Psych · Old age psychiatry — neurocognitive disorders
Young-onset dementia
Also known as Early-onset dementia · YOD · EOD · Presenile dementia (historical) · Early-onset Alzheimer disease · Working-age dementia
Exam-exhaustive fellowship reference on young-onset dementia (onset before 65): definitions, Hendriks/Harvey epidemiology, aetiologic spectrum (EOAD, FTD, vascular, alcohol, rapidly progressive, genetic-metabolic), dementia-plus signs, psychiatric misdiagnosis, structured work-up, APP/PSEN1/PSEN2 and FTD genetics, aetiology-directed treatment including donepezil when AD, antipsychotic caution, capacity, employment, and dependent children. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Young-onset dementia (YOD), also called early-onset dementia, is a high-yield old-age and adult neuropsychiatry examination topic. FRANZCP MEQs test the under-65 definition, the broader aetiologic mix than late-onset clinic samples, a named genetic pathway, and a working-age psychosocial plan. MRCPsych stations test communication about diagnosis delay, genetics, and family impact. ABPN items test EOAD genetics, FTD versus AD discrimination, and investigation strategy. This page is written so a candidate who has read nothing else can answer at consultant depth.[1][4][5]
Overview and definition
Young-onset dementia means a dementia syndrome in which first symptoms begin before 65 years. The cut-off is operational and epidemiologic, not a biological cliff — pathology overlaps late-onset disease, but relative frequencies, genetics, atypical phenotypes, and life-stage impact differ sharply.[1][4]
Do not confuse labels:
- YOD / EOD = age-of-onset descriptor for any aetiology.
- EOAD = early-onset Alzheimer disease specifically (often more aggressive or atypical than late-onset AD).
- Historical presenile dementia is obsolete exam language except as a distractor. Keep YOD (age) separate from EOAD (aetiology) in every formulation.[1][4]
DSM-5-TR codes major (or mild) neurocognitive disorder by aetiology (Alzheimer, frontotemporal, Lewy body, vascular, etc.) with age noted clinically. ICD-11 similarly codes dementia by type; YOD remains a clinical/service descriptor. State which framework you are using when asked for nosology.[6][12]
