Psych · Old age psychiatry — psychotropic prescribing
Prescribing psychotropics in older adults
Also known as Geriatric psychopharmacology · Psychotropics in the elderly · Beers criteria psychotropics · STOPP START psychiatry · Start low go slow · Antipsychotics black box dementia · Geriatric prescribing safety
Exam-exhaustive fellowship reference on prescribing psychotropics in older adults — age-related PK/PD, Beers and STOPP/START, start-low-go-slow-but-go, antipsychotic mortality/stroke black-box in dementia, QTc, falls, SIADH, anticholinergic burden, class-specific dosing and monitoring, deprescribing. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
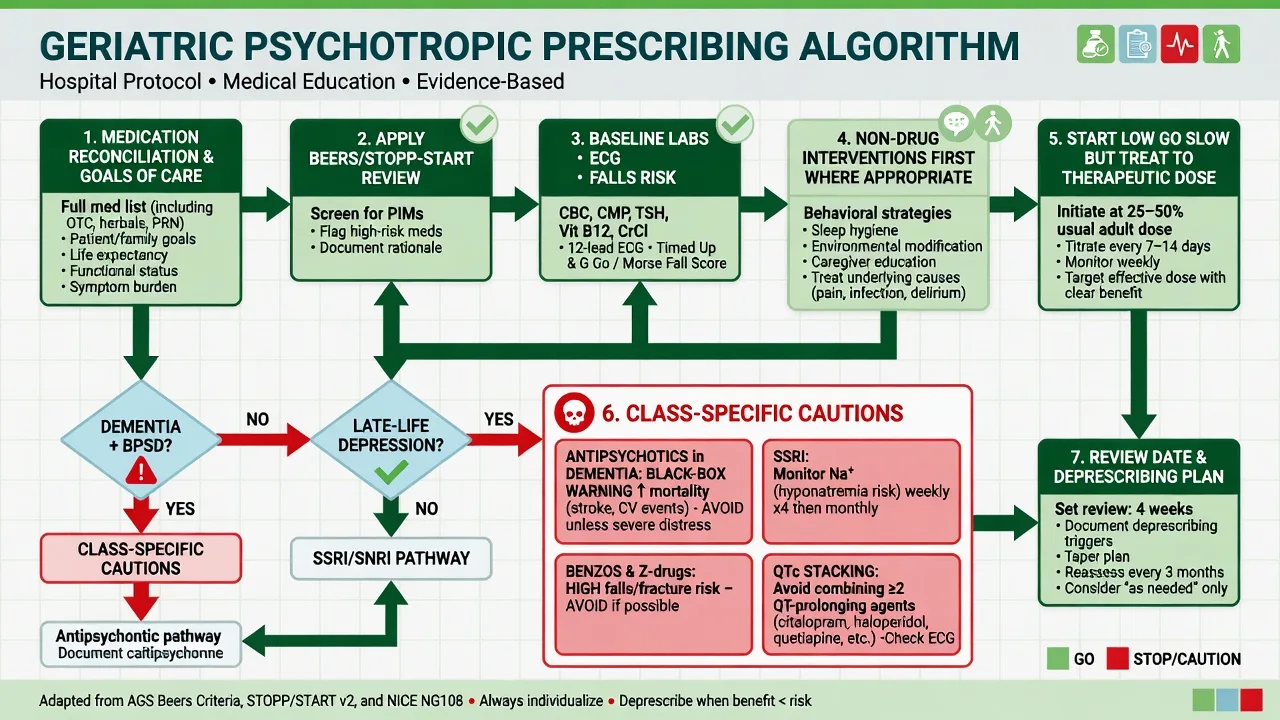
Fellowship viva language is concrete: named PIMs, age-related clearance, illustrative start doses with monitoring, black-box framing for antipsychotics in dementia, and the classic fail of under-treating late-life depression while oversedating behaviour.[1][5][20]
Definition and classification
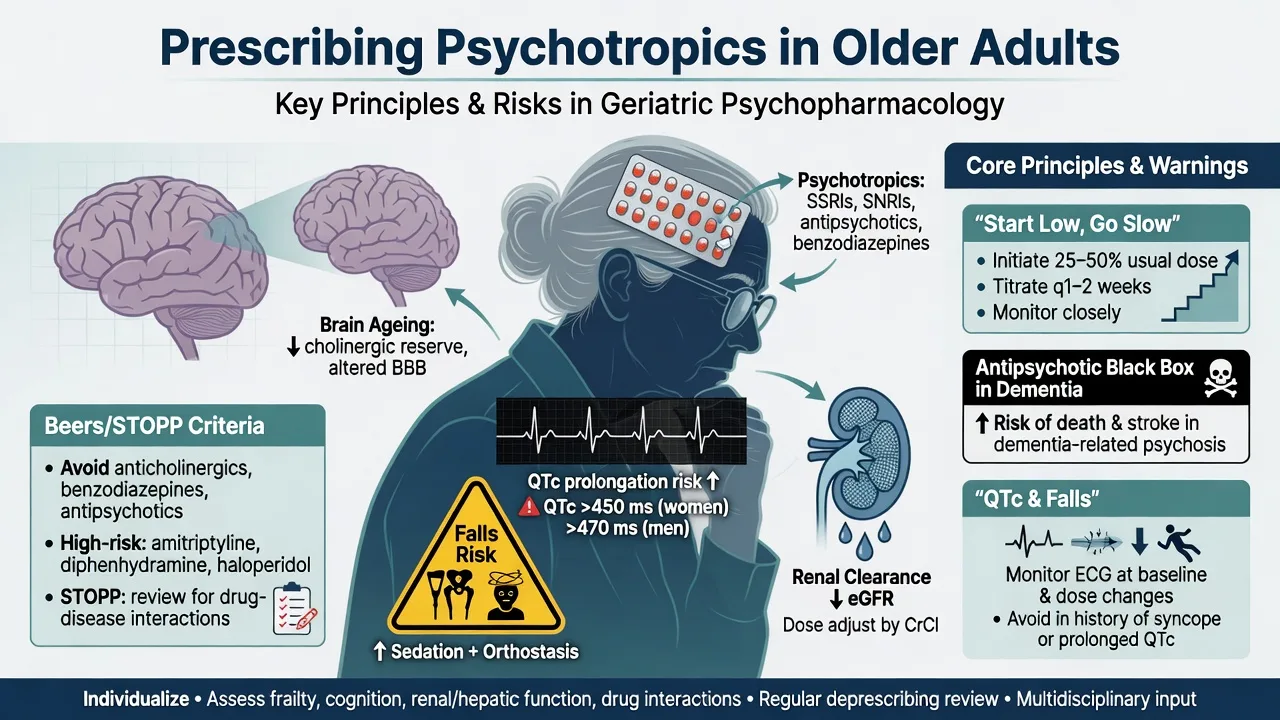
Geriatric psychotropic prescribing is the application of psychopharmacology to older adults (commonly 65 years and over, or clinically frail younger people) where multimorbidity, polypharmacy, reduced physiological reserve, and goals-of-care framing change the risk–benefit equation for every agent.[1]
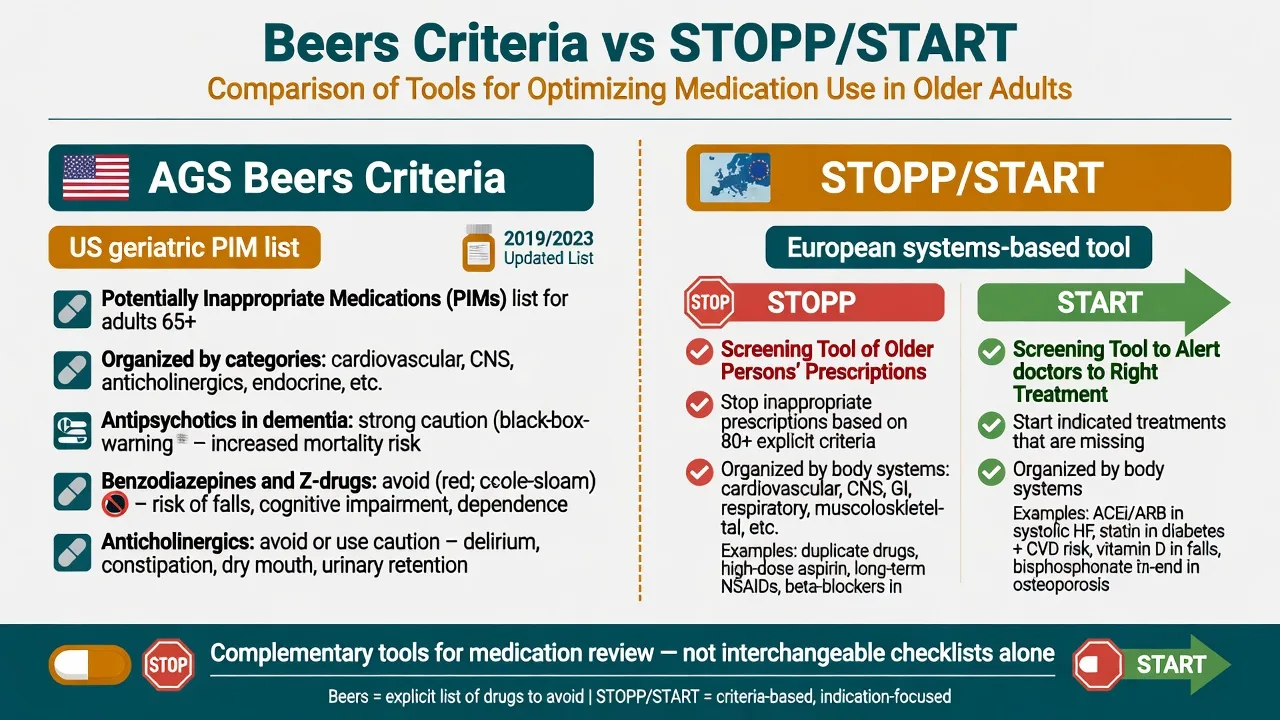
Potentially inappropriate medications (PIMs) are drugs where risk usually outweighs benefit in older adults for a given indication or context. Two complementary frameworks dominate exams.[2][3][4]
| Framework | Origin / logic | Exam use |
|---|---|---|
