Psych · Professional — psychological therapies
CBT fundamentals for psychiatrists
Also known as Cognitive behavioural therapy · Cognitive behavioral therapy · Cognitive therapy · Beckian CBT · Behavioural experiments · Case conceptualisation CBT · CBTp · Exposure and response prevention
Exam-exhaustive fellowship reference on CBT for psychiatrists — cognitive model, five-area formulation, session and course structure, behavioural experiments and exposure, indications and evidence by disorder, integration with medication, therapist drift, and supervision. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship examiners (FRANZCP clinical assessments, MRCPsych CASC/Paper B, ABPN, MD/DNB viva) expect you to use CBT language: name maintaining cycles, design a behavioural experiment, justify when BA precedes complex cognition work, and know when CBT is first-line, adjunctive, or the wrong tool today because risk or mania dominates.[6][8]
Definition and scope
CBT grew from Beck’s cognitive model of depression and from behavioural science (exposure, activation, operant principles).[1][2][3] Modern CBT is a family, not one brand:
| Package | Core targets | Exam note |
|---|---|---|
| Beckian cognitive therapy | Automatic thoughts, intermediate beliefs, core beliefs/schemas | Classic depression/anxiety formulation |
| Behavioural activation (BA) | Low reinforcement, avoidance, inactivity loops | Often first when depression is severe or rumination-heavy |
