Psych · Old age psychiatry — psychosis
Late-onset psychosis
Also known as Very late-onset schizophrenia-like psychosis · VLOSLP · Late-onset schizophrenia · Late paraphrenia · Late-life psychosis · Geriatric psychosis
Exam-exhaustive fellowship reference on late-onset and very late-onset schizophrenia-like psychosis (LOS/VLOSLP) — Howard consensus age cut-offs; phenomenology including partition delusions; organic work-up and neuroimaging; differentials of dementia (including DLB), delirium, and affective psychosis; sensory impairment; antipsychotic start-low-go-slow with dementia mortality/stroke cautions; RANZCP and NICE framing. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Why this topic matters in exams
Old-age stations reward candidates who do not treat first late-life psychosis like young adult first-episode schizophrenia. Examiners probe: age cut-offs and nosology, partition delusions, sensory impairment, organic work-up including imaging, dementia/DLB traps, and whether you can name a safe geriatric antipsychotic start with monitoring and a review date.[2][4][5]
Definition and classification
Clinical problem. Psychotic symptoms (delusions, hallucinations, disorganised behaviour/thought when present) beginning for the first time in later life, after careful exclusion or concurrent evaluation of competing causes.[3][8]
Howard 2000 international consensus (must-know). The International Late-Onset Schizophrenia Group recommended:
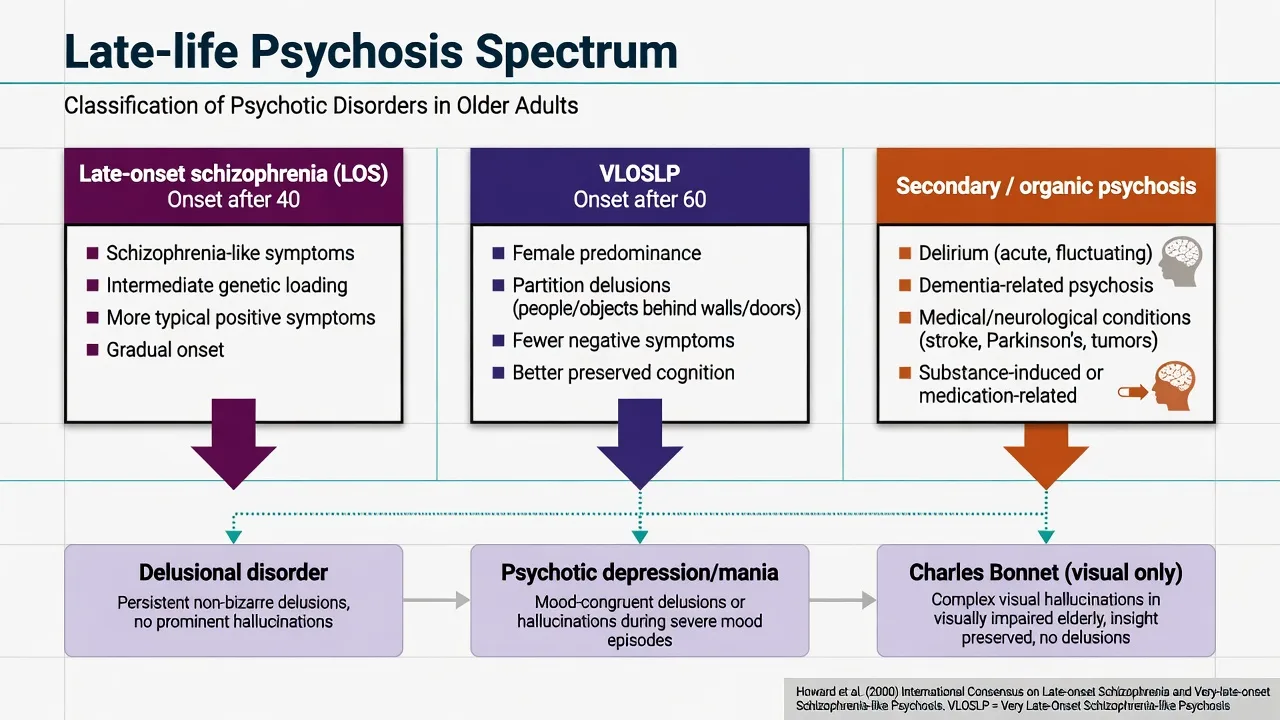
- Late-onset schizophrenia (LOS): onset after age 40
- Very-late-onset schizophrenia-like psychosis (VLOSLP): onset after age 60
These are research and clinical descriptors. They are not freestanding DSM-5-TR or ICD-11 diagnoses. In coding practice you still map to schizophrenia, delusional disorder, other specified schizophrenia spectrum disorder, or psychotic disorder due to another medical condition as the evidence dictates.[1]
Historical note. Late paraphrenia described older adults (often women) with prominent persecutory delusions and hallucinations, relatively preserved personality, and less formal thought disorder than classic early-onset schizophrenia. Modern LOS/VLOSLP literature largely absorbs this teaching.[9]