| AGS Beers Criteria | US expert consensus lists of PIMs, drug–disease interactions, and drugs to use with caution | Name class-level avoids (benzodiazepines, many anticholinergics, antipsychotics in dementia except limited scenarios) |
| STOPP | Screening Tool of Older Person's Prescriptions — systems-based stop rules | Find what to stop (e.g. long-term benzodiazepines, duplicative CNS drugs) |
| START | Screening Tool to Alert to Right Treatment | Find what is missing (under-treatment is also unsafe) |
| Evidence anchors | AGS Beers updates; STOPP/START v2 (O'Mahony) | Use both as medication-review scaffolds |
Risk clusters examiners use. Antipsychotics in dementia; benzodiazepines and Z-drugs; TCAs and strong anticholinergics; high-QTc agents and QT stacking; lithium with falling GFR; sedating polypharmacy (any combination of sedating antidepressant + antipsychotic + benzo + opioid).[2][15][18]
Epidemiology and risk
Polypharmacy and PIM use are common in community and residential aged care. Psychotropic exposure associates with falls, fractures, delirium, hospitalisation, and — for antipsychotics in dementia — increased mortality and cerebrovascular events in trial meta-analysis and observational cohorts.[5][7][8][18]
Headline risk anchors for viva recall
Risk amplifiers. Frailty, prior falls, dementia (especially DLB for neuroleptic sensitivity), renal impairment, diuretics (SIADH and volume issues), cardiac disease and electrolyte depletion (QTc/TdP), CYP inhibitors, female sex for some hyponatraemia signals, residential care PRN culture, and stacked CNS-active drugs.[1][15][16]
Pathophysiology — age-related PK/PD
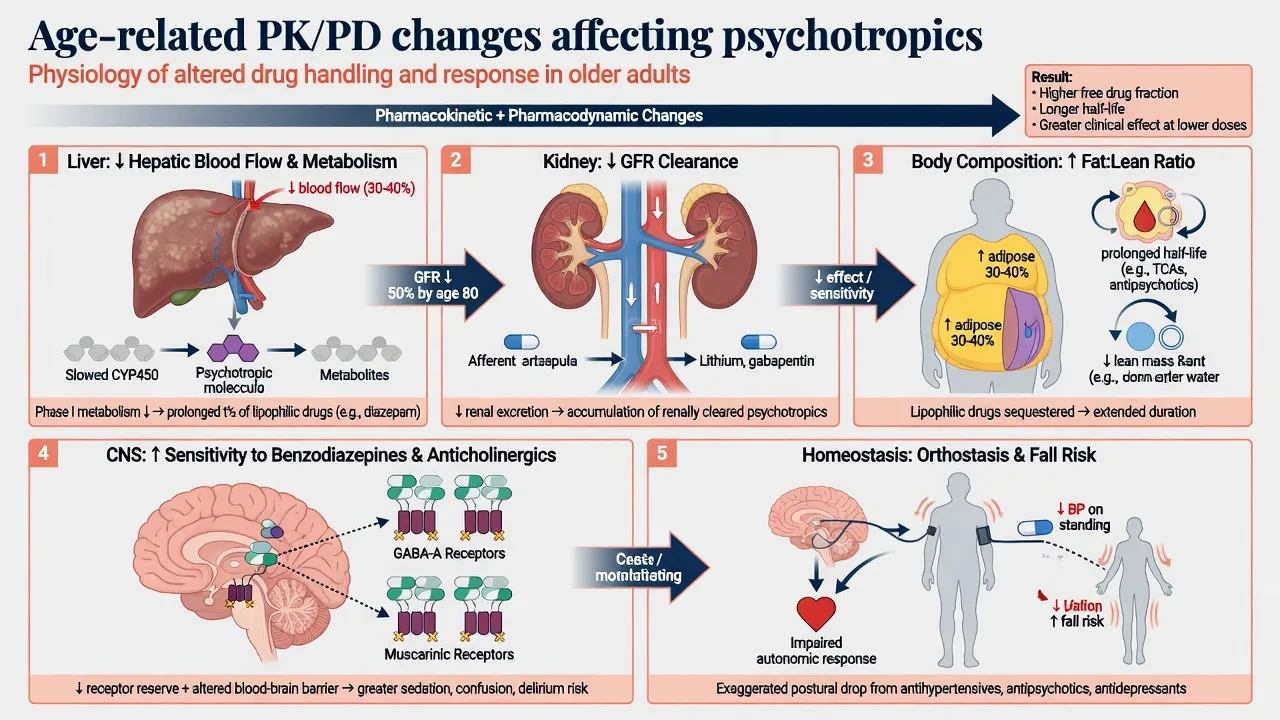