| Exposure / ERP | Avoidance, rituals, safety behaviours | OCD, panic, phobia, social anxiety |
| Trauma-focused CBT / CT-PTSD | Trauma memory processing, appraisals, strategies | PTSD — protocol competence required |
| CBTp | Appraisals of voices/paranoia, safety behaviours, reasoning | Adjunctive to antipsychotics |
| Third-wave relatives | Acceptance, values, mindfulness, skills (ACT, DBT, MBCT) | Related but not interchangeable with classic CBT in stems |
Cognitive-behavioural model (mechanisms)
Levels of cognition
- Automatic thoughts (ATs): rapid, situation-linked appraisals (“I’ll mess this up”).
- Intermediate beliefs / rules: “If I show weakness, people leave.”
- Core beliefs / schemas: global self/world/other assumptions (“I am defective”). [1] [2] [3]
Stress and mood activate deeper structures; biased attention, memory, and interpretation keep them online.[1][2][3]
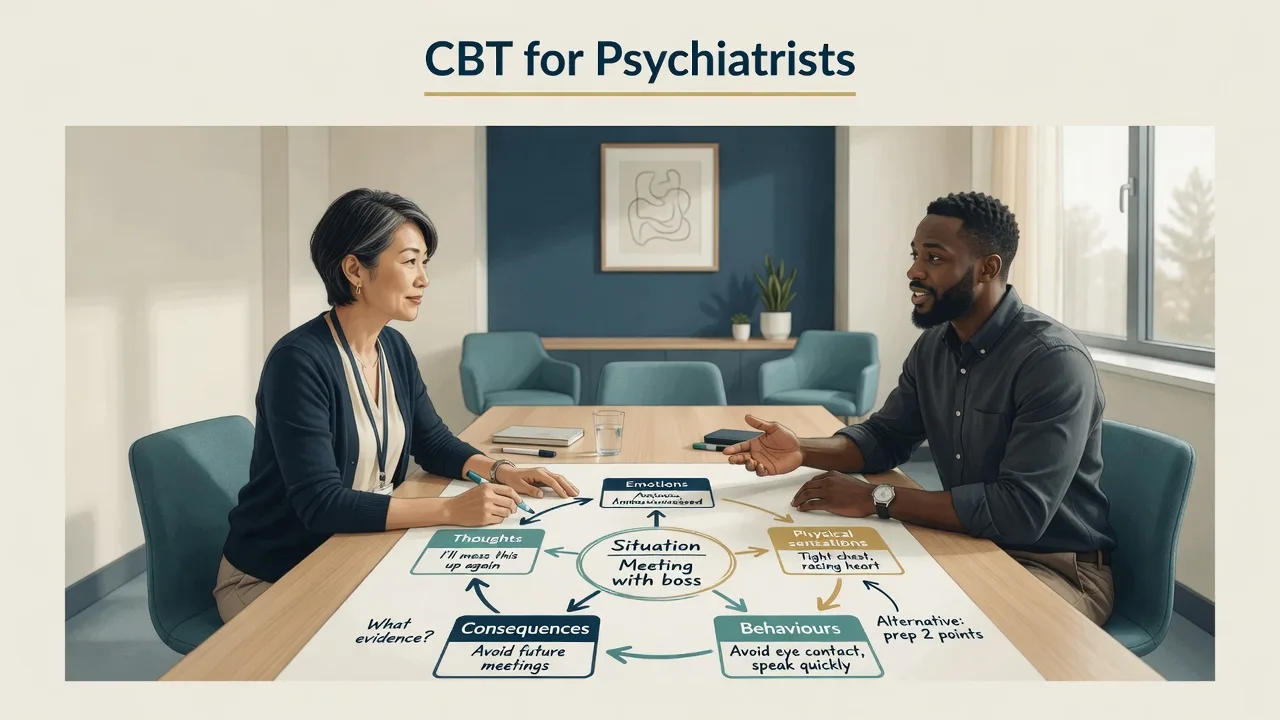
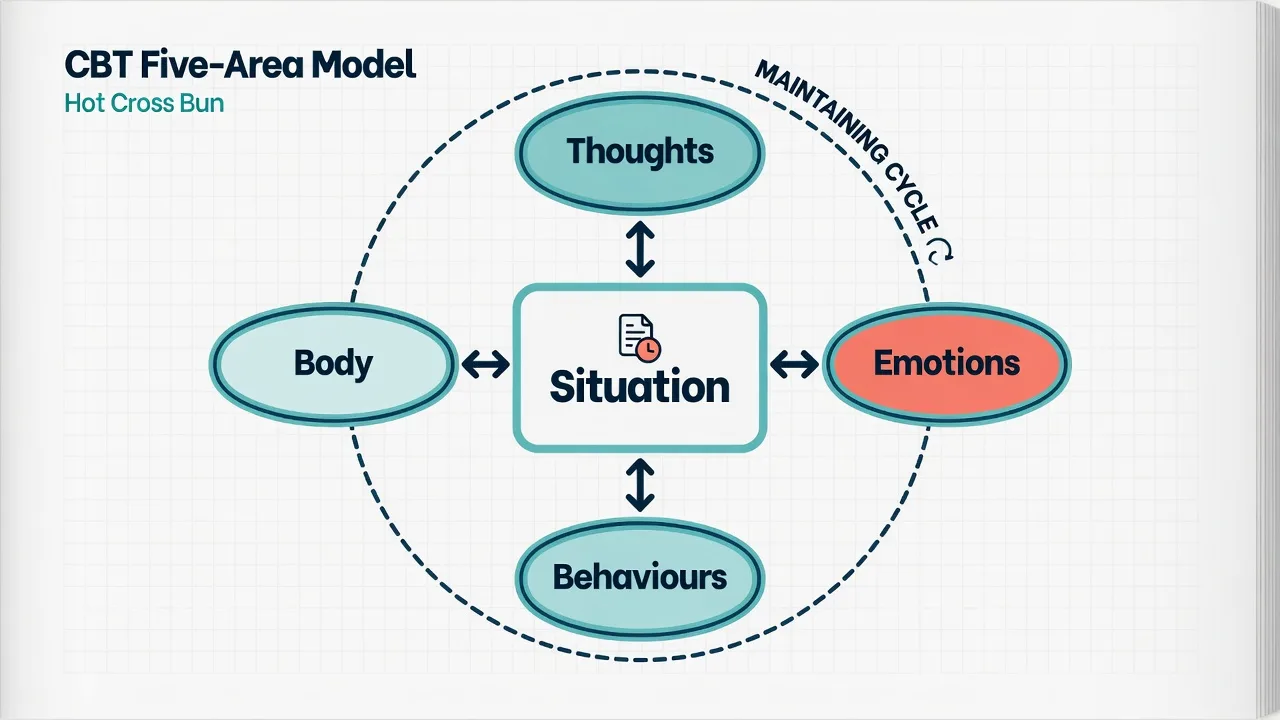
Five-area (hot-cross-bun) model
A practical cross-sectional map: situation linked bidirectionally to thoughts, emotions, body sensations, and behaviours, with loops that maintain the problem.[2]
Disorder-specific cognitive models (high-yield)
Depression (Beck). Negative cognitive triad (self, world, future), schema activation, processing biases; behavioural withdrawal reduces reinforcement and confirms hopelessness.[1][2][3]
