Psych · Old age psychiatry — neurocognitive disorders
Vascular cognitive impairment and dementia
Also known as Vascular dementia · VaD · Vascular cognitive impairment · VCI · Major vascular neurocognitive disorder · Multi-infarct dementia · Subcortical ischaemic vascular dementia · Post-stroke dementia
Exam-exhaustive fellowship reference on vascular cognitive impairment and vascular dementia — VCI spectrum, NINDS-AIREN/VASCOG/VICCCS/DSM-5-TR criteria, multi-infarct stepwise versus subcortical small-vessel phenotypes, STRIVE imaging vocabulary, post-stroke dementia epidemiology, SPRINT MIND blood-pressure signal, secondary stroke prevention as disease modification, and modest AChEI/memantine trial evidence. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Vascular cognitive impairment is a high-yield old-age psychiatry topic because examiners test criteria evolution, tempo phenotypes (stepwise versus subcortical), imaging language without fake scans, post-stroke epidemiology, and the hard truth that risk-factor control beats cognitive enhancers as disease modification.[5][6][7]
Overview and definition
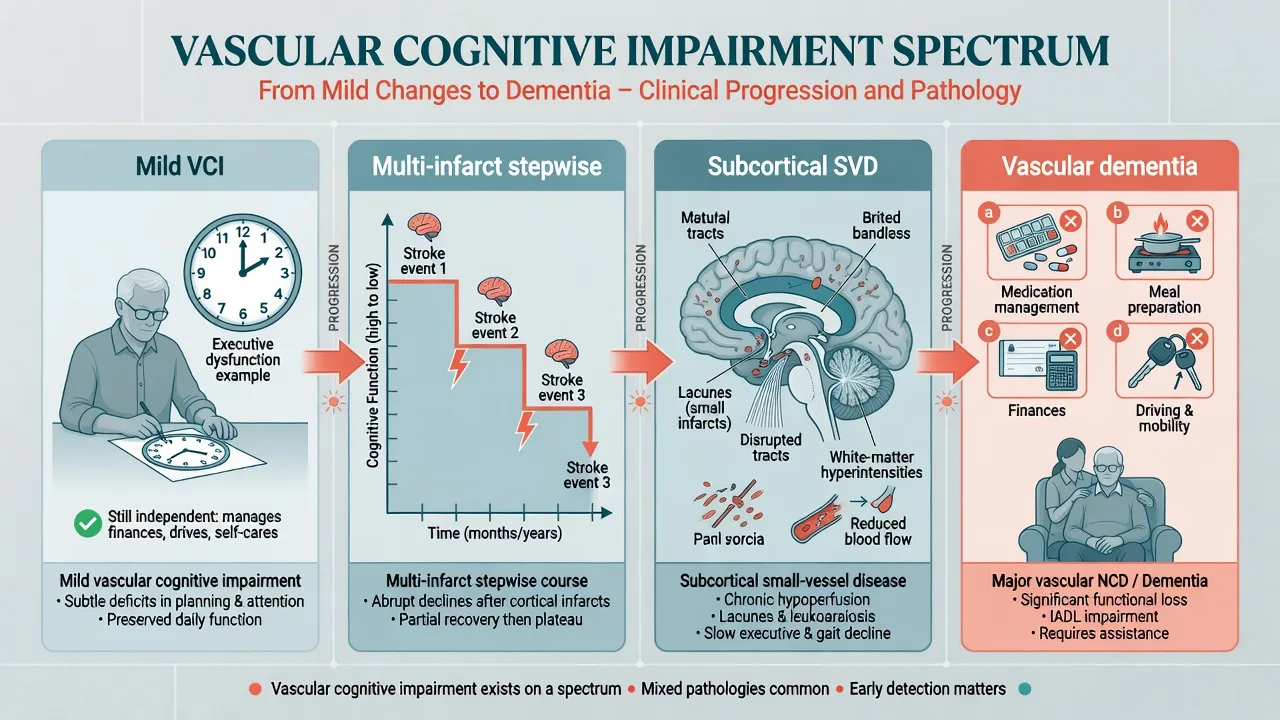
Vascular cognitive impairment (VCI) is the umbrella term for the full range of cognitive deficits attributable to cerebrovascular disease, from mild impairment through dementia. The American Heart Association/American Stroke Association statement frames vascular contributions to cognitive impairment and dementia as a public-health and clinical priority spanning pure vascular disease and mixed pathology.[3][6][7]
In DSM-5-TR language (Sachdev review of the DSM-5 NCD approach), the clinician specifies mild or major neurocognitive disorder due to vascular disease when the cognitive syndrome is consistent with a vascular aetiology and either neuroimaging evidence of cerebrovascular disease or a temporal association with one or more cerebrovascular events supports the link. Major disease requires interference with independence; mild does not, though compensation may be needed.[21]
ICD-11 retains dementia due to cerebrovascular disease / vascular dementia terminology. Fellowship answers should be bilingual: VCI for the spectrum, vascular dementia or major vascular NCD for the functionally impairing pole.[5][21]
Classification and diagnostic criteria

Historical NINDS-AIREN (Román 1993)
NINDS-AIREN research criteria for vascular dementia required a dementia syndrome, cerebrovascular disease (focal signs and imaging), and a relationship between the two (onset within about three months of a recognised stroke, or abrupt deterioration, or fluctuating stepwise course). Categories of probable, possible, and definite (histopathology) remain exam vocabulary even when clinical practice uses broader VCI language.[1]