DSM-5-TR / ICD-11 application. Apply standard schizophrenia-spectrum criteria when met. Late age at onset does not create a separate code, but atypical age is an organic red flag. ICD-11 allows course and severity descriptors; always document medical and substance contributors when present.[5]
Epidemiology and risk
First-onset schizophrenia-spectrum illness is less common after midlife than in adolescence and early adulthood, but late first presentations are clinically important and exam-favoured because of high organic yield and treatment hazard.[2][3]
Associations repeatedly described in LOS/VLOSLP series:
- Female predominance (especially VLOSLP)
- Social isolation and living alone
- Sensory impairment (hearing more than vision in classic schizophrenia-like late psychosis literature)
- Premorbid schizoid, paranoid, or avoidant traits in a subset
- Lower genetic loading and fewer negative symptoms than early-onset schizophrenia in many comparisons
- Medical multimorbidity and cerebrovascular risk factors
Dementia risk signal. VLOSLP is associated in systematic review with higher rates of cognitive impairment and subsequent dementia diagnosis than age-matched non-psychotic populations — enough to mandate longitudinal cognitive surveillance, not enough to equate every VLOSLP case with prodromal dementia on day one.[6] A subset may represent prodromal dementia with Lewy bodies or other neurodegenerative disease; watch for core DLB features over time.[7]
Mechanisms (exam-level, not speculative fluff)
No single pathway explains all late first-onset psychosis. Useful frameworks for viva:
- Neurodevelopmental residual vulnerability unmasked by ageing, sensory loss, or social isolation (closer to LOS)
- Neurodegenerative / cerebrovascular contribution (closer to some VLOSLP and mixed pictures)
- Sensory deprivation and misattribution amplifying persecutory content
- Medical, toxic, and medication triggers producing secondary psychosis
Dopamine-blocking antipsychotics can still reduce positive symptoms in primary LOS/VLOSLP even when etiology is multi-factorial — response does not prove idiopathic schizophrenia.[3][8][11]