Mangoni and Jackson summarise the practical physiology examiners want — ageing changes both pharmacokinetics and pharmacodynamics in ways that reshape psychotropic risk.[1]
Pharmacokinetics. Reduced hepatic blood flow and phase I capacity; reduced first-pass extraction for some drugs; declining GFR reducing renally cleared drug and metabolite clearance; increased fat:lean ratio prolonging half-life of lipophilic agents (many psychotropics); lower albumin potentially increasing free fraction of highly protein-bound drugs in acute illness.[1]
Pharmacodynamics. Greater CNS sensitivity to GABA-A positive allosteric modulators and anticholinergics; impaired baroreflex and orthostatic tolerance; reduced thermoregulatory and cognitive reserve so sedation becomes delirium and a missed step becomes a hip fracture.[1][17]
Antipsychotic harm in dementia. Meta-analysis of RCTs shows increased risk of death with atypical antipsychotics versus placebo in dementia; observational data extend the mortality signal; risperidone dementia trials signalled higher cerebrovascular events — the regulatory and exam black-box teaching is a class-level caution, not a single-brand curiosity.[5][7][8]
QTc and sudden death. Many antipsychotics and some antidepressants prolong QTc via potassium-channel effects; population data link atypical antipsychotics to sudden cardiac death risk; clinical risk multiplies with dose, co-drugs, bradycardia, female sex, and low K/Mg.[12][13][14][15]
Clinical presentation of iatrogenic harm
Think drug toxicity as a differential for every new fall, confusion, or "behaviour change".[1][18]
- Sedation / falls: benzodiazepines, Z-drugs, antipsychotics, sedating antidepressants, antihistamines.[17][18]