VASCOG 2014
The VASCOG statement defines vascular cognitive disorders with mild and major tiers and emphasises objective cognitive deficits plus vascular aetiology supported by history and/or imaging — moving beyond pure multi-infarct dogma toward a clinically usable spectrum construct.[2]
VICCCS (Skrobot 2017/2018)
The Vascular Impairment of Cognition Classification Consensus Study standardised major VCI (vascular dementia) versus mild VCI and catalogued phenotypes including multi-infarct, subcortical ischaemic, strategic infarct, post-stroke dementia, and mixed presentations — the taxonomy most viva examiners now expect alongside DSM wording.[8][9]
AHA/ASA and harmonization standards
Gorelick and colleagues synthesised prevention and clinical care priorities for VCI; Hachinski and colleagues published NINDS–Canadian Stroke Network harmonization standards for VCI assessment protocols (5-, 30-, and 60-minute cognitive batteries) used in research and specialist clinics.[3][4]
| System | Core idea examiners want | Severity cut |
|---|---|---|
| NINDS-AIREN 1993 | Dementia + CVD + temporal/clinical relationship | Research VaD probable/possible |
| VASCOG 2014 | Vascular cognitive disorders spectrum | Mild vs major vascular cognitive disorder |
| VICCCS 2017/18 | Standardised major vs mild VCI + phenotypes | Functional interference |
| DSM-5-TR | Mild/major NCD due to vascular disease | Independence hinge |
Epidemiology and risk
Pendlebury and Rothwell meta-analysed pre-stroke and post-stroke dementia: rates are substantial, pre-stroke cognitive impairment is often under-recognised, and risk climbs with older age, low education, prior cognitive impairment, diabetes, atrial fibrillation, and recurrent stroke — examiners use this to demand secondary prevention, not only a memory clinic label.[10]
The Lancet Commissions place midlife hypertension, diabetes, smoking, obesity, physical inactivity, and excessive alcohol among population-attributable dementia risks; vascular risk control is therefore both stroke medicine and dementia prevention.[12][13]
SPRINT MIND randomised intensive versus standard systolic blood-pressure control among adults with hypertension and elevated cardiovascular risk. Intensive control significantly reduced mild cognitive impairment and the composite of MCI or probable dementia; the primary endpoint of probable dementia alone was not statistically significant — quote the trial accurately in viva, never invent a primary-endpoint win on dementia.[11]
Pathophysiology

Three mechanistic stories dominate exams:[5][6][7][15]
- Large-vessel multi-infarct disease — atherothromboembolism or cardioembolism produces multiple cortical and/or subcortical infarcts; cognition falls in steps related to events, with partial recovery plateaus.