Panic (Clark). Catastrophic misinterpretation of benign bodily sensations (e.g. palpitations → “heart attack”) plus safety behaviours that prevent disconfirmation and maintain threat belief.[4]
PTSD (Ehlers–Clark line / CT-PTSD). Poorly elaborated trauma memory, negative appraisals, and strategies intended to control threat that maintain a sense of current danger; cognitive therapy protocols target these processes.[5]
OCD. Inflated responsibility/threat appraisals; compulsions and avoidance function as safety behaviours that block learning that obsessions do not require ritual — same safety-behaviour logic that maintains anxiety disorders more broadly.[4][6]
Psychosis (CBTp). Focus on meaning of experiences, safety behaviours, and reasoning biases — not arguing the person out of voices by force; always adjunctive to medical care.[11]
Longitudinal and cross-sectional formulation
Exam-standard CBT formulation has two layers: (1) Longitudinal — early experiences → core beliefs → conditional rules → compensatory strategies; (2) Cross-sectional — trigger → automatic thoughts → emotion/body → safety behaviours/avoidance → belief maintained.[2][13][14]
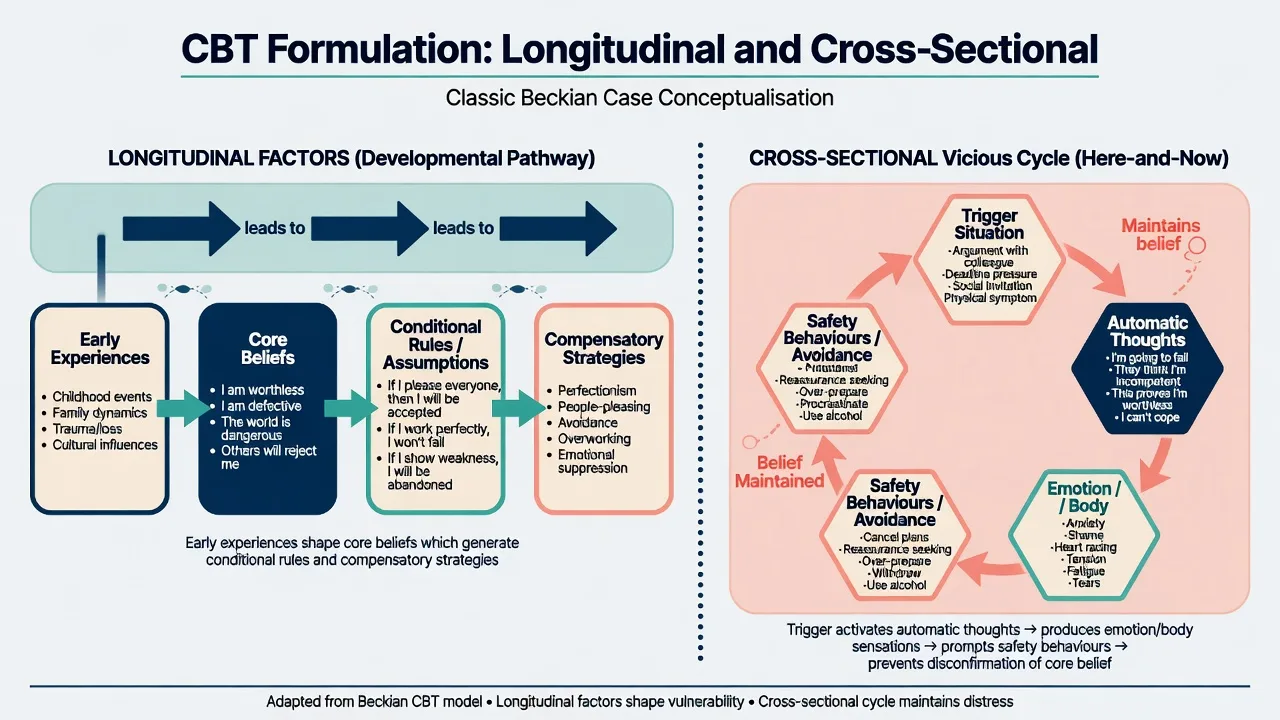
Collaborative conceptualisation can be rated for competence; shared, testable formulations outperform secret theories the patient never owns.[14] Formulation-driven CBT in routine anxious-depressed outpatients shows naturalistic benefit when problems are prioritised and methods matched to mechanisms.[13]
Course and session structure
