Psych · Old age psychiatry — mood disorders
Late-life depression
Also known as Geriatric depression · Depression in older adults · Late-onset depression · Vascular depression · Depressive pseudodementia · Old-age depression
Exam-exhaustive fellowship reference on late-life depression — early- vs late-onset and vascular depression constructs; suicide risk and high lethality in older adults; depressive cognitive impairment (pseudodementia) versus dementia and delirium; medical comorbidity work-up; SSRI/SNRI dosing and safety (hyponatraemia, falls, bleeding, QTc); collaborative care (IMPACT/PROSPECT); maintenance (Reynolds); ECT (PRIDE); bereavement differential. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Late-life depression is a high-stakes old-age psychiatry examination topic. FRANZCP MEQs demand formulation of early versus late onset, vascular features, suicide risk with means restriction, a named drug with older-adult dose and monitoring, and when ECT is first-line. MRCPsych CASC stations test communication with patients and carers about antidepressants, hyponatraemia, and bereavement differentials. ABPN items test vascular depression constructs, collaborative-care evidence, and geriatric pharmacotherapy pitfalls. This topic is written so a candidate who has read nothing else can answer those questions at consultant depth.[1][5][13]
Overview and definition
Late-life depression refers to clinically significant depressive syndromes in older adults (commonly operationalised as age 60 or 65 years and older). It is not a single DSM code. It includes: (1) early-onset recurrent major depressive disorder continuing into old age; (2) late-onset first major depressive episodes; (3) clinically defined vascular depression phenotypes; and (4) depressive episodes co-occurring with cognitive impairment, medical multimorbidity, and bereavement contexts.[3][4]
DSM-5-TR. Major depressive episode criteria still apply: five or more symptoms during the same 2-week period, with depressed mood or anhedonia required as one of the five, plus distress or impairment, and exclusions for substances, medical conditions as sole explanation, and prior mania/hypomania when diagnosing unipolar MDD. Older adults may under-report mood and over-report somatic symptoms; examiners expect you to still seek affective and anhedonic anchors rather than diagnosing from fatigue alone.[4][12]
ICD-11. Depressive episode and depressive disorder use a comparable symptom menu with severity and course descriptors. State which manual you are using when duration language is examined.[12]
Classification and clinical constructs
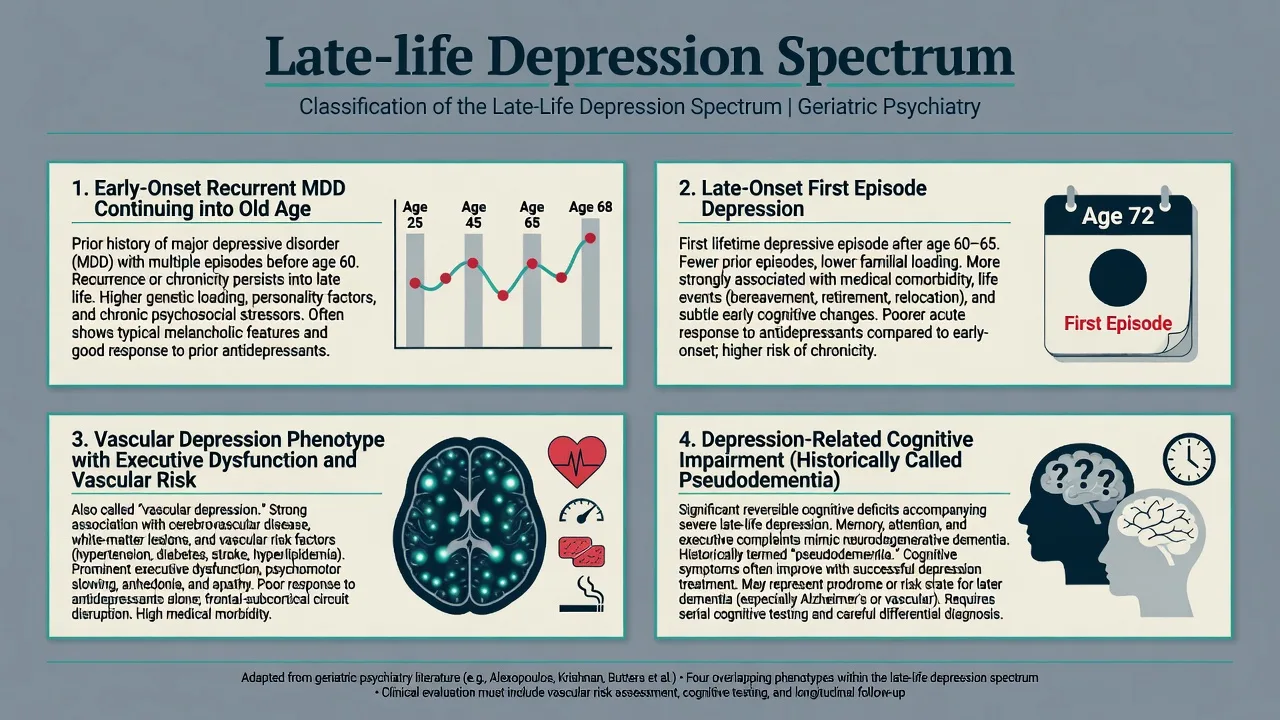
