Psych · Old age psychiatry — mood disorders
Late-life bipolar disorder
Also known as Older-age bipolar disorder · OABD · Geriatric bipolar disorder · Late-onset bipolar disorder · Late-onset mania · Secondary mania in older adults
Exam-exhaustive fellowship reference on late-life bipolar disorder — early-onset vs late-onset bipolarity, secondary/organic mania, lithium in the elderly (targets, interactions, toxicity), medical comorbidity, suicide risk and lethality, GERI-BD, maintenance (BALANCE), bipolar depression without antidepressant monotherapy, ECT, RANZCP/CANMAT/BAP. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Late-life bipolar disorder (often framed as older-age bipolar disorder, OABD) is a high-yield FRANZCP old-age and general-adult topic. Examiners test early- versus late-onset constructs, secondary mania work-up, lithium pharmacokinetics in frailty, medical comorbidity, and suicide. MRCPsych and ABPN items probe GERI-BD, interaction traps, and guideline-aligned bipolar depression care. This page is written so a candidate who has read nothing else can answer those questions at consultant depth.[1][2][15]
Overview and definition
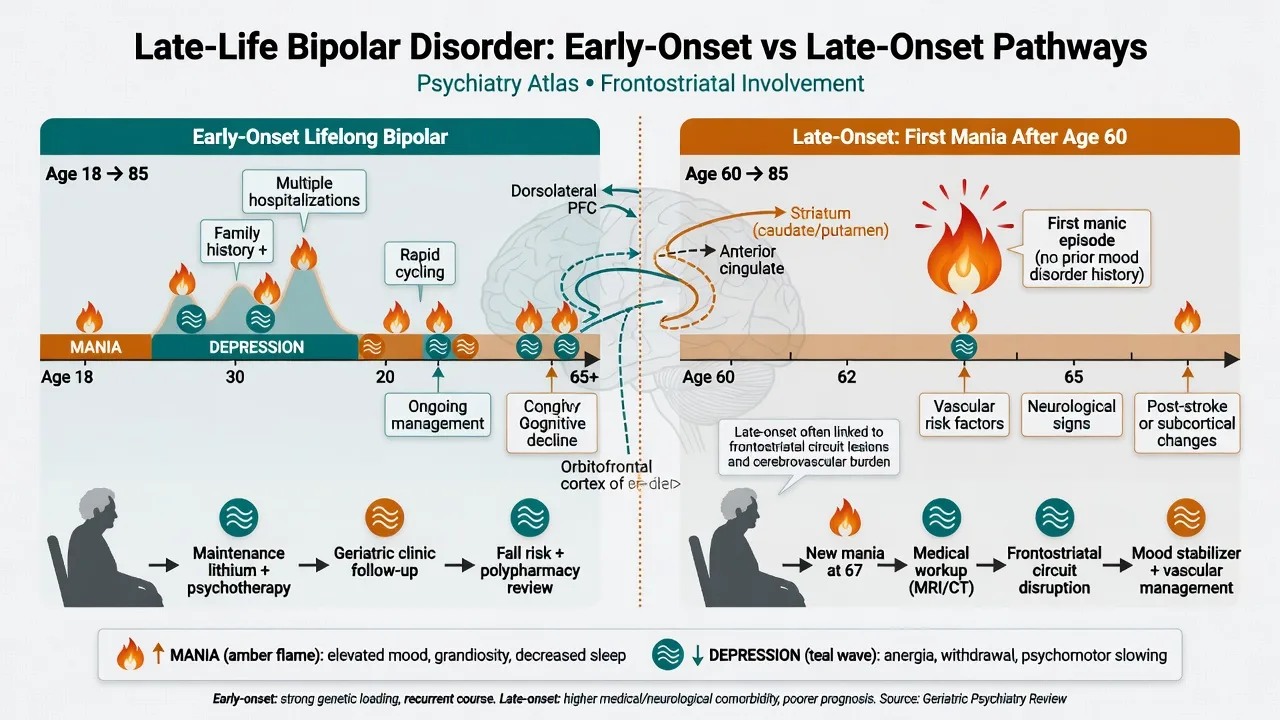
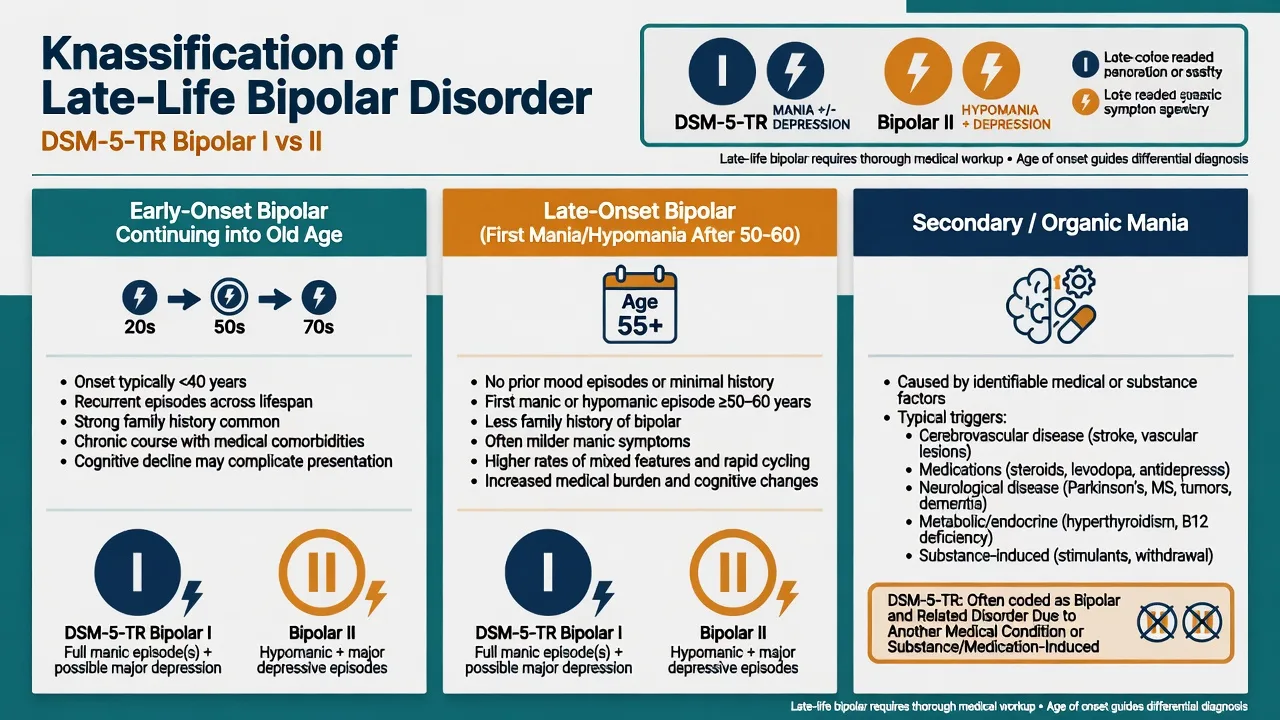
Late-life bipolar disorder is not a single DSM code. It describes clinically significant bipolar I, bipolar II, and related bipolar spectrum syndromes in older adults (commonly operationalised as age 60 or 65 years and older). Two populations dominate clinical and exam thinking: (1) early-onset bipolar disorder (EOBD) beginning in youth or midlife and continuing into old age; and (2) late-onset bipolar disorder (LOBD) with first mania or hypomania in later life (literature cut-offs commonly 50 or 60 years — state the threshold you use).[1][3][5]
DSM-5-TR. Bipolar I requires a lifetime manic episode; major depression is common but not required. Bipolar II requires at least one hypomanic and one major depressive episode without lifetime mania. Specifiers (mixed features, psychotic features, rapid cycling, anxious distress, catatonia, seasonal pattern) remain examinable and clinically useful in older adults.[12][15]
ICD-11. Bipolar type I/II and related mood episode descriptors parallel DSM with course and severity language. When a manic syndrome is fully explained by a medical condition or substance, classify as secondary/organic mood disorder rather than primary bipolar.[13][15]
Classification: EOBD, LOBD, and secondary mania
