Psych · Professional — boundary violations and sexual misconduct
Boundary violations and sexual misconduct
Also known as Sexual boundary violations · Physician sexual misconduct · Professional boundary violations · Post-termination sexual relationships · Slippery-slope boundary erosion · Therapist–patient sexual contact · Gutheil Gabbard boundaries
Exam-exhaustive fellowship reference on professional boundary violations and sexual misconduct in psychiatry — Gutheil–Gabbard crossing vs violation, slippery-slope mechanisms, epidemiology caveats from PHP series, sexual boundary violations (current, former, trainee), response algorithms, prevention and supervision, patient harm and professional consequences, dual-relationship risk, and RANZCP/GMC/AMA principle-level codes without invented statute numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
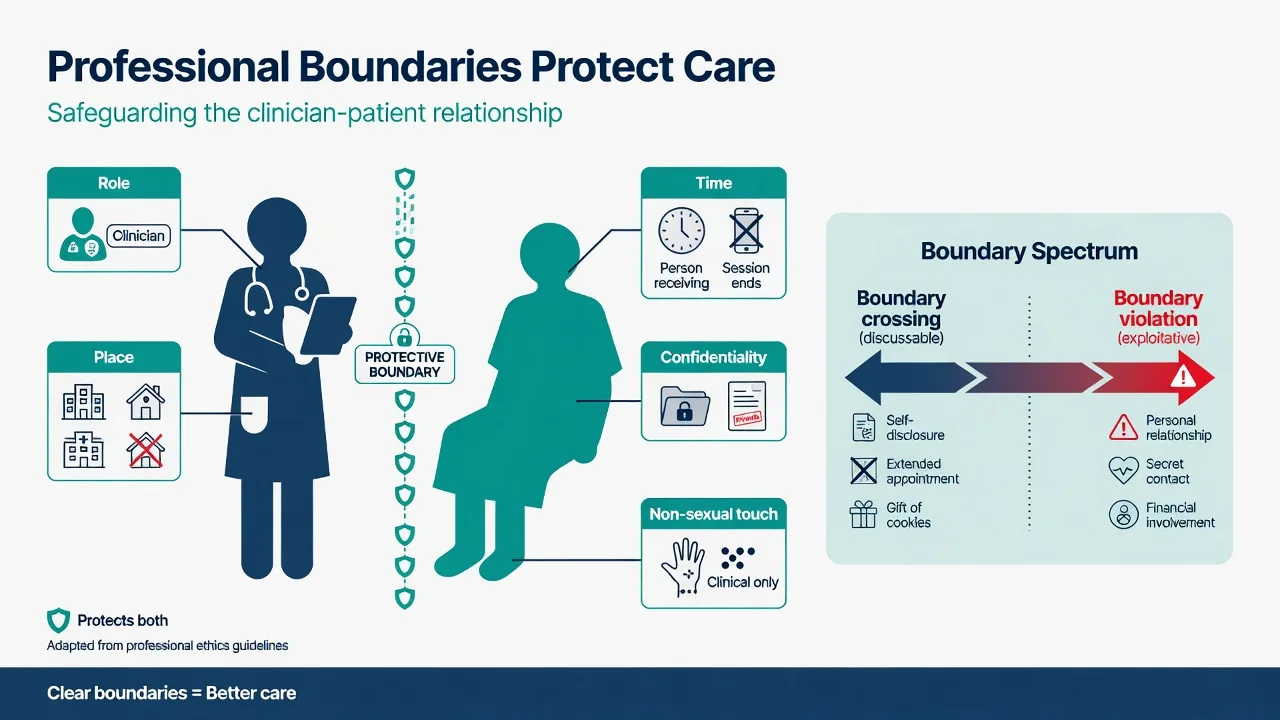
Boundary theory is high-yield across FRANZCP, MRCPsych, ABPN, and MD/DNB exams because psychiatry concentrates power, secrecy, dependency, and emotional intensity. A professional boundary is the edge of appropriate role behaviour that keeps the relationship therapeutic rather than personal, sexual, financial, or otherwise exploitative. The therapeutic frame includes role, time, place, fee, confidentiality, and rules for non-sexual physical contact.[1][8]
Sexual misconduct and sexual boundary violations (SBVs) form a spectrum from sexualised comments and harassment, through genital examination without clinical indication, to sexual contact (kissing, fondling, intercourse). With a current patient, sexual activity is never a legitimate clinical option. Hierarchical sexual relationships with current trainees or supervisees are likewise misconduct because of power abuse.[5][6]
This leaf topic deepens the sexual-misconduct and progressive-violation material beyond general professionalism. Related College themes — patient welfare, integrity, non-exploitation, collegial responsibility — sit in the RANZCP Code of Ethics literature; candidates should know themes, not invent clause numbers as universal law.[11][12][16]