- Strategic infarct — a single lesion in thalamus, angular gyrus, caudate, medial frontal territory, or hippocampus can produce disproportionate cognitive collapse.
- Cerebral small vessel disease (SVD) — arteriolosclerosis, lipohyalinosis, and chronic hypoperfusion generate lacunes, white-matter hyperintensities, microbleeds, and enlarged perivascular spaces; clinical phenotype is often gradual executive/processing-speed decline, gait disorder, and urinary symptoms rather than pure amnesia.[14][15]
Mixed Alzheimer and vascular pathology is the real-world majority in many oldest-old brains: vascular injury can unmask or amplify degenerative disease, so forcing a single pure subtype is often false precision.[5][7][23]
Clinical presentation — stepwise multi-infarct versus subcortical
Multi-infarct stepwise phenotype
Classic exam stem: abrupt cognitive drops after clinical strokes, plateaus between events, focal neurological signs, and cortical deficits (aphasia, neglect, hemiparesis) matching infarct topography. History of large-vessel or cardioembolic stroke is often clear.[1][5]
Subcortical ischaemic (small-vessel) phenotype
More often gradual or fluctuating than textbook stepwise. Early executive dysfunction and slowed processing speed, relatively better recognition memory early, apathy, gait disturbance (short-stepped, magnetic), urinary urgency/incontinence, and sometimes pseudobulbar affect. MMSE may look deceptively mild while MoCA and clock/executive tasks fail.[5][6][15][22]
Strategic infarct and post-stroke dementia
A single strategic lesion can meet dementia-level impairment after one stroke. Post-stroke dementia (VICCCS framing) is dementia temporally linked to stroke; distinguish evolving post-stroke recovery, delirium, depression, and pre-existing unrecognised NCD.[8][9][10]
Neuropsychiatric features
Depression, apathy, and emotional lability are common. Well-formed recurrent visual hallucinations with REM sleep behaviour disorder and spontaneous parkinsonism should pivot the differential toward Lewy body disease, not pure VaD.[5][24]
Differential diagnosis
| Mimic | Discriminators |
|---|---|
| Mixed AD + vascular | Amnestic + vascular tempo/imaging both meaningful — common and honest label |
| DLB | Fluctuations, visual hallucinations, RBD, parkinsonism, neuroleptic sensitivity |
| bvFTD | Early disinhibition/empathy loss without vascular story; younger onset |
| Delirium | Hours–days, inattention, marked fluctuation — treat medical cause |
| Late-life / vascular depression | Mood, anhedonia, effortful testing; treat and reassess cognition |
| NPH | Gait + incontinence + cognitive change — hydrocephalus pathway |
| CADASIL (younger) | Recurrent lacunar strokes, migraine, family history — genetics/neurology |
Assessment
- Collateral history — onset, tempo (stepwise vs gradual), stroke/TIA dates, AF, hypertension, diabetes, smoking, alcohol, medications (anticholinergics, sedatives, anticoagulants), function (IADL/ADL), BPSD, falls, driving.[3][4]
- MSE and bedside cognition — attention (delirium screen), processing speed, executive tasks, memory (free recall vs recognition), language, visuospatial, mood, apathy, insight, risk.
- Screens — MoCA is often more sensitive than MMSE for mild executive/visuospatial deficits; both are education- and culture-sensitive. Formal neuropsychology when subtype or capacity is contested.[22][27]
- Neurologic exam — focal signs, pyramidal/extrapyramidal features, gait, primitive reflexes, pseudobulbar signs.