Clinical presentation and MSE
Classic VLOSLP teaching phenotype
- Persecutory and referential delusions (neighbours, landlords, conspiracy)
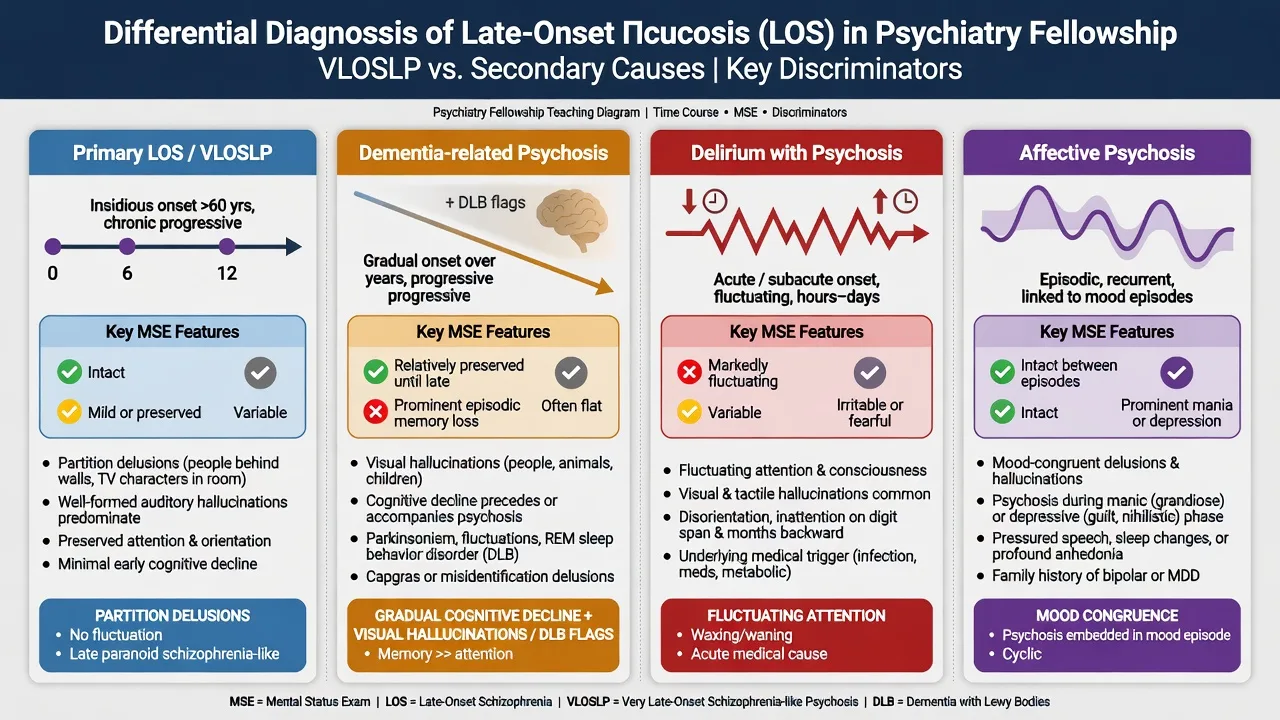
- Partition delusions — belief that people, gases, electricity, or rays pass through walls, floors, or ceilings (high-yield)
- Third-person auditory hallucinations; visual hallucinations more often reported than in young adult schizophrenia in some series
- Relatively preserved affective warmth and less formal thought disorder / negative symptom burden than early-onset schizophrenia
- Functional impact via self-neglect, service refusal, neighbour conflict, police contact
LOS (onset 40–60) often looks more classically schizophrenia-like than pure delusional disorder, with intermediate negative-symptom and genetic loading relative to early-onset illness.[1][2]
Do not miss: Concurrent depression or anxiety without assuming primary affective psychosis; hearing impairment maintaining misinterpretation of environmental noise; capacity issues for treatment, finances, and residence.[4][8][10]
Differential diagnosis (discriminators, not lists)
| Competing diagnosis | Fast discriminators |
|---|---|
| Delirium | Hours–days, fluctuating attention/arousal, medical driver |
| Alzheimer / vascular dementia psychosis | Progressive cognitive decline preceding or outpacing psychosis; functional cognitive trajectory |
| Dementia with Lewy bodies | Fluctuation, recurrent well-formed visual hallucinations, RBD, spontaneous parkinsonism; neuroleptic sensitivity |
| Psychotic depression / mania | Mood congruence, neurovegetative cluster, bipolar history |
| Delusional disorder | Non-bizarre, often mono-thematic; functioning outside delusional system relatively preserved |
| Charles Bonnet | Isolated visual hallucinations with ocular disease, insight often partial, no multi-modal psychosis |
| Substance / medication | Steroids, dopamine agonists, anticholinergics, stimulants, alcohol/benzodiazepine withdrawal |
| Other medical | CNS lesion, epilepsy, infection, autoimmune encephalitis, endocrine/metabolic |
Assessment