Early-onset recurrent MDD in old age. Higher likelihood of family history, prior treatment response patterns, residual dysthymic traits, and classic melancholic phenomenology in some patients. Recurrence risk after multiple episodes remains high without maintenance.[3][7]
Late-onset first episode. Often more strongly associated with medical comorbidity, cerebrovascular disease, sensory impairment, isolation, and emerging cognitive change. Always intensify organic and cognitive work-up for first late-life episodes.[1][4]
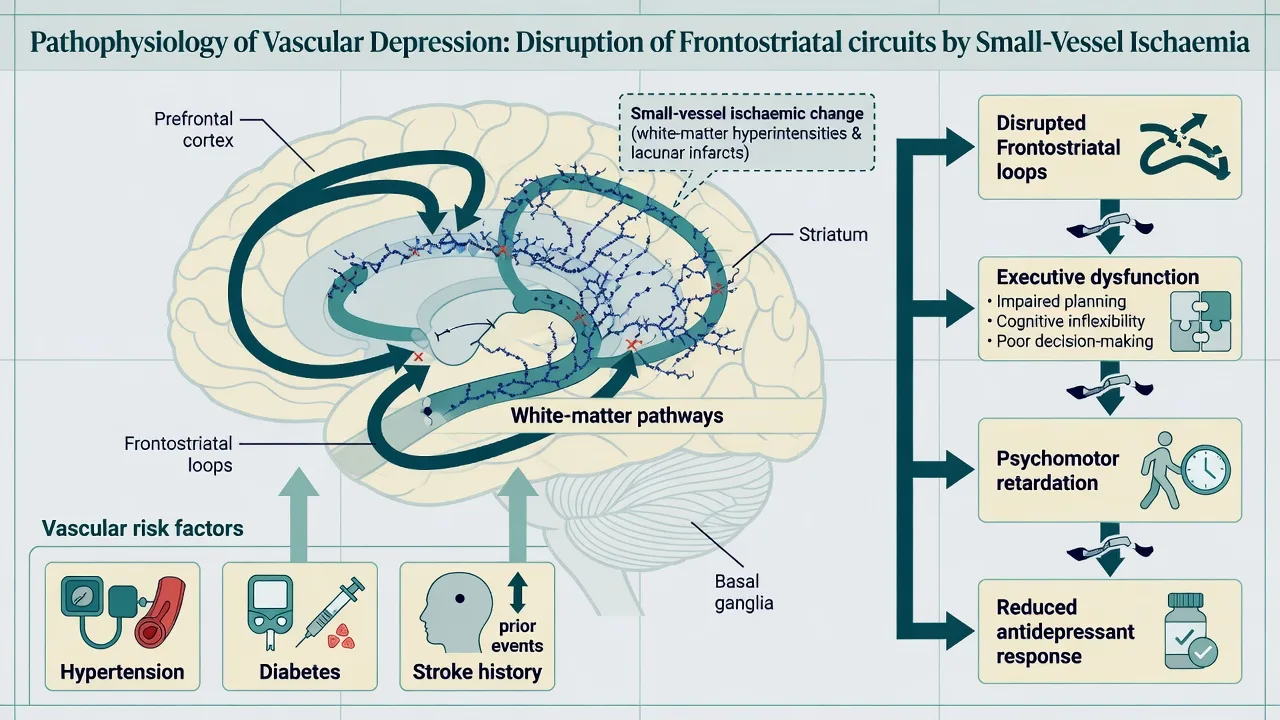
Vascular depression. A research and clinical construct (Alexopoulos), not a separate DSM diagnosis. Core idea: cerebrovascular disease contributes to late-life depression via disruption of frontostriatal and limbic circuits, producing executive dysfunction, psychomotor retardation, apathy-leaning pictures, and often poorer or slower antidepressant response. Clinically defined vascular depression emphasises vascular risk history and characteristic phenomenology; imaging may support burden of small-vessel disease but does not alone make the diagnosis.[1][2][17]
Depression-related cognitive impairment (historical "pseudodementia"). Significant cognitive deficits can accompany severe late-life depression and may partially reverse with successful treatment. Modern teaching: do not treat "pseudodementia" as fake dementia or as proof that the patient will never develop neurodegenerative disease — depression is also a risk factor/prodrome for later dementia. Treat the depression, reassess cognition after recovery, and follow longitudinally.[3][4]
Epidemiology and suicide risk
Clinically significant depressive symptoms are common in community-dwelling older adults and substantially more common in medical, hospital, and residential aged-care settings. Prevalence estimates vary by instrument and threshold; examiners care more that you know rates rise with disability, institutionalisation, and multimorbidity than that you recite a single percentage.[3][4]
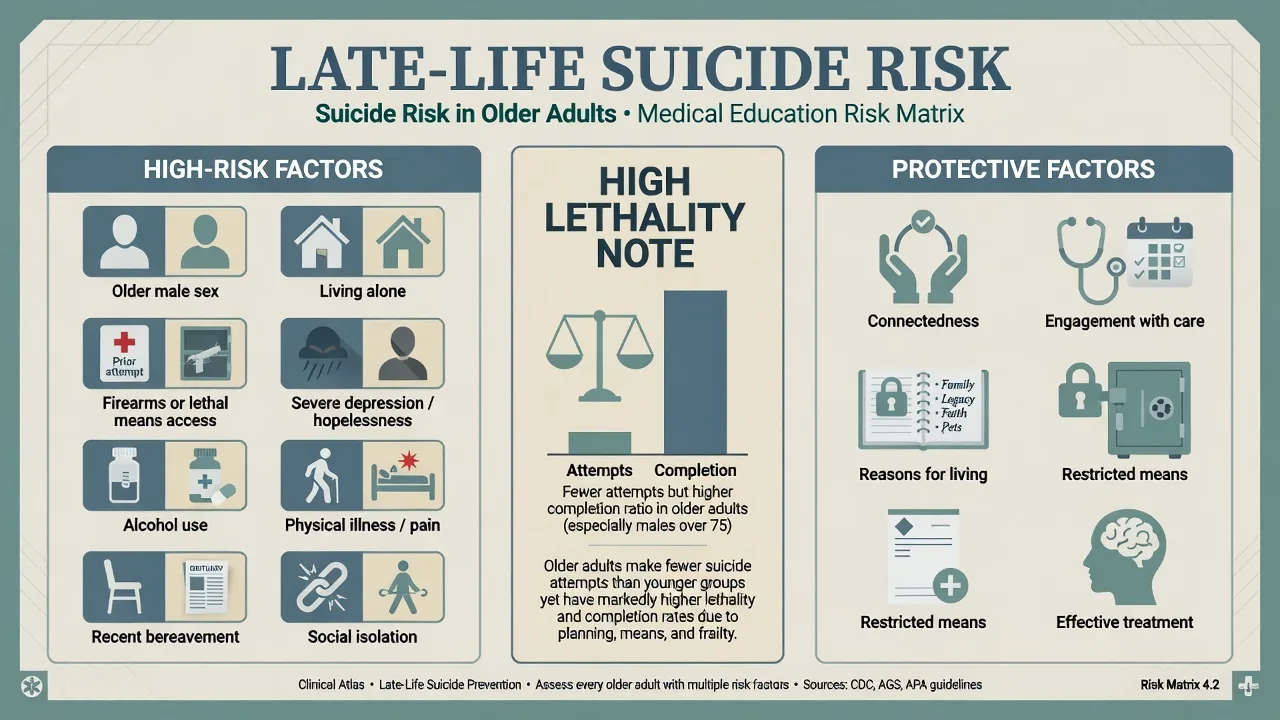
Suicide. Older adults, particularly older men, have high suicide completion rates and high lethality of methods. Risk clusters include: prior attempt, severe depression/hopelessness, living alone, bereavement, physical illness and pain, alcohol misuse, social isolation, and access to firearms or stockpiled medications. Protective factors include connectedness, engagement with care, reasons for living, restricted means, and effective treatment. Always ask directly about ideation, plan, intent, and means; under-reporting and "tired of living" language are traps.[6][13]