Classification — crossing, violation, and sexual misconduct
| Construct | Core meaning | Exam anchor |
|---|---|---|
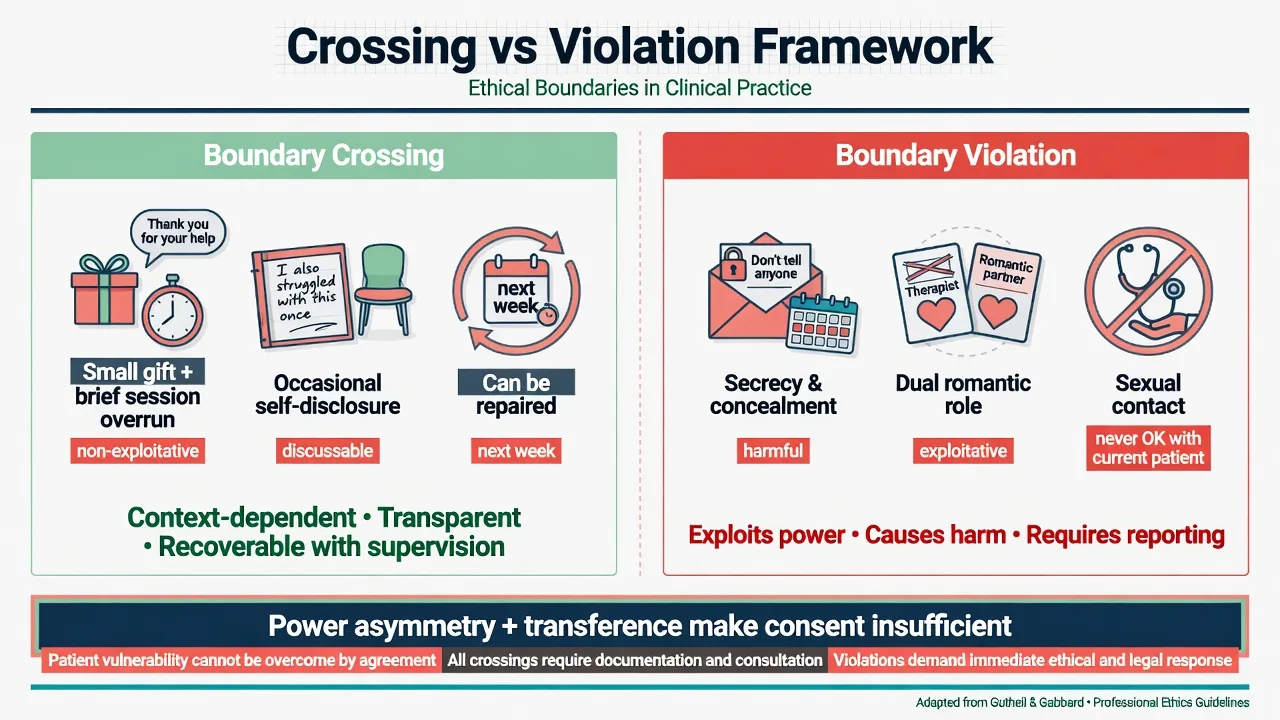
| Boundary crossing | Non-exploitative departure from usual frame; may be harmless, discussable, occasionally helpful | Gutheil and Gabbard 1993 |
| Boundary violation | Harmful or exploitative breach | Same; misuses warned 1998 |
| Sexual boundary violation | Sexualised use of the professional relationship | Norris; Gulrajani; Gabbard post-termination |
| Dual relationship | Second significant role outside professional care | Scopelliti; Endacott (ANZ) |
Boundary crossing examples: accepting a low-value handmade card after reflection; carefully considered brief self-disclosure for the patient's therapy; a one-off session extension after acute distress. Crossings should be reversible, patient-centred, and examinable in supervision.[1][8]
Boundary violation examples: sexual contact; financial exploitation; using the patient for the clinician's emotional or sexual needs; progressive secrecy and specialness that collapses the frame. Gutheil and Gabbard warned against misuse of boundary theory — either pathologising every human gesture or rationalising misconduct as "flexible technique". Context, exploitability, power, and harm matter, but some acts are violations regardless of claimed intent.[2][5]
Taxonomy of sexual boundary situations
| Setting | Ethical status | Notes |
|---|---|---|
| Current patient — sexual contact | Always violation / misconduct | Consent does not legitimise |
| Current patient — sexualised remarks, dual social-romantic roles | Violation / high-risk misconduct | Stop, supervise, transfer as needed |
| Former patient — post-termination sexual relationship | High-risk; often prohibited or tightly constrained by codes | Residual dependency and power remain |
| Termination engineered to enable sex | Misconduct | Not a loophole |
| Supervisee / trainee | Misconduct (power hierarchy) | Safe reporting pathways required |