Rossor and colleagues framed young-onset diagnosis around careful clinical phenotyping and recognition of dementia-plus features — additional neurological signs that shift the differential toward genetic, metabolic, inflammatory, or prion disease rather than common late-life patterns alone.[1]
Classification and aetiologic spectrum
Major clinical groups (exam map)
| Group | Core teaching points | Classic discriminators |
|---|---|---|
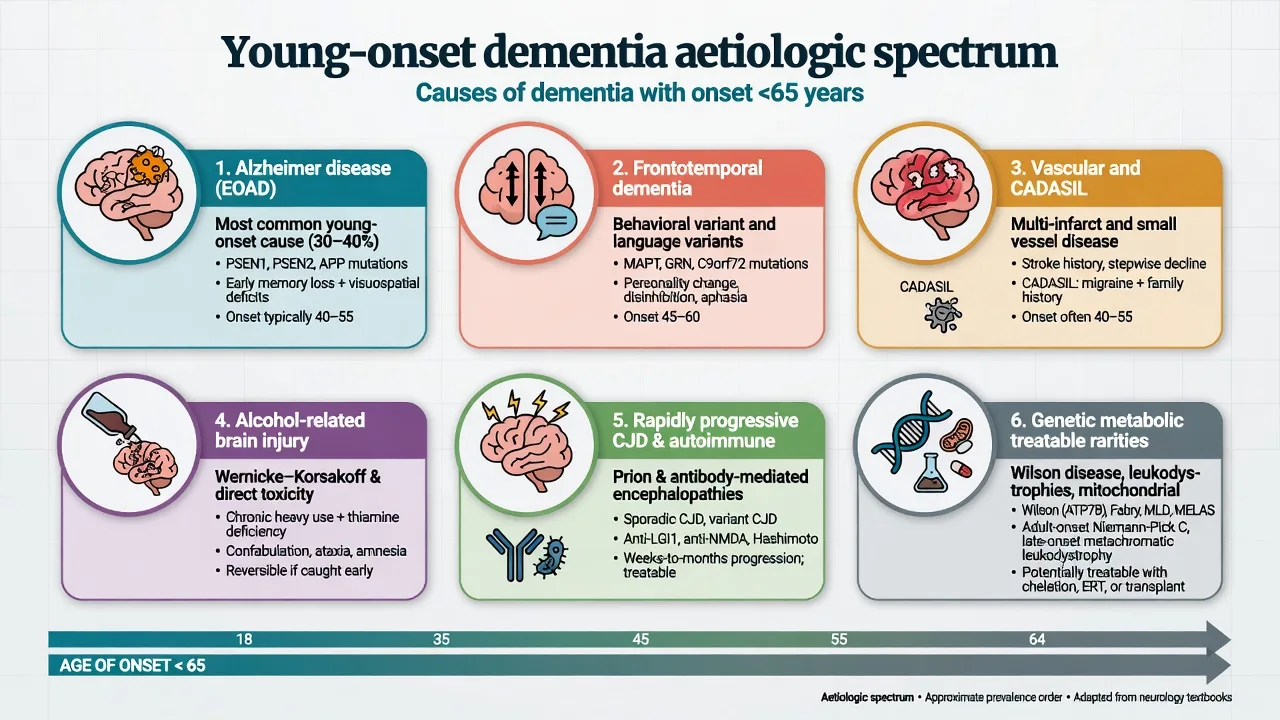
| EOAD | Most common neurodegenerative YOD in many series; amnestic or atypical (language, visuospatial, behavioural) | Progressive multi-domain decline; AD biomarkers when needed; APP/PSEN1/PSEN2 if familial |
| FTD spectrum | Disproportionately important under 65; bvFTD and PPA | Behaviour/language first; relative memory sparing early; Rascovsky/Gorno-Tempini criteria |
| Vascular / CADASIL | Strategic infarcts, small-vessel disease; NOTCH3 young strokes + dementia | Stepwise or frontal-subcortical pattern; vascular risk or familial young stroke |
| DLB / PDD | Less common than AD/FTD in YOD but examinable | Fluctuations, RBD, visual hallucinations, parkinsonism, neuroleptic sensitivity |
| Alcohol-related | Reversible contributors common; Wernicke–Korsakoff spectrum | Heavy use, nutrition, thiamine pathway |
| Rapidly progressive | Weeks–months | CJD, autoimmune encephalitis, infection, malignancy, toxic-metabolic |
| Genetic-metabolic rarities | Wilson, leukodystrophies, storage disorders, mitochondrial | Age, systemic and dementia-plus signs |
| These groups structure the under-65 differential used in Rossor-style and early-onset diagnostic frameworks; AD, vascular disease, and FTD dominate many clinic series, with alcohol and mixed pathology important in some catchments.[1][3][4][5] |
Epidemiology and risk
A UK population study of dementia under 65 reported prevalence on the order of tens per 100,000 in the 30–64 band and catalogued cause distributions dominated by AD, vascular disease, and FTD in that era — still a classic exam citation for service planning context.[3]
A 2021 global systematic review and meta-analysis estimated an age-standardised YOD prevalence of about 119 per 100,000 people aged 30–64, higher than older UK and Japanese point estimates and implying millions of working-age people living with dementia worldwide.[2] Prevalence rises steeply across successive age bands within the under-65 window.