Landmark primary-care trials. IMPACT demonstrated that collaborative care management improved late-life depression outcomes versus usual primary care.[5] PROSPECT showed that a structured depression care algorithm in older primary-care patients reduced depressive symptoms and suicidal ideation compared with usual care.[6]
Pathophysiology
Monoamine, HPA-axis, inflammatory, and psychosocial stress models all remain relevant. In late life, the vascular contribution is the high-yield viva layer: small-vessel ischaemic change and white-matter pathway disruption can disconnect prefrontal control networks from subcortical and limbic nodes, yielding executive dysfunction and reduced treatment responsiveness. Sheline and colleagues provided prospective treatment-trial support linking vascular burden concepts to late-life depression outcomes.[1][17]
Psychological models map to therapy choice: cognitive distortions and behavioural inactivation to CBT/behavioural activation; role transitions, grief, and interpersonal deficits to IPT; problem-solving deficits to problem-solving therapy in collaborative-care models.[4][5]
Clinical presentation
Classic major depression in late life. Low mood and/or anhedonia, guilt or worthlessness, early morning waking, anorexia and weight loss, fatigue, impaired concentration, psychomotor retardation or agitation, and passive or active death wishes. Melancholic and psychotic features (nihilistic, somatic, or guilt delusions) raise ECT priority.[3][4]
Atypical older-adult presentations. Somatic preoccupation, amplified pain, irritability, anxiety, apathy-dominant pictures, and less explicit sadness. Do not miss depression because the patient "doesn't look tearful."[4]
Vascular phenotype. Prominent executive dysfunction, slowed processing, reduced initiation, apathy, and less classic guilty ruminative content; history of hypertension, diabetes, stroke, or coronary disease supports the construct.[1][2]
Bereavement interface. Acute grief includes yearning, waves of emotion, and preserved self-worth more often than pervasive worthlessness, psychomotor retardation, and suicidal intent. When major depressive criteria are met after loss — especially with marked functional collapse, psychotic guilt, or active suicidality — treat as depression while still supporting bereavement work. Do not invent outdated bereavement-exclusion myths as current absolute rules.[4][12]
Differential diagnosis
| Discriminator | Depression | Dementia | Delirium |
|---|---|---|---|
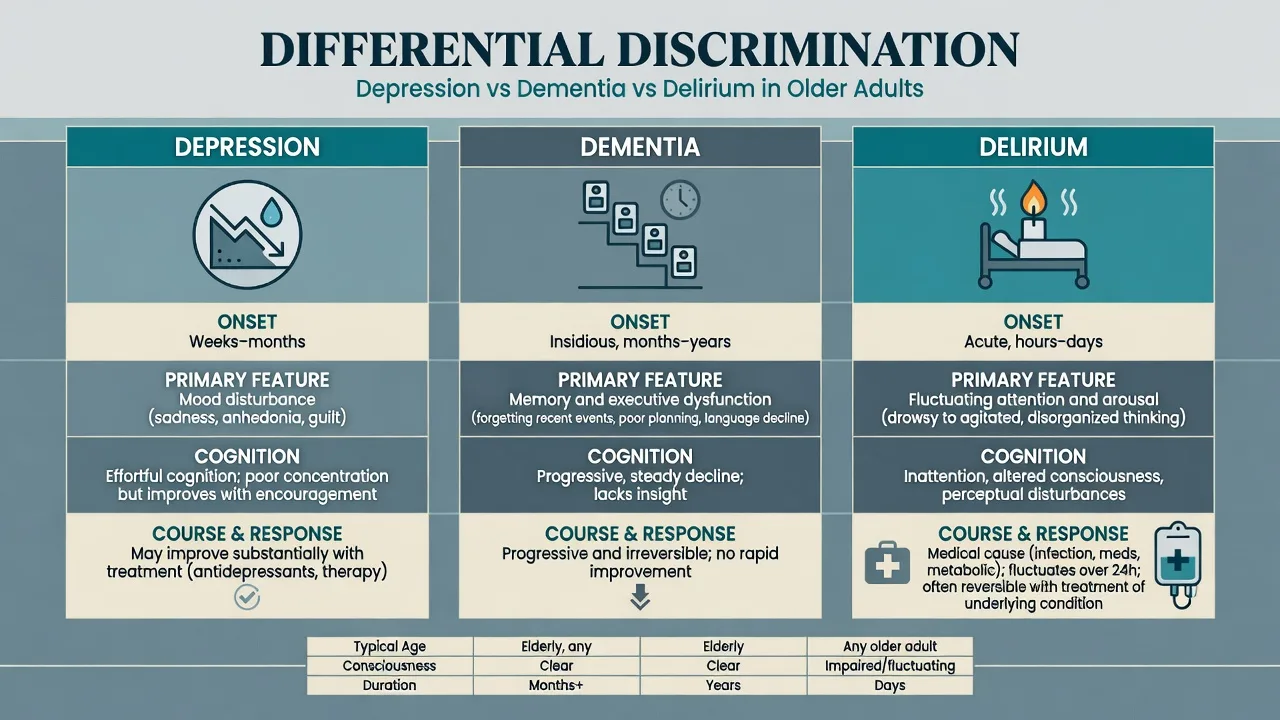
| Onset | Weeks to months | Insidious months to years | Hours to days |