| Staff sexual harassment by psychiatrist | Professional and often employment/criminal issue | Escalate via workplace and regulator pathways |
- Non-exploitative
- Discussable in supervision
- Often reversible
- Patient-centred rationale
- Document if significant
- Exploitative or harmful
- Often secretive
- Serves clinician needs
- Sexual/financial prototypes
- Report and protect
- Never OK with current patient
- Power voids 'consent'
- Post-termination still high-risk
- May be criminal assault
- Career-ending risk high
Epidemiology and risk contexts
True population prevalence of SBV is unknown because of under-reporting, delayed disclosure, and selection into board or physician-health-programme (PHP) samples. Candidates should describe patterns with caveats, not invent fixed percentages as universal rates.[7]
A 19-year PHP review of physician boundary violations found that referred violators were disproportionately men, often mid-career, and that psychiatrists were over-represented relative to the PHP base rate. Most violations in that series were sexual (though not always intercourse); non-sexual violations also occurred. Prior boundary violations were associated with sexual presentations as the current offence — a risk signal for boards and employers, not a deterministic "profile" for scapegoating individuals in ordinary practice.[7]
High-risk contexts examiners love: long-term psychotherapy with isolation; solo private practice without peer contact; after-hours personal digital contact; rural and small-community dual roles; clinician personal crisis, loneliness, depression, or substance use; intense personality pathology work without supervision; hierarchical supervisor–trainee relationships; and secrecy about "special" arrangements.[1][5][7][9]
Managing boundaries is itself stressful; reflective practice and supervision protect patient and clinician, whereas unexamined boundary strain contributes to burnout risk — strain is a risk context, never an excuse for misconduct.[13][14]
Mechanisms — why sexual misconduct happens