| Feature | Early-onset bipolar into late life | Late-onset bipolar | Secondary (organic) mania |
|---|---|---|---|
| First mania/hypomania | Youth or midlife | Often after 50–60 years | Any age; temporal link to cause |
| Family history | More often positive | Less often | Variable; less specific |
| Neurology/medical load | Cumulative comorbidity with age | Higher at onset | Causal driver required |
| Exam priority | Long lithium history, renal decline, maintenance | Exclude secondary causes | Identify and treat driver |
| These contrasts are teaching constructs from critical reviews; individual patients may not fit cleanly into one column.[1][5][8] |
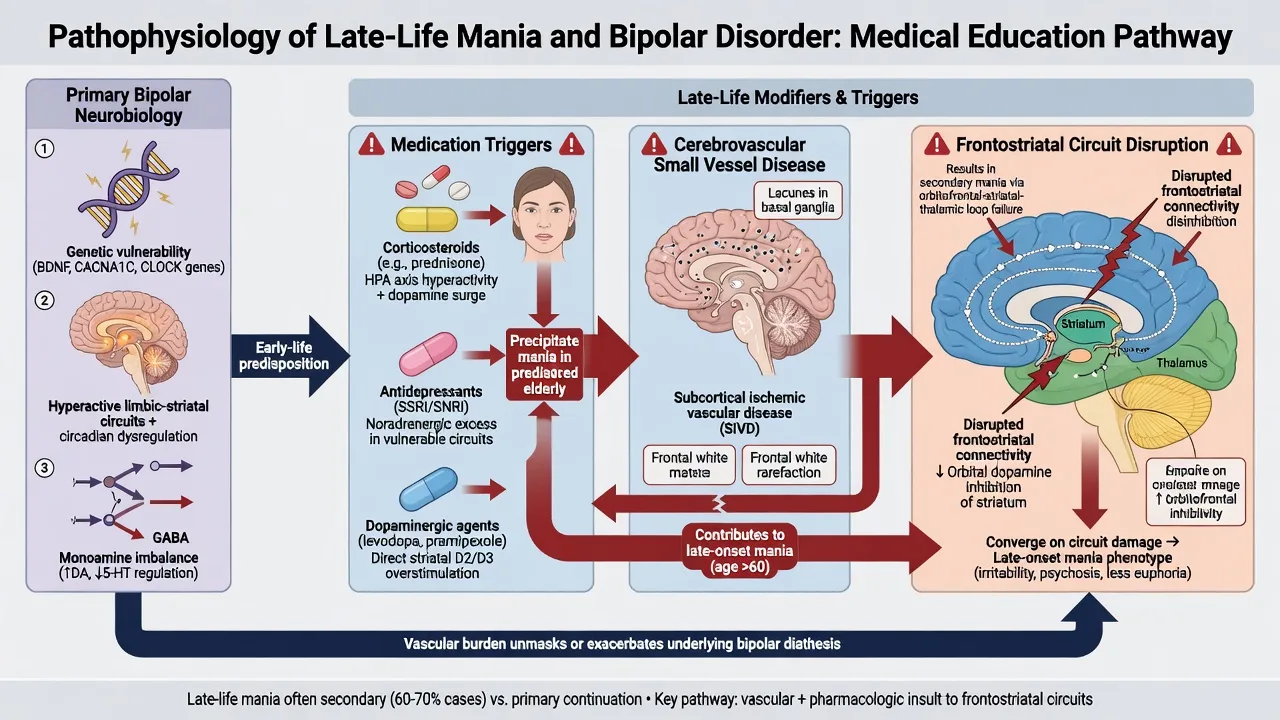
Secondary mania (Krauthammer and Klerman). Manic syndromes can follow physical illness or drugs without primary bipolar diathesis. Classic associations include corticosteroids, dopaminergic agents, stimulants, antidepressants, hyperthyroidism, stroke and other CNS lesions, infection, and space-occupying pathology. Temporal association, neurological signs, and absence of prior bipolar course raise secondary mania probability.[8]
Epidemiology, comorbidity, and suicide
Community prevalence of bipolar spectrum disorders is lower in older than younger adult samples in large surveys, but OABD remains clinically important in old-age psychiatry services and medical wards. Survivor bias, premature cardiovascular mortality, and under-recognition of hypomania shape epidemiology estimates.[1][15]
Medical comorbidity is the rule, not the exception: cardiovascular disease, metabolic syndrome, renal impairment, thyroid disease, diabetes, neurological disease, and polypharmacy cluster in elderly bipolar samples and drive agent choice and monitoring intensity.[4][5]
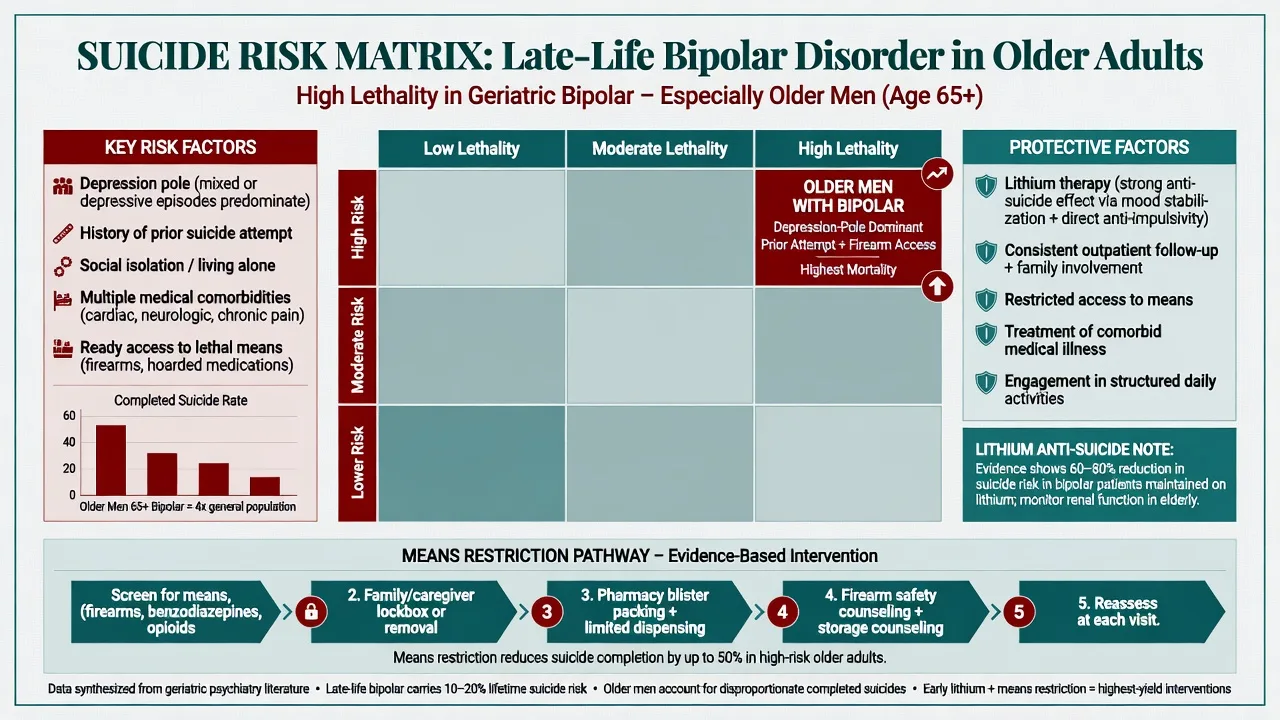
Suicide. Bipolar disorder confers elevated suicide risk across the lifespan. In older adults, attempt rates may be lower than in younger groups but completion and lethality are high, especially in older men with access to firearms or stockpiled medications. Depressive and mixed poles, prior attempts, hopelessness, isolation, alcohol, and medical pain amplify risk. Lithium has the strongest randomised and meta-analytic signal among mood agents for reducing suicide in mood disorders — a key reason not to abandon lithium solely because of age when it is still tolerated and monitored.[10][14]
Pathophysiology