- Anticholinergic toxidrome spectrum: dry mouth, constipation, urinary retention, blurred vision, delirium, tachycardia — TCAs, oxybutynin-class agents, some antipsychotics, many OTC cold remedies.[2]
- EPS / parkinsonism / akathisia: especially first-generation antipsychotics and high-D2 atypicals; akathisia is often misread as primary agitation and treated with more antipsychotic — a classic fail.[6][19]
- Hyponatraemia: headache, nausea, confusion, falls, seizures after SSRI/SNRI start.[16]
- Cardiac: orthostasis, syncope, documented QTc prolongation.[13][15]
Opposite error: the quiet, under-dosed late-life depression patient who is "not on much" but still suicidal — start low, stay low is not geriatric excellence.[20]
Differential diagnosis when a new psychotropic is considered
Delirium
- Acute fluctuating inattention
- Medical driver almost always
- Do not label pure delirium as BPSD alone
- Review meds as cause and solution
BPSD / NPS
- Domain-specific (agitation, psychosis, apathy)
- DICE/ABC first
- Pain and environment common drivers
- Drug only for severe risk
Primary mood / psychosis
- Late-life MDD, bipolar, late-onset psychosis
- Treat to therapeutic intensity
- Avoid under-treatment
- Still use geriatric safety monitoring
Iatrogenic
- Akathisia, anticholinergic delirium
- Benzo withdrawal agitation
- Hyponatraemia, QTc syncope
- Fix the drug list before adding more
Bedside assessment and medication review
- Full reconciliation — prescribed, PRN residential care stock, OTC anticholinergics, alcohol, opioids, herbal agents.[2][4]
- Indication audit — does each psychotropic have a current target symptom and response?