Psychiatry concentrates asymmetric power: the patient discloses secrets, depends on the clinician, and often idealises or fears them. Transference and countertransference charge the relationship. Boundaries exist to prevent exploitation of that asymmetry and to preserve conditions under which psychological treatment can work.[1][5]
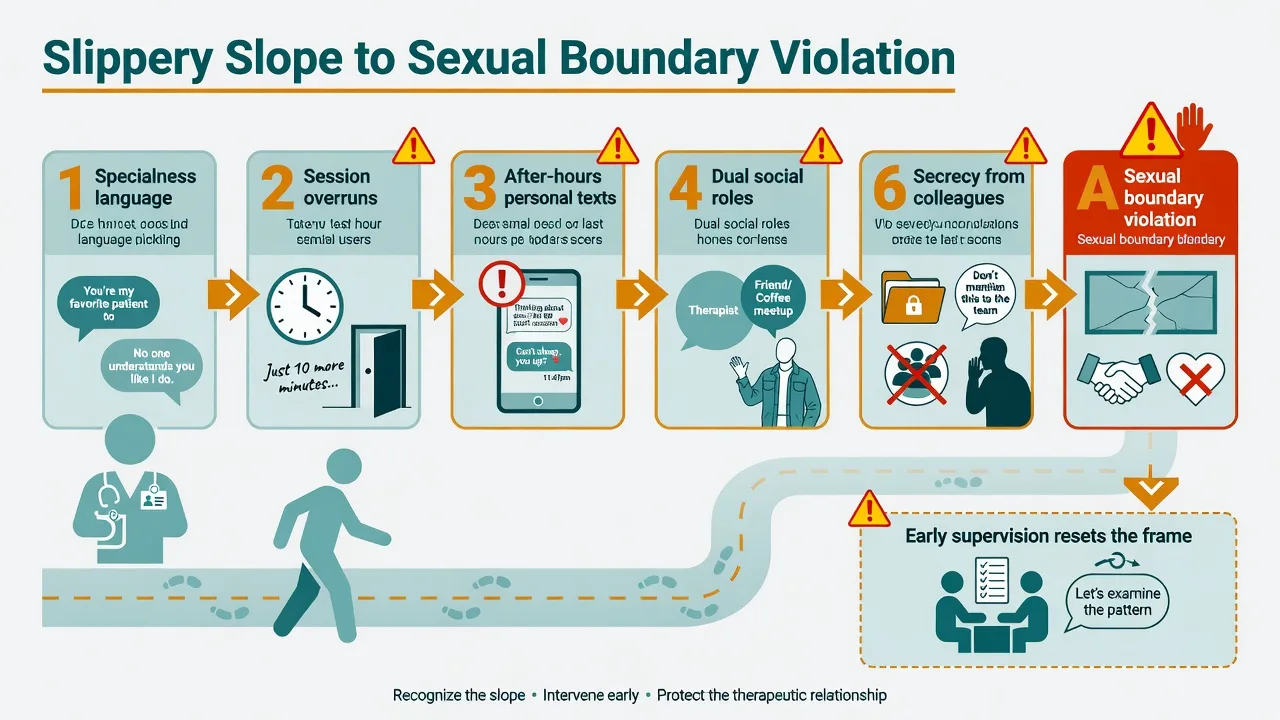
The classic slippery-slope pathway moves from small self-serving deviations — extra time "only for this special patient", personal texting, meetings outside the clinic, progressive personal self-disclosure — to dual social or romantic roles and sexual contact. Secrecy is the accelerant: what cannot be brought to supervision is already ethically dangerous.[1][5][8]
Clinician factors described in the literature include rescue fantasies, narcissistic need for admiration, loneliness, untreated mood or substance problems, and grandiosity about unique therapeutic capacity. Celenza and Gabbard's work on analysts who commit sexual boundary violations addresses typology and the limits of rehabilitation after serious SBV — exam-relevant when discussing "can this psychiatrist return to unrestricted practice?".[4][5]
Never blame the patient. The "seductive patient" myth shifts responsibility from the professional who holds the duty of care. Vulnerability, attachment hunger, trauma history, and idealisation increase risk of being exploited; they do not create ethical permission for the clinician to act sexually.[5][6]
Dual roles create role conflict — judgment is compromised when the clinician is simultaneously friend, employer, business partner, or lover. ANZ dual-relationship studies show these pressures are common in rural and small-community practice; sexual dual roles remain absolutely forbidden even when social dual roles are partly unavoidable.[9][10]
Clinical presentations (exam stems)
Expect stems such as: a long-term therapy patient discloses love and invites coffee; session overruns and personal after-hours texts have become habitual; a patient discloses that a previous psychiatrist made sexual advances; a colleague is rumoured to be in a sexual relationship with an outpatient; a trainee reports sexualised comments from a supervisor; a former patient contacts the doctor seeking a romantic relationship months after discharge; or a rural dual-role neighbour asks to become "friends outside clinic".[1][5][8][9]