Risk and clustering. Monogenic mutations drive a minority but high-stakes subset (APP, PSEN1, PSEN2 for familial AD; C9orf72, MAPT, GRN and others for FTD/ALS spectra). Vascular risks, heavy alcohol, traumatic brain injury, Down syndrome (premature AD pathology), and inflammatory disease contribute. Delayed diagnosis and first psychiatric labels are service-level risks, especially when behaviour or mood dominates early FTD presentations.[1][5][9][10][11]
Pathophysiology (exam-level mechanisms)
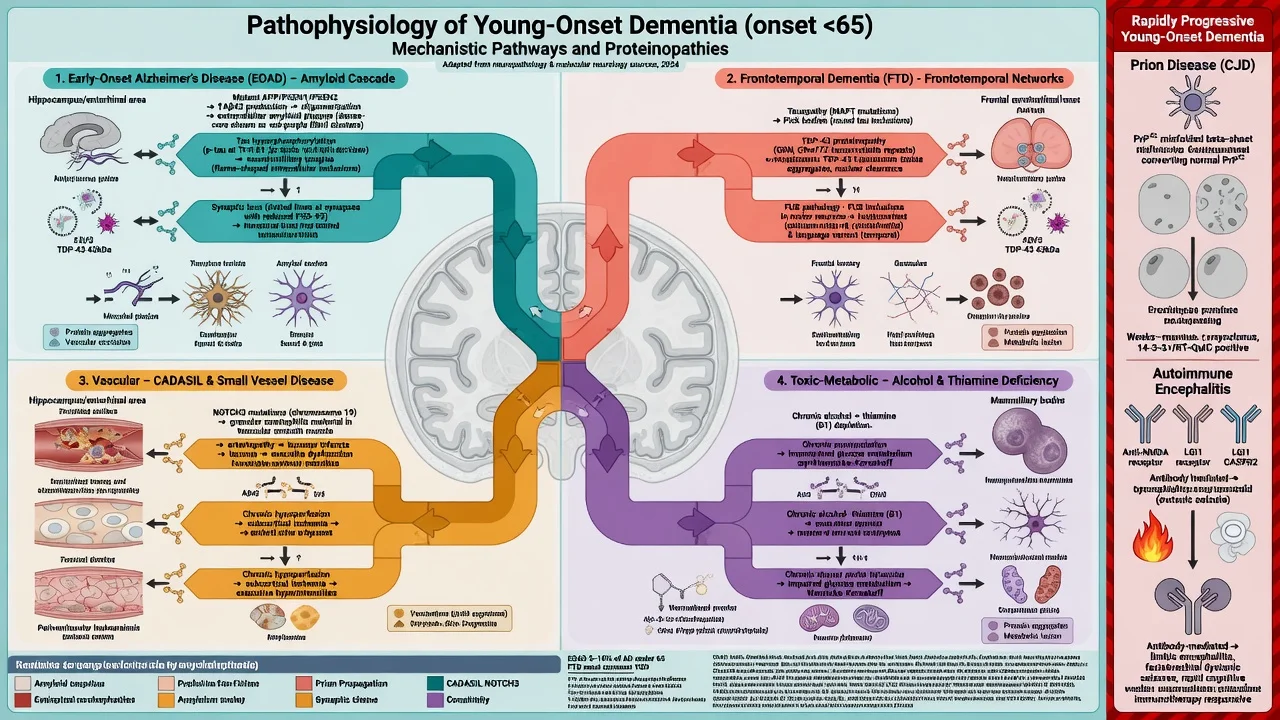
EOAD. Amyloid and tau pathophysiology as in late-onset AD, but monogenic defects in APP and presenilin (PSEN1/PSEN2) pathways accelerate early familial disease — foundational molecular discoveries that still structure viva genetics answers.[9][10][16] Phenotypes may be more atypical (language, posterior cortical, behavioural) than pure amnestic late-onset patterns; research frameworks such as LEADS characterise sporadic EOAD biomarkers and trajectories.[16]
FTD. Frontotemporal network proteinopathies (tau, TDP-43, FUS) produce behavioural and language syndromes disproportionately represented in midlife dementia clinics.[7]
Other pathways. Vascular ischaemic injury and genetic small-vessel disease (e.g. CADASIL teaching); thiamine deficiency and toxic-metabolic injury in alcohol-related brain disease; prion protein misfolding in CJD; antibody-mediated cortical/limbic dysfunction in autoimmune encephalitis; copper metabolism failure in Wilson disease at the younger edge of the YOD window.[1][4][5]
Clinical presentation
Presentation is progressive interference with complex work and life roles before 65 — not merely subjective forgetfulness. First domains vary by aetiology.[1][4]
- EOAD: memory encoding failure, word-finding, navigation, progressive multipledomain loss; may present as work inefficiency rather than "memory clinic classic."[6][16]
- bvFTD: disinhibition, apathy, loss of empathy, dietary change, rituals — often with relatively preserved bedside memory early and poor insight.[7][11]
- PPA: progressive language collapse as principal early deficit.[1][7]
- DLB: cognitive fluctuations, well-formed visual hallucinations, REM sleep behaviour disorder, spontaneous parkinsonism.[8]
- Rapid: subacute decline with myoclonus, startle, ataxia, seizures, or psychiatric prodrome — treat as emergency until proven otherwise.[1][4]
Psychiatric overlay is common: depression, anxiety, irritability, apathy, psychosis. In neurodegenerative disease — especially FTD — a prior primary psychiatric diagnosis is frequent before the correct label is reached. Longitudinal functional decline is the practical discriminator from remitting primary mood or psychotic episodes.[11]