Primary bipolar mechanisms (genetic loading, circadian disruption, monoaminergic and inflammatory pathways) remain relevant for EOBD surviving into late life.[15] Late-onset and secondary mania emphasise network disruption: cerebrovascular and neurodegenerative disease can disconnect frontostriatal and limbic circuits that regulate mood, sleep, and impulse control; right-hemisphere lesions are classically taught associations for secondary mania. Medication-induced monoaminergic excess (steroids, dopamine agonists, some antidepressants) provides a reversible mechanism when the drug is identified and reduced.[1][8]
Cognitive impairment in OABD is multifactorial: residual mood symptoms, cumulative illness burden, white-matter disease, and iatrogenic sedation or anticholinergic load. Treat mood aggressively while minimising cognitive toxicity and reassess cognition after stabilisation.[4][5]
Clinical presentation
Late-life mania and hypomania. Elevated, expansive, or irritable mood; decreased need for sleep; pressured speech; flight of ideas or racing thoughts; grandiosity; distractibility; increased goal-directed activity or psychomotor agitation; high-risk behaviours (spending, sexual disinhibition, dangerous driving). Older adults more often show irritability-dominant or mixed pictures, medical decompensation, and less classic euphoria than textbook young-adult mania.[1][3]
Bipolar depression. Anhedonia, low mood, anergia, psychomotor change, sleep and appetite disturbance, cognitive complaints, guilt or worthlessness, and passive or active suicidal ideation. Psychotic depression (nihilistic, guilt, or somatic delusions) raises ECT priority.[12][13]
LOBD clues. First elevation in late life, weaker family history, prominent neurological or vascular comorbidity, and concurrent medication changes should push secondary mania work-up to the front of the assessment, not the afterthought list.[1][8]
Differential diagnosis
| Discriminator | Mania (primary/secondary) | Delirium | Frontotemporal/BPSD disinhibition |
|---|---|---|---|
| Onset | Days to weeks (or drug-timed) | Hours to days | Insidious months (FTD) or context-linked (BPSD) |
| Attention/arousal | Usually clear until exhausted | Fluctuating inattention core | Often clear early |
| Mood polarity | Elevated/irritable with bipolar features | Variable; not clean bipolar package | Apathy or disinhibition without full mania package |
| Medical drivers | Secondary mania if causal link | Almost always | Dementia pathology primary |
| Time course, attention, and whether a full manic syndrome is present remain the fastest bedside discriminators.[1][8][13] |