- Risk and capacity — driving, fire, finances, wandering, elder abuse, carer burnout; Appelbaum four abilities for decision-specific capacity.[26]
Investigations and imaging framework
- Bloods: FBC, electrolytes, renal/liver, glucose/HbA1c, lipids, B12, folate, TSH; syphilis/HIV if atypical.[3][5]
- Cardiac/vascular: ECG for AF; further rhythm monitoring, echocardiography, and carotid imaging as the stroke pathway indicates — psychiatry owns the cognitive formulation but must not skip secondary prevention work-up.[3][10]
- Structural imaging: MRI preferred; CT when MRI unavailable. Educational vocabulary from STRIVE (Wardlaw): recent small subcortical infarct, lacune, white-matter hyperintensity, perivascular space, cerebral microbleed, brain atrophy — describe patterns generically; never invent a radiographic report for a fictional patient as if it were a real scan.[14]
- Imaging supports but does not alone diagnose VaD: white-matter hyperintensities are common in ageing; require clinical–radiologic correlation.[14][15]
Acute management and crisis care

Acute cognitive worsening on a vascular brain is delirium or new stroke until proven otherwise: infection, metabolic disturbance, pain, constipation, urinary retention, hypoxia, medication toxicity/withdrawal, and recurrent cerebrovascular events.[10][24]
Stabilise medically, de-escalate environment, and avoid reflexive antipsychotics. If imminent risk of harm persists after non-drug measures in established dementia, use the lowest effective dose for the shortest time, document mortality risk counselling (Schneider meta-analysis signal for atypical antipsychotics in dementia RCTs), and review daily for cessation.[24][25]
Hyperacute stroke/TIA features go to the stroke pathway, not a delayed memory clinic letter.[3]
Definitive management — vascular risk first
Disease-modifying lever: risk control and secondary prevention
This is the fellowship message. Optimise vascular risk and secondary stroke prevention as the primary disease-modifying strategy for VCI.[3][4]
- Blood pressure — individualised targets; SPRINT MIND supports intensive SBP lowering for cognitive outcomes (MCI reduction) in selected high-CV-risk hypertensives without diabetes in that trial population — translate carefully to frail multimorbid older adults.[11]
- Glycaemia, lipids, smoking cessation, physical activity, diet, alcohol limits — Lancet Commission multi-domain framing.[12][13]
- Atrial fibrillation — anticoagulation when indicated after stroke/TIA risk–benefit assessment.[3][10]
- Antiplatelet and secondary stroke prevention after atherothrombotic events per stroke guidelines (local stroke service protocols).[3][10]
- Hearing, social engagement, depression treatment as additional modifiable dementia risks.[12]
Person-centred care, rehabilitation (OT/PT/SALT), carer education, advanced care planning, and driving advice are core, not optional add-ons.[3][5][12]
Symptomatic cognitive pharmacotherapy (modest evidence)
Cholinesterase inhibitors and memantine are not primary disease-modifying therapy in pure VaD. Trial signals exist for modest symptomatic cognitive effects only.[16]
- Donepezil: Black and Wilkinson 24-week RCTs in VaD showed cognitive and some global benefits versus placebo.[17][18]
- Galantamine: Erkinjuntti trial in probable VaD and AD with cerebrovascular disease showed benefit versus placebo.[19]
- Memantine: Orgogozo MMM 300 found cognitive benefits in mild-to-moderate VaD with memantine 20 mg/day total (typically titrated toward 10 mg orally twice daily).[20]
- Kavirajan and Schneider meta-analysis: small cognitive benefits of AChEI and memantine in VaD with adverse-effect trade-offs — modest effect sizes, not a cure narrative.[16]