Early warning signs of progressive boundary erosion: language of specialness ("only I understand you"); chronic session overruns; after-hours personal messaging; meetings outside clinical settings; shift from professional to personal self-disclosure; secrecy from colleagues; avoidance of notes; gifts that create indebtedness; and the clinician feeling rescued by the patient's admiration.[1][5][8]
Patient presentations after SBV may include delayed disclosure, trauma and PTSD-spectrum symptoms, shame, self-harm or suicide risk, mistrust of all clinicians, and ambivalence about reporting. Respond with trauma-informed care and non-judgmental support.[5][6]
Differential and discriminators
| Dilemma pair | Discriminator |
|---|---|
| Crossing vs violation | Exploitability, harm, secrecy, who benefits, reversibility |
| Erotic transference vs acting out | Worked with inside the frame vs acted on outside it |
| Warmth vs over-disclosure | For patient's therapy vs clinician's needs |
| Necessary rural dual role vs sexual dual role | Social dual roles may be unavoidable; sexual dual roles never are |
| Clinical examination vs sexualised examination | Indication, consent, chaperone, documentation vs no clinical purpose |
| Collegial rumour vs substantiated allegation | Facts, formal pathways, no gossip investigation |
Assessment — facts, power, and countertransference
There is no laboratory test for misconduct. Assessment means gathering facts, examining power and secrecy, consulting, and using proper institutional pathways when sexual misconduct is alleged.[5][8]
FRAME
Assess your own countertransference — attraction, rescue, anger, boredom, idealisation — in supervision, not by acting. Assess the patient's capacity and vulnerability carefully, but never use capacity language to claim that sexual contact with a current patient is ethically permitted.[1][5]