History structure. Exact age at first psychotic symptom; prior psychiatric illness (including untreated midlife prodrome); substance use; medications (especially dopamine agonists, steroids, anticholinergics); sensory deficits; social network; forensic/police contacts; weapons/fire risk; elder abuse and exploitation; driving.[4][8]
MSE. Delusional content and systematisation; hallucination modality; thought form; affect; insight/judgment; cognition with attention, orientation, memory, and executive probes. Collateral is mandatory when insight is poor.[4][8]
Risk. Harm to others driven by persecution; self-neglect; suicide; fire; financial abuse; wandering. Preserved affect does not equal low risk.[3][5]
Capacity. Treatment, residence, and finances — supported decision-making first; jurisdiction-specific guardianship/mental health statutes when incapacitous and high risk (name the principle, do not invent section numbers across countries).[4][16]
Scales. BPRS/PANSS for symptom tracking; MoCA/MMSE as screens, not dementia diagnoses during untreated psychosis.[4][6]
Investigations — organic work-up
First late-onset psychosis is an investigation-heavy presentation.[3][4]
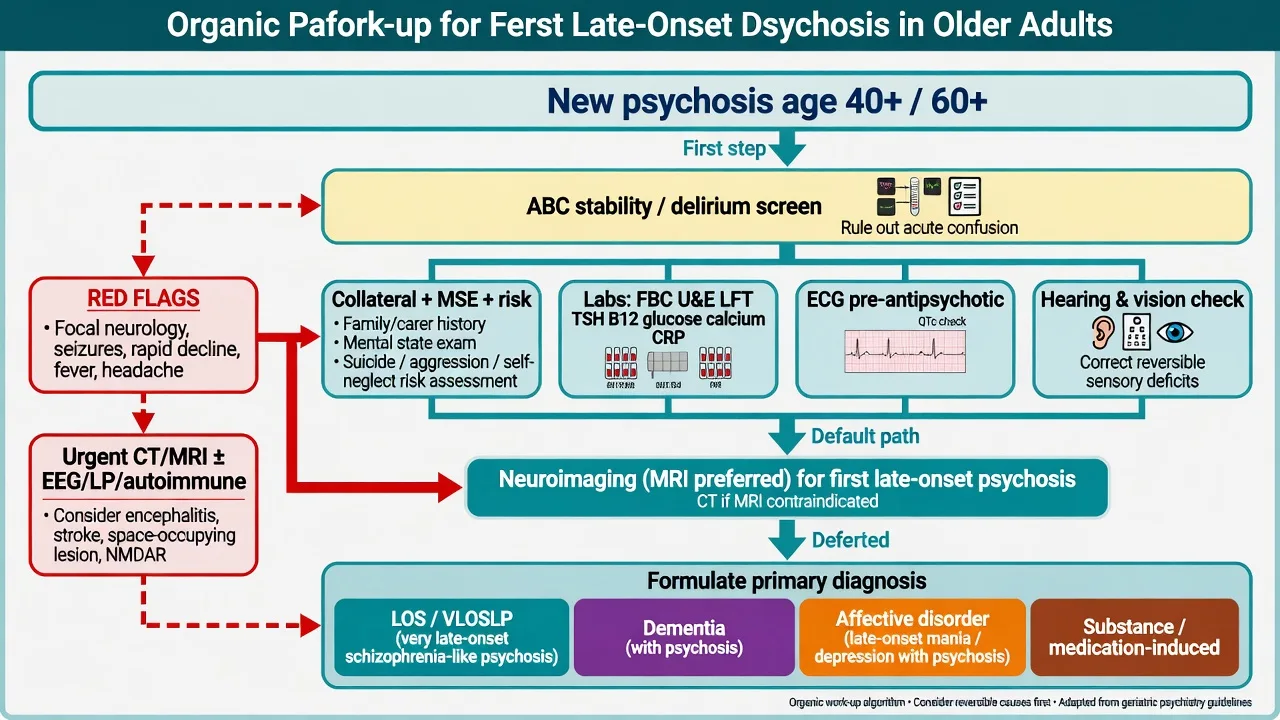
Baseline almost always: FBC, U&E, LFT, glucose, lipids, TSH, B12/folate, calcium; CRP/ESR when systemic disease suspected; urine drug screen when indicated; ECG before antipsychotic (QTc, conduction) given sudden cardiac death association with antipsychotics in population studies; formal hearing and vision assessment.[4][10][18]
Neuroimaging. For first psychotic presentation in later life, brain imaging (MRI preferred when feasible; CT if MRI unavailable/urgent) is standard teaching because structural and vascular yields matter and missing a lesion is an exam fail. Escalate urgency for focal neurology, seizures, rapid decline, severe headache, immunosuppression, or fever.[3][4]
Extended: EEG if seizures/fluctuating consciousness; LP and autoimmune encephalitis panel when indicated; more detailed cognitive battery after acute psychosis settles.[3][4]
Acute / emergency management
- Safety and legal status — least restrictive setting that contains risk; involuntary principles when high risk and incapacitous (jurisdiction-specific).