Collateral history from partner, adult children, and (with consent) workplace is often more informative than the patient's self-report, particularly when insight is limited.[1][11]
Differential diagnosis
Neither column is absolute — depression can coexist with true YOD, and FTD is repeatedly mislabelled bipolar or personality disorder. Follow the curve over time and complete the organic work-up when progression continues.[1][11][12]
Key organic differentials within YOD: EOAD vs FTD vs vascular vs DLB vs alcohol-related vs mixed; space-occupying lesions; autoimmune encephalitis; CJD and other rapid dementias; HIV and other infections; B12/thyroid/metabolic; Wilson disease and adult storage/leukodystrophy disorders in selected ages and signs.[1][4][5]
Assessment
History structure. Exact age at first symptom; tempo (insidious vs rapid); first cognitive or behavioural domain; occupational complexity and safety-sensitive roles; driving incidents; financial errors; parenting and dependent children; alcohol and other substances; head injury; systemic disease; three-generation pedigree for dementia, ALS, young stroke, psychiatric institutionalisation, and consanguinity.[1][4][5]
Examination. Full MSE; cognitive screen (prefer MoCA or ACE-style tools over MMSE alone — FTD may score deceptively well early); neurologic exam for eye movements, pyramidal and extrapyramidal signs, cerebellar features, fasciculations, myoclonus, primitive reflexes, and Kayser–Fleischer rings when Wilson is plausible.[1][7][12]
Risk and capacity. Assess driving, occupation, finances, exploitation, aggression, fire/cooking, sexual disinhibition, child safety, and suicide risk (role loss with retained insight is high-stakes). Capacity is decision-specific: understand, appreciate, reason, and communicate a choice (Appelbaum). Use supported decision-making and least-restrictive legal pathways; statutes are jurisdiction-specific.[15]
Investigations
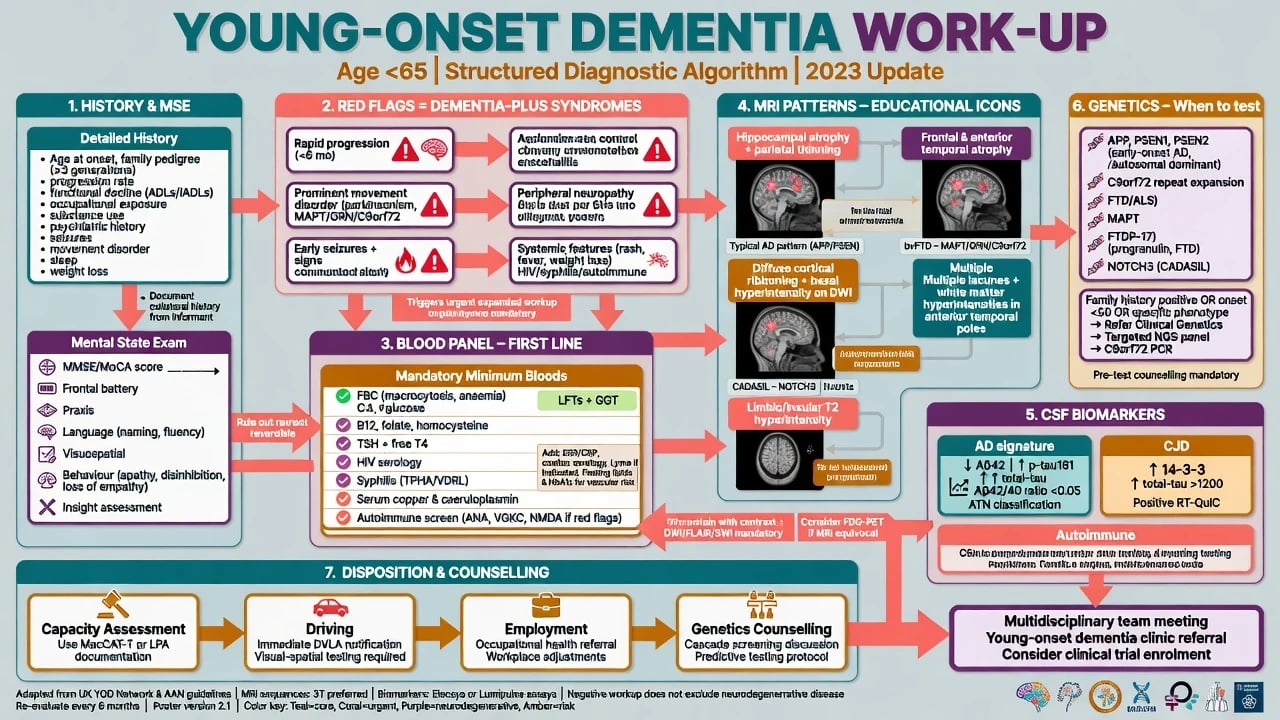
Bloods. FBC, U&E, LFT, glucose, B12, folate, TSH as baseline; HIV and syphilis when risk or atypical; consider copper studies and other metabolic tests when phenotype fits. These exclude contributors; they do not prove neurodegenerative subtype.[12]
Imaging. Structural MRI is preferred to exclude mass, inflammatory, and pattern-support findings (educational language only — never invent a patient scan). CT is a fallback when MRI unavailable. FDG-PET or amyloid PET may help in specialist pathways when structure is equivocal.[1][6][12]
CSF and EEG. AD core biomarkers support EOAD pathways when clinical distinction from non-AD is uncertain. Rapid courses may need CJD pathways (including RT-QuIC where available) and autoimmune encephalitis panels. EEG supports seizure, CJD, and encephalitic thinking.[1][4][16]