Typical course architecture
Typical course architecture: (1) assessment and engagement (problem list, goals, measures, suitability, risk); (2) shared formulation (written/diagrammed, revisable); (3) active treatment (often about 8–20 sessions depending on disorder, severity, and protocol — OCD/PTSD often need fuller courses); (4) relapse prevention (self-therapy plan, early-warning signs, boosters).[6][8]
Session structure (non-negotiable for “this is CBT”)
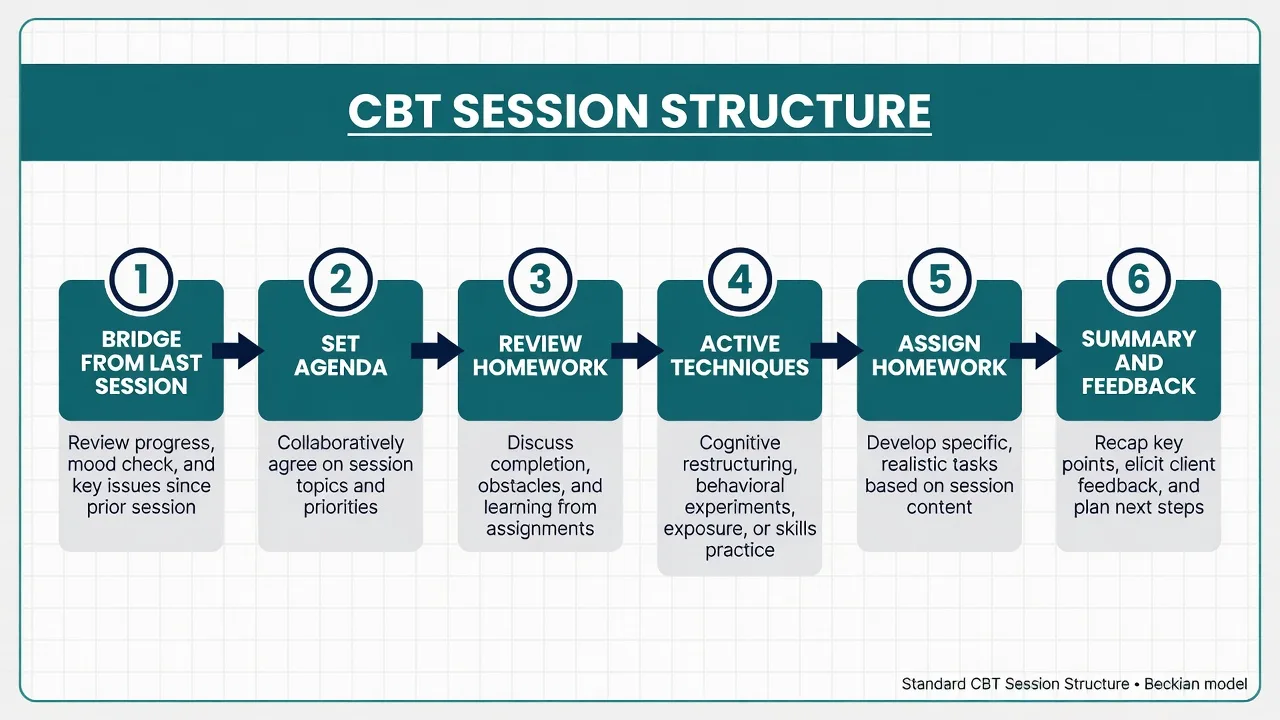
Standard session steps are: bridge (mood/risk check), collaborative agenda, homework review, active techniques matched to formulation, new specific homework, then summary and feedback. Session structure with homework review is core to fidelity; sessions without agenda and homework review are the classic exam definition of drift toward supportive counselling.[12][15][16]
Core technique families
Cognitive techniques
Thought records; identifying cognitive biases; evidence for/against; alternative balanced thoughts; continuum work; downward arrow to core beliefs when appropriate. In severe psychomotor slowing or dense rumination, do not force complex schema work first.[2][3]
Behavioural activation
Activity monitoring → values-linked scheduling → graded tasks → anti-avoidance. Targets the withdrawal–low reward–hopelessness loop of depression.[2][6]
Exposure and ERP
- Classic graded exposure: hierarchy, prolonged contact, drop safety behaviours.