| Primary domain | Mood/anhedonia | Memory/executive (type-dependent) | Attention/arousal fluctuation |
| Consciousness | Usually clear | Usually clear until advanced | Impaired/fluctuating |
| Course | May improve with treatment | Progressive without disease-modifying reversal | Tracks medical drivers |
| Time course and primary domain remain the fastest bedside discriminators between depression, dementia, and delirium in older adults.[3][4] |
Other key differentials. Bipolar depression (prior hypomania/mania, family history, mixed features); substance/medication-induced mood disorders (alcohol, benzodiazepines, steroids); medical mimics (hypothyroidism, B12 deficiency, anaemia, OSA, Parkinson disease, malignancy, heart failure, chronic pain); primary anxiety disorders; late-life psychosis with secondary dysphoria; prolonged grief disorder; elder abuse trauma presentations.[3][4][12]
Depression-related cognitive impairment and neurodegenerative dementia can be discriminated clinically but frequently coexist; treat mood fully and reassess cognition after recovery.[3][4]
Many patients have both. Treat depression fully, reassess cognition after recovery, and do not discharge cognitive concern after a single improved PHQ-9.[3][4]
Assessment
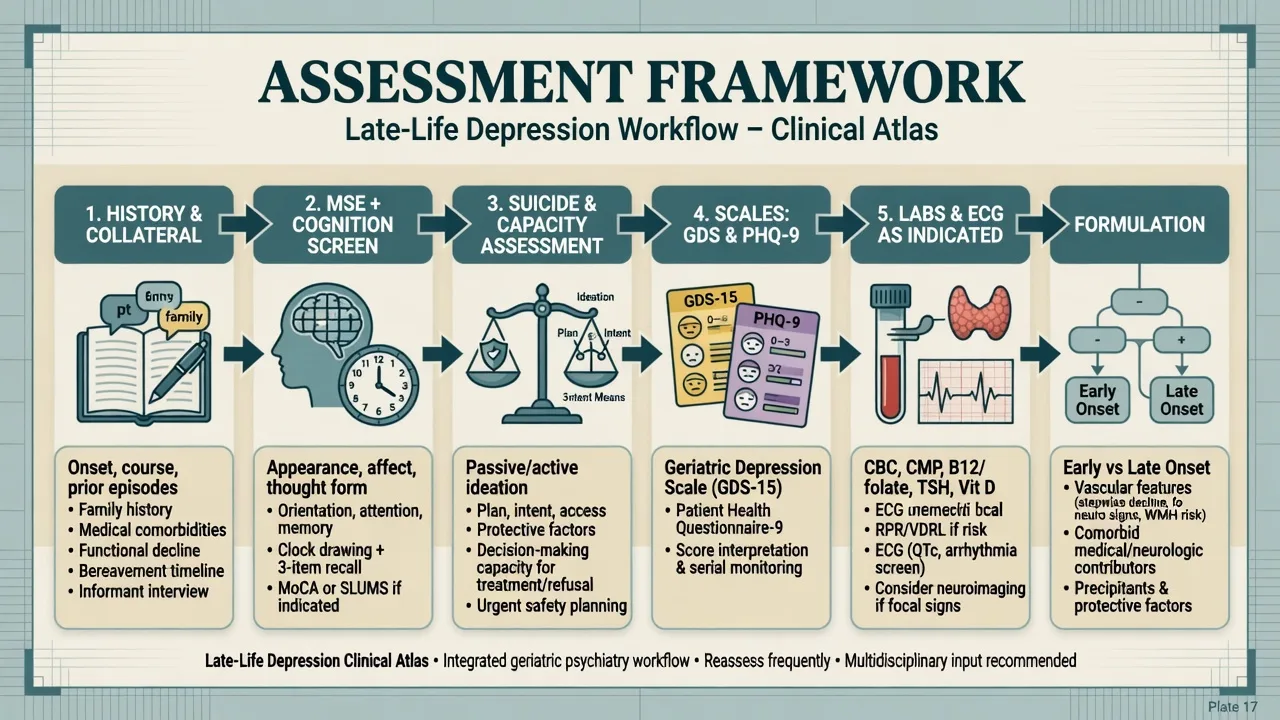
History structure. Chronology of early versus late onset; prior episode adequacy of treatment; bipolar screen; vascular risk; cognitive trajectory; bereavement and losses; living situation and isolation; alcohol and sedatives; polypharmacy and anticholinergic burden; falls; pain; elder abuse screen; functional ADLs/IADLs; carer strain.[4][12]
MSE. Affect, anhedonia language, psychomotor status, psychotic content, insight, and a full suicide risk assessment (ideation frequency, intent, plan, means, prior attempts, hopelessness, protective factors). Add bedside cognitive screening (attention, orientation, memory, clock/executive tasks). Collateral from family, GP, or aged-care staff is mandatory when under-reporting or cognitive impairment is possible.[13]
Scales. Geriatric Depression Scale (GDS) was developed specifically for older adults and reduces some somatic-item bias of younger-adult instruments.[15] PHQ-9 remains widely used for measurement-based care, including item 9 as a screen that never replaces a full risk assessment.[16] Interpret scores cautiously in marked cognitive impairment and severe medical illness.
Capacity and legal principles. Assess capacity for the specific treatment decision; use supported decision-making; invoke least-restrictive care. Mental health statutes and guardianship frameworks are jurisdiction-specific — name principles and your local Act; do not invent section numbers for other countries in the exam.[12]