When a patient discloses alleged SBV by another clinician: believe and support; assess safety and suicide/self-harm risk; do not investigate alone or force confrontation; discuss reporting options and support pathways; assist with alternative care; preserve records; protect against retaliation. Thresholds for mandatory reporting of practitioners are jurisdiction-specific — state principles, not invented section numbers.[6][15]
Investigations and governance
"Investigate" means clinical governance, not blood tests: contemporaneous notes, appointment systems, message logs on governed platforms, prior complaints, and employer policy. Do not conduct a private detective process that retraumatises the complainant or contaminates evidence. Preserve documentation integrity — never alter or destroy records after an allegation.[5][6]
Depending on severity and jurisdiction, pathways may include clinical director review, employer sexual-misconduct procedures, medical board or regulator notification, physician health programmes for non-sexual or impairment issues, and police when criminal thresholds (sexual assault) may apply. Name the principle and local process; do not invent tribunal form names.[6][7][15]
Acute management — when SBV is alleged or imminent
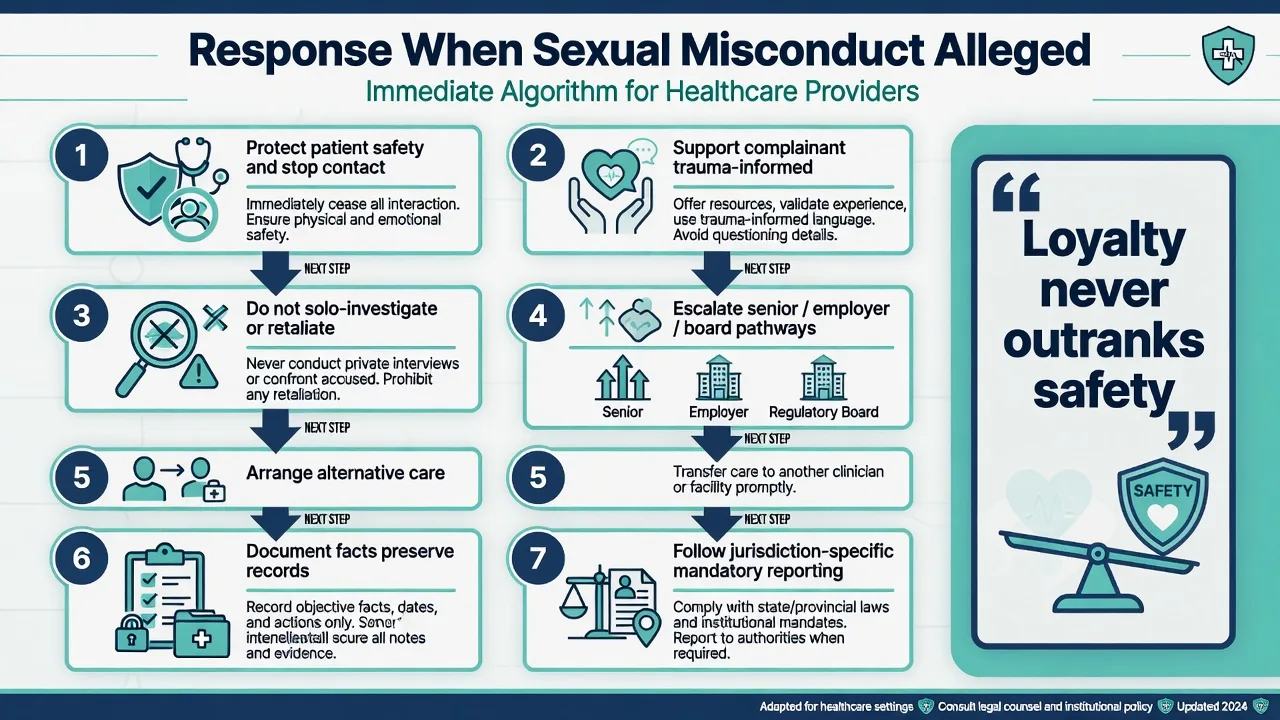
Immediate priorities when sexual misconduct is alleged or discovered include patient safety, stopping exploitation, supporting the complainant without coercion, proper escalation, alternative care, and documentation — without solo investigation or retaliation.[5][6]
- Patient safety — physical and psychological; assess suicide and self-harm risk.
- Stop exploitation — remove the alleged clinician from that patient's care; no further dual contact.
- Support the complainant — trauma-informed, non-blaming stance; advocacy without coercion.
- Do not solo-investigate, retaliate, or silence — no pressure to withdraw a complaint.
- Escalate — senior clinician, employer incident system, medical board or regulator as required by local law and policy.
- Arrange alternative care promptly — avoid abandonment.