- Inhibitory learning emphasis (viva depth): design exposures for expectancy violation, variability, and removal of safety strategies so new learning inhibits old threat associations — not only “stay until anxiety halves.”
- ERP for OCD: exposure to obsession triggers plus response prevention of rituals.
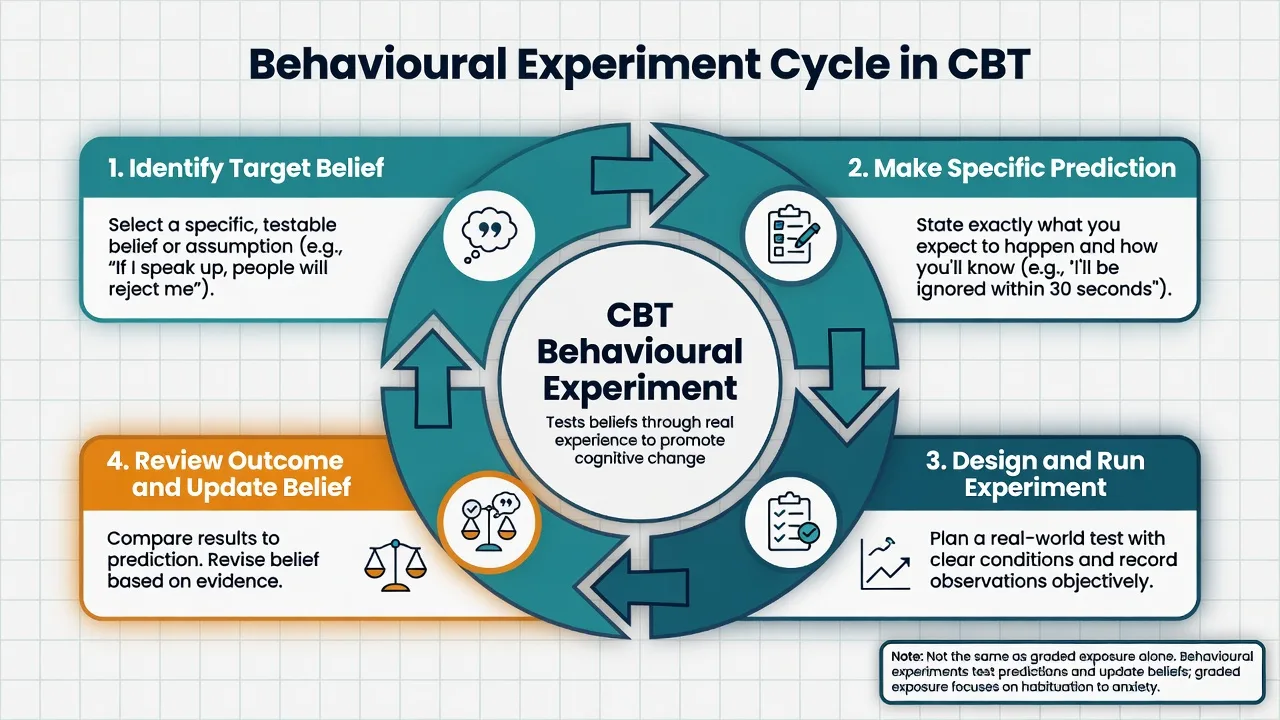
Behavioural experiments
Purpose-built belief tests: identify target belief → specific prediction → design and run experiment → review outcome and update belief. Related to exposure but not identical: the primary metric is belief change, not only fear reduction.[4][14]
Homework
Homework quantity and quality associate with better CBT outcomes in meta-analysis — design tasks that are specific, agreed, and reviewed.[12]
Indications and evidence by disorder
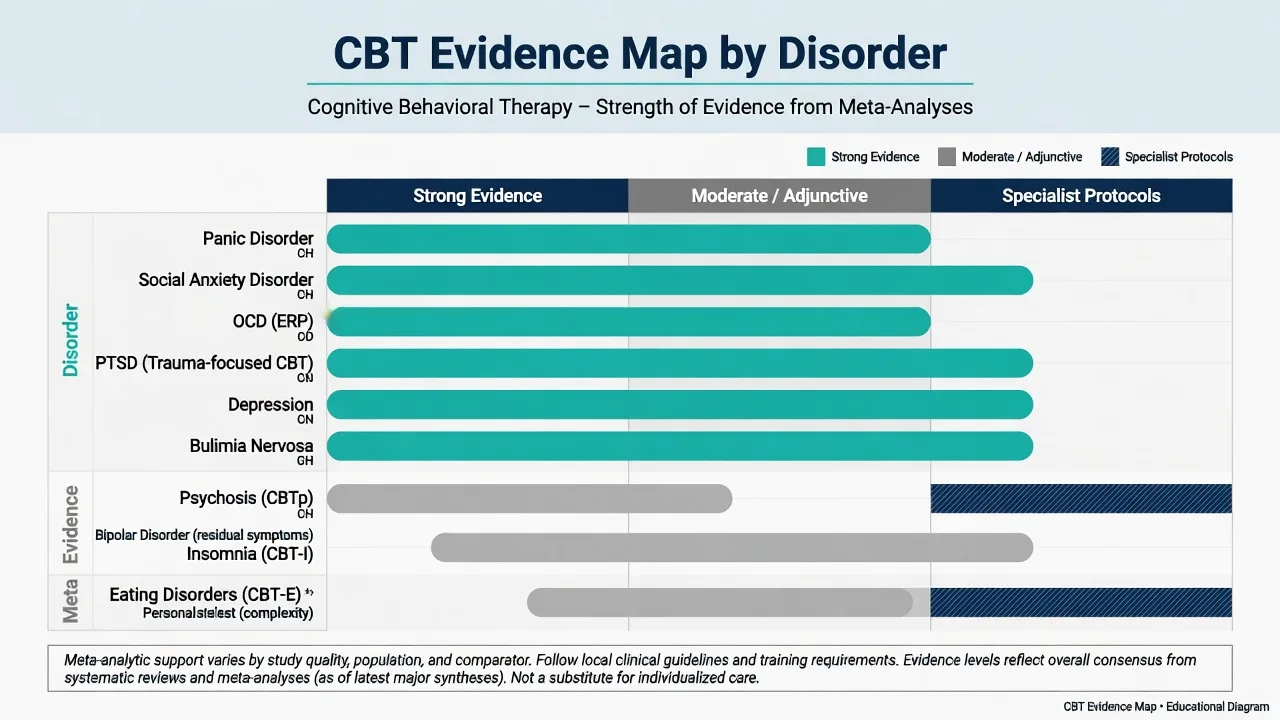
Meta-analytic reviews place CBT among the strongest evidence-based psychotherapies across many conditions; strongest signals often include anxiety disorders, depression, bulimia, and related problems, with more mixed or adjunctive roles elsewhere.[6][7][8]
Depression
Cognitive therapy can match antidepressant medication for moderate–severe depression in specialised settings, and shows advantages for relapse prevention after treatment ends compared with medication discontinued without skills transfer.[9][10] In practice, combine when severity, prior response, patient preference, or access demand it; never delay risk management for pure modality purity.