Other differentials. Agitated unipolar depression and mixed features; substance-induced mood disorders; late-onset psychosis with secondary elevation; hyperthyroidism; stroke; CNS infection or encephalitis; space-occupying lesion; B12 deficiency; corticosteroid or L-dopa-induced states.[8][13]
Primary bipolar and secondary mania can coexist (a vulnerable bipolar brain plus a steroid trigger); treat both the episode and the precipitant.[1][8]
Assessment
History structure. Age at first depression and first mania/hypomania; number and polarity of episodes; prior lithium, valproate, antipsychotic, and antidepressant trials with levels and adverse effects; adherence; alcohol and sedatives; medical and neurological comorbidity; polypharmacy; cognitive trajectory; suicide, violence, self-neglect, and financial vulnerability; living situation and carers; elder abuse screen; driving and firearms.[1][4][13]
MSE and risk. Full manic or depressive syndrome documentation, insight, capacity for specific decisions, and a direct suicide assessment (ideation, intent, plan, means, prior attempts, protective factors). Collateral is mandatory when insight is poor.[14]
Scales. YMRS and CGI for manic severity tracking; PHQ-9/GDS in depressive poles with bipolar interpretation caveats. Scales never replace clinical risk assessment.[12]
Investigations
Baseline. FBC, U&E with creatinine/eGFR, LFT, TSH, calcium, glucose and lipids as indicated, B12/folate when cognitive change present; ECG before QT-risk antipsychotics or when cardiac disease is known; urine drug screen when indicated.[2][13]
Imaging and special tests. Strongly consider neuroimaging for late first mania/hypomania, focal neurology, atypical cognitive decline, or new neurological signs. EEG/LP when encephalitis, seizure, or autoimmune differentials are live.[1][8]
Drug-specific monitoring. Lithium: baseline renal and thyroid function, calcium, ECG; trough levels; early and then periodic renal/thyroid/calcium surveillance. Valproate: LFT, platelets, levels when used. Antipsychotics: weight, glucose, lipids, EPS, falls, QTc as indicated.[7][9][12]
Acute and emergency management
Stabilise airway/medical status, exclude delirium, secure means (medications, firearms, heights), determine intensity of care, and apply least-restrictive legal frameworks when capacity and risk demand involuntary care (jurisdiction-specific statutes — name principles and your local Act).[13][14]