- Document objective facts contemporaneously; preserve records.[5][6]
If you recognise early crossings in your own practice (personal texts, specialness, session overruns): stop personal contact immediately; reinstate time and place boundaries; take the case to urgent supervision; document; consider transfer of care if the frame cannot be restored or if your needs are driving the contact. Do not shame the patient for erotic transference; hold the limit and work with the material clinically when appropriate.[1][5][8]
Definitive management — prevention, codes, and remediation
Prevention (the real definitive treatment)
| Domain | Practical standard |
|---|---|
| Frame | Clear role, time, place, fee, confidentiality, touch rules |
| Supervision | Regular peer review especially for long-term psychotherapy and intense attachment work |
| Digital contact | Governed clinical systems; no personal after-hours romantic or dual-role messaging |
| Dual relationships | Avoid when alternatives exist; document unavoidable rural dual roles; never sexual or exploitative financial dual roles |
| Self-care | Treat personal crisis, loneliness, substance use before they leak into the dyad |
| Culture | Normalise discussion of attraction and specialness in supervision without shame |
| Codes | Know RANZCP Code themes and local medical-board sexual-boundaries guidance |
Response ladder for emerging (non-sexual) boundary concern
| Stage | Action |
|---|---|
| Mild single crossing | Reflect; document rationale; discuss in supervision |
| Pattern emerging | Modify practice; tighten frame; consider transfer |
| Sexualised content or exploitation risk | Stop; transfer care; senior consultation; report as required |
| Alleged SBV by other | Safety first; formal pathways; no solo investigation |
Post-termination sexual relationships
Post-termination sexual boundary violations remain ethically and clinically high-risk because residual dependency, transference, and power often persist. Gabbard's analysis is a classic viva anchor: ending formal treatment does not automatically create an equal peer relationship. Many professional codes prohibit or tightly constrain post-termination sexual relationships for prolonged periods or indefinitely in psychotherapy contexts — know local code language rather than inventing a universal fixed-year rule as law. Engineering termination to enable sex is misconduct.[3][4]
Remediation and return to practice
Some non-sexual boundary problems and impairment issues can be addressed through physician health programmes with monitoring and supervised practice. Serious sexual misconduct is frequently career-ending; boards may impose suspension, conditions, or deregistration, and criminal proceedings may apply. Celenza and Gabbard's discussion of analysts who commit SBV challenges naive optimism about unrestricted return after serious sexual exploitation.[4][7]
Subtypes and high-yield scenarios
Current outpatient psychotherapy. Classic slippery-slope setting. Hold the frame; erotic material is clinical, not social opportunity.[1][5]
Inpatient / acute settings. Vulnerability and power differentials are extreme; sexual contact and dual social roles remain forbidden.[6]
Historical disclosure of prior clinician SBV. Support, pathways, trauma care, documentation; do not minimise as gossip.[6]
Rural dual-relationship pressure. Minimise scope, document, supervise, use referral/telehealth when dual-role risk is high; sexual dual roles remain absolute no.[9][10]
Trainee–supervisor. Hierarchical power; sexual or romantic relationships with current trainees are misconduct; services need safe reporting routes.[6]
Gifts and social invitations as precursors. Expensive gifts and dinner invitations are dual-relationship risks that can sit on the slope toward violation if met with secrecy or collusion; decline kindly, explore meaning, document, supervise.[1][8]
Complications and pitfalls
Classic pitfalls: rationalising progressive crossings as special technique; blaming the patient; treating "consent" as ethical absolution; terminating care to enable sex; protecting a colleague's reputation over patient safety; solo investigation that retraumatises; destroying or altering records; failing to arrange alternative care (abandonment); inventing universal statute numbers for reporting; and assuming rural practice is an ethics-free zone.[2][3][5][6][9][15]
Prognosis, consequences, and disposition