Genetics. Offer testing with pre- and post-test counselling for early onset, autosomal-dominant family patterns, or syndrome-guided genes (APP/PSEN1/PSEN2; FTD/ALS panel including C9orf72/MAPT/GRN; NOTCH3 for CADASIL phenotype, etc.). Do not force predictive testing on asymptomatic relatives without formal genetic counselling infrastructure.[5][9][10]
Acute and emergency management
Behavioural crisis. Safety first: remove access to cars, weapons, and unsupervised finances as needed; treat delirium triggers; de-escalate environmentally. Avoid reflexive high-dose antipsychotics. If imminent risk persists after non-drug measures, a time-limited lowest-effective-dose antipsychotic may be considered with explicit documentation of increased mortality risk in people with dementia and a stop/review plan.[14]
Definitive management
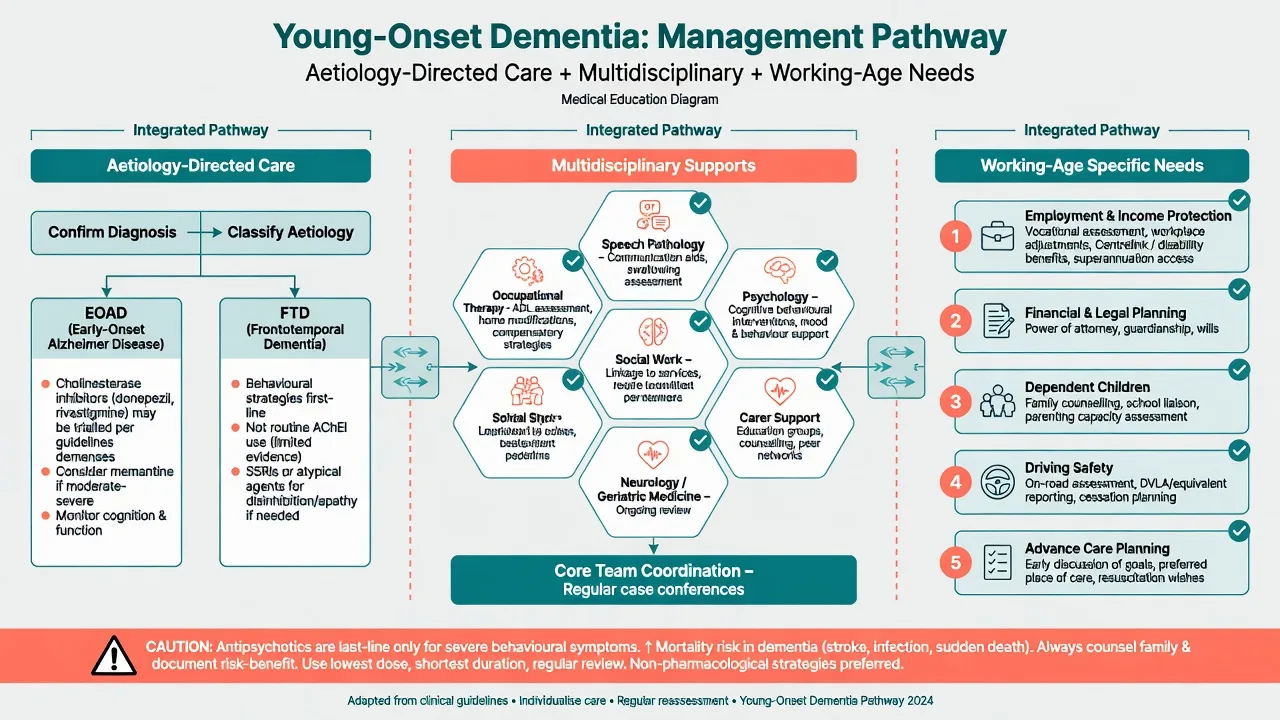
Aetiology-directed pharmacotherapy
When Alzheimer disease is the working diagnosis, cholinesterase inhibitors have evidence for symptomatic cognitive benefit in AD dementia. A Cochrane review supports donepezil for dementia due to Alzheimer disease with modest average effects and GI/cholinergic adverse effects to monitor.[6][13]
Named example (individualise; confirm local product information): donepezil 5 mg orally once daily, increase to 10 mg orally once daily after 4 weeks if tolerated; monitor nausea, diarrhoea, anorexia, vivid dreams/insomnia, bradycardia/syncope risk, and weight. Memantine may be considered in moderate–severe AD per usual AD pathways. This is not automatic therapy for pure FTD.[7][13]
Pure FTD: behavioural strategies first; limited symptomatic roles for serotonergic agents in specialist practice; do not copy-paste AChEI algorithms expecting AD-like benefit.[7]
DLB: if cholinesterase inhibition is used for cognitive/neuropsychiatric symptoms, respect neuroleptic sensitivity — avoid typical antipsychotics; any antipsychotic decision is high-risk.[8][14]
Vascular: aggressive vascular risk-factor control; no disease-modifying "dementia pill" replaces stroke prevention — secondary prevention is the disease-modifying step in this pathway.[4][12]
Alcohol-related: abstinence support, nutrition, thiamine repletion, treat depression and withdrawal carefully, and reassess cognition after sustained sobriety before locking a progressive neurodegenerative label.[4][12]
Non-pharmacological and service design
YOD care fails if it only offers aged-care packages. Essential elements: memory/behaviour clinic with adult neuropsychiatry or old-age expertise; occupational therapy for work and home safety; speech pathology for language variants; psychology for adjustment and carer support; social work for income protection, housing, and childcare; specialist YOD peer supports where available; early advance care planning while residual capacity exists.[1][4][12]