Anxiety disorders
Disorder-specific CBT (panic with interoceptive work and drop of safety behaviours; social anxiety with attention/video feedback and experiments; GAD with intolerance-of-uncertainty and worry postponement strategies) underpins guideline first-line psychological care.[4][6][7]
OCD
ERP-centred CBT is the psychological gold standard in meta-analytic overviews of CBT efficacy; SSRIs are pharmacological counterparts — combination is common for partial response. Psychiatrist role: accurate diagnosis, medical differentials, meds, and ensuring ERP actually happens (not only “anxiety management”).[6][7]
PTSD
Trauma-focused CBT/CT-PTSD protocols process memory and appraisals; non-trauma-focused supportive therapy is not a substitute when TF-CBT is indicated and available.[5]
Psychosis
CBTp shows modest average effect sizes as an adjunct; models and methods matter; it is not an alternative to antipsychotic treatment or acute risk care.[11]
Other
CBT packages extend across insomnia (CBT-I), specialised eating-disorder protocols (CBT-E), and bipolar residual work (adherence, early warning — not acute mania). Complex personality presentations may need longer, formulation-heavy CBT or alternative packages (e.g. DBT/schema pathways) depending on goals and risk — always matched to the evidence map for that presentation.[6][7][13]
Assessment for CBT (psychiatrist lens)
- Problem list and goals the person owns.