Investigations
Baseline before antidepressants (individualise). FBC, U&E with sodium, LFT, TSH, B12/folate as indicated, glucose/lipids when relevant; ECG when cardiac risk factors, QT-prolonging agents, or high-risk pharmacology are planned. Consider urine drug screen, calcium, inflammatory markers, and sleep study referral when indicated by history.[4][12]
Imaging. Consider neuroimaging for late first onset with atypical features, focal neurology, stepwise cognitive decline, or unexplained executive syndrome. White-matter burden may support a vascular depression formulation but is not diagnostic in isolation.[1][17]
Measurement-based care. Serial GDS or PHQ-9 plus clinical global impression; track sodium after SSRI/SNRI initiation in frail older adults, especially with diuretics.[5][14][16]
Acute and emergency management
Manage medical emergencies of treatment as medical first: symptomatic hyponatraemia, delirium, falls with injury, serotonin toxicity, and significant bleeding on SSRI plus anticoagulant/NSAID combinations. Superimposed delirium is common in hospitals — treat drivers (infection, metabolic, medications, constipation, pain) while continuing depression planning.[4][14]
Definitive management
Collaborative care and psychotherapy
IMPACT-style collaborative care (care manager, measurement-based algorithms, stepped protocols, psychiatry supervision) outperforms usual primary care for late-life depression outcomes.[5] PROSPECT supports structured primary-care algorithms that also address suicidal ideation.[6]
Evidence-based psychotherapies adapted for older adults include CBT, interpersonal psychotherapy (IPT), behavioural activation, and problem-solving therapy. Use them alone for mild–moderate illness when appropriate, and combined with medication for moderate–severe illness or partial response.[4][12]
Pharmacotherapy principles
Second-generation antidepressants are efficacious in late-life depression, though effect sizes and response rates can be more modest than in younger adults and time to response may be longer.[10]
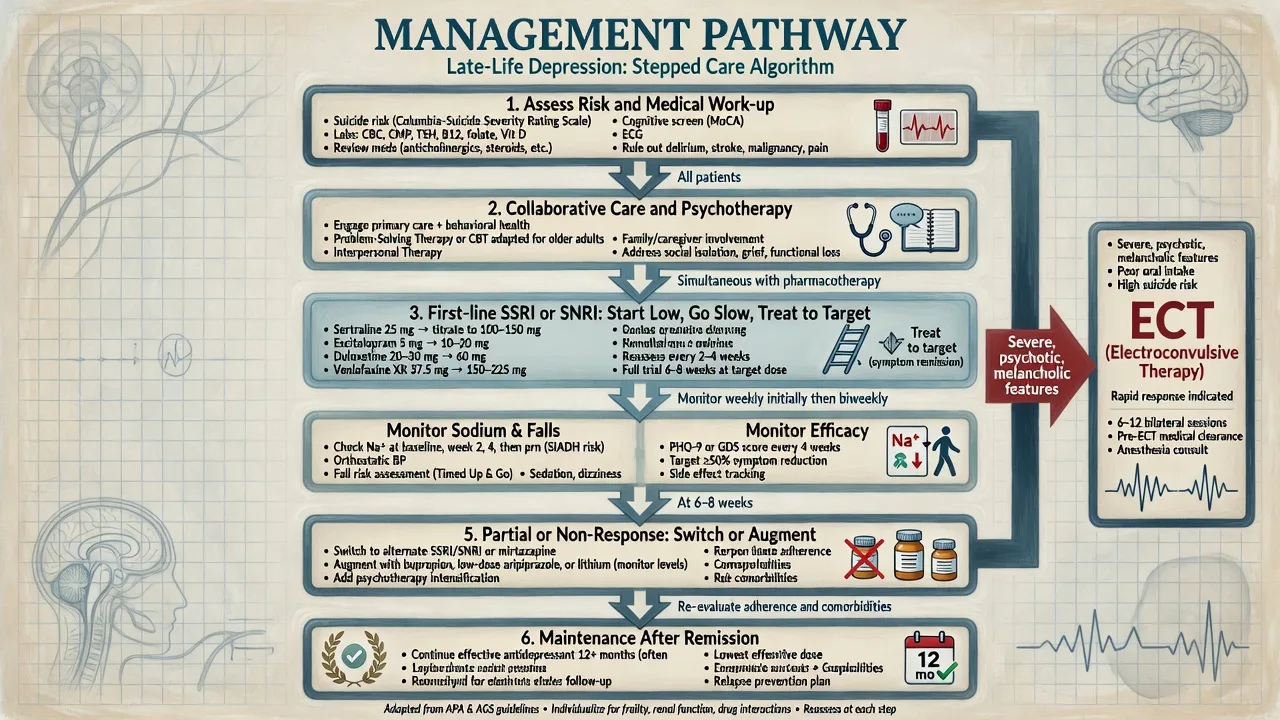
Exam mantra: start low, go slow, but go — under-dosing produces pseudo-resistance. Individualise agent choice to comorbidity, falls risk, cardiac status, and polypharmacy, guided by RANZCP mood-disorder principles and geriatric practice reviews.[4][10][12]
Named first-line examples (individualise; check local product information and comorbidity):
| Agent | Example older-adult start | Typical target range (oral daily) | Key cautions |
|---|---|---|---|