Antipsychotics and BPSD
Reserve antipsychotics for severe psychosis or dangerous aggression after behavioural measures. Counsel on the increased mortality signal from meta-analysis of atypical antipsychotics in dementia; use lowest dose, shortest duration, and documented review.[14]
Prognosis and disposition
Prognosis is aetiology-dependent. EOAD often declines faster on average than typical late-onset amnestic AD, but avoid single-number dogma — genetics, atypical phenotype, comorbidity, and support modify course. FTD survival varies by subtype and MND overlap. Rapid prion disease is measured in months; treatable autoimmune or metabolic disease may partially reverse if caught early.[1][4][16]
Disposition ladder. Community memory clinic; specialist YOD service; genetics clinic; hospital for rapid work-up; residential care earlier than chronological age peers may expect; involuntary pathways only when risk and incapacity meet local legal thresholds. Plan powers of attorney and guardianship interfaces early.[12][15]
Special populations and psychosocial axes
Working-age onset collides with employment, mortgages, dependent children, and identity. Assess parenting capacity and child safeguarding when relevant; involve family support services rather than framing everything as "aged care." Down syndrome and other intellectual disability populations develop AD pathology earlier — interpret baseline carefully. Cultural formulation affects help-seeking and decision styles. Forensic issues arise when disinhibition produces offending — assess neurocognitive contribution without excusing risk.[1][4][15]
Regional guideline notes
ANZ (FRANZCP / RANZCP context). Frame YOD within old-age and adult neuropsychiatry, cognitive disorders clinics, and jurisdiction-specific guardianship/mental health law. Service gaps for under-65 dementia are a known systems issue — name the need for age-appropriate supports.[1][12]
UK (NICE dementia principles). Person-centred care, carer support, non-drug approaches for behaviour, careful antipsychotic use, and structured assessment principles apply; YOD still requires broader differential and genetics literacy.[12][14]
US (APA / ABPN). Emphasise NIA-AA AD criteria literacy, EOAD genetics, LEADS-style biomarker thinking in specialist settings, and DLB/FTD criteria discrimination.[6][8][16]
India (MD/DNB / NEET-SS). Same clinical criteria and gene teaching; adapt drug availability, family-based care structures, and infection/metabolic differentials to local epidemiology while still naming agents you can monitor.[5][12]
Exam pearls
YOD exam checklist
This checklist compresses definition, differential expansion, work-up, genetics, and working-age care into a viva-ready scaffold.[1][2][5][12][13][14]