Lithium toxicity. Early GI upset, coarse tremor, ataxia, dysarthria, confusion, myoclonus, seizures, and coma. Stop lithium, check urgent level and renal function, intravenous fluids as indicated, discuss dialysis for severe toxicity or very high levels with nephrology. Review interacting drugs and volume status.[9]
Definitive management
Acute mania in older adults
The GERI-BD randomised double-blind trial compared lithium and divalproex in older patients with bipolar mania and found both agents efficacious when carefully dosed and monitored — foundational exam evidence that lithium is not automatically off the table in geriatric mania.[6] Atypical antipsychotics (for example quetiapine, olanzapine, risperidone, aripiprazole) are used for acute control with start-low geriatric dosing, falls and metabolic vigilance, and caution when cerebrovascular disease or frailty is prominent.[2][3][12]
Named dosing anchors (individualise; check product information and eGFR):
| Agent | Example older-adult approach | Monitoring focus |
|---|---|---|
| Lithium carbonate | Start low (e.g. 100–300 mg orally daily or divided, titrate slowly) aiming for lower geriatric targets than young-adult acute ranges | Trough level, eGFR, TSH, calcium, ECG, interactions |
| Divalproex/valproate | Start low (e.g. 125–250 mg orally two to three times daily, titrate to response/level) | LFT, platelets, level, ammonia if encephalopathy, sedation |
| Quetiapine | Start low (e.g. 25–50 mg orally, titrate) for mania/bipolar depression per indication | Sedation, orthostasis, metabolic panel, QTc if risk |
| These are illustrative older-adult practice anchors aligned with geriatric bipolar reviews and GERI-BD-era dosing philosophy — not fixed protocols for every patient.[2][6][7][12] |
Lithium in the elderly
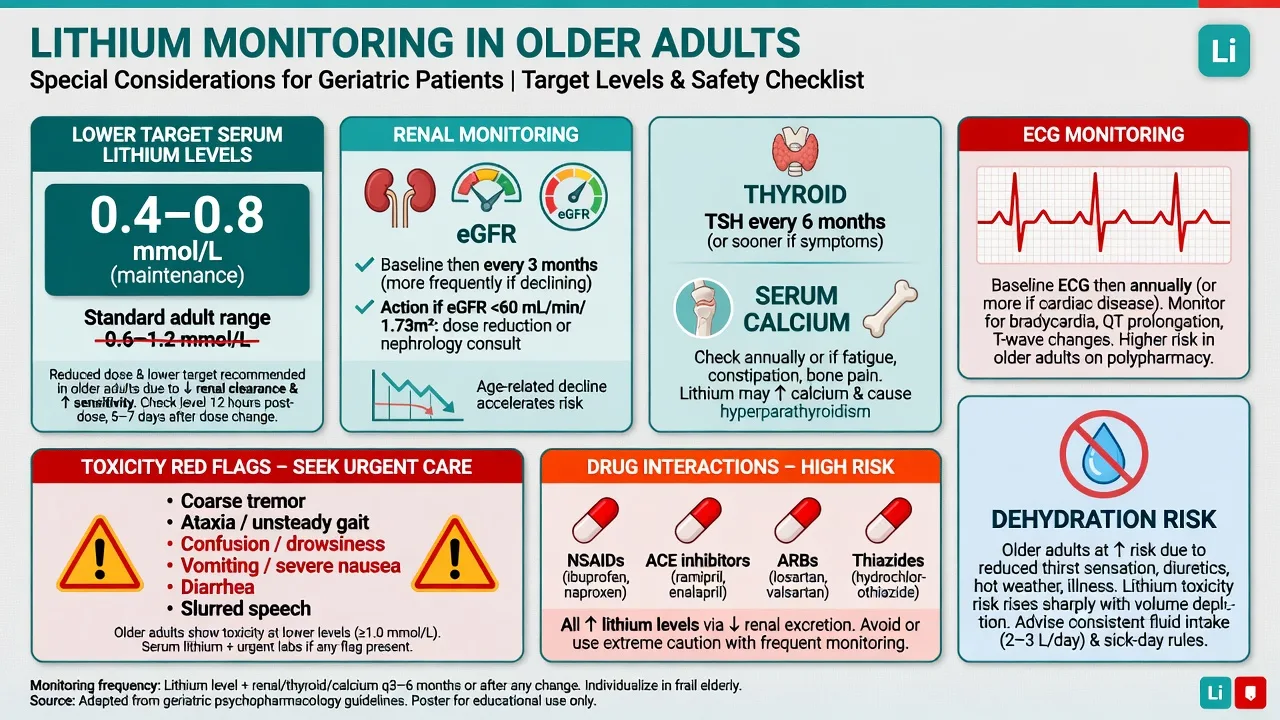
ISBD task-force Delphi consensus on maintenance lithium in older adults supports continued lithium use with age-attuned targets and monitoring rather than reflexive deprescribing solely for age.[7] Many experts target maintenance serum lithium roughly in the 0.4–0.8 mmol/L range in older adults (individualise by polarity risk, renal function, and tolerability); acute mania may briefly need higher levels under close supervision, but toxicity risk rises steeply with frailty and reduced eGFR.[2][7]
Toxicity profile. Systematic review evidence links lithium to reduced urinary concentrating ability and increased risk of hypothyroidism, hyperparathyroidism/raised calcium, and weight gain; absolute risks must be balanced against relapse and suicide prevention benefits.[9] High-risk interactions: NSAIDs, ACE inhibitors, ARBs, thiazide diuretics, dehydration, low-salt diets, and intercurrent illness. Educate patients and carers on sick-day rules and early toxicity symptoms.[7][9]