| Sertraline | 25–50 mg | 50–150 mg | GI effects; hyponatraemia; bleeding risk |
| Escitalopram | 5–10 mg | 10–20 mg | Hyponatraemia; QT considerations at higher doses/comorbidity |
| Citalopram | low start | often capped lower in older adults (product-label QT limits) | QT prolongation; prefer alternatives if cardiac risk high |
| Mirtazapine | 7.5–15 mg nocte | 15–45 mg | Sedation, weight gain — sometimes useful for insomnia/anorexia |
| Duloxetine | 30 mg | 60 mg | Nausea; avoid in significant hepatic impairment; pain comorbidity niche |
| Venlafaxine XR | 37.5–75 mg | 75–225 mg | BP rise; discontinuation symptoms; hyponatraemia |
| These starting and target ranges are illustrative older-adult practice anchors from clinical reviews and guideline-aligned prescribing; always confirm local product information and titrate to response and tolerability.[4][10][12] |
Titrate according to tolerability and response; plan an adequate trial (commonly several weeks at a therapeutic dose with adherence confirmed). Review early for activation, increased anxiety, or suicidal ideation after initiation or dose increases. Avoid first-line TCA use in frail older adults because of anticholinergic, cardiac, and overdose lethality concerns; specialist nortriptyline use with levels remains historically important in maintenance trial literature but is not a default first step for most contemporary outpatients.[4][7][10][12]
Switch vs augment. After non-response, re-check diagnosis (bipolarity, substances, medical drivers, dementia, adherence). Switch within or across class, or augment with evidence-informed strategies. Specialist options include carefully monitored lithium (renal/thyroid risk in elderly), low-dose atypical antipsychotic for selected non-psychotic TRD or for psychotic depression, and — in selected research/specialist contexts — methylphenidate combination with citalopram improved outcomes in one RCT but requires cardiac/risk scrutiny and is not a primary-care default.[12][18]
ECT
ECT is highly effective in severe depressive disorders and is often first-line for psychotic late-life depression, catatonic features, life-threatening poor intake, and high acute suicide risk, as well as for non-response to adequate pharmacotherapy.[11] The PRIDE study demonstrated robust acute response to right unilateral ultrabrief-pulse ECT combined with venlafaxine in geriatric depression, and evaluated a novel continuation strategy combining medication with additional ECT to sustain benefits.[8][9] Consent discussion covers benefits, anaesthetic/cardiac risk, cognitive side-effects, and expected course — framed as a medical procedure, not punishment or folklore.