- Risk (suicide, violence, self-neglect) at baseline and each session.
- Organic/substance factors that alter formulation (thyroid, stimulant use, sleep apnoea, medication side effects).
- Alliance capacity, literacy/language, cultural explanatory models.
- Serial measures matched to disorder (e.g. PHQ-9, GAD-7, Y-BOCS, PCL — use local approved tools).
- Prior therapy: what was tried, homework adherence, exposure avoided? [13] [14]
Integrating CBT with pharmacotherapy
Practical stances: moderate depression — CT/CBT with or without antidepressant by preference, severity, access, and past response; severe depression with psychosis — antipsychotic/antidepressant pathways primary, CBT adjunct when able; panic/OCD — CBT/ERP often first-line psychological care, SSRI when preferred or needed; schizophrenia — antipsychotic foundation with CBTp for residual distress/appraisals; benzodiazepine dependence — plan deprescribing while exposure skills reduce “pill as safety behaviour.” Integration choices should reflect comparative efficacy data (e.g. CT vs antidepressants in depression trials) and the adjunctive role of CBTp in psychosis, not modality ideology.[9][10][11]
Shared formulation language helps MDTs avoid split plans (“meds team vs therapy team”) and keeps pharmacological and psychological targets aligned.[13][14]
Therapist drift, fidelity, and supervision
Therapist drift is delivering something safer/easier for the clinician than the evidence-based active ingredients (e.g. endless validation without exposure; skipping homework review; delaying ERP).[15][16] Patients and clinicians may disagree on which techniques matter — supervision and outcome data realign practice.[16]
Supervision for psychiatrists who deliver or oversee CBT should review: recordings or detailed process notes, formulation updates, homework design, exposure quality, risk, and cultural fit — not only case support — so that active ingredients are delivered rather than avoided.[14][15]
Special populations
- Youth: developmental language, parent/carer involvement, school behavioural experiments.
- Older adults: pacing, sensory limits, medical comorbidity, grief, polypharmacy.
- Perinatal: risk, sleep, attachment, medication co-decision; do not moralise help-seeking.
- Intellectual disability / neurodivergence: simplify, more behavioural, visual supports, carer coaching.
- Cultural diversity / Indigenous care: co-construct meaning of “thoughts” and family roles; use interpreters properly; avoid cognitive imperialism (correcting culturally normative beliefs as “distortions”).
- Forensic: motivation, secondary gain, risk-focused targets, clear boundaries. [7] [14]
Regional guidance (ANZ-aware)
ANZ / FRANZCP context. Psychological therapies including CBT are core to comprehensive psychiatric care and WBAs. Access is uneven (public waitlists, Better Access / private psychology interfaces, rural gaps). Psychiatrists must still formulate and refer competently, deliver elements within skill, and not claim protocol competence they lack (e.g. intensive ERP, CT-PTSD). UK NICE pathways heavily feature stepped CBT for depression and anxiety; APA practice guidelines similarly endorse CBT for many disorders; RANZCP clinical practice guidelines embed psychological therapy recommendations disorder-by-disorder. Always apply the current local guideline and service pathway rather than memorised session counts alone.[6][7][8]
Complications and pitfalls
- Pseudo-CBT without structure.
- Over-intellectual cognitive work without behavioural change.
- Premature deep schema work in acute depression.
- Exposure with intact safety behaviours.
- Cultural invalidation via “cognitive distortion” language.
- Boundary failures in longer therapy relationships.