- Beers + STOPP thinking — list PIMs; apply START so under-treatment (e.g. untreated severe depression) is not missed.[2][4]
- Frailty and falls — orthostatic BP, gait, prior fractures, visual impairment, footwear and environment.[18]
- Capacity and shared decisions — substitute decision-maker discussion for dementia antipsychotic risk–benefit; jurisdiction-specific statutes for involuntary care (do not invent section numbers).[5][20]
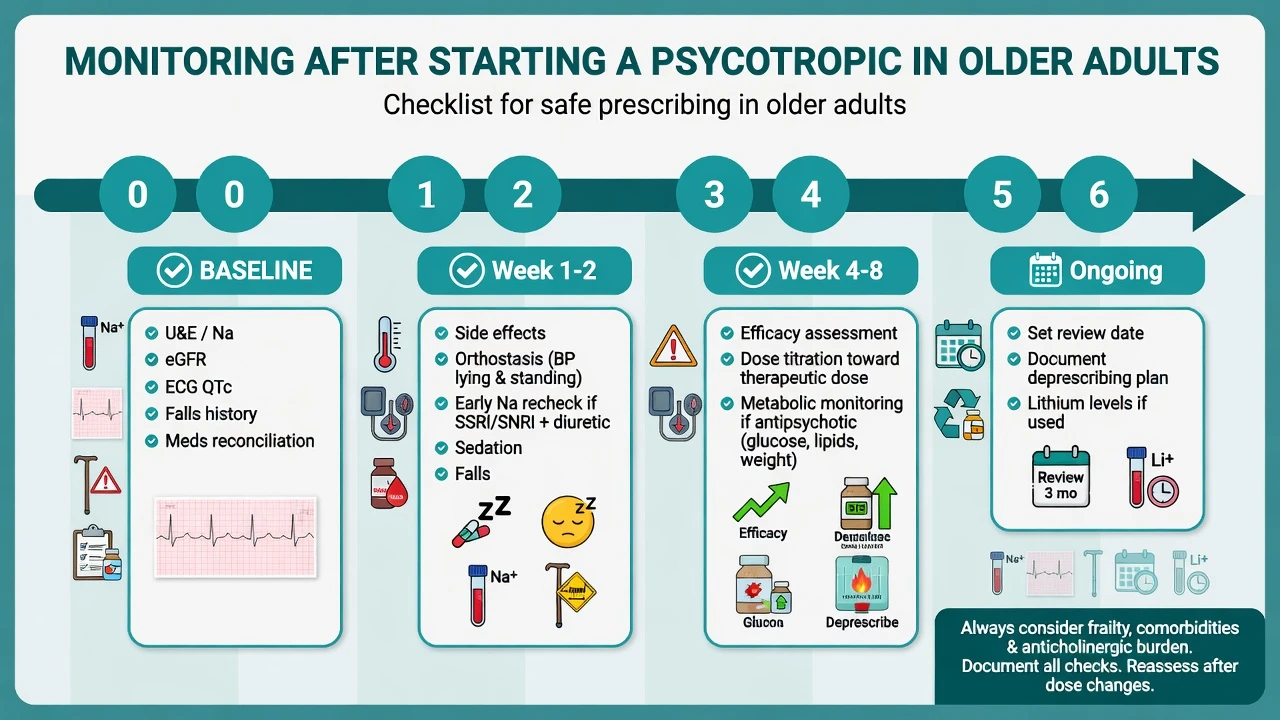
- Baseline investigations — U&E with sodium and eGFR, LFT, glucose/lipids if antipsychotic planned, TSH as indicated, ECG with QTc before higher-risk agents or in cardiac multimorbidity.[15]
Investigations and monitoring
| Timepoint | What to check |
|---|---|
| Baseline | U&E/Na, eGFR, LFT, ECG/QTc as indicated, falls/orthostasis, meds list, weight/metabolic if AP |
| 1–2 weeks after SSRI/SNRI | Clinical SIADH symptoms; repeat sodium especially with diuretics/age/frailty |
| Early after sedative or AP | Sedation, gait, EPS/akathisia, orthostasis, constipation/retention |
| Dose increases / new QT co-drug | Symptoms of arrhythmia; consider repeat ECG; fix K/Mg |
| Ongoing AP in dementia | Target symptom score, review/stop date, metabolic and neurological AEs |
| Lithium (if continued) | Levels, renal, thyroid, calcium per protocol — clearance falls with age |
Acute / emergency management
Definitive management — principles and algorithms
Core maxim
Start low, go slow, but go. Reduce starting dose and slow titration because of PK/PD change, but define an adequate trial at a therapeutic dose and duration for serious illness (especially late-life major depression). Token micro-doses for months produce pseudo-resistance and unfinished MEQs.[1][20]
Antidepressants (illustrative older-adult starts — individualise, check product information)
| Agent | Example start approach | Key older-adult monitors |
|---|---|---|
| Sertraline | 25 mg orally daily for several days then 50 mg daily; titrate toward therapeutic range if needed | Na, falls, GI, bleeding risk with anticoagulants/NSAIDs |
| Escitalopram | Low oral start (often 5 mg daily); respect labelled max in older adults | Na, QTc caution vs citalopram class teaching |
| Mirtazapine | 7.5–15 mg orally at night when sedation/appetite help desired | Sedation, falls, weight, rare agranulocytosis teaching |
| Avoid first-line frail | Most TCAs (anticholinergic, orthostasis, QTc); high-dose citalopram | Cardiac, falls, delirium |