Maintenance and social care
After remission of major depression in old age, maintenance antidepressant treatment reduces recurrence risk compared with placebo in randomised evidence (Reynolds et al., NEJM 2006).[7] Duration lengthens with number of prior episodes, residual symptoms, severity, and psychosis history. Combine with psychosocial recovery: isolation reduction, bereavement support, treat pain and sensory deficits, optimise medical comorbidity, support carers, and coordinate aged-care services.[4][12]
Safety monitoring and pitfalls
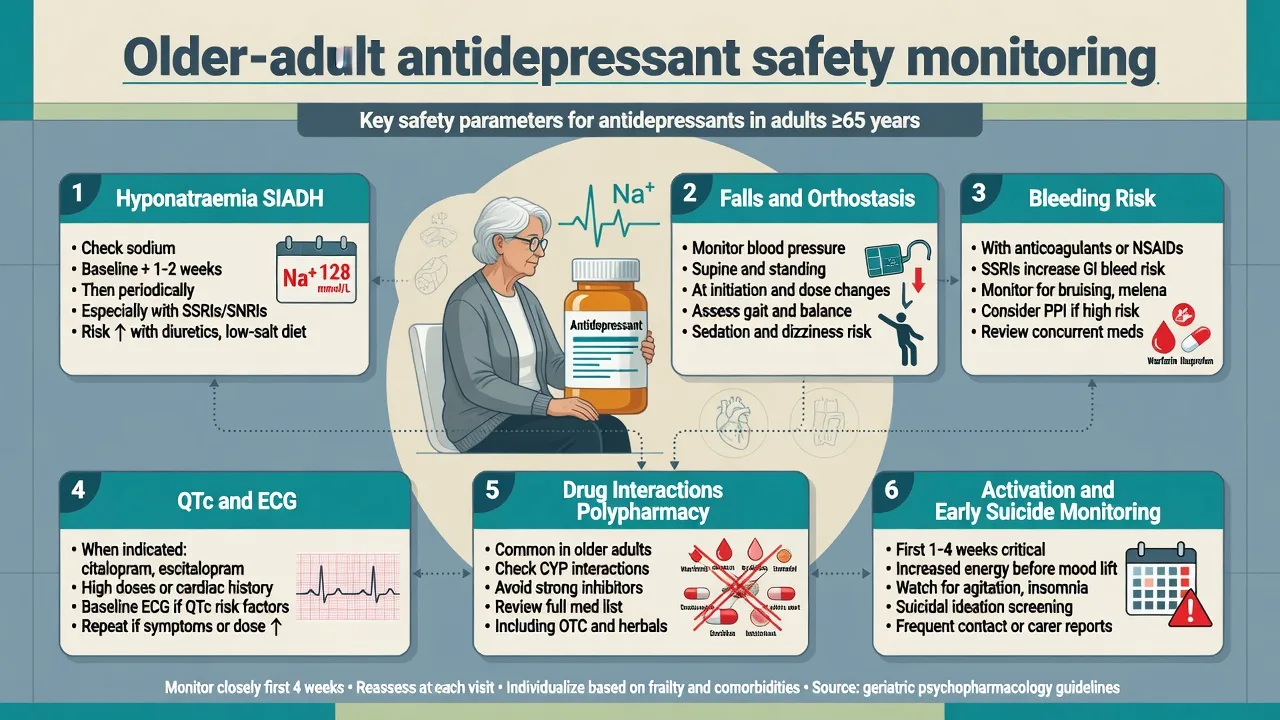
Hyponatraemia. Prospective data show paroxetine can induce clinically important hyponatraemia in older adults, typically early in treatment, often via SIADH. Check baseline sodium, recheck after initiation/dose change in high-risk patients, and educate about confusion, falls, and seizures.[14]
Other traps. Falls from sedation or orthostasis; GI bleeding risk with SSRIs plus NSAIDs/anticoagulants; QTc issues with selected agents; CYP interactions in polypharmacy; alcohol and benzodiazepine dependence; missed bipolarity; under-treatment; diagnostic overshadowing of medical illness or elder abuse.[4][12]
Prognosis and disposition
Response may be slower and residual executive symptoms more common than in midlife depression, especially with vascular burden. Residual symptoms predict relapse and functional disability. Late-life depression associates with excess medical morbidity, mortality, and cognitive decline risk — treat depression as a systemic risk factor, not a soft optional extra.[3][4][17]
Disposition ladder. Primary-care collaborative care; old-age community mental health; day programmes; residential aged-care liaison; voluntary or involuntary inpatient psychiatry; ECT suite. Follow-up intensity should be highest after treatment initiation, after discharge, and when suicidal ideation has been present.[5][6][12]
Regional guideline notes
ANZ (RANZCP). Mood disorder guidelines provide stepped care, severity-based treatment intensity, and explicit attention to older adults, medical comorbidity, and ECT indications — use them as the primary local framework in FRANZCP settings.[12]
UK (NICE). Emphasises stepped care, psychological therapies, and careful antidepressant use in older people with medical comorbidity and suicide risk monitoring, aligned with the same clinical severity ladder used internationally.[4][12]
US (APA practice context / ABPN). Collaborative care evidence (IMPACT/PROSPECT), measurement-based care, and ECT for severe late-life depression are high-yield. Product labels drive citalopram dose caps for QT risk in older adults.[5][6][11]
India (MD/DNB / NEET-SS). Same clinical constructs of late-life depression, vascular phenotype, suicide risk, and ECT thresholds apply; drug availability and family-based care structures may differ — name the agent you can actually access and monitor.[4][12]
Exam pearls
Late-life depression exam checklist
This checklist compresses the high-yield late-life depression viva axes: vascular formulation, safe pharmacotherapy, suicide lethality, cognitive differentials, and maintenance after recovery.[1][4][12][13]
High-yield traps for MCQ/MEQ
- Starting an SSRI without suicide means assessment or sodium plan in a frail diuretic-treated patient.[13][14]