Professional consequences of serious SBV include medical-board sanctions, conditions on practice, suspension or deregistration, civil liability, criminal charges for sexual assault, and lasting reputational harm. Patients may experience betrayal trauma, deterioration, self-harm, and avoidance of future care — arrange trauma-informed alternative treatment and risk assessment.[5][6][7]
Disposition after a boundary crisis: transfer care to another clinician; avoid ongoing dual roles with the complainant; document handover factually; support complaint pathways without coercion; protect access to care without abandonment.[5][6]
Special populations
Intense attachment and personality organisation. Idealisation and eroticised transferences increase crossing pressure; a firmer frame and more supervision are protective, not punitive.[1][13]
Child and adolescent. Absolute prohibition of sexual contact; boundaries extend to parents and schools; child-protection principles apply when abuse is disclosed.[6]
Intellectual disability and capacity-impaired patients. Heightened vulnerability; power asymmetry is greater, not lesser.[6]
Cultural contexts. Gift and kinship norms may create dual relationships; curiosity and cultural supervision are required — never a pathway to sexual dual roles.[9][16]
Trainees. Hierarchical power; safe reporting; no retaliation for raising concerns.[6]
Evidence, guidelines, and regional differences
Landmark anchors: Gutheil and Gabbard boundary theory (1993, 1998); Gabbard on post-termination SBV; Celenza and Gabbard on analysts who commit SBV; Norris, Gutheil, and Strasburger on "this couldn't happen to me"; Gulrajani on duty to protect patients from physician sexual misconduct; Brooks PHP series; Pope and Keith-Spiegel practical boundary decision-making; Scopelliti and Endacott dual-relationship ANZ studies; RANZCP Code revision and anniversary literature; Robertson values study; Lampe on boundary strain and burnout; Bismark on mandatory reporting tensions in Australia.[1][2][3][4][5][6][7][11][15]
Exam pearls
STOPSEX
References
- [1]Gutheil TG, Gabbard GO The concept of boundaries in clinical practice: theoretical and risk-management dimensions Am J Psychiatry, 1993.PMID 8422069
- [2]Gutheil TG, Gabbard GO Misuses and misunderstandings of boundary theory in clinical and regulatory settings Am J Psychiatry, 1998.PMID 9501754
- [3]Gabbard GO Post-termination sexual boundary violations Psychiatr Clin North Am, 2002.PMID 12232973
- [4]Celenza A, Gabbard GO Analysts who commit sexual boundary violations: a lost cause? J Am Psychoanal Assoc, 2003.PMID 12866759
- [5]Norris DM, Gutheil TG, Strasburger LH This couldn't happen to me: boundary problems and sexual misconduct in the psychotherapy relationship Psychiatr Serv, 2003.PMID 12663839
- [6]Gulrajani C A Duty to Protect Our Patients from Physician Sexual Misconduct J Am Acad Psychiatry Law, 2020.PMID 32393516
- [7]Brooks E, Gendel MH, Early SR, et al. Physician boundary violations in a physician's health program: a 19-year review J Am Acad Psychiatry Law, 2012.PMID 22396343
- [8]Pope KS, Keith-Spiegel P A practical approach to boundaries in psychotherapy: making decisions, bypassing blunders, and mending fences J Clin Psychol, 2008.PMID 18386835
- [9]Scopelliti J, Judd F, Grigg M, et al. Dual relationships in mental health practice: issues for clinicians in rural settings Aust N Z J Psychiatry, 2004.PMID 15555031
- [10]Endacott R, Wood A, Judd F, et al. Impact and management of dual relationships in metropolitan, regional and rural mental health practice Aust N Z J Psychiatry, 2006.PMID 17054567
- [11]Bloch S, Kenn F, Smith G Revising the Royal Australian and New Zealand College of Psychiatrists code of ethics Australas Psychiatry, 2018.PMID 30058364
- [12]Lim I, Kenn F, Bloch S The 30th anniversary of the code of ethics of the Royal Australian and New Zealand College of Psychiatrists-a worthy milestone Australas Psychiatry, 2022.PMID 35077253
- [13]Lampe L, Hitching R, Hammond TE, et al. Being a 'good' doctor: Understanding and managing professional boundaries is challenging and can lead to stress and burnout Australas Psychiatry, 2023.PMID 37563780
- [14]Reyes Nieva H, Ruan E, Schiff GD Professional-Patient Boundaries: a National Survey of Primary Care Physicians' Attitudes and Practices J Gen Intern Med, 2020.PMID 31755012
- [15]Bismark MM, Mathews B, Morris JM, et al. Views on mandatory reporting of impaired health practitioners by their treating practitioners: a qualitative study from Australia BMJ Open, 2016.PMID 27993902
- [16]Robertson M, Kerridge I, Walter G Ethnomethodological study of the values of Australian psychiatrists: towards an empirically derived RANZCP Code of Ethics Aust N Z J Psychiatry, 2009.PMID 19373701