Bipolar depression
Prefer agents with bipolar depression evidence within guideline frameworks (for example quetiapine, lurasidone, lamotrigine, olanzapine–fluoxetine combination where available and appropriate), plus optimised mood stabiliser cover.[12][13][16] STEP-BD showed that adjunctive antidepressant added to a mood stabiliser was not more effective than mood stabiliser plus placebo for bipolar depression recovery overall — exam pearl: do not use antidepressant monotherapy, and use adjunctive antidepressants cautiously if at all, with switch monitoring.[17] Lithium retains anti-suicide importance in mood disorders meta-analysis.[10]
ECT
ECT is highly effective for severe depressive episodes and is used for severe mania, mixed states, catatonia, psychotic bipolar depression, life-threatening poor intake, and high acute suicide risk, as well as pharmacotherapy non-response.[18][13] Consent discussion covers anaesthetic risk, cognitive side-effects, and expected course.
Maintenance and psychosocial care
BALANCE demonstrated that lithium monotherapy and lithium–valproate combination were superior to valproate monotherapy for relapse prevention in bipolar I disorder — lithium remains a maintenance cornerstone when tolerated.[11] Apply RANZCP mood and CANMAT/ISBD bipolar guidance with older-adult pharmacokinetic adaptation; BAP guidelines similarly prioritise evidence-based long-term prophylaxis.[12][13][16]
Psychosocial pillars: psychoeducation for patient and carers, sleep regularity, alcohol reduction, adherence support, social connection, treat medical comorbidity, and coordinate aged-care and GP shared care.[3][4]
Complications and pitfalls
- Missing secondary mania and treating only as primary bipolar.[8]
- Using young-adult lithium targets without renal and frailty adjustment.[7]
- Toxicity from NSAID/ACEI/thiazide/dehydration in long-term lithium users.[9]
- Antidepressant monotherapy for bipolar depression.[17]
- Sedating polypharmacy producing falls, delirium, and aspiration.[4]
- Under-estimating suicide risk in quieter depressive poles.[14]
Prognosis and disposition
OABD is typically recurrent. Residual symptoms, non-adherence, substances, and medical multimorbidity predict poorer course. Cognitive and functional decline risk is higher than age-matched peers without bipolar illness, especially with vascular burden.[1][4][5]