Exam dosing example when an AChEI is used after counselling and local formulary review (often more restricted than pure AD pathways in ANZ PBS practice): donepezil 5 mg orally once daily for at least 4 weeks, then 10 mg once daily if tolerated — monitor nausea, diarrhoea, anorexia, vivid dreams, bradycardia/syncope; obtain ECG when cardiac risk or interacting drugs. Review benefit and harm at about 3 months; stop if no meaningful gain.[16][17][18]
Do not prescribe cognitive enhancers as a substitute for blood-pressure control, AF management, or smoking cessation.[3][11][16]
BPSD
Use non-drug approaches first (Describe–Investigate–Create–Evaluate style systematic assessment). Treat pain, constipation, infection, and sensory impairment. Time-limited antipsychotics only for severe danger after non-drug care, with mortality counselling.[24][25]
Subtypes and scenarios
- Multi-infarct cortical VaD — stepwise, focal signs, secondary prevention urgency.[1][5]
- Subcortical ischaemic VaD — executive/gait/urinary triad, SVD imaging pattern.[15]
- Strategic infarct dementia — one lesion, large cognitive effect.[5][6]
- Post-stroke dementia — Pendlebury epidemiology; reassess after acute recovery window.[10]
- Mixed AD-vascular — dual formulation; cognitive enhancers may still be considered if AD phenotype is substantial and local criteria allow.[7][23]
- CL/stroke unit — avoid premature permanent labels while delirium and recovery evolve.[10][24]
Complications and pitfalls
Classic fails: equating any white-matter change with VaD; missing mixed AD; calling delirium "progression of VaD"; starting antipsychotics for apathy; AChEI without vascular optimisation or formulary realism; omitting driving and capacity; ignoring AF anticoagulation; young-onset SVD without CADASIL thought.[5][14][16][25][26]
Prognosis and disposition
Trajectory depends on recurrent stroke control, cardiac comorbidity, and mixed pathology. Recurrent events drive stepwise worsening; SVD may progress more gradually. Disposition ladder: home with packages of care and carer respite → residential care when night-time risk or carer collapse makes home unsafe. Shared care among GP, stroke/geriatric medicine, memory clinic, and old-age psychiatry.[5][10][12]
Special populations
Younger adults after stroke need vocational and family planning and genetic SVD awareness. Oldest-old usually have mixed pathology. CALD and Indigenous assessment requires interpreters and caution with unvalidated cut-offs. Capacity remains decision-specific (understand, appreciate, reason, communicate choice).[12][26]
Evidence, guidelines, and regional notes
- Criteria: NINDS-AIREN, VASCOG, VICCCS, DSM-5-TR NCD framing, AHA/ASA VCI statement, NINDS-CSN protocols.[1][2][3][4][8][9][21]
- Imaging: STRIVE; SVD review (Pantoni).[14][15]
- Prevention: Lancet Commissions; SPRINT MIND.[11][12][13]
- Drugs: Black/Wilkinson, Erkinjuntti, Orgogozo, Kavirajan meta-analysis.[16][17][18][19][20]
ANZ: Prioritise stroke secondary prevention pathways and PBS/TGA product information for any cognitive enhancer — access is often tighter for pure VaD than for AD; coordinate old-age psychiatry with geriatric medicine and stroke services; guardianship and driving authorities are state/territory-specific. UK: NICE dementia principles emphasise non-drug care and structured cognitive-drug pathways that may differ by aetiology. US: AHA/ASA VCI statement plus FDA boxed-warning-style antipsychotic mortality caution in dementia-related psychosis.[3][16][25]
Exam pearls
Vascular phenotype map
- VCI = spectrum; vascular dementia = severe end with functional loss.[3][21]
- Stepwise multi-infarct ≠ only phenotype — subcortical SVD is gradual executive/gait/urinary.[15]
- SPRINT MIND: intensive BP reduced MCI; probable dementia alone not significant — say it that way.[11]
- AChEI/memantine: modest RCT signals; Kavirajan meta-analysis; risk control is the main lever.[16]
- STRIVE vocabulary for SVD imaging education.[14]