- Medical exclusion — delirium and life-threatening organic disease first.
- De-escalation before medication when possible.
- Medication for acute agitation — age-reduced doses; avoid stacking multiple sedatives; extreme caution if DLB suspected (prefer non-drug measures and specialist advice; avoid first-generation high-potency agents).
- Safeguarding — self-neglect, elder abuse, fire, weapons.
Watch for NMS, severe EPS, falls, aspiration, and anticholinergic delirium after chemical restraint.[15][18]
Definitive management
Non-pharmacological (always document)
- Psychoeducation for patient and carers
- Hearing aids / vision correction / environmental noise reduction
- Reduce isolation; structured day supports
- CBT for psychosis adapted to older adults where available and cognitive ability allows
- Mediate neighbour/housing conflict via social work when safe
- Address sleep, pain, constipation, and other physical maintainers
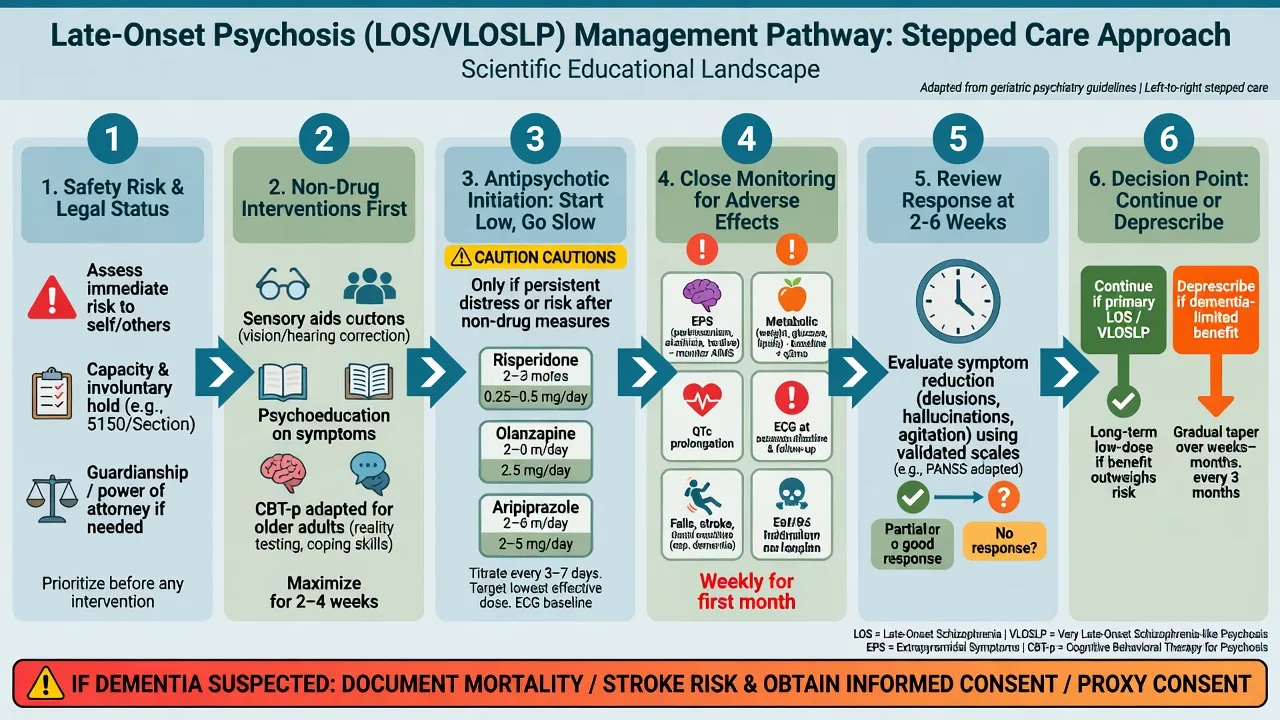
Antipsychotics — primary LOS/VLOSLP
Evidence is thinner than for young adult schizophrenia, but clinical series support second-generation antipsychotics at low–moderate doses with meaningful response rates in VLOSLP.[11] Apply adult schizophrenia guideline principles (RANZCP / NICE) with geriatric dose adjustment and physical health monitoring.[16][17]
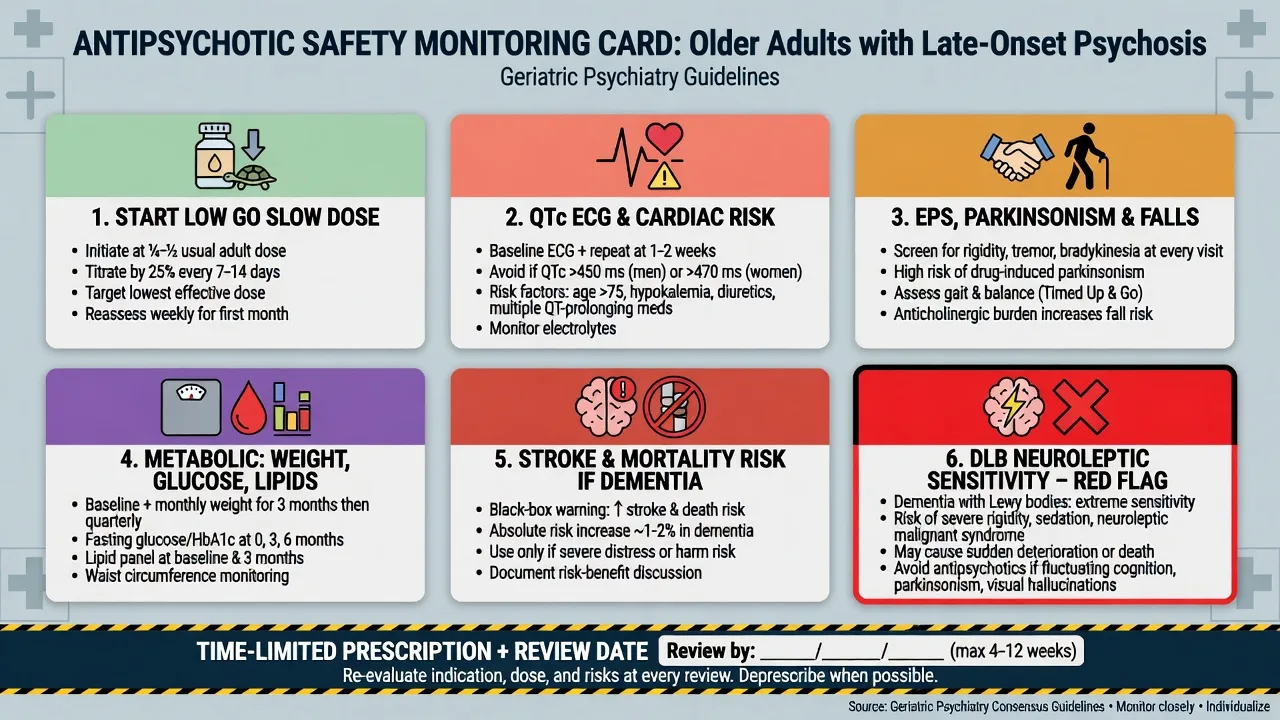
Principles: start low, go slow, lowest effective dose, oral preferred, single agent, written review date, metabolic + EPS + falls monitoring.[11][16]