Disposition ladder. Old-age community mental health teams; intensive community support; voluntary or involuntary inpatient care; ECT suite; residential aged-care liaison. Temporarily restrict driving and review finances/firearms during mania. Follow-up intensity is highest after lithium initiation or dose change and after hospital discharge.[2][13]
Special populations
Oldest-old and frail patients need the lowest effective doses and fall-focused regimens. Parkinson disease and dopaminergic therapy can precipitate mania-like states. Post-stroke mania requires neurological co-management. Intellectual disability ageing into late life needs adapted communication and carer partnership. Cultural safety and family decision styles matter for Indigenous and culturally diverse older adults.[1][4][13]
Regional guideline notes
ANZ (RANZCP). Mood disorder guidelines provide severity-based bipolar pathways, ECT indications, and medical comorbidity emphasis — primary local framework for FRANZCP practice, with geriatric dosing adaptation for OABD.[13]
Canada/international (CANMAT/ISBD). Hierarchical acute and maintenance recommendations for mania and bipolar depression; apply older-adult start-low principles and lithium monitoring consensus when treating OABD.[12][7]
UK (BAP / NICE-aligned practice). Evidence-based long-term prophylaxis, careful antidepressant use, and lithium monitoring culture map closely to exam answers for MRCPsych.[16]
US (APA practice context / ABPN). GERI-BD, STEP-BD antidepressant lessons, lithium toxicity, and suicide risk in older adults are high-yield item drivers.[6][14][17]
Exam pearls
Late-life bipolar exam checklist
This checklist compresses the high-yield OABD viva axes: secondary mania, geriatric lithium, GERI-BD, suicide, and maintenance.[6][7][8][14]
High-yield traps for MCQ/MEQ
- Treating first late-life mania as primary bipolar without imaging or drug review.[8]
- Continuing NSAIDs and thiazides without checking lithium level after a diarrhoeal illness.[9]
- Antidepressant monotherapy for an older patient with prior hypomania.[17]
- Abandoning lithium solely for age when eGFR and monitoring would allow continued prophylaxis and suicide benefit.[7][10]
- Inventing identical Mental Health Act section numbers for Australia, NZ, UK, and US in one answer.[13]
References
- [1]Depp CA, Jeste DV Bipolar disorder in older adults: a critical review Bipolar Disord, 2004.PMID 15383127
