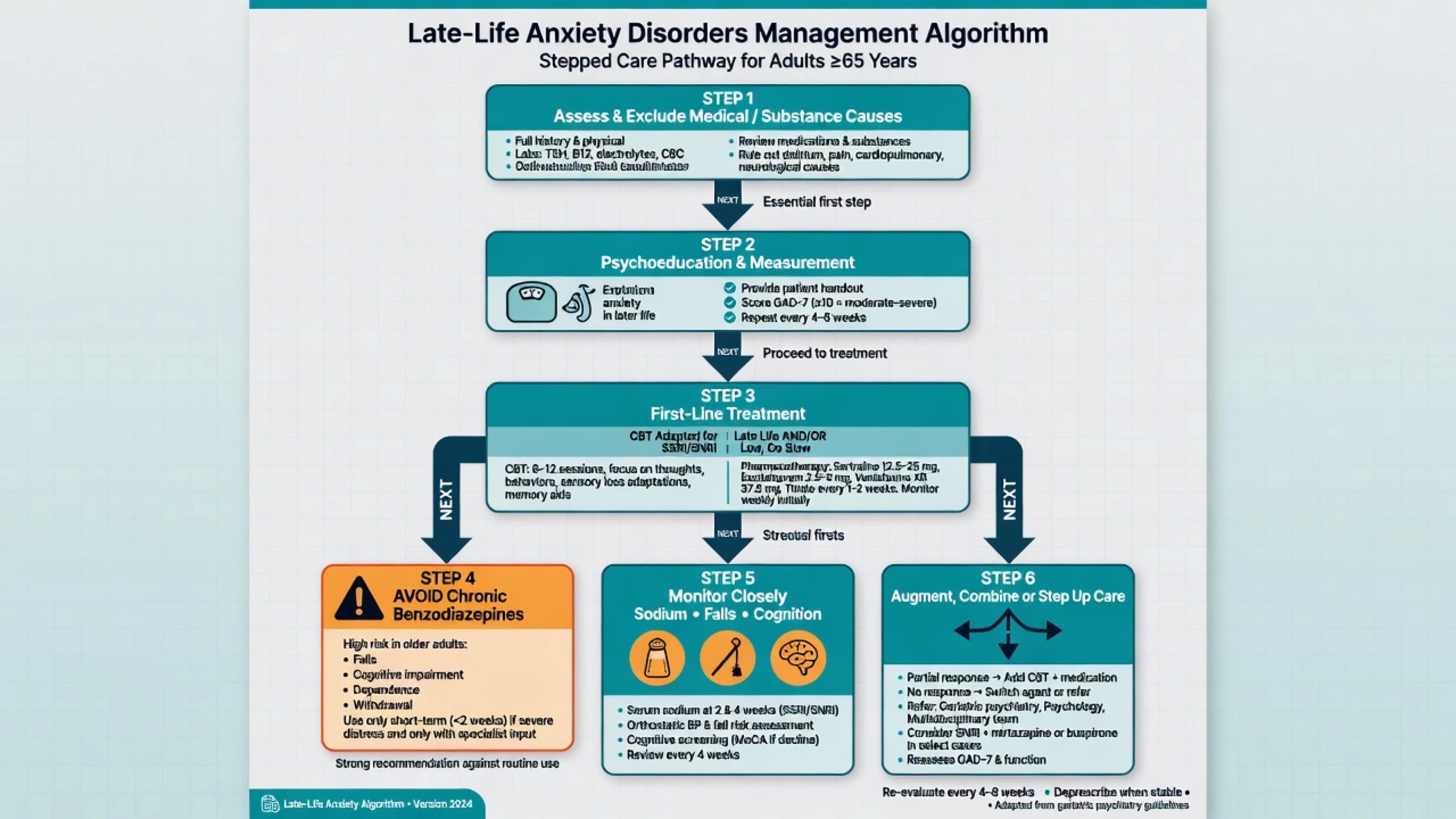
Stepped care principles
- Psychoeducation, sleep, physical activity, treat pain and sensory deficits, reduce caffeine/alcohol.
- Guided self-help or structured CBT adapted for late life when mild–moderate and patient-preferring.
- SSRI/SNRI pharmacotherapy for moderate–severe illness, prior non-response to psychology alone, or patient preference.
- Combine medication and CBT for residual symptoms.