- Declaring dementia on day one of severe depression without reassessing cognition after treatment.[3]
- Using ECT only after years of incomplete low-dose trials in psychotic late-life depression.[8][11]
- Stopping antidepressants the week the patient feels better after a severe late-life episode.[7]
- Inventing identical Mental Health Act section numbers for Australia, NZ, UK, and US in one answer.[12]
References
- [1]Alexopoulos GS, Meyers BS, Young RC, Campbell S, Silbersweig D, Charlson M 'Vascular depression' hypothesis Arch Gen Psychiatry, 1997.PMID 9337771
- [2]Alexopoulos GS, Meyers BS, Young RC, Kakuma T, Silbersweig D, Charlson M Clinically defined vascular depression Am J Psychiatry, 1997.PMID 9090349
- [3]Alexopoulos GS Depression in the elderly Lancet, 2005.PMID 15936426
- [4]Taylor WD Clinical practice. Depression in the elderly N Engl J Med, 2014.PMID 25251617
- [5]Unützer J, Katon W, Callahan CM, Williams JW Jr, Hunkeler E, Harpole L, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial JAMA, 2002.PMID 12472325
- [6]Bruce ML, Ten Have TR, Reynolds CF 3rd, Katz II, Schulberg HC, Mulsant BH, et al. Reducing suicidal ideation and depressive symptoms in depressed older primary care patients: a randomized controlled trial JAMA, 2004.PMID 14996777
- [7]Reynolds CF 3rd, Dew MA, Pollock BG, Mulsant BH, Frank E, Miller MD, et al. Maintenance treatment of major depression in old age N Engl J Med, 2006.PMID 16540613
- [8]Kellner CH, Husain MM, Knapp RG, McCall WV, Petrides G, Rudorfer MV, et al. Right Unilateral Ultrabrief Pulse ECT in Geriatric Depression: Phase 1 of the PRIDE Study Am J Psychiatry, 2016.PMID 27418379
- [9]Kellner CH, Husain MM, Knapp RG, McCall WV, Petrides G, Rudorfer MV, et al. A Novel Strategy for Continuation ECT in Geriatric Depression: Phase 2 of the PRIDE Study Am J Psychiatry, 2016.PMID 27418381
- [10]Nelson JC, Delucchi K, Schneider LS Efficacy of second generation antidepressants in late-life depression: a meta-analysis of the evidence Am J Geriatr Psychiatry, 2008.PMID 18591576
- [11]UK ECT Review Group Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis Lancet, 2003.PMID 12642045
- [12]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [13]Conwell Y, Van Orden K, Caine ED Suicide in older adults Psychiatr Clin North Am, 2011.PMID 21536168
- [14]Fabian TJ, Amico JA, Kroboth PD, Mulsant BH, Corey SE, Begley AE, et al. Paroxetine-induced hyponatremia in older adults: a 12-week prospective study Arch Intern Med, 2004.PMID 14769630
- [15]Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey M, et al. Development and validation of a geriatric depression screening scale: a preliminary report J Psychiatr Res, 1982.PMID 7183759
- [16]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [17]Sheline YI, Pieper CF, Barch DM, Welsh-Bohmer K, McKinstry RC, MacFall JR, et al. Support for the vascular depression hypothesis in late-life depression: results of a 2-site, prospective, antidepressant treatment trial Arch Gen Psychiatry, 2010.PMID 20194828
- [18]Lavretsky H, Reinlieb M, St Cyr N, Siddarth P, Ercoli LM, Senturk D Citalopram, methylphenidate, or their combination in geriatric depression: a randomized, double-blind, placebo-controlled trial Am J Psychiatry, 2015.PMID 25677354