High-yield traps for MCQ/MEQ
- Equating YOD with EOAD only — FTD and others matter.[3][4]
- Closing midlife behavioural change as bipolar without longitudinal organic thinking.[11]
- Starting donepezil automatically for every under-65 dementia including pure bvFTD.[7][13]
- Skipping MRI and pedigree because "the patient is too young for dementia."[1]
- Ignoring employment, driving, and dependent children in the management plan.[4][15]
- Offering predictive genetic testing without counselling infrastructure.[5][9]
- Using long-term antipsychotics for wandering without behavioural formulation or mortality counselling.[14]
References
- [1]Rossor MN, Fox NC, Mummery CJ, Schott JM, Warren JD The diagnosis of young-onset dementia Lancet Neurol, 2010.PMID 20650401
- [2]Hendriks S, Peetoom K, Bakker C, et al. Global Prevalence of Young-Onset Dementia: A Systematic Review and Meta-analysis JAMA Neurol, 2021.PMID 34279544
- [3]Harvey RJ, Skelton-Robinson M, Rossor MN The prevalence and causes of dementia in people under the age of 65 years J Neurol Neurosurg Psychiatry, 2003.PMID 12933919
- [4]Kuruppu DK, Matthews BR Young-onset dementia Semin Neurol, 2013.PMID 24234358
- [5]Masellis M, Sherborn K, Neto P, et al. Early-onset dementias: diagnostic and etiological considerations Alzheimers Res Ther, 2013.PMID 24565469
- [6]McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease Alzheimers Dement, 2011.PMID 21514250
- [7]Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia Brain, 2011.PMID 21810890
- [8]McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium Neurology, 2017.PMID 28592453
- [9]Sherrington R, Rogaev EI, Liang Y, et al. Cloning of a gene bearing missense mutations in early-onset familial Alzheimer's disease Nature, 1995.PMID 7596406
- [10]Goate A, Chartier-Harlin MC, Mullan M, et al. Segregation of a missense mutation in the amyloid precursor protein gene with familial Alzheimer's disease Nature, 1991.PMID 1671712
- [11]Woolley JD, Khan BK, Murthy NK, et al. The diagnostic challenge of psychiatric symptoms in neurodegenerative disease: rates of and risk factors for prior psychiatric diagnosis in patients with frontotemporal dementia J Clin Psychiatry, 2011.PMID 21382304
- [12]Arvanitakis Z, Shah RC, Bennett DA Diagnosis and Management of Dementia: Review JAMA, 2019.PMID 31638686
- [13]Birks JS, Harvey RJ Donepezil for dementia due to Alzheimer's disease Cochrane Database Syst Rev, 2018.PMID 29923184
- [14]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [15]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [16]Apostolova LG, Aisen P, Eloyan A, et al. The Longitudinal Early-onset Alzheimer's Disease Study (LEADS): Framework and methodology Alzheimers Dement, 2021.PMID 34018654