- Specialist old-age psychiatry for complexity, high risk, treatment resistance, or cognitive comorbidity.[2][8][9]
Psychological therapies
Evidence-based reviews support CBT and related behavioural interventions for late-life anxiety; meta-analysis shows both behavioural and pharmacological treatments can work, so modality choice is clinical and preference-sensitive rather than ideology-driven.[8][9]
Stanley and colleagues demonstrated that CBT for GAD among older adults in primary care improves outcomes in a randomised clinical trial — foundational exam evidence that psychological treatment is not “too hard” for older patients when adapted (shorter sessions, memory aids, health-relevant examples).[7] Schuurmans and colleagues compared CBT and sertraline with waitlist control in older adults with anxiety disorders, supporting active treatment over neglect.[11]
Wetherell and colleagues showed that modular CBT can augment antidepressant medication for residual late-life GAD, a high-yield combination strategy for incomplete SSRI response.[10] Telephone-delivered CBT has expanded access for rural and mobility-limited older adults in randomised work (Brenes and related programmes) — cite the principle of accessible CBT delivery when transport is a barrier.[2][9]
Pharmacotherapy
First-line. SSRI or SNRI, start low, go slow, but titrate to an adequate trial. Landmark older-adult data include escitalopram for late-life GAD (Lenze et al., JAMA RCT) and citalopram for late-life anxiety disorders (Lenze et al., placebo-controlled RCT). Apply current product-information maximums and QT cautions for citalopram/escitalopram in older adults; many clinicians prefer sertraline or carefully dosed escitalopram depending on comorbidity and interactions.[5][6]
| Agent (examples) | Older-adult approach (illustrative) | Monitoring focus |
|---|---|---|
| Escitalopram | Start 5 mg orally daily; titrate cautiously toward effective dose within geriatric product limits | Sodium, QT risk factors, falls, activation |
| Sertraline | Start 25 mg orally daily; titrate (e.g. toward 50–100 mg as tolerated) | Sodium, GI effects, hyponatraemia, interactions |
| Citalopram | Use only within current older-adult max dose guidance; QT caution | ECG if risk, sodium, falls |
| Venlafaxine XR / duloxetine | Start low (e.g. venlafaxine XR 37.5 mg orally daily) if SNRI chosen | BP, sodium, discontinuation symptoms |
| These are illustrative geriatric starting strategies aligned with late-life trial dosing philosophy — individualise to eGFR, interactions, and product information.[5][6][11][12] |
Hyponatraemia. Prospective study of paroxetine in older adults demonstrated clinically important rates of sodium decline — treat this as a class-relevant SSRI/SNRI teaching point: check baseline and early follow-up sodium, especially with diuretics, low body weight, or prior SIADH.[12]
Benzodiazepines — exam red zone
AGS Beers Criteria list benzodiazepines as potentially inappropriate in older adults because of falls, fractures, cognitive impairment, and delirium risk. Chronic BZD as sole “treatment” of late-life GAD is a classic fail answer.[14] Observational case-control data associate benzodiazepine use with increased Alzheimer disease risk signals (Billioti de Gage et al.) — discuss carefully as association with confounding, but still favour time-limited use only if a short bridge is essential, with an explicit exit plan.[13][14]
If a short-term BZD is used for severe acute distress (e.g. lorazepam 0.25–0.5 mg orally as needed, time-limited), document indication, review date, falls risk, and concurrent deprescribing plan while SSRI/CBT take effect.[14]
Social and functional interventions
Reduce isolation; optimise hearing and vision; treat pain; involve physiotherapy/OT for fear of falling; support carers; coordinate GP shared care and old-age CMHT when complexity is high.[2][4]
Complications and pitfalls
- Labelling disabling worry as normal ageing and under-treating.[2][4]
- Chronic benzodiazepines without CBT/SSRI pathway.[14]
- Missing hyponatraemia after SSRI/SNRI start.[12]
- Missing comorbid depression and suicide risk.[16]
- Misreading akathisia or medical disease as primary GAD.[2]
- Ignoring fear of falling and housebound panic/agoraphobia.[2]
Prognosis and disposition
Untreated late-life GAD is often chronic with residual worry, disability, and high service use. With CBT and/or adequate antidepressant trials, many patients improve, though residual symptoms are common and may need combination treatment.[4][7][10]
Disposition ladder. Primary care with measurement-based follow-up; psychology/CBT pathways; old-age community mental health teams; intensive community support; voluntary or involuntary inpatient care when suicide risk, severe self-neglect, or medical complexity demands it. Follow-up intensity is highest in the first weeks after SSRI start and during benzodiazepine taper.[2][16]