Named starting examples (oral; individualise; check local formulary and product information): Age-adjusted low starting doses and slow titration are standard for VLOSLP-type illness after organic work-up — risperidone 0.25–0.5 mg daily (EPS and prolactin caution); olanzapine 2.5 mg daily (metabolic, sedation, falls); aripiprazole 2–5 mg daily (akathisia; sometimes better metabolic profile); quetiapine low dose only with caution (sedation, orthostasis, QTc; weak antipsychotic potency at very low doses) — reassess benefit and harm at each review.[11][16]
Avoid high-potency first-generation agents as first-line in frail older adults, especially if DLB is on the differential. Clozapine and ECT are specialist refractory pathways with age-adjusted monitoring — not routine first steps.[7][15][16]
When dementia is possible or confirmed
This is a different risk calculus. Meta-analysis shows increased mortality with atypical antipsychotics in dementia versus placebo; efficacy is modest and adverse effects include cerebrovascular events, sedation, and EPS.[12][13] CATIE-AD effectiveness data show limited overall benefit and trade-offs in Alzheimer disease neuropsychiatric symptoms.[14] ACNP guidance emphasises cautious, targeted, time-limited use.[15]
Document: target symptom, non-drug measures tried, dose, consent/capacity discussion including stroke/mortality risk, and deprescribing plan. Prefer non-antipsychotic strategies for mild distress; for severe risk, short specialist-supervised trials may still be justified.[12][15]
Population data also link atypical antipsychotics with sudden cardiac death risk — ECG and cardiac history are not optional theatre.[18]
Subtypes and scenarios