- [2]Young RC, Gyulai L, Mulsant BH, Flint A, et al. Pharmacotherapy of bipolar disorder in old age: review and recommendations Am J Geriatr Psychiatry, 2004.PMID 15249272
- [3]Sajatovic M, Madhusoodanan S, Coconcea N Managing bipolar disorder in the elderly: defining the role of the newer agents Drugs Aging, 2005.PMID 15663348
- [4]Lala SV, Sajatovic M Medical and psychiatric comorbidities among elderly individuals with bipolar disorder: a literature review J Geriatr Psychiatry Neurol, 2012.PMID 22467842
- [5]Sajatovic M, Forester BP, Gildengers A, Mulsant BH Aging changes and medical complexity in late-life bipolar disorder: emerging research findings that may help advance care Neuropsychiatry (London), 2013.PMID 24999372
- [6]Young RC, Mulsant BH, Sajatovic M, Gildengers AG, et al. GERI-BD: A Randomized Double-Blind Controlled Trial of Lithium and Divalproex in the Treatment of Mania in Older Patients With Bipolar Disorder Am J Psychiatry, 2017.PMID 29088928
- [7]Shulman KI, Almeida OP, Herrmann N, Schaffer A, et al. Delphi survey of maintenance lithium treatment in older adults with bipolar disorder: An ISBD task force report Bipolar Disord, 2019.PMID 30375703
- [8]Krauthammer C, Klerman GL Secondary mania: manic syndromes associated with antecedent physical illness or drugs Arch Gen Psychiatry, 1978.PMID 757997
- [9]McKnight RF, Adida M, Budge K, Stockton S, et al. Lithium toxicity profile: a systematic review and meta-analysis Lancet, 2012.PMID 22265699
- [10]Cipriani A, Hawton K, Stockton S, Geddes JR Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis BMJ, 2013.PMID 23814104
- [11]BALANCE investigators and collaborators, Geddes JR, Goodwin GM, et al. Lithium plus valproate combination therapy versus monotherapy for relapse prevention in bipolar I disorder (BALANCE): a randomised open-label trial Lancet, 2010.PMID 20092882
- [12]Yatham LN, Kennedy SH, Parikh SV, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder Bipolar Disord, 2018.PMID 29536616
- [13]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [14]Conwell Y, Van Orden K, Caine ED Suicide in older adults Psychiatr Clin North Am, 2011.PMID 21536168
- [15]Grande I, Berk M, Birmaher B, Vieta E Bipolar disorder Lancet, 2016.PMID 26388529
- [16]Goodwin GM, Haddad PM, Ferrier IN, et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2016.PMID 26979387
- [17]Sachs GS, Nierenberg AA, Calabrese JR, et al. Effectiveness of adjunctive antidepressant treatment for bipolar depression N Engl J Med, 2007.PMID 17392295
- [18]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045