| Citations | Illustrative starts only — individualise and check product information | See Fabian SIADH monitoring; RANZCP mood guidance |
Antipsychotics in dementia — black-box literacy
Efficacy is modest and often offset by intolerance (CATIE-AD). Meta-analysis and observational data support increased mortality; cerebrovascular events are a documented trial signal. Off-label use reviews show small benefits and clear harms in elderly dementia populations.[5][6][7][8][19]
When use may be justified. Severe aggression or distressing psychosis with risk of harm after non-drug care, medical exclusion, and pain review — with documented target, consent discussion, lowest effective dose, and a stop/review date.[5][6]
Illustrative low starts (frail older adult, oral). Risperidone 0.25–0.5 mg once or twice daily (commonly keep total daily dose modest, often at or under about 1–2 mg in dementia populations); olanzapine examples around 2.5 mg at night; quetiapine examples 12.5–25 mg when EPS risk is high — always reassess early for sedation, orthostasis, EPS and falls.[6][19]
Deprescribing nuance. DART-AD supports attempting withdrawal for many stable patients and raises long-term mortality concerns with continued neuroleptics; Devanand et al. show that among risperidone responders, discontinuation increases relapse risk — so plan a supervised taper with a restart threshold, not chaotic cessation or indefinite continuation by default.[9][10][11]
Anxiolytics and hypnotics
Benzodiazepines and Z-drugs are classic Beers PIMs. Glass meta-analysis shows unfavourable risk–benefit for sedative-hypnotics in older people with insomnia; Woolcott meta-analysis links sedatives/hypnotics, antidepressants and benzodiazepines to falls.[2][17][18] Prefer non-drug sleep strategies, treat pain/nocturia/depression causes, and if a medicine is unavoidable use the lowest dose for the shortest time with falls precautions — never "PRN forever" without a deprescribing plan.[2][17]
Mood stabilisers and other agents
Lithium remains highly effective for bipolar maintenance but requires proactive dose/level revision as GFR falls, plus renal, thyroid and calcium monitoring — toxicity risk rises with dehydration, NSAIDs, ACE inhibitors and diuretics.[20] Valproate and carbamazepine demand interaction literacy and laboratory monitoring; prefer specialist oversight in frailty.