Special populations
Oldest-old and frailty. Prefer agents with cleaner interaction profiles, lowest effective doses, and aggressive falls prevention. Cognitive impairment. Simplify CBT, involve carers, avoid sedating polypharmacy. Parkinson disease. Anxiety is common; review dopaminergic and anticholinergic load. Cultural diversity. Worry may be expressed somatically; use interpreters and family decision styles appropriately. Residential aged care. High BZD exposure historically — prioritise deprescribing and non-drug strategies.[2][14]
Regional guideline notes
ANZ (RANZCP practice). Anxiety management follows stepped psychological care and antidepressant principles with geriatric prescribing adaptation; deprescribe inappropriate benzodiazepines in older adults and coordinate with GPs and old-age services.[2][14]
UK (NICE-aligned / MRCPsych). Stepped care for GAD and panic — low-intensity psychology first when appropriate, SSRI when indicated, caution with BZD — maps cleanly to late-life answers when start-low pharmacology is added.[2][8]
Canada / international. Canadian anxiety guidelines support CBT and SSRI/SNRI hierarchies; apply older-adult safety filters (sodium, falls, Beers).[2]
US (APA context / ABPN). Lenze escitalopram, Stanley CBT, hyponatraemia, and Beers criteria benzodiazepine items are high-yield board drivers.[5][7][12][14]
Exam pearls
Late-life anxiety exam checklist
This checklist compresses the high-yield viva axes: secondary causes, CBT, SSRI safety, and benzodiazepine deprescribing.[2][7][12][14]
High-yield traps for MCQ/MEQ
- Starting long-term diazepam as definitive late-life GAD care.[14]
- Ignoring sodium after SSRI start in a patient on thiazides.[12]
- Declaring CBT ineffective in older adults contrary to Stanley and related trials.[7][9]
- Missing medical mimics in late first-onset anxiety.[2]
- Inventing identical Mental Health Act section numbers across Australia, NZ, UK, and US in one answer.[2]
References
- [1]Beekman AT, Bremmer MA, Deeg DJ, et al. Anxiety disorders in later life: a report from the Longitudinal Aging Study Amsterdam Int J Geriatr Psychiatry, 1998.PMID 9818308
- [2]Wolitzky-Taylor KB, Castriotta N, Lenze EJ, Stanley MA, Craske MG Anxiety disorders in older adults: a comprehensive review Depress Anxiety, 2010.PMID 20099273
- [3]Byers AL, Yaffe K, Covinsky KE, Friedman MB, Bruce ML High occurrence of mood and anxiety disorders among older adults: The National Comorbidity Survey Replication Arch Gen Psychiatry, 2010.PMID 20439830
- [4]Porensky EK, Dew MA, Karp JF, et al. The burden of late-life generalized anxiety disorder: effects on disability, health-related quality of life, and healthcare utilization Am J Geriatr Psychiatry, 2009.PMID 19472438
- [5]Lenze EJ, Rollman BL, Shear MK, et al. Escitalopram for older adults with generalized anxiety disorder: a randomized controlled trial JAMA, 2009.PMID 19155456
- [6]Lenze EJ, Mulsant BH, Shear MK, et al. Efficacy and tolerability of citalopram in the treatment of late-life anxiety disorders: results from an 8-week randomized, placebo-controlled trial Am J Psychiatry, 2005.PMID 15625213
- [7]Stanley MA, Wilson NL, Novy DM, et al. Cognitive behavior therapy for generalized anxiety disorder among older adults in primary care: a randomized clinical trial JAMA, 2009.PMID 19351943
- [8]Pinquart M, Duberstein PR Treatment of anxiety disorders in older adults: a meta-analytic comparison of behavioral and pharmacological interventions Am J Geriatr Psychiatry, 2007.PMID 17670995
- [9]Ayers CR, Sorrell JT, Thorp SR, Wetherell JL Evidence-based psychological treatments for late-life anxiety Psychol Aging, 2007.PMID 17385978
- [10]Wetherell JL, Petkus AJ, White KS, et al. Antidepressant medication augmented with cognitive-behavioral therapy for generalized anxiety disorder in older adults Am J Psychiatry, 2013.PMID 23680817
- [11]Schuurmans J, Comijs H, Emmelkamp PM, et al. A randomized, controlled trial of the effectiveness of cognitive-behavioral therapy and sertraline versus a waitlist control group for anxiety disorders in older adults Am J Geriatr Psychiatry, 2006.PMID 16505130
- [12]Fabian TJ, Amico JA, Kroboth PD, et al. Paroxetine-induced hyponatremia in older adults: a 12-week prospective study Arch Intern Med, 2004.PMID 14769630
- [13]Billioti de Gage S, Moride Y, Ducruet T, et al. Benzodiazepine use and risk of Alzheimer's disease: case-control study BMJ, 2014.PMID 25208536
- [14]By the 2023 American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [15]Spitzer RL, Kroenke K, Williams JB, Löwe B A brief measure for assessing generalized anxiety disorder: the GAD-7 Arch Intern Med, 2006.PMID 16717171
- [16]Conwell Y, Van Orden K, Caine ED Suicide in older adults Psychiatr Clin North Am, 2011.PMID 21536168