- LOS 40–60: FEP-style psychosocial package with physical health monitoring and lower expectation of classic neurodevelopmental deficit profile.[1]
- VLOSLP with partition delusions + deafness: classic old-age psychiatry viva stem — fix hearing, reduce isolation, low-dose antipsychotic, risk to neighbours.[9][10]
- Possible prodromal DLB: longitudinal follow-up; avoid typical antipsychotics.[7]
- Residential aged care: multi-professional plan; avoid sedating polypharmacy.[5][15]
- Charles Bonnet: ophthalmology pathway; do not escalate antipsychotics for isolated visual phenomena with insight and ocular disease.[3][8]
- Police/neighbour conflict: risk formulation and legal interface, not insight lectures alone.[3][5]
Complications and pitfalls
Missing delirium or structural brain disease; missing DLB and precipitating catastrophic neuroleptic sensitivity; long-term high-dose antipsychotics for dementia psychosis without review; ignoring sensory impairment; premature permanent dementia diagnosis during untreated psychosis; underestimating violence/self-neglect because the patient is "pleasant"; metabolic syndrome, falls, stroke, and death — especially in frail and demented patients.[7][10][12][15]
Prognosis and disposition
Many patients with primary LOS/VLOSLP improve on low–moderate antipsychotic doses, though residual delusions are common.[11] Cognitive course is heterogeneous: some remain stable; a clinically important minority progress to dementia and need surveillance.[6] Disposition balances risk, supports, insight, and medical frailty — community old-age psychiatry, inpatient admission, or residential care.