QTc and falls — integrated safety
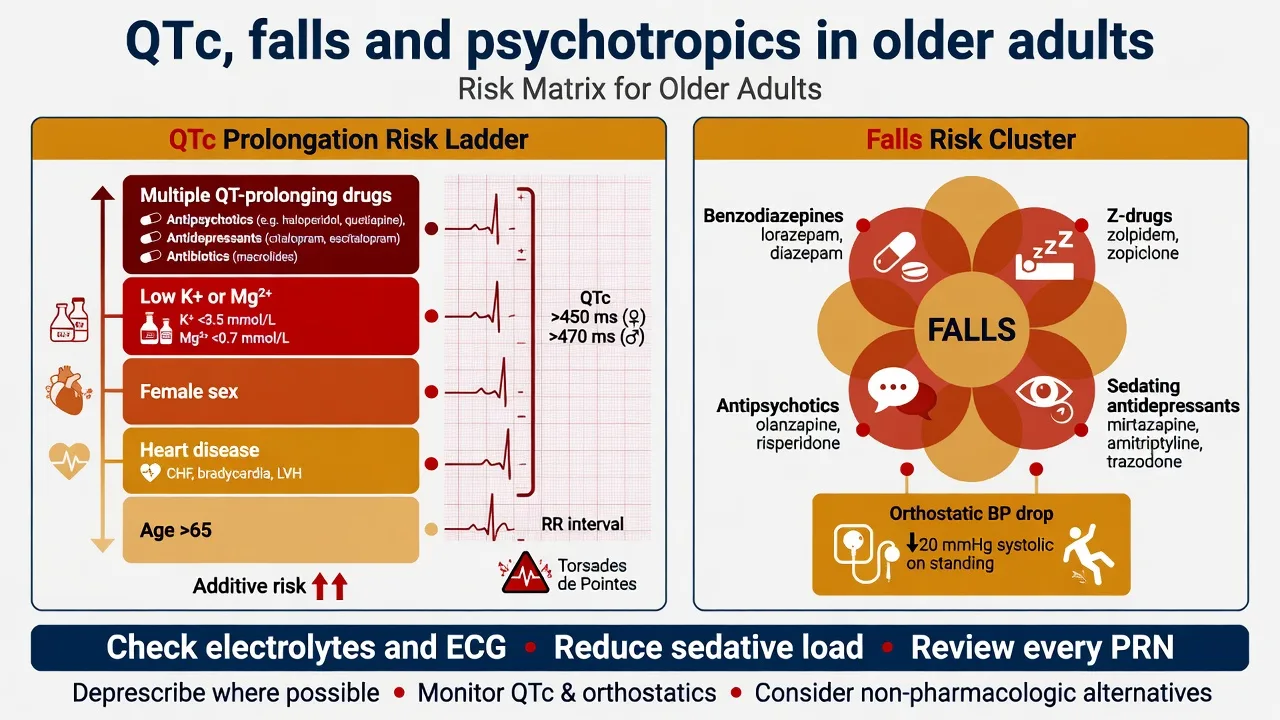
Teaching thresholds used in psychotropic QTc guidance: concern rises as QTc approaches 500 ms or with large increases from baseline (often taught around 60 ms); stop or switch culprits, fix electrolytes, and reassess co-drugs.[13][14][15] Falls prevention is medication review, not only physiotherapy referral.[18]
Subtypes and high-yield scenarios
Frail RACF resident on three psychotropics. Reconcile PRNs; stop duplicative sedation; treat pain; if antipsychotic lacks current target, taper with staff education (DART-AD mindset).[9][10]
Late-life MDD on thiazide. Start sertraline low, monitor sodium early, still titrate to efficacy; address suicide means.[16][20]
BPSD with severe aggression. Safety → delirium/pain → non-drug → time-limited low-dose atypical if risk persists; write stop date.[5][6]
Possible DLB. Avoid typical antipsychotics; extreme caution with any antipsychotic; rethink diagnosis if severe sensitivity appears.[5]
Cardiac disease needing antipsychotic. Prefer lower QTc-risk agents where efficacy allows; baseline and follow-up ECG; avoid QT stacking with methadone, macrolides, high-dose citalopram.[12][15]
Complications and pitfalls
- Antipsychotics for wandering, calling out, or mild irritability (wrong targets).[5][19]
- Start-low-stay-low under-treatment of depression.[20]
- Missing SIADH, anticholinergic delirium, constipation/retention, akathisia.[16]
- Assuming Z-drugs are "safe benzos."[2][17]
- No ECG or electrolyte attention when stacking QT risk.[15]
- No review date after dementia antipsychotic start.[9][11]
Prognosis and disposition
Appropriate prescribing and deprescribing reduce iatrogenic harm; inappropriate psychotropic load increases falls, delirium and mortality risk signals in vulnerable groups.[5][7][18] Disposition spans GP collaborative care, pharmacist-led reviews, old-age CMHT, residential medication advisory processes, and hospital CL psychiatry for complex polypharmacy. Intensity of follow-up peaks after new starts and after antipsychotic taper.[11][20]
Special populations
Oldest-old and frailty — even lower starts, fewer concurrent changes, goals-of-care honesty.[1] Renal impairment — lithium and renally cleared metabolites; dose by eGFR. Parkinson / PDD / DLB — antipsychotic and anticholinergic caution extreme.[5] Cultural diversity and Indigenous older adults — family decision styles, language, access to review. Intellectual disability ageing — diagnostic overshadowing and higher anticholinergic/polypharmacy risk.