- Delirium first in any acute change.[24]
- Capacity: understand, appreciate, reason, communicate choice.[26]
- Mixed AD-vascular is common — do not force purity.[7][23]
References
- [1]Román GC, Tatemichi TK, Erkinjuntti T, et al. Vascular dementia: diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop Neurology, 1993.PMID 8094895
- [2]Sachdev P, Kalaria R, O'Brien J, et al. Diagnostic criteria for vascular cognitive disorders: a VASCOG statement Alzheimer Dis Assoc Disord, 2014.PMID 24632990
- [3]Gorelick PB, Scuteri A, Black SE, et al. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the american heart association/american stroke association Stroke, 2011.PMID 21778438
- [4]Hachinski V, Iadecola C, Petersen RC, et al. National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards Stroke, 2006.PMID 16917086
- [5]O'Brien JT, Thomas A Vascular dementia Lancet, 2015.PMID 26595643
- [6]Dichgans M, Leys D Vascular Cognitive Impairment Circ Res, 2017.PMID 28154105
- [7]van der Flier WM, Skoog I, Schneider JA, et al. Vascular cognitive impairment Nat Rev Dis Primers, 2018.PMID 29446769
- [8]Skrobot OA, O'Brien J, Black S, et al. The Vascular Impairment of Cognition Classification Consensus Study Alzheimers Dement, 2017.PMID 27960092
- [9]Skrobot OA, Black SE, Chen C, et al. Progress toward standardized diagnosis of vascular cognitive impairment: Guidelines from the Vascular Impairment of Cognition Classification Consensus Study Alzheimers Dement, 2018.PMID 29055812
- [10]Pendlebury ST, Rothwell PM Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis Lancet Neurol, 2009.PMID 19782001
- [11]Williamson JD, Pajewski NM, Auchus AP, et al. Effect of Intensive vs Standard Blood Pressure Control on Probable Dementia: A Randomized Clinical Trial JAMA, 2019.PMID 30688979
- [12]Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission Lancet, 2020.PMID 32738937
- [13]Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care Lancet, 2017.PMID 28735855
- [14]Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration Lancet Neurol, 2013.PMID 23867200
- [15]Pantoni L Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges Lancet Neurol, 2010.PMID 20610345
- [16]Kavirajan H, Schneider LS Efficacy and adverse effects of cholinesterase inhibitors and memantine in vascular dementia: a meta-analysis of randomised controlled trials Lancet Neurol, 2007.PMID 17689146
- [17]Black S, Román GC, Geldmacher DS, et al. Efficacy and tolerability of donepezil in vascular dementia: positive results of a 24-week, multicenter, international, randomized, placebo-controlled clinical trial Stroke, 2003.PMID 12970516
- [18]Wilkinson D, Doody R, Helme R, et al. Donepezil in vascular dementia: a randomized, placebo-controlled study Neurology, 2003.PMID 12939421
- [19]Erkinjuntti T, Kurz A, Gauthier S, et al. Efficacy of galantamine in probable vascular dementia and Alzheimer's disease combined with cerebrovascular disease: a randomised trial Lancet, 2002.PMID 11965273
- [20]Orgogozo JM, Rigaud AS, Stöffler A, et al. Efficacy and safety of memantine in patients with mild to moderate vascular dementia: a randomized, placebo-controlled trial (MMM 300) Stroke, 2002.PMID 12105362
- [21]Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 approach Nat Rev Neurol, 2014.PMID 25266297
- [22]Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [23]McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514250
- [24]Kales HC, Gitlin LN, Lyketsos CG Assessment and management of behavioral and psychological symptoms of dementia BMJ, 2015.PMID 25731881
- [25]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [26]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [27]Folstein MF, Folstein SE, McHugh PR Mini-mental state. A practical method for grading the cognitive state of patients for the clinician J Psychiatr Res, 1975.PMID 1202204