Regional guideline notes
ANZ (primary). Apply RANZCP schizophrenia and related disorders guidance for schizophrenia-spectrum care, then age-adjust doses, physical health checks, and recovery-oriented supports. Late first onset still needs full medical work-up; dementia pathways and antipsychotic cautions apply when neurocognitive disorder is the driver.[16]
UK. NICE adult psychosis/schizophrenia principles (psychological and pharmacological care, physical health) remain relevant for primary schizophrenia-like illness; dementia antipsychotic restrictions and primary-care physical health monitoring culture are examinable alongside.[17]
US / global boards. ABPN-style items emphasise organic differentials, DLB caution, FDA boxed-warning style mortality framing in dementia, and ECG/metabolic monitoring.[12][15][18]
Exam pearls
One-page revision checklist
- Define LOS (more than 40) and VLOSLP (more than 60) as Howard constructs, not DSM codes.[1]
- List partition delusions, female predominance, isolation, sensory impairment.[9][10]
- Discriminate delirium, AD/vascular psychosis, DLB, affective psychosis, Charles Bonnet, substances.[3][7]
- Write the organic work-up including MRI/CT and ECG.[4][18]
- Name a low-dose antipsychotic start, monitoring, and review date.[11][16]
- State Schneider mortality meta-analysis implication when dementia is present.[12]
- Plan cognitive follow-up because of elevated dementia risk in VLOSLP cohorts.[6]
References
- [1]Howard R, Rabins PV, Seeman MV, Jeste DV Late-onset schizophrenia and very-late-onset schizophrenia-like psychosis: an international consensus. The International Late-Onset Schizophrenia Group Am J Psychiatry, 2000.PMID 10671383
- [2]Suen YN, Wong SMY, Hui CLM, Chan SKW, et al. Late-onset psychosis and very-late-onset-schizophrenia-like-psychosis: an updated systematic review Int Rev Psychiatry, 2019.PMID 31599177
- [3]Devanand DP, Jeste DV, Stroup TS, Goldberg TE Overview of late-onset psychoses Int Psychogeriatr, 2024.PMID 36866576
- [4]Kim K, Jeon HJ, Myung W, Suh SW, et al. Clinical Approaches to Late-Onset Psychosis J Pers Med, 2022.PMID 35330384
- [5]Fischer CE, Namasivayam A, Crawford-Holland L, Hakobyan N, et al. Psychotic Disorders in the Elderly: Diagnosis, Epidemiology, and Treatment Psychiatr Clin North Am, 2022.PMID 36396273
- [6]Yang VX, Sin Fai Lam CC, Kane JPM Cognitive impairment and development of dementia in very late-onset schizophrenia-like psychosis: a systematic review Ir J Psychol Med, 2023.PMID 34187604
- [7]Kanemoto H, Satake Y, Suehiro T, Taomoto D, et al. Characteristics of very late-onset schizophrenia-like psychosis as prodromal dementia with Lewy bodies: a cross-sectional study Alzheimers Res Ther, 2022.PMID 36138485
- [8]Colijn MA, Nitta BH, Grossberg GT Psychosis in Later Life: A Review and Update Harv Rev Psychiatry, 2015.PMID 26332218
- [9]Howard R, Almeida O, Levy R Phenomenology, demography and diagnosis in late paraphrenia Psychol Med, 1994.PMID 8084935
- [10]Prager S, Jeste DV Sensory impairment in late-life schizophrenia Schizophr Bull, 1993.PMID 8303225
- [11]Scott J, Greenwald BS, Kramer E, Shuwall M Atypical (second generation) antipsychotic treatment response in very late-onset schizophrenia-like psychosis Int Psychogeriatr, 2011.PMID 21118614
- [12]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [13]Schneider LS, Dagerman K, Insel PS Efficacy and adverse effects of atypical antipsychotics for dementia: meta-analysis of randomized, placebo-controlled trials Am J Geriatr Psychiatry, 2006.PMID 16505124
- [14]Sultzer DL, Davis SM, Tariot PN, Dagerman KS, et al. Clinical symptom responses to atypical antipsychotic medications in Alzheimer's disease: phase 1 outcomes from the CATIE-AD effectiveness trial Am J Psychiatry, 2008.PMID 18519523
- [15]Jeste DV, Blazer D, Casey D, Meeks T, et al. ACNP White Paper: update on use of antipsychotic drugs in elderly persons with dementia Neuropsychopharmacology, 2008.PMID 17637610
- [16]Castle DJ, Galletly CA, Dark F, Humberstone V, et al. The 2016 Royal Australian and New Zealand College of Psychiatrists guidelines for the management of schizophrenia and related disorders Med J Aust, 2017.PMID 28918734
- [17]Kuipers E, Yesufu-Udechuku A, Taylor C, Kendall T Management of psychosis and schizophrenia in adults: summary of updated NICE guidance BMJ, 2014.PMID 24523363
- [18]Ray WA, Chung CP, Murray KT, Hall K, et al. Atypical antipsychotic drugs and the risk of sudden cardiac death N Engl J Med, 2009.PMID 19144938