Evidence and regional guidelines
Landmark anchors: Mangoni PK/PD; AGS Beers updates; STOPP/START v2; Schneider mortality meta-analysis; CATIE-AD; DART-AD and long-term follow-up; Devanand discontinuation; Gill mortality; Wooltorton CVA; Ray sudden cardiac death; Glass sedative-hypnotics; Woolcott falls; Fabian hyponatraemia; Funk/Beach-style QTc psychotropic guidance; RANZCP mood disorder guidelines for older-adult antidepressant principles.[1][2][4][5][6][15][20]
Australian and New Zealand practice emphasises RANZCP mood guidance for late-life depression dosing philosophy, TGA/Medsafe product information for any limited dementia behavioural wording (especially risperidone historically), and service BPSD protocols that still treat mortality/stroke risk as real. Prefer non-drug care; if antipsychotics are used, lowest dose, shortest time, documented indication, active deprescribing. Do not invent Mental Health Act section numbers across states/territories or NZ.[5][20]
Exam pearls
OLDER Rx safety
OLDER-RX
References
- [1]Mangoni AA, Jackson SHD Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications Br J Clin Pharmacol, 2004.PMID 14678335
- [2]By the 2023 American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [3]By the 2019 American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2019 Updated AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults J Am Geriatr Soc, 2019.PMID 30693946
- [4]O'Mahony D, O'Sullivan D, Byrne S, O'Connor MN, Ryan C, Gallagher P STOPP/START criteria for potentially inappropriate prescribing in older people: version 2 Age Ageing, 2015.PMID 25324330
- [5]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [6]Schneider LS, Tariot PN, Dagerman KS, Davis SM, Hsiao JK, Ismail MS, et al. Effectiveness of atypical antipsychotic drugs in patients with Alzheimer's disease N Engl J Med, 2006.PMID 17035647
- [7]Gill SS, Bronskill SE, Normand SL, Anderson GM, Sykora K, Lam K, et al. Antipsychotic drug use and mortality in older adults with dementia Ann Intern Med, 2007.PMID 17548409
- [8]Wooltorton E Risperidone (Risperdal): increased rate of cerebrovascular events in dementia trials CMAJ, 2002.PMID 12451085
- [9]Ballard C, Lana MM, Theodoulou M, Douglas S, McShane R, Jacoby R, et al. A randomised, blinded, placebo-controlled trial in dementia patients continuing or stopping neuroleptics (the DART-AD trial) PLoS Med, 2008.PMID 18384230
- [10]Ballard C, Hanney ML, Theodoulou M, Douglas S, McShane R, Kossakowski K, et al. The dementia antipsychotic withdrawal trial (DART-AD): long-term follow-up of a randomised placebo-controlled trial Lancet Neurol, 2009.PMID 19138567
- [11]Devanand DP, Mintzer J, Schultz SK, Andrews HF, Sultzer DL, de la Pena D, et al. Relapse risk after discontinuation of risperidone in Alzheimer's disease N Engl J Med, 2012.PMID 23075176
- [12]Ray WA, Chung CP, Murray KT, Hall K, Stein CM Atypical antipsychotic drugs and the risk of sudden cardiac death N Engl J Med, 2009.PMID 19144938
- [13]Glassman AH, Bigger JT Jr Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death Am J Psychiatry, 2001.PMID 11691681
- [14]Reilly JG, Ayis SA, Ferrier IN, Jones SJ, Thomas SH QTc-interval abnormalities and psychotropic drug therapy in psychiatric patients Lancet, 2000.PMID 10744090
- [15]Funk MC, Beach SR, Bostwick JR, et al. QTc Prolongation and Psychotropic Medications Am J Psychiatry, 2020.PMID 32114782
- [16]Fabian TJ, Amico JA, Kroboth PD, Mulsant BH, Corey SE, Begley AE, et al. Paroxetine-induced hyponatremia in older adults: a 12-week prospective study Arch Intern Med, 2004.PMID 14769630
- [17]Glass J, Lanctôt KL, Herrmann N, Sproule BA, Busto UE Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits BMJ, 2005.PMID 16284208
- [18]Woolcott JC, Richardson KJ, Wiens MO, Patel B, Marin J, Khan KM, Marra CA Meta-analysis of the impact of 9 medication classes on falls in elderly persons Arch Intern Med, 2009.PMID 19933955
- [19]Maher AR, Maglione M, Bagley S, Suttorp M, Hu JH, Ewing B, et al. Efficacy and comparative effectiveness of atypical antipsychotic medications for off-label uses in adults: a systematic review and meta-analysis JAMA, 2011.PMID 21954480
- [20]Malhi GS, Bell E, Bassett D, Boyce P, Bryant R, Hazell P, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391