- Ignoring iatrogenic perpetuating factors (invalidating systems, chaotic care). [15] [16]
Prognosis and disposition
Outcomes depend on diagnosis, severity, fidelity, homework, comorbidity, and social context.[6][7] Non-response after an adequate dose of competent CBT should trigger reformulation (wrong targets? undiagnosed OCD/PTSD/autism? substance? bipolar? secondary gain? drift?), not endless unstructured extension. Step up intensity, switch protocol, add or optimise medication, or change modality with a clear rationale. Relapse-prevention planning is part of ending, not an afterthought.[10]
Exam pearls
CBT session checklist (BRIDGE)
- Primary aim: test a specific belief/prediction
- Success metric: belief update after review
- May include exposure elements but is hypothesis-driven
- Primary aim: new learning about threat and drop of avoidance/rituals
- Success metric: reduced avoidance, expectancy violation, ritual prevention
- Safety behaviours must be identified and removed
- Warmth without agenda, homework, or active methods
- High risk of therapist drift
- Fails exam and fidelity standards
*Effects depend on sample, therapist competence, and setting — quote cautiously in viva; cite the trial context.[9][10][12]
Summary for viva / CASC
- Define CBT as structured collaborative empiricism targeting maintaining processes.
- Draw a five-area cycle and a longitudinal belief pathway.
- Structure every session (agenda, homework, active work).
- Match techniques to disorder models (panic, OCD ERP, BA, TF-CBT, CBTp adjunct).
- Integrate meds without modality wars; never drop risk or antipsychotics for therapy ideology.
- Name drift, supervise fidelity, measure outcomes, revise formulation.
References
- [1]Beck AT Thinking and depression. II. Theory and therapy Arch Gen Psychiatry, 1964.PMID 14159256
- [2]Beck AT The evolution of the cognitive model of depression and its neurobiological correlates Am J Psychiatry, 2008.PMID 18628348
- [3]Kovacs M, Beck AT Maladaptive cognitive structures in depression Am J Psychiatry, 1978.PMID 645943
- [4]Clark DM A cognitive approach to panic Behav Res Ther, 1986.PMID 3741311
- [5]Ehlers A, Clark DM, Hackmann A, et al. Cognitive therapy for post-traumatic stress disorder: development and evaluation Behav Res Ther, 2005.PMID 15701354
- [6]Butler AC, Chapman JE, Forman EM, Beck AT The empirical status of cognitive-behavioral therapy: a review of meta-analyses Clin Psychol Rev, 2006.PMID 16199119
- [7]Hofmann SG, Asnaani A, Vonk IJ, et al. The Efficacy of Cognitive Behavioral Therapy: A Review of Meta-analyses Cognit Ther Res, 2012.PMID 23459093
- [8]David D, Cristea I, Hofmann SG Why Cognitive Behavioral Therapy Is the Current Gold Standard of Psychotherapy Front Psychiatry, 2018.PMID 29434552
- [9]DeRubeis RJ, Hollon SD, Amsterdam JD, et al. Cognitive therapy vs medications in the treatment of moderate to severe depression Arch Gen Psychiatry, 2005.PMID 15809408
- [10]Hollon SD, DeRubeis RJ, Shelton RC, et al. Prevention of relapse following cognitive therapy vs medications in moderate to severe depression Arch Gen Psychiatry, 2005.PMID 15809409
- [11]Wykes T, Steel C, Everitt B, Tarrier N Cognitive behavior therapy for schizophrenia: effect sizes, clinical models, and methodological rigor Schizophr Bull, 2008.PMID 17962231
- [12]Kazantzis N, Whittington C, Zelencich L, et al. Quantity and Quality of Homework Compliance: A Meta-Analysis of Relations With Outcome in Cognitive Behavior Therapy Behav Ther, 2016.PMID 27816086
- [13]Persons JB, Roberts NA, Zalecki CA, et al. Naturalistic outcome of case formulation-driven cognitive-behavior therapy for anxious depressed outpatients Behav Res Ther, 2006.PMID 16209865
- [14]Kuyken W, Beshai S, Dudley R, et al. Assessing Competence in Collaborative Case Conceptualization: Development and Preliminary Psychometric Properties of the Collaborative Case Conceptualization Rating Scale Behav Cogn Psychother, 2016.PMID 25629820
- [15]Mulkens S, de Vos C, de Graaff A, Waller G To deliver or not to deliver cognitive behavioral therapy for eating disorders: Replication and extension of our understanding of why therapists fail to do what they should do Behav Res Ther, 2018.PMID 29763767
- [16]Hernandez Hernandez ME, Waller G Are we on the same page? A comparison of patients' and clinicians' opinions about the importance of CBT techniques Cogn Behav Ther, 2021